Embed Size (px)
Citation preview

TREAT – A Decision Support System TREAT – A Decision Support System for Antibiotic Treatmentfor Antibiotic Treatment
S. Andreassen1, L.E Kristensen2,
L. Leibovici3, U. Frank4,
J. H. Jensen1, H. C. Schønheyder5 1Aalborg University, Denmark
2Judex Datasystems A/S, Denmark3Rabin Med. Ctr., Petah-Tiqva, Israel
4Freiburg Univ. Hosp., Germany
5Aalborg Hospital, Denmark
Supported by an EU 5th Framework grant
(TREAT, IST 1999-11459)
Operational project goals
1. Build TREAT - a model of infections and their therapy, based on Causal Probabilistic Nets and on Decision Theory
2. Implement TREAT as a system integrated into the hospital information infrastructure (TREAT-LAB and TREAT-WARD)
3. Test TREAT in 3 countries to show that it can improve diagnosis and treatment of severe infections by
• reducing the percentage (30-40%) of inappropriate antibiotic treatments to half, thereby reducing the infection related mortality
• reducing cost of therapy
• restricting the use of broad-spectrum antibiotics
• stemming the rise of antibiotic resistance
4. Achieve scientific and commercial dissemination
A model of infections
A (very) simplified version of the TREAT CPN will be used:
1. to demonstrate the concepts of • infection• sepsis• prognosis (sepsis*)• treatment• coverage and• mortality
2. to demonstrate the value of morphology, Gram stain and motility

Two urinary tract pathogens

Sepsis = Yes, Treatment = No,Res. Factor = Present (Hosp. Acq.)
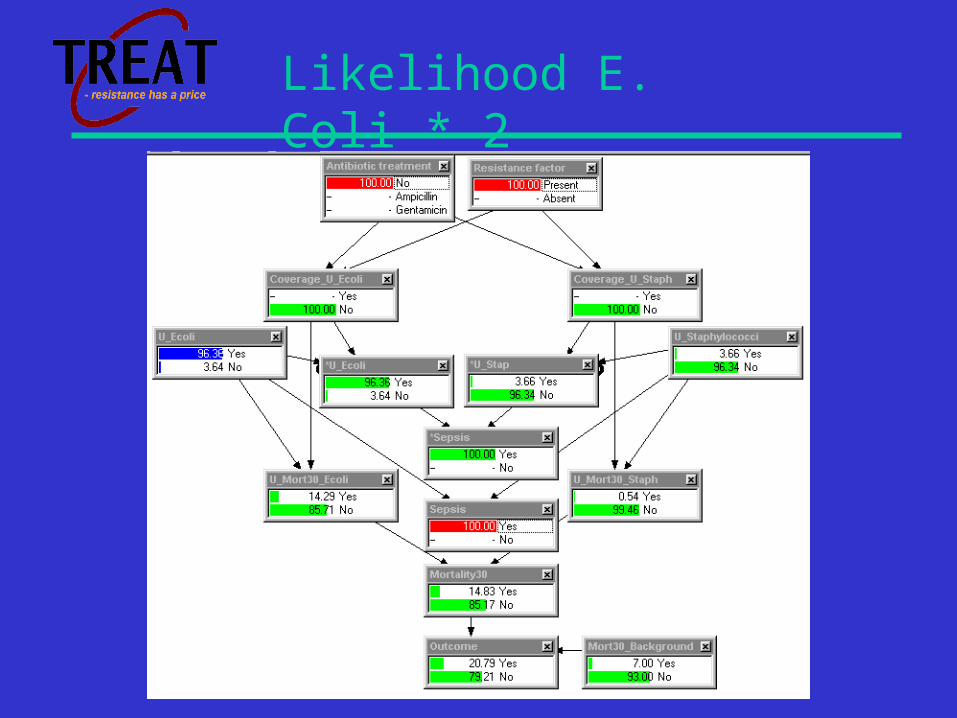
Likelihood E. Coli * 2

Treatment = Gentamicin
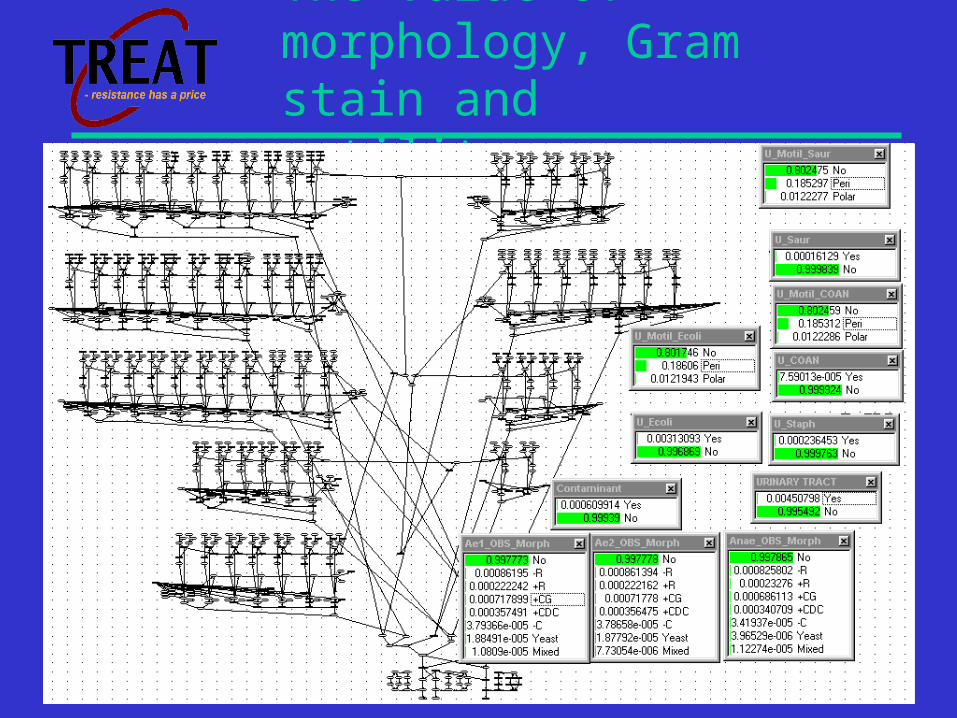
The value of morphology, Gram stain and motility

Gram negative rods isolated from blood culture
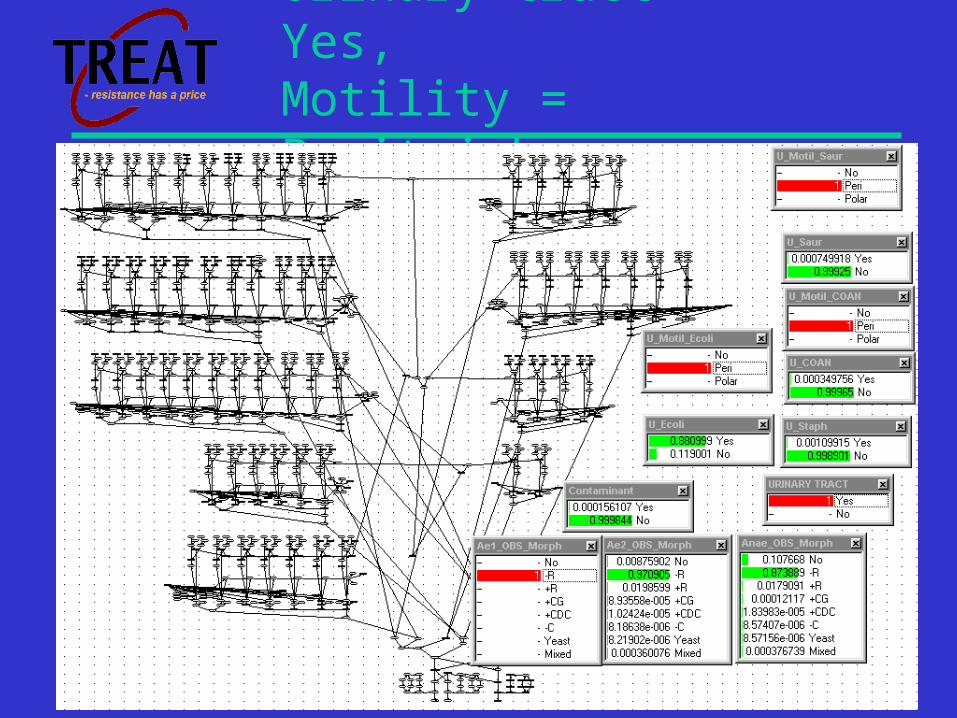
Urinary tract = Yes,Motility = Peritrichous

Databases for local calibrations
To adapt the TREAT system to a given hospital,
databases are needed for:
• Infection related mortality
• Cost of treatments
• Antibiotics
• Resistance and cross-resistance
• Pathogen prevalences (influenced by risk factors,
ICD diagnoses)

Database for crude mortality
Mortality per site of infection dependent on coverage of empirical and semi-empirical treatment

Database for costs of treatments considered by TREAT

Database for antibiotics
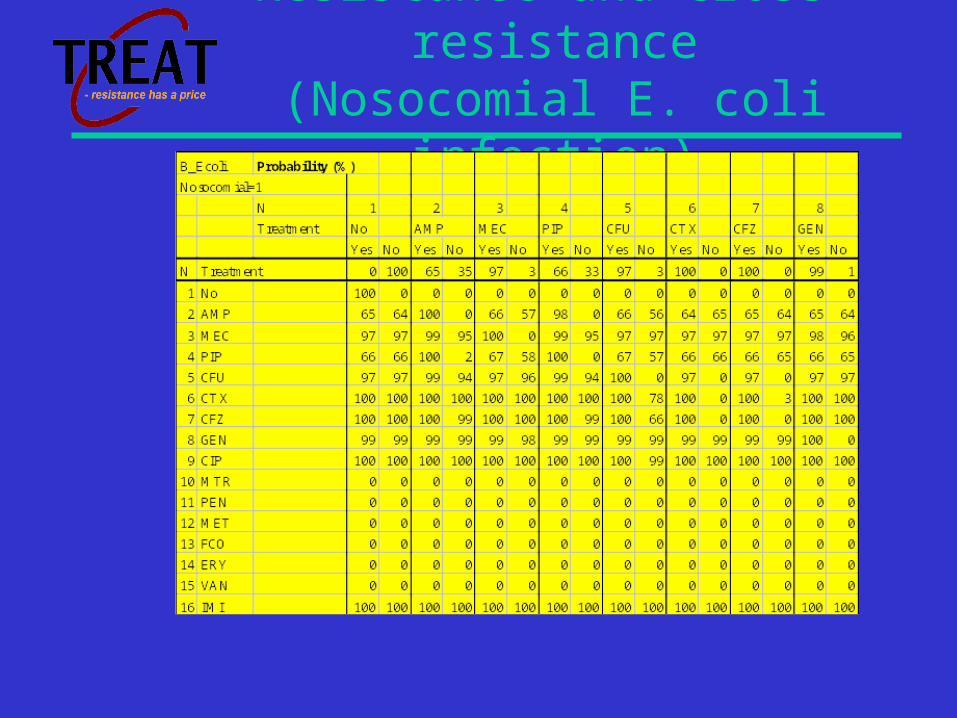
Resistance and cross-resistance (Nosocomial E. coli infection)

Balance for each antibiotic drug:
• Benefits:– reduced mortality,
morbidity and hospital stay related to coverage, activity at the site of infection, and synergism.
• Detriments:– cost of drug,
administration and monitoring.
– side-effects.– ecological costs.

Non-interventional study in 813 Danish bacteraemic patients:
N=813
Age>65 yrs. 61%
ICU 11%
Source: Urinary 28%
Source: Abdominal 23%
Source: Lungs 13%
30-day fatality 20%

Non-interventional study in 813 Danish bacteraemic patients:
Physician - empirical
Physician-semi
DSS
Coverage 59% 78% 87%
Mean cost, $ 187.5 223.5 201.0
Mean, side-effects, $
100.0 115.0 117.5
Mean, resistance, $
1626.5 1874.5 1511
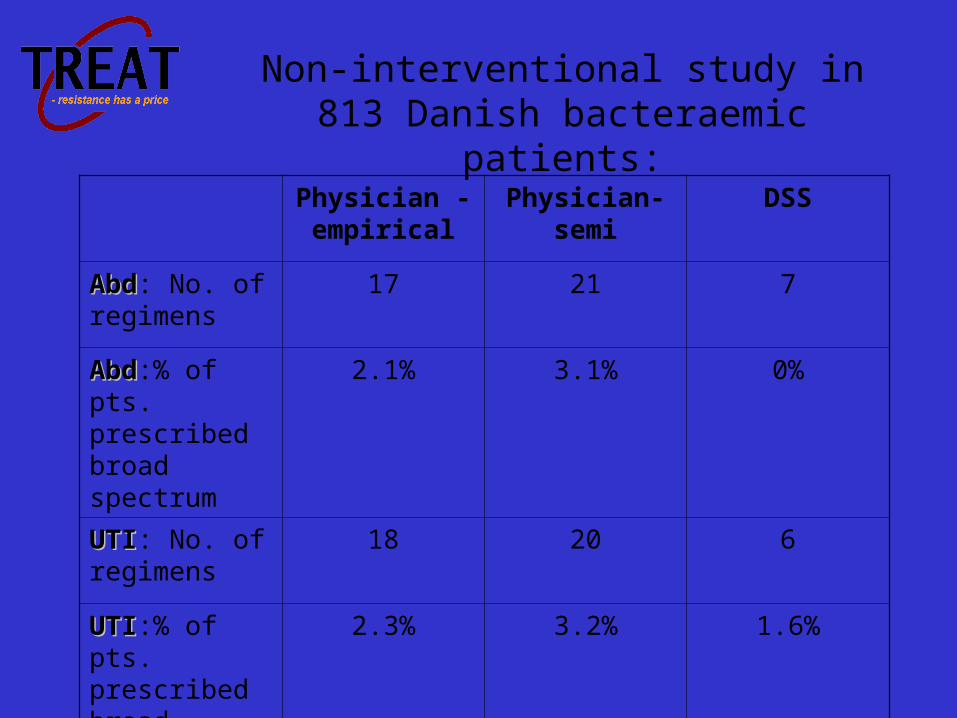
Physician - empirical
Physician-semi DSS
AbdAbd: No. of regimens
17 21 7
AbdAbd:% of pts. prescribed broad spectrum
2.1% 3.1% 0%
UTIUTI: No. of regimens
18 20 6
UTIUTI:% of pts. prescribed broad spectrum
2.3% 3.2% 1.6%
Non-interventional study in 813 Danish bacteraemic patients:

Conclusions:
• TREAT – a computerised DSS – prescribed appropriate antibiotic treatment more often than the attending physician, while using less broad-spectrum antibiotics at a lesser cost.
• The use of a causal probabilistic net as the basic model allowed us to combine data from several sources with knowledge; and to calibrate the system to different sites, in different countries.
• A randomised, controlled trial of the system in 3 countries is due to start in 6 months.