Embed Size (px)
Citation preview

NATURE REVIEWS | CARDIOLOGY VOLUME 9 | MARCH 2012 | 133
Department of Cardiac Surgery, San Raffaele University Hospital, Via Olgettina 60, 20132 Milan, Italy (M. De Bonis, F. Maisano, G. La Canna, O. Alfieri).
Correspondence to: M. De Bonis [email protected]
Treatment and management of mitral regurgitationMichele De Bonis, Francesco Maisano, Giovanni La Canna and Ottavio Alfieri
Abstract | Mitral regurgitation (MR) is the most-common valvular heart disease in the western world. From an etiologic point of view, MR can be either organic (mainly degenerative in western countries) or functional (secondary to left ventricular remodeling in the context of ischemic or idiopathic dilated cardiomyopathy). Degenerative and functional MR are completely different disease entities that pose specific decision-making problems and require different management. The natural history of severe degenerative MR is clearly unfavorable. However, the appropriate and timely correction of degenerative MR is associated with a life expectancy similar to that of the normal population. By contrast, the prognostic impact of the correction of functional MR is still a matter of debate. In this Review, we discuss the optimal treatment of both degenerative and functional MR, taking into account all presently available therapeutic options, including novel percutaneous methods. Since a clear understanding of the etiology and mechanisms of valvular dysfunction is important to guide the timing and choice of treatment, the role of echocardiography in the management of MR is also addressed.
De Bonis, M. et al. Nat. Rev. Cardiol. 9, 133–146 (2012); published online 22 November 2011; doi:10.1038/nrcardio.2011.169
IntroductionMitral regurgitation (MR) is the most-frequent clini-cally recognizable valvular heart disease in the western world.1 MR can be the consequence of primary anato mical changes that affect the leaflets and subvalvular appara tus (organic MR), or result from left ventricular (LV) remodel-ing that has led to the dislocation of the papillary muscles and tethering of the leaflets in the presence of a morpho-logically normal valve (functional MR). Organic and functional MR are totally different disease entities with regard to pathophysiology, prognosis, decision-making problems, and management and are, therefore, discussed separately in this article. The most-common etiology of organic MR in industrialized countries is degenerative mitral valve (MV) disease, either as a result of myxoma-tous degeneration or of fibroelastic deficiency of the valve tissue, leading to MV prolapse. Less-common etiologies of organic MR are rheumatic heart disease, which remains prevalent in developing countries, and congenital anom-alies.2 Functional MR worsens the prognosis of patients with dilated cardiomyopathy.3,4 Ischemic MR is a sub-category of functional MR in which LV dysfunction is the consequence of a previous myocardial infarction. The natural history of severe MR is clearly unfavorable, leading to LV failure, pulmonary hypertension, atrial fibrillation,
stroke, and death.5 Appropriate and timely correction of degenerative MR, however, has a highly beneficial impact on the prognosis of patients and can even be associated with a life expectancy and a quality of life similar to those of the general population.6
Guidelines for the management of patients with organic and functional MR have been published by the American College of Cardiology (ACC)/American Heart Association (AHA),7 as well as by the European Society of Cardiology (ESC).8 Although recommendations are rarely made on the basis of results from randomized clinical trials, a con-sensus among experts was achieved after an extensive review of published data. However, low adherence to exist-ing guidelines in clinical practice has been documented,9 and persistent dissemination of updated knowledge in the field is, therefore, important to favorably influence the outcome of patients with MR.
Over the past decade, new information on the natural history and risk stratification of patients with MR has accumulated, and new imaging modalities have been introduced. Reliable and reproducible techniques for MV repair have been developed together with minimally invasive approaches, and even percutaneous methods are emerging as convenient therapeutic options in parti-cular circumstances. A multidisciplinary approach to the evaluation and treatment of patients with valvular heart disease is becoming a reality in many institutions, where cardiologists, cardiac surgeons, imaging specialists, and anesthesiologists cooperate to provide the best treatment for the individual patient.
In this Review, we focus on the optimal management of patients with degenerative or functional MR. The current
Competing interestsF. Maisano declares associations with the following companies: Abbott, Medtronic, St Jude Medical, and Valtech Cardio. G. La Canna declares an association with Abbott. O. Alfieri declares associations with the following companies: 4Tech, Edwards Lifesciences, Symetis, and Valtech Cardio. See the article online for full details of the relationships. M. De Bonis declares no competing interests.
REVIEWS
© 2012 Macmillan Publishers Limited. All rights reserved
134 | MARCH 2012 | VOLUME 9 www.nature.com/nrcardio
position of percutaneous methods in the armamentarium for treatment of patients with MR is discussed on the basis of the available data. Because the essential role of echo-cardiography in diagnosis, comprehensive evaluation, and decision-making is universally recognized, we first provide an update on the use of this imaging modality in the setting of MR.
Key points
■ Degenerative and functional mitral regurgitation (MR) are completely different disease entities, each posing specific challenges with regard to decision-making and management
■ 2D and 3D echocardiography capture important physiological information and provide the roadmap for the treatment of patients with MR
■ Surgical mitral valve (MV) repair is the preferred treatment for patients with severe degenerative MR and can improve life expectancy to normal levels if performed adequately and in a timely manner
■ In patients with functional MR, annuloplasty should only be carried out in the presence of echocardiographic predictors of successful repair; MV replacement should be considered when unsatisfactory results are expected
■ Transcatheter correction of MR (MV repair or replacement) represents a novel field of cardiovascular medicine and is expected to change surgical practice in the future
■ Use of the MitraClip® should currently be reserved for patients with functional or degenerative MR who are unsuitable for surgery or have a very high surgical risk
The role of echocardiographyEchocardiography provides most of the relevant infor-mation for the decision-making process with regard to treatment of patients with MR, including the severity of MR, the type of lesion and mechanism according to the Carpentier classification for MR, and the anatomical feat-ures of the valve. Furthermore, information about size and function of the left ventricle, the dimensions of the left atrium, and the presence of pulmonary hyper tension is provided. In patients with severe degenerative MR, optimal outcome is achieved when surgery is carried out before symptoms, or LV dysfunction, pulmonary hyper-tension, and arrhythmias are detectable. Such early surgery, however, is only recommended if a durable MV repair is likely, and assessing the feasibility of successful repair is thus crucial. Matching 2D-multiplane images and Doppler analysis, echocardiography enables clinicians to evaluate reliably the cross-sectional anatomy of the MV apparatus. 2D-transthoracic echocardiography and trans-esophageal echocardiography (TEE) can provide useful information concerning the likelihood of MV repair.10,11 However, 2D echocardiography can be affected by limited cut planes and is operator-dependent. Therefore, particu-larly for patients with complex MV lesions, evaluating the feasibility of repair before surgery might be difficult.
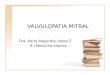
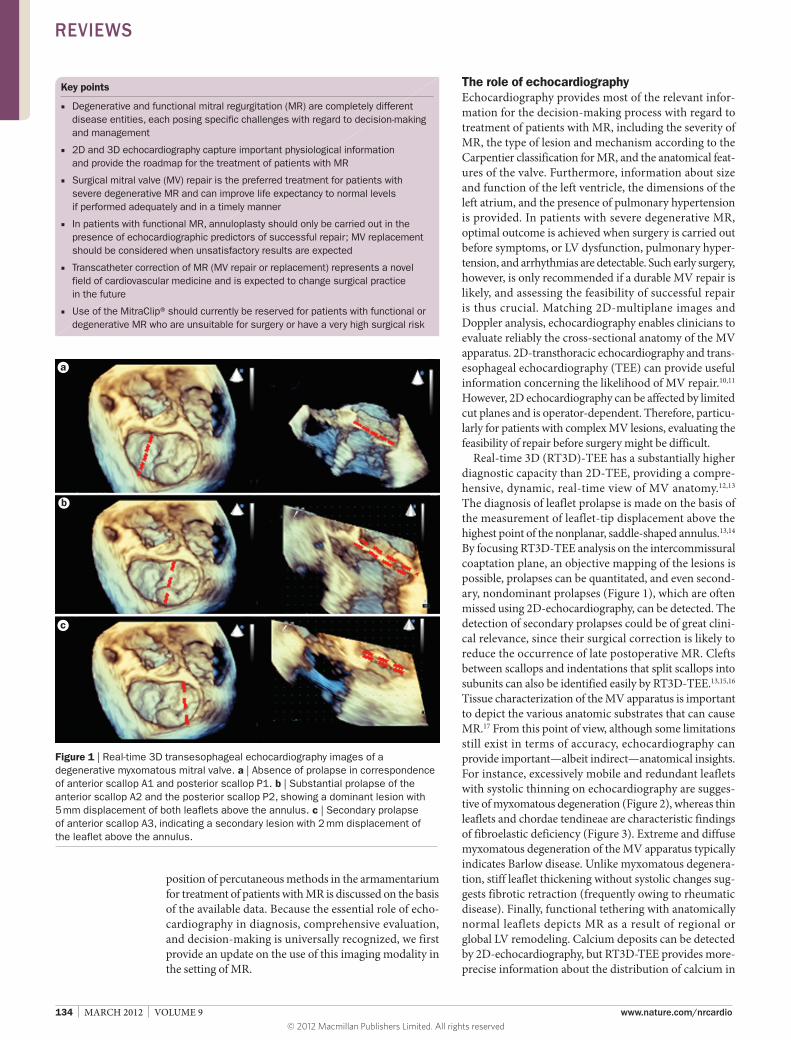
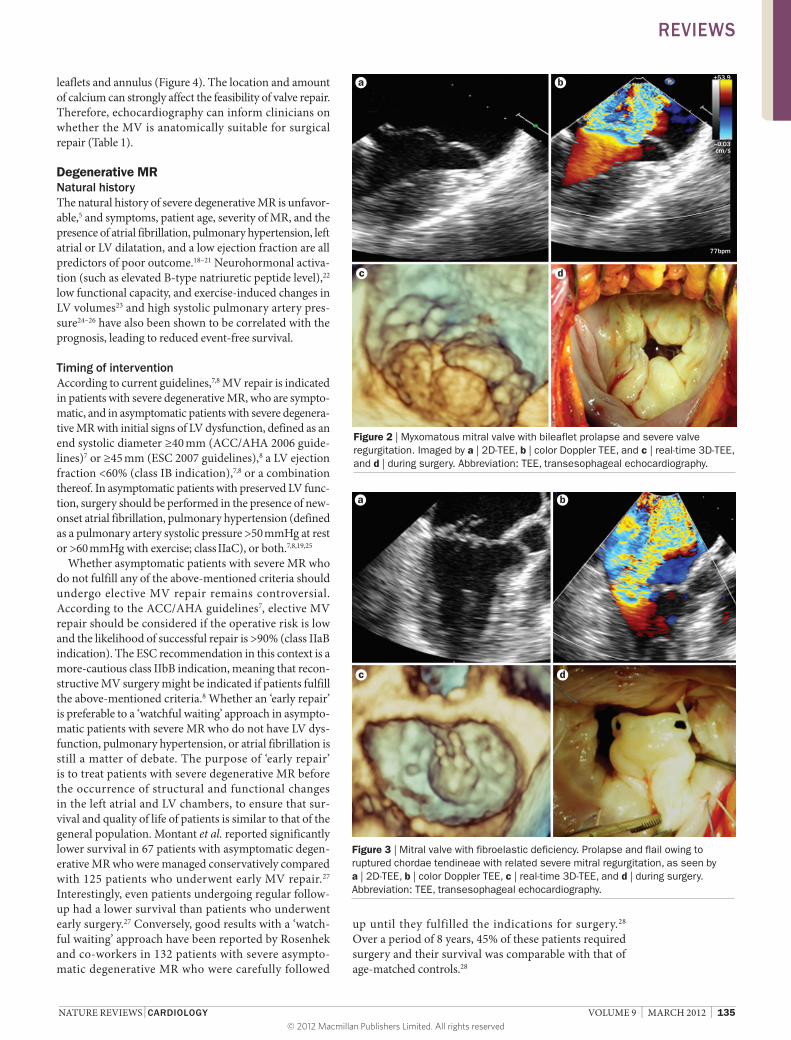
Real-time 3D (RT3D)-TEE has a substantially higher diagnostic capacity than 2D-TEE, providing a compre-hensive, dynamic, real-time view of MV anatomy.12,13 The diagnosis of leaflet prolapse is made on the basis of the measurement of leaflet-tip displacement above the highest point of the nonplanar, saddle-shaped annulus.13,14 By focusing RT3D-TEE analysis on the intercommissural coaptation plane, an objective mapping of the lesions is possible, prolapses can be quantitated, and even second-ary, nondominant prolapses (Figure 1), which are often missed using 2D-echocardiography, can be detected. The detection of secondary prolapses could be of great clini-cal relevance, since their surgical correction is likely to reduce the occurrence of late postoperative MR. Clefts between scallops and indentations that split scallops into subunits can also be identified easily by RT3D-TEE.13,15,16 Tissue characterization of the MV apparatus is important to depict the various anatomic substrates that can cause MR.17 From this point of view, although some limitations still exist in terms of accuracy, echocardiography can provide important—albeit indirect —anatomical insights. For instance, excessively mobile and redundant leaflets with systolic thinning on echocardiography are sugges-tive of myxomatous degeneration (Figure 2), whereas thin leaflets and chordae tendineae are characteristic findings of fibroelastic deficiency (Figure 3). Extreme and diffuse myxomatous degeneration of the MV apparatus typically indicates Barlow disease. Unlike myxomatous degenera-tion, stiff leaflet thickening without systolic changes sug-gests fibrotic retraction (frequently owing to rheumatic disease). Finally, functional tethering with anatomically normal leaflets depicts MR as a result of regional or global LV remodeling. Calcium deposits can be detected by 2D-echocardiography, but RT3D-TEE provides more-precise information about the distribution of calcium in
Figure 1 | Real-time 3D transesophageal echocardiography images of a degenerative myxomatous mitral valve. a | Absence of prolapse in correspondence of anterior scallop A1 and posterior scallop P1. b | Substantial prolapse of the anterior scallop A2 and the posterior scallop P2, showing a dominant lesion with 5 mm displacement of both leaflets above the annulus. c | Secondary prolapse of anterior scallop A3, indicating a secondary lesion with 2 mm displacement of the leaflet above the annulus.
a
b
c
REVIEWS
© 2012 Macmillan Publishers Limited. All rights reserved
NATURE REVIEWS | CARDIOLOGY VOLUME 9 | MARCH 2012 | 135
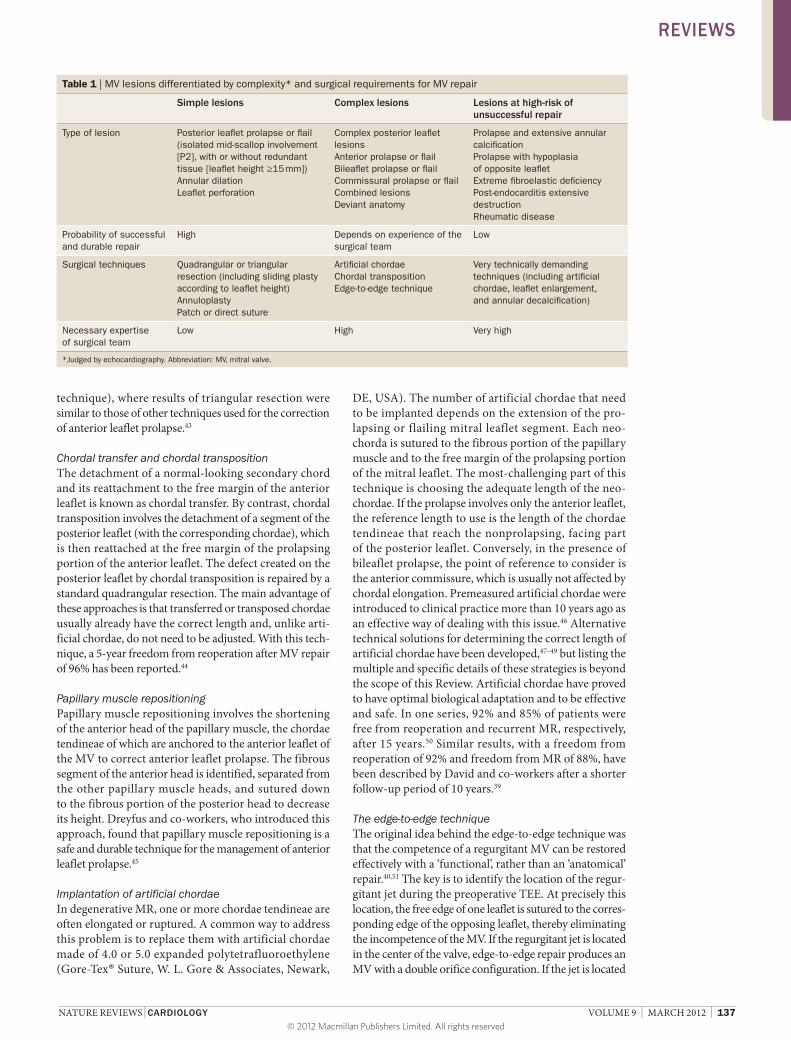
leaflets and annulus (Figure 4). The location and amount of calcium can strongly affect the feasibility of valve repair. Therefore, echocardiography can inform clinicians on whether the MV is anatomically suitable for surgical repair (Table 1).
Degenerative MRNatural historyThe natural history of severe degenerative MR is unfavor-able,5 and symptoms, patient age, severity of MR, and the presence of atrial fibrillation, pulmonary hypertension, left atrial or LV dilatation, and a low ejection fraction are all predictors of poor outcome.18–21 Neurohormonal activa-tion (such as elevated B-type natriuretic peptide level),22 low functional capacity, and exercise-induced changes in LV volumes23 and high systolic pulmonary artery pres-sure24–26 have also been shown to be correlated with the prognosis, leading to reduced event-free survival.
Timing of interventionAccording to current guidelines,7,8 MV repair is indicated in patients with severe degenerative MR, who are sympto-matic, and in asymptomatic patients with severe degenera-tive MR with initial signs of LV dysfunction, defined as an end systolic diameter ≥40 mm (ACC/AHA 2006 guide-lines)7 or ≥45 mm (ESC 2007 guidelines),8 a LV ejection fraction <60% (class IB indication),7,8 or a combination thereof. In asymptomatic patients with preserved LV func-tion, surgery should be performed in the presence of new-onset atrial fibrillation, pulmonary hypertension (defined as a pulmonary artery systolic pressure >50 mmHg at rest or >60 mmHg with exercise; class IIaC), or both.7,8,19,25
Whether asymptomatic patients with severe MR who do not fulfill any of the above-mentioned criteria should undergo elective MV repair remains controversial. According to the ACC/AHA guidelines7, elective MV repair should be considered if the operative risk is low and the likelihood of successful repair is >90% (class IIaB indication). The ESC recommendation in this context is a more-cautious class IIbB indication, meaning that recon-structive MV surgery might be indicated if patients fulfill the above-mentioned criteria.8 Whether an ‘early repair’ is preferable to a ‘watchful waiting’ approach in asympto-matic patients with severe MR who do not have LV dys-function, pulmonary hypertension, or atrial fibrillation is still a matter of debate. The purpose of ‘early repair’ is to treat patients with severe degenerative MR before the occurrence of structural and functional changes in the left atrial and LV chambers, to ensure that sur-vival and quality of life of patients is similar to that of the general population. Montant et al. reported significantly lower survival in 67 patients with asymptomatic degen-erative MR who were managed conservatively compared with 125 patients who underwent early MV repair.27 Interestingly, even patients undergoing regular follow-up had a lower survival than patients who underwent early surgery.27 Conversely, good results with a ‘watch-ful waiting’ approach have been reported by Rosenhek and co-workers in 132 patients with severe asympto-matic degenerative MR who were carefully followed
up until they fulfilled the indications for surgery.28 Over a period of 8 years, 45% of these patients required surgery and their survival was comparable with that of age-matched controls.28
Figure 2 | Myxomatous mitral valve with bileaflet prolapse and severe valve regurgitation. Imaged by a | 2D-TEE, b | color Doppler TEE, and c | real-time 3D-TEE, and d | during surgery. Abbreviation: TEE, transesophageal echocardiography.
77bpm
–0.03cm/s
+53.9a
c d
b
Figure 3 | Mitral valve with fibroelastic deficiency. Prolapse and flail owing to ruptured chordae tendineae with related severe mitral regurgitation, as seen by a | 2D-TEE, b | color Doppler TEE, c | real-time 3D-TEE, and d | during surgery. Abbreviation: TEE, transesophageal echocardiography.
a
c d
b
REVIEWS
© 2012 Macmillan Publishers Limited. All rights reserved

136 | MARCH 2012 | VOLUME 9 www.nature.com/nrcardio
Clearly, the choice of strategy should be made according to the specific characteristics of each individual patient. For instance, elderly patients with relevant comorbidities, complex valve lesions, or both might have an operative risk that outweighs the prognostic advantages of correct-ing MR. Under these circumstances, a ‘watchful waiting’ approach with close clinical and echocardiographic follow- up might be appropriate. Clinicians should also take into consideration the results of prospective studies suggest-ing that MV repair might be beneficial in asymptomatic patients with a high likelihood of successful repair and low surgical risk, if these patients present with severe left atrial dilatation (volume index ≥60 ml/m2)29 or flail leaflet with an LV end-systolic dimension ≥40 mm or ≥22 mm/m2.21,30 These findings are likely to be considered in future guide-lines. However, only referral centers with a very high repair rate (>90%) should consider adopting an ‘early repair’ strategy in asymptomatic patients with severe degenerative MR.31–33
Surgical accessesThe options for surgical access in MV repair have changed over time. Although the most-common approach remains a full median sternotomy, less- invasive options, including ministernotomy and right mini thoracotomies, are increas-ingly performed in many expert centers. These methods are technically more demanding and usually require longer cross-clamp times, but have proved to be safe and, compared with full median sternotomy, are associ ated with better cosmetic results, a high degree of patient satis-faction, less postoperative pain, a lower number of blood transfusions, and excellent repair durabi lity.33–35 Totally endoscopic robotic MV repair is used in a small number of high-volume centers, particularly in the USA, but has not been widely adopted, probably because of its high cost and long learning curve. Midterm results of robotic MV repair performed by experienced surgeons are good, but long-term follow-up is necessary.36
Surgical techniques—general remarksPatients with ‘repairable’ MR should be referred to centers with a high level of experience in the field to maximize the likelihood of a successful and durable reconstructive procedure. At the present time, more than
90% of degenerative lesions can be repaired successfully with contemporary techniques in expert centers.31,32,37 Early surgical methods, such as chordal shortening or techniques that do not involve the use of annuloplasty rings, are associated with suboptimal results and have been abandoned.38 New technical solutions have been added to the list of fundamental methods of MV repair first described by Carpentier,15 including the use of arti-ficial chordae39 and the edge-to-edge technique.40 From a technical point of view, valve repair for degenerative MR currently includes a large array of valvular, sub valvular, and annular procedures; the choice between these techniques depends on the type of lesions identified pre operatively and intraoperatively.
Surgical repair of posterior leaflet prolapseIn patients with isolated prolapse of the middle scallop of the posterior leaflet (P2), as encountered in the major-ity of patients with degenerative MR, MV repair usually involves the quadrangular resection of this scallop. Annular plication can be performed at the base of the resected segment, and the remaining portions of the posterior leaflet are then brought together and sutured directly. Published 20-year results of quadrangular resec-tions are excellent, with a freedom from reoperation of 96.9%.41 Annular plication has been replaced in many institutions by other techniques, such as sliding plasty or folding plasty, which are particularly indicated in the presence of redundant leaflet tissue to reduce the risk of systolic anterior motion, a complication that occurs in 5–10% of patients submitted to simple quadrangular resection of the posterior leaflet.42 Folding plasty and sliding plasty decrease the height of the posterior leaflet and move the coaptation point of the MV posteriorly, thereby avoiding the possibility of dynamic obstruction of the LV outflow tract. In patients with posterior leaflet prolapse without redundant leaflet tissue, the most-appropriate surgical solution may be the implantation of artificial chordae (also known as the ‘respect-rather-then-resect’ approach) or a very limited triangular or quadrangular resection.
Surgical repair of anterior leaflet prolapseMV lesions involving the anterior leaflet, or both leaflets, are more difficult to repair and require greater experi-ence than lesions involving only the posterior leaflet. Accordingly, rates of recurrent MR and reoperation are higher after anterior MV repair than after posterior MV repair. Various techniques can be used, the most common of which are briefly discussed here.
Triangular resectionA limited prolapse of the anterior leaflet can be treated easily by triangular resection of the prolapsing segment, followed by direct suture of the remaining leaflet portions. A successful result can be obtained if the resection involves <10% of the total surface of the anterior leaflet. At 5 years, a freedom from reoperation of 93% has been reported by the team from New York University School of Medicine, NY, USA (the center with the largest experience with this
Figure 4 | Barlow disease with calcific degeneration (arrow) involving the posterior leaflet. a | Imaged by real-time 3D transesophageal echocardiography. b | As observed during surgery.
a b
REVIEWS
© 2012 Macmillan Publishers Limited. All rights reserved
NATURE REVIEWS | CARDIOLOGY VOLUME 9 | MARCH 2012 | 137
technique), where results of triangular resection were similar to those of other techniques used for the correction of anterior leaflet prolapse.43
Chordal transfer and chordal transpositionThe detachment of a normal-looking secondary chord and its reattachment to the free margin of the anterior leaflet is known as chordal transfer. By contrast, chordal transposition involves the detachment of a segment of the posterior leaflet (with the corresponding chordae), which is then reattached at the free margin of the prolapsing portion of the anterior leaflet. The defect created on the posterior leaflet by chordal transposition is repaired by a standard quadrangular resection. The main advantage of these approaches is that transferred or transposed chordae usually already have the correct length and, unlike arti-ficial chordae, do not need to be adjusted. With this tech-nique, a 5-year freedom from reoperation after MV repair of 96% has been reported.44
Papillary muscle repositioningPapillary muscle repositioning involves the shortening of the anterior head of the papillary muscle, the chordae tendineae of which are anchored to the anterior leaflet of the MV to correct anterior leaflet prolapse. The fibrous segment of the anterior head is identified, separated from the other papillary muscle heads, and sutured down to the fibrous portion of the posterior head to decrease its height. Dreyfus and co-workers, who introduced this approach, found that papillary muscle repositioning is a safe and durable technique for the management of anterior leaflet prolapse.45
Implantation of artificial chordaeIn degenerative MR, one or more chordae tendineae are often elongated or ruptured. A common way to address this problem is to replace them with artificial chordae made of 4.0 or 5.0 expanded polytetrafluoroethylene (Gore-Tex® Suture, W. L. Gore & Associates, Newark,
DE, USA). The number of artificial chordae that need to be implanted depends on the extension of the pro-lapsing or flailing mitral leaflet segment. Each neo-chorda is sutured to the fibrous portion of the papil lary muscle and to the free margin of the prolapsing portion of the mitral leaflet. The most-challenging part of this technique is choosing the adequate length of the neo-chordae. If the prolapse involves only the anterior leaflet, the reference length to use is the length of the chordae tendineae that reach the nonprolapsing, facing part of the posterior leaflet. Conversely, in the presence of bileaflet prolapse, the point of reference to consider is the anterior commissure, which is usually not affected by chordal elongation. Premeasured artificial chordae were introduced to clinical practice more than 10 years ago as an effective way of dealing with this issue.46 Alternative technical solutions for determining the correct length of artificial chordae have been developed,47–49 but listing the multiple and speci fic details of these strategies is beyond the scope of this Review. Artificial chordae have proved to have optimal biological adaptation and to be effective and safe. In one series, 92% and 85% of patients were free from reoperation and recurrent MR, respectively, after 15 years.50 Similar results, with a freedom from reoperation of 92% and freedom from MR of 88%, have been described by David and co-workers after a shorter follow-up period of 10 years.39
The edge-to-edge techniqueThe original idea behind the edge-to-edge technique was that the competence of a regurgitant MV can be restored effectively with a ‘functional’, rather than an ‘anatomical’ repair.40,51 The key is to identify the location of the regur-gitant jet during the preoperative TEE. At precisely this location, the free edge of one leaflet is sutured to the corres-ponding edge of the opposing leaflet, thereby elimina ting the incompetence of the MV. If the regurgitant jet is located in the center of the valve, edge-to-edge repair produces an MV with a double orifice configuration. If the jet is located
Table 1 | MV lesions differentiated by complexity* and surgical requirements for MV repair
Simple lesions Complex lesions Lesions at high-risk of unsuccessful repair
Type of lesion Posterior leaflet prolapse or flail (isolated mid-scallop involvement [P2], with or without redundant tissue [leaflet height ≥15 mm])Annular dilationLeaflet perforation
Complex posterior leaflet lesionsAnterior prolapse or flailBileaflet prolapse or flailCommissural prolapse or flailCombined lesionsDeviant anatomy
Prolapse and extensive annular calcificationProlapse with hypoplasia of opposite leafletExtreme fibroelastic deficiencyPost-endocarditis extensive destructionRheumatic disease
Probability of successful and durable repair
High Depends on experience of the surgical team
Low
Surgical techniques Quadrangular or triangular resection (including sliding plasty according to leaflet height)AnnuloplastyPatch or direct suture
Artificial chordaeChordal transpositionEdge-to-edge technique
Very technically demanding techniques (including artificial chordae, leaflet enlargement, and annular decalcification)
Necessary expertise of surgical team
Low High Very high
*Judged by echocardiography. Abbreviation: MV, mitral valve.
REVIEWS
© 2012 Macmillan Publishers Limited. All rights reserved

138 | MARCH 2012 | VOLUME 9 www.nature.com/nrcardio
in the proximity of a commissure, the edge-to-edge proce-dure creates a single orifice MV with a smaller area than a normal valve. The technique is attractive because of its sim-plicity, reproducibility, and effectiveness, even in complex settings.52–55 In a series of patients with complex mitral lesions, who underwent edge-to-edge repair, freedom from reoperation at 5 years was 91 ± 4.2% (mean ± stan-dard error); no patient required reoperation for MV ste-nosis.40 Long-term results in specific subsets of patients, such as those with segmental prolapse of the anterior leaflet, have been excellent. Freedom from re operation at a follow-up of 4.50 ± 3.12 years (mean ± standard devia-tion) was 96 ± 2.3% (mean ± standard error) and the echo-cardiographic recurrence rate of severe MR was 2.2%.56 Commissural prolapse57,58 and bileaflet prolapse of facing segments in the context of global myxomatous degen-eration of the MV have also been effectively treated with this approach.59
The edge-to-edge technique is contraindicated in patients with degenerative MR if they have multiple lesions involving segments of the anterior and posterior leaflets that do not face each other, or in patients with a small mitral annulus or rheumatic MR for the risk of inducing stenosis.
Other techniques and associated proceduresAll the previously described surgical techniques should be followed by ring annuloplasty to restore the normal size and geometry of the annulus, to prevent further dilata-tion, and to increase the coaptation surface of the leaflets, which is important for repair durability. In the presence of substantial dilatation of the tricuspid annulus, pro-phylactic tricuspid annuloplasty is becoming increasingly associated with MV repair, even in patients with mild or moderate tricuspid regurgitation, to prevent worsen-ing of tricuspid regurgitation late after MV surgery.60 Surgical ablation of atrial fibrillation is also increasingly performed during MV repair in patients with paroxysm al, persistent, or permanent atrial fibrillation. As a result, sinus rhythm is restored in a substantial number of patients, which improves prognosis.61–63
Evaluating the success of repairTo assess the final result of the repair procedure, valves are inspected visually and a saline test is routinely per-formed. The injection of saline into the left ventricle through the MV allows the evaluation of MV compe-tence. TEE is mandatory after weaning from cardio-pulmonary bypass to confirm perfect competence of the valve. This final assessment of repair should be performed once optimal loading conditions have been reached. If residual regurgitation is more than ‘mild’, the reconstructive procedure should be revised to further improve the competence of the valve before leaving the operating theater.
Results of surgeryIn patients with severe degenerative MR, MV repair rep-resents the optimal surgical treatment, owing to its well-documented advantages over MV replacement in terms
of perioperative mortality, preservation of postoperative LV function, and long-term survival.64,65 Hospital mortal-ity after isolated MV repair in patients with degenerative MR in high-volume centers is less than 1%,66,67 and the rate of major complications is also low (<5%).68 In the study with the longest follow-up of patients after MV repair so far, freedom from cardiac events was 74% after 20 years.41 In other series, at 12-years follow-up, freedom from thromboembolism was 84%, freedom from bleed-ing complications was 94%, and freedom from infective endocarditis was 99%.69 Lifelong anticoagulation therapy is not required after a reconstructive mitral procedure. Therefore, the risk of thromboembolism and bleeding after MV repair is lower than after MV replacement.70 The likelihood of prosthetic valve endocarditis is decreased as well. Whether these advantages of MV repair over MV replacement also apply to elderly patients is contro-versial. Results of a meta-analysis published in 2011, however, showed a clear survival benefit of MV repair compared with MV replacement, even in patients who are older than 80 years, and the authors recommended that MV repair be the preferential treatment for patients with degenerative MR irrespective of a patient’s age.71 We and others share this opinion, even if MV replacement remains an acceptable option when the success of MV repair seems uncertain.72
Long-term survivalLong-term survival and quality of life of patients after MV repair are identical to those of the age-matched general population, provided that surgery is performed before the occurrence of symptoms or LV dysfunction.73,74 By contrast, long-term survival is reduced if MV repair is carried out in patients with symptoms of congestive heart failure, reduced LV ejection fraction, or both.73 Besides the presence of symptoms, the most-important nega-tive predictors of postoperative outcome are advanced age, atrial fibrillation, low preoperative LV function, and pulmonary hypertension.
MV repair failure and reoperationDurability of MV repair is extremely important, particu-larly if a policy of ‘early repair’ is adopted. Severe degenera-tive MR as a result of segmental prolapse of the posterior leaflet can be treated with a very low risk of reoperation. Conversely, the risk of MV repair failure substantially increases in patients with MR resulting from multiple lesions that involve both leaflets or from extensive annular calcification. The failure rate of MV repair, defined by the recurrence of moderate or severe MR, or reopera-tion because of MR, is strictly related to the mechanism of mitral insufficiency, the techniques of repair, and the experience of the center. Most early failures are the result of technical issues, such as residual prolapse, rupture of leaflet tissue, or incorrect annuloplasty, whereas late recur-rence of MR is usually related to the progression of degen-erative valve disease or to infection. The risk of recurrence of moderate or severe MR after repair is 1–2% per year, but is higher in patients with anterior or bileaflet prolapse, which is technically more challenging to treat.17,38 Indeed,
REVIEWS
© 2012 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | CARDIOLOGY VOLUME 9 | MARCH 2012 | 139
the most-durable results have been reported in patients with isolated posterior leaflet prolapse. The surgical techni que usually adopted in this context—quadrangular resection followed by ring annuloplasty—has been associ-ated with a freedom from reoperation of >95% at 10-years follow-up.69,75 In the study with the longest follow-up available in the literature, Braunberger et al. reported a freedom from reoperation of 96.9% for patients with post-erior leaflet prolapse, of 86.2% for patients with isolated anterior leaflet prolapse, and 82.6% for patients with bileaflet prolapse.41 Similarly, David and co-workers reported higher 12-year freedom-from-reoperation in patients with MR owing to posterior leaflet prolapse (96%) than in patients with prolapse involving the ant-erior leaflet (88%) or both leaflets (94%).69 These results clearly demon strate that reoperation rates underscore the incidence of MV-repair failure, since freedom from echocardio graphic moderate or severe MR at 12-years follow-up was 80% for posterior leaflet prolapse, 65% for anterior leaflet prolapse, and 67% for bileaflet prolapse.69
More-recently, however, comparable long-term results have been achieved in patients with posterior, anterior, and bileaflet prolapse.56,76 With continued refinement of strategies for mitral repair, anterior and bileaflet prolapse will probably no longer be considered risk factors for recurrent MR after MV repair in experienced centers. By contrast, in the vast majority of centers with little experi-ence in MV repair, those lesions are still treated mainly with MV replacement, considering that the overall rate of MV repair in patients with MR in the USA in 2005–2007 was only 41%.77
Functional MRFunctional MR often occurs in patients with ischemic or idiopathic dilated cardiomyopathy as a consequence of remodeling of the LV chamber with displacement of the papillary muscles and tethering of the mitral leaflets. The mitral annulus is usually dilated and deformed, whereas the leaflets are morphologically normal.78 Patients with functional MR have a poor prognosis and increasing severity of MR is associated with worse outcome.4,79
Assessment of functional MR Most of the anatomical information is provided by echo-cardiography, which remains the most-frequently used imaging modality for the assessment of functional MR. However, cardiac MRI is progressively emerging as an important diagnostic tool in this setting. Cardiac MRI is not limited by body shape or the inadequacy of (acoustic) windows, and provides a global morphofunctional evalu-ation of the cardiac chambers and, in particular, of the left ventricle. Using cardiac MRI, clinicians can quantify the extension of scar burden in the inferior LV wall, which provides insight into the mechanism of functional MR. For instance, the severity of posterior papillary muscle region scarring correlated with the recurrence of MR after MV repair.80 Therefore, routine quantification of necrosis in the inferior myocardial segments with cardiac MRI might help identifying patients in whom an isolated annuloplasty is unlikely to eliminate functional MR.80
Undersized annuloplastyTechniqueSurgical correction of functional MR in patients with ischemic or nonischemic dilated cardiomyopathy is mainly performed by means of an undersized (or ‘restrictive’) annuloplasty. This technique consists of the implantation of an annuloplasty ring that is at least two sizes smaller than an annuloplasty ring that would have been chosen on the basis of measuring the intertrigonal distance and the surface of the anterior leaflet as a refer-ence. By substantially reducing the annular dimension, restrictive annuloplasty forces coaptation of the leaflets and thereby eliminates regurgitation.81–83 Complete and rigid annulo plasty rings are more effective than partial and flexible rings,84,85 and a leaflet coaptation length of at least 8 mm should be obtained at the end of the procedure to ensure a durable repair.86,87
Coaptationlength
0 23 180
Box 1 | Predictors of MR after restrictive annuloplasty*
■ Mild annular dilatation
■ Complex multiple regurgitant jets137
■ Advanced LV remodeling138
■ Excessive tethering (coaptation depth >1.5 cm)
■ Posterior mitral leaflet angle >45°139
■ Distal anterior mitral leaflet angle >25°140
■ Systolic tenting area >2.5 cm2
■ Endsystolic interpapillary muscle distance >20 mm
■ Systolic specificity index >0.7141
*These preoperative predicitors of residual or recurrent functional MR are according to the authors’ own clinical experience, unless otherwise stated. Abbreviations: LV, left ventricular; MR, mitral regurgitation.
Figure 5 | Echocardiographic parameters in functional mitral regurgitation. The coaptation depth (solid line) is the distance between the annular plane of the mitral valve and the coaptation point of the leaflets. The tenting area (dotted lines) is the area enclosed by the mitral leaflets and the annular plane. Coaptation length is the length of apposition of the mitral leaflets, whereas the tethering angle describes the angle between the annular plane and the basal portion of the anterior or posterior leaflet.
REVIEWS
© 2012 Macmillan Publishers Limited. All rights reserved
140 | MARCH 2012 | VOLUME 9 www.nature.com/nrcardio
Outcomes and patient selectionRestrictive annuloplasty is simple and reproducible. The procedure has a low operative mortality and can improve patient symptoms and quality of life.82,83,87 Reverse LV remodeling has been described in many patients late after surgery.86,87 Although no randomized trial has been performed, observational studies have not shown a long-term survival benefit for patients with functional MR and severe LV dysfunction who undergo MV repair by annulo plasty compared with those receiv-ing only pharmaco logical therapy.88 Residual or recur-rent MR after restrictive annulo plasty still occurs in a considerable number of patients (20% after 3–5 years), enhancing the frequency of heart-failure episodes and increasing mortality.89,90
In our opinion, patient selection is extremely important to prevent the recurrence of MR. In particular, the pres-ence of clinical and echocardiographic predictors of post-operative residual or recurrent MR (Box 1, Figure 5)90–95 should be taken into consideration when selecting patients for restrictive annuloplasty, together with the clinical history and the severity of the LV remodeling process. Indeed, the best outcome after restrictive annuloplasty was
obtained in patients with a short duration of heart-failure symptoms and a small preoperative LV size.86 Therefore, an isolated restrictive annuloplasty only seems to represent a good solution in patients with a short history of heart failure if the left ventricle is not excessively dilated, and the well-defined echocardiographic predictors of MR recur-rence after MV repair are absent. Importantly, in patients with functional MR and no indication for myocardial revascularization, correction of MR is not recommended by current guidelines.7,8
Under certain circumstances, restrictive annuloplasty is combined with other surgical techniques to improve the durability of repair. Resection of the secondary chordae attached to the anterior leaflet,96 repositioning of the papil lary muscle,97–99 the addition of the edge-to-edge suture,100 the use of external cardiac support,101 and a con-comitant LV restoration procedure102 have all increased the effectiveness of restrictive annuloplasty in specific patient groups.
MV repair versus MV replacementWhenever the likelihood of a durable repair by annulo-plasty is low, we recommend MV replacement with a
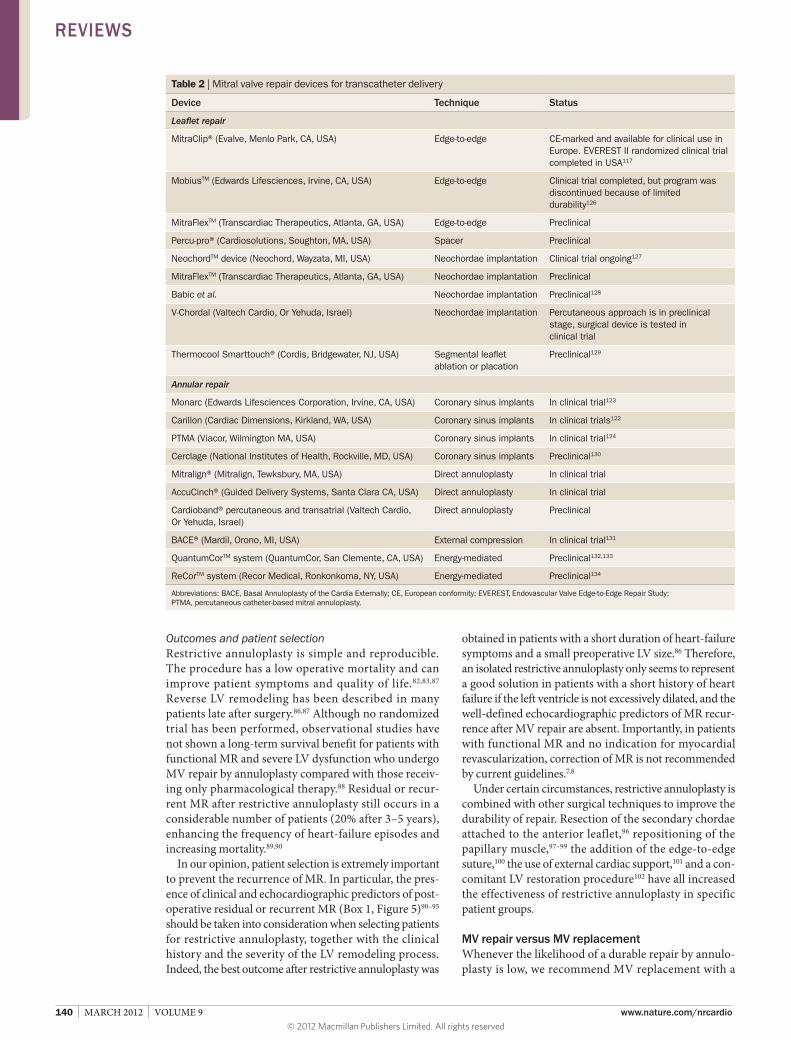
Table 2 | Mitral valve repair devices for transcatheter delivery
Device Technique Status
Leaflet repair
MitraClip® (Evalve, Menlo Park, CA, USA) Edge-to-edge CE-marked and available for clinical use in Europe. EVEREST II randomized clinical trial completed in USA117
MobiusTM (Edwards Lifesciences, Irvine, CA, USA) Edge-to-edge Clinical trial completed, but program was discontinued because of limited durability126
MitraFlexTM (Transcardiac Therapeutics, Atlanta, GA, USA) Edge-to-edge Preclinical
Percu-pro® (Cardiosolutions, Soughton, MA, USA) Spacer Preclinical
NeochordTM device (Neochord, Wayzata, MI, USA) Neochordae implantation Clinical trial ongoing127
MitraFlexTM (Transcardiac Therapeutics, Atlanta, GA, USA) Neochordae implantation Preclinical
Babic et al. Neochordae implantation Preclinical128
V-Chordal (Valtech Cardio, Or Yehuda, Israel) Neochordae implantation Percutaneous approach is in preclinical stage, surgical device is tested in clinical trial
Thermocool Smarttouch® (Cordis, Bridgewater, NJ, USA) Segmental leaflet ablation or placation
Preclinical129
Annular repair
Monarc (Edwards Lifesciences Corporation, Irvine, CA, USA) Coronary sinus implants In clinical trial123
Carillon (Cardiac Dimensions, Kirkland, WA, USA) Coronary sinus implants In clinical trials122
PTMA (Viacor, Wilmington MA, USA) Coronary sinus implants In clinical trial124
Cerclage (National Institutes of Health, Rockville, MD, USA) Coronary sinus implants Preclinical130
Mitralign® (Mitralign, Tewksbury, MA, USA) Direct annuloplasty In clinical trial
AccuCinch® (Guided Delivery Systems, Santa Clara CA, USA) Direct annuloplasty In clinical trial
Cardioband® percutaneous and transatrial (Valtech Cardio, Or Yehuda, Israel)
Direct annuloplasty Preclinical
BACE® (Mardil, Orono, MI, USA) External compression In clinical trial131
QuantumCorTM system (QuantumCor, San Clemente, CA, USA) Energy-mediated Preclinical132,133
ReCorTM system (Recor Medical, Ronkonkoma, NY, USA) Energy-mediated Preclinical134
Abbreviations: BACE, Basal Annuloplasty of the Cardia Externally; CE, European conformity; EVEREST, Endovascular Valve Edge-to-Edge Repair Study; PTMA, percutaneous catheter-based mitral annuloplasty.
REVIEWS
© 2012 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | CARDIOLOGY VOLUME 9 | MARCH 2012 | 141
bioprosthesis, with complete preservation of the sub-valvular apparatus. Although data from a meta-analysis of retrospective studies indicated better short-term and long-term survival after MV repair than after MV replacement,103 results of a randomized trial compar-ing the two procedures have not been published to date, and some data show that survival of high-risk patients is similar after MV repair and MV replacement.104
Despite these uncertainties, surgical correction of functional MR still remains a widely performed pro-cedure,105,106 mainly because of the postoperative improvement in symptoms and quality of life. These improvements represent a major advantage for patients who experience repeated hospital admissions for congestive heart failure despite maximal pharmaco-therapy.83,86,87,100 Obviously, the potential benefit of the operation has to be carefully weighed against the surgi-cal risk. In our opinion, heavy comorbidities, severe right ventricular dysfunction, and severe LV dysfunction without contractile reserve under dobutamine infusion during echocardiography are absolute contraindications to surgery.
Role of transcatheter methodsResults of the Euro Heart Survey showed that up to 50% of symptomatic patients hospitalized with severe MR are not referred for surgery.107 As these patients are usually elderly (70–75 years) and have comorbidities as well as depressed LV function, the risk of surgery is considered too high. Minimally invasiveness transcatheter techniques for MV repair and MV replacement are emerging as an alternative for high-risk and inoperable surgical candi-dates with functional or degenerative MR. Most percuta-neous MV repair technologies involve the implanta tion of a device. In a few cases, the clinical effect is achieved by delivering some form of energy to the target lesion. Moreover, the ‘revalving’ of a previously implanted bio-prosthesis or an annular device in the mitral position is possible using a valve-in-valve108–110 or valve-in-ring 111 percutaneous intervention.
Most transcatheter devices are delivered through a venous approach and via trans-septal puncture, whereas valve-in-valve implants are usually performed with a transapical or transatrial hybrid solution, which offers the benefit of a more-direct approach to the MV. For some direct annuloplasty devices, a retrograde approach from the arterial root is used. Several devices have been designed to treat MR at the leaflet level but the most-common approach is the creation of a double orifice valve using the simple and versatile Alfieri technique. Transcatheter devices for MV repair can be classi-fied according to repair techniques (Table 2). Several transcatheter devices for MV replacement are under development (Table 3).
Imaging during transcatheter proceduresImaging has a major role in percutaneous MV proce-dures. Whereas most transcatheter procedures target-ing the aortic valve can be carried out effectively under guidance by fluoroscopy, mitral interventions
require RT 3D-navigation. During percutaneous MV procedures, devices are usually guided by 2D and 3D-echocardiography,109,112,113 but other technologies, including intracardiac echocardiography and image fusion, could possibly increase the success of implantation.114
Guidance of transcatheter MV procedures by Doppler echocardiography has a potential advantage over surgery in that therapy is not only guided by the anatomy of lesions, but also by the hemodynamic dysfunction. Furthermore, the functional outcome is optimized under physiological conditions (that is, on the beating heart), guided by the hemodynamic effect of the therapeutic intervention. These advantages could increase efficacy of repair, parti cularly in patients with functional MR in whom lesions are dynamic and anatomical landmarks are rarely found during open-heart surgery. To over-come this limitation of MV surgery, novel hybrid surgi-cal devices that enable physiological tuning of surgically implanted devices, such as the adjustment of neo chordae after surgical implantation on the beating heart, are under development.115
The MitraClip®Procedure and outcomesThe MitraClip® (Evalve, Menlo Park, CA, USA) MV repair system is currently the only percutaneous device that is available for clinical use in Europe. The procedure involves the implantation of one or more clips at the site of regurgita tion using a sophisticated triaxial delivery system that is introduced into the femoral vein and posi-tioned trans-septally into the left atrium. The procedure is guided by fluoroscopy and TEE (Figure 6). The MitraClip® is fully repositionable and retrievable until detached from the delivery system, so that the operator can implant it at an ideal location, taking into account the specific anatomy of the patient. The first implantation was performed in 2003 in a patient with anterior leaflet prolapse; sustained clinical benefit and mild residual MR were demonstrated 2 years after the procedure.116 In the unblinded, prospec-tive, multi center (n = 37), randomized Endovascular Valve Edge-to-Edge Repair Study (EVEREST) II, 279 surgi cally operable patients with significant MR (grade 3+ or 4+) and suitable valve anatomy were randomly assigned in a 2:1 ratio to the MitraClip® procedure (device group; 184 patients enrolled, 178 treated) or MV surgery (control group; 95 patients enrolled, 80 treated).117 Patients were considered anatomically suitable if the target lesion was confined to the central portion of the leaflets (A2–P2). The objective of EVEREST II was to evaluate safety and effectiveness of the MitraClip® system compared with
Table 3 | Mitral valve replacement devices for transcatheter delivery
Device Approach Status
Endovalve® (Endovalve, Princeton, NJ, USA) Minithoracotomy Preclinical
‘Lutter prostheses’ Transapical Preclinical135,136
CardiaQTM system (CardiaQ Valve Technologies, Irvine, CA, USA)
Trans-septal Preclinical
Cardiovalve® (Valtech Cardio, Or Yehuda, Israel) Trans-septal Preclinical
REVIEWS
© 2012 Macmillan Publishers Limited. All rights reserved

142 | MARCH 2012 | VOLUME 9 www.nature.com/nrcardio
conventional MV surgery. Patients with rheumatic disease, active endocarditis, or with a baseline valve area <4 cm2 were excluded. For patients with degenerative lesions (type II Carpentier classification15) the prolapsing or flail lesions should show a flail gap <10 mm (measured as the distance between the free edge of the prolapsing segment and the co apting edge of the facing leaflet) and a flail width <15 mm (the intercommissural extension of the prolapse or flail). For patients with functional disease, the coaptation depth was <11 mm and the coaptation length >2 mm. Most of these criteria are reflected in current guidelines7,8 and recommendations of the manu-facturer, although several patients with anatomical charac-teristics beyond the classical EVEREST criteria have been treated successfully.118
The trial has been much debated both in terms of its design and the interpretation of its results. EVEREST II suffered from the early learning curve of a rather dif-ficult procedure, the results of which might improve with increasing experience of the operating surgeon. Moreover, some have emphasized that most of the data were collected from centers performing a fairly small number of MitraClip® implantations. In addition, the value of the results is diminished by the small number of enrolled patients with functional MR and by the fact that only operable patients were included. By contrast, most of those currently undergoing MitraClip® implanta-tion are either high-risk or inoperable patients with functional MR.
Long-term outcomes of patients who underwent this procedure are still unavailable, but several registries are collecting such invaluable information. In Europe, the ACCESS registry holds data from patients undergoing the procedure in specialist centers.119 In the USA, a regis-try of patients who were excluded from the EVEREST II trial, owing to high-risk conditions, and the Real World Expanded Multicenter Study of the MitraClip® System (REALISM) registry (a continued access regis-try of EVEREST II) exist. Early data indicate that the MitraClip® procedure can be carried out effectively and with a reasonably low risk compared with surgery, even in high-risk patients with a complex anatomy (outside the ideal characteristics defined in EVEREST II).118,120
The results of MitraClip® implantation might be improved if the technique is combined with some form of annuloplasty. Although the edge-to-edge procedure alone can lead to durable results in selected patients with functional MR (for example, in patients without substan-tial annular dilation),118 the addition of an annuloplasty increases repair durability in most patients.40
Recommendations for MitraClip® useData from EVEREST II, the registries, and from the European clinical experience provide the basis for some recommendations. The implantation of a MitraClip® is a fairly safe procedure that is tolerated well, even by patients with severe LV dysfunction, comorbid ities, and poor general health. The feasibility of the procedure is evaluated on the basis of specific echocardio graphic cri-teria, which then determine the eligibility of the patient. Compared with MV surgery, MitraClip® implantation is less effective in eliminating MR and is associated with a higher rate of residual or recurrent mitral insufficiency. Nevertheless, the MitraClip® reduces the severity of MR in most patients, which can be benefi cial in very sick patients with severe MR and serious comorbidities, who have a high surgical risk. In addition to reducing MR, MitraClip® implantation also decreases LV dimensions over time117 and substantially improves cardiac output and LV loading conditions.121 If MitraClip® implanta-tion fails, surgical MV repair can still be performed in some patients.117 In many circumstances, however, valve replacement is the only therapeutic option after unsuc-cessful MitraClip® implantation. At present, the typical candidate for a MitraClip® is a symptomatic patient with severe degenerative or functional MR, who is considered inoperable or has a high surgical risk, fulfills the echo-cardiographic criteria of eligibility, and has a life expec-tancy of at least 1 year. Conversely, patients who can be offered MV surgery with an acceptable risk should not be considered for the MitraClip® procedure.
Other annuloplasty devicesSeveral new annular devices are under development. Initially, most research efforts were devoted to the develop ment of coronary sinus implants with the premise
Figure 6 | MitraClip® (Evalve, Menlo Park, CA, USA) implantation. The implantation of the a | MitraClip® is guided by b | real-time 3D transesophageal echocardiography. Permission for panel a obtained from Abbott Laboratories © 2011.
a b
REVIEWS
© 2012 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | CARDIOLOGY VOLUME 9 | MARCH 2012 | 143
that such devices would be easy to implant and effective owing to the close vicinity of the mitral annulus. The Carillon Mitral Countour System® (Cardiac Dimensions, Kirkland, WA, USA),122 the Monarc® (Edwards Lifesciences Corporation, Irvine, CA, USA) annulo-plasty system,123 and the PTMA® (Viacor, Wilmington MA, USA) device124 have been tested in clinical trials, but showed suboptimal results in terms of rate of successful implantations and incidence of complications.
The clinical application of coronary sinus devices is limited by anatomical restrictions. For example, the circum flex artery crosses the coronary sinus in up to 50% of patients, and the distance between the coronary sinus and the annular plane is very variable.125 As a result, the implantation of coronary sinus devices increases the risk of acute and chronic ischemic events owing to coronary compression, and the efficacy of the procedure is low if the annulus cannot be remodeled efficiently.
Direct annuloplasty methods are being investigated in an effort to better replicate surgical annuloplasty. The Mitralign® percutaneous annuloplasty system (Mitralign, Tewksbury, MA, USA) adopts a retrograde approach to the annulus via the femoral artery. Once the delivery system is positioned in the left ventricle, two or more anchor pairs are deployed across the annulus from the ventricular to the atrial side. The anchors are tethered and then put into tension to achieve selective plications of the annulus in a similar way to the surgical Key proce-dure. The AccuCinch® device (Guided Delivery Systems, Santa Clara CA, USA) is designed for the implantation of a series of anchors in the subannular region of the base of the left ventricle, using an arterial retrograde approach from the aortic valve. The anchors are con-nected by a cable that can be tethered under echocardio-graphic guidance until the intended amount of annular cinching is obtained. A third direct annuloplasty solu-tion under development is the Cardioband® device (Valtech Cardio, Or Yehuda, Israel), which is implanted antegradely, adopting a standard transeptal approach. It delivers a Dacron band (which is similar to a surgical annuloplasty band and can be adjusted in length) into the left atrium, where the band is implanted into the annular tissue using proprietary anchors. This sophisti cated tri-axial delivery system is guided by echocardiography. Following implantation, the Dacron band is shortened until the desired annular reduction is obtained. Other technologies for percutaneous annular remodeling include external compression devices, and remodeling using radiofrequency or other forms of energy to shrink collagen (Table 2).
Transcatheter-based MV replacementSeveral devices for the percutaneous implantation of an MV prosthesis are under development. Compared with transcatheter aortic valve implantation, a mitral implant is more challenging. For example, because of the more-complex and nontubular anatomy of the mitral annulus, the mitral device must be larger than an aortic device and its fixation using radial force would not be effec-tive and could cause serious adverse effects. In addition, whereas perivalvular leakage is considered an acceptable complica tion of transcatheter aortic valve implantation, leaks in the mitral position would be intolerable because of higher pressure gradients. The ideal MV prosthesis would be implanted without radial force to avoid obstruc-tion of LV outflow, without impingement into the aortic root, and no (or only minimal) perivalvular leakage. Moreover, the valve would be delivered percutaneously and be durable (depending on the age of the patient). If all these challenges are overcome, percutaneous MV replacement could become a valid alternative to surgical MV implantation and to percutaneous MV repair.
ConclusionsSurgical MV repair is the treatment of choice for patients with severe degenerative MR. If the procedure is carried out in a timely and effective manner at centers with high expertise in the field, the operative risk is low and life expectancy of patients is similar to that of the general population. In patients with MR secondary to dilated cardio myopathy, mitral repair is more challenging and the careful selection of patients is mandatory to minimize the risk of unfavorable outcomes. Restrictive annuloplasty alone should be carried out only in the early stages of the disease and in patients without echocardiographic predictors of postoperative residual or recurrent MR. Otherwise, MV replacement is preferrable. Transcatheter correction of MR regurgitation, either through MV repair or MV replacement, represents a new and emerging field of cardiovascular medicine and is expected to have a substantial impact on surgical practice in the future.
1. Nkomo, V. T. et al. Burden of valvular heart diseases: a population-based study. Lancet 368, 1005–1011 (2006).
2. Iung, B. & Vahanian A. Epidemiology of valvular heart disease in the adult. Nat. Rev. Cardiol. 8, 162–172 (2011).
3. Bursi, F. et al. Heart failure and death after myocardial infarction in the community: the emerging role of mitral regurgitation. Circulation 111, 295–301 (2005).
4. Grigioni, F., Enriquez-Sarano, M., Zehr, K. J., Bailey, K. R. & Tajik, A. J. Ischemic mitral regurgitation: long-term outcome and prognostic implications with quantitative Doppler assessment. Circulation 103, 1759–1764 (2001).
5. Ling, L. H. et al. Clinical outcome of mitral regurgitation due to flail leaflet. N. Engl. J. Med. 335, 1417–1423 (1996).
6. Detaint, D. et al. Surgical correction of mitral regurgitation in the elderly: outcomes and recent
improvements. Circulation 114, 265–272 (2006).
7. Bonow, R. O. et al. 2008 focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to revise the 1998 guidelines for the management of patients with valvular heart
Review criteria
The PubMed database was searched for articles to be included in this Review using the terms “mitral regurgitation”, “degenerative mitral disease”, and “functional mitral regurgitation” combined with “mitral repair”, “treatment”, and “management”. We selected mainly full-text, original articles that were written in English and published between 1990 and 2010, and also searched the reference lists of these papers for further leads.
REVIEWS
© 2012 Macmillan Publishers Limited. All rights reserved
144 | MARCH 2012 | VOLUME 9 www.nature.com/nrcardio
disease). Endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J. Am. Coll. Cardiol. 52, e1–e142 (2008).
8. Vahanian, A. et al. Guidelines on the management of valvular heart disease: The Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology. Eur. Heart J. 28, 230–268 (2007).
9. Iung, B. et al. A prospective survey of patients with valvular heart disease in Europe: The Euro Heart Survey on Valvular Heart Disease. Eur. Heart J. 24, 1231–1243 (2003).
10. Monin, J. L. et al. Functional assessment of mitral regurgitation by transthoracic echocardiography using standardized imaging planes. J. Am. Coll. Cardiol. 46, 302–309 (2005).
11. Foster, G. P. et al. Accurate localization of mitral regurgitant defects using multiplane transesophageal echocardiography. Ann. Thorac. Surg. 65, 1025–1031 (1998).
12. Grewal, J. et al. Real-time three-dimensional transesophageal echocardiography assessment of mitral valve disease. J. Am. Soc. Echocardiography 22, 34–41 (2009).
13. La Canna, G. et al. Real-time three-dimensional transesophageal echocardiography for assessment of mitral valve functional anatomy in patients with prolapse-related regurgitation. Am. J. Cardiol. 107, 1365–1374 (2011).
14. Levine, R. A. et al. Three-dimensional echocardiographic reconstruction of the mitral valve, with implications for the diagnosis of mitral valve prolapse. Circulation 80, 589–598 (1989).
15. Carpentier, A. Cardiac valve surgery—the “French correction”. J. Thorac. Cardiovasc. Surg. 86, 323–337 (1983).
16. Kumar, N., Kumar, M. & Duran C. M. A revised terminology for recording surgical findings of the mitral valve. J. Heart Valve Dis. 4, 70–75 (1995).
17. Flameng, W., Meuris, B., Herijgers, P. & Herregods, M. C. Durability of mitral repair in Barlow disease versus fibroelastic deficiency. J. Thorac. Cardiovasc. Surg. 135, 274–282 (2008).
18. Enriquez-Sarano, M. et al. Quantitative determinants of the outcome of asymptomatic mitral regurgitation. N. Engl. J. Med. 352, 875–883 (2005).
19. Barbieri, A. et al. Prognostic and therapeutic implications of pulmonary hypertension complicating degenerative mitral regurgitation due to flail leaflet: a multicenter long-term international study. Eur. Heart J. 32, 751–759 (2011).
20. Messika-Zeitoun, D. et al. Left atrial remodelling in mitral regurgitation—methodologic approach, physiological determinants, and outcome implications: a prospective quantitative Doppler-echocardiographic and electron beam-computed tomographic study. Eur. Heart J. 28, 1773–1781 (2007).
21. Tribouilloy, C. et al. Survival implication of left ventricular end-systolic diameter in mitral regurgitation due to flail leaflets. J. Am. Coll. Cardiol. 54, 1961–1968 (2009).
22. Pizarro, R. et al. Prospective validation of the prognostic usefulness of brain natriuretic peptide in asymptomatic patients with chronic severe mitral regurgitation. J. Am. Coll. Cardiol. 54, 1099–1106 (2009).
23. Messika Zeitoun, D. et al. Cardiopulmonary exercise testing determination of functional capacity in mitral regurgitation: physiologic and outcome implications. J. Am. Coll. Cardiol. 47, 2521–2527 (2006).
24. Lancellotti, P. et al. Importance of left ventricular longitudinal function and functional reserve in patients with degenerative mitral regurgitation: assessment by 2-D speckle tracking. J. Am. Soc. Echocardiogr. 21, 1331–1336 (2008).
25. Magne, J., Lancellotti, P. & Piérard, L. A. Exercise pulmonary hypertension in asymptomatic degenerative mitral regurgitation. Circulation 122, 33–41 (2010).
26. Magne, J., Lancellotti, P. & Piérard, L. A. Exercise-induced changes in degenerative mitral regurgitation. J. Am. Coll. Cardiol. 56, 310–313 (2010).
27. Montant, P. et al. Long-term survival in asymptomatic patients with severe degenerative mitral regurgitation: a propensity score-based comparison between an early surgical strategy and a conservative treatment approach. J. Thorac. Cardiovasc. Surg. 138, 1339–1348 (2009).
28. Rosenhek, R. et al. Outcome of watchful waiting in asymptomatic severe mitral regurgitation. Circulation 113, 2238–2244 (2006).
29. Le Tourneau, T. et al. Impact of left atrial volume on clinical outcome in organic mitral regurgitation. J. Am. Coll. Cardiol. 56, 570–578 (2010).
30. Grigioni, F. et al. Outcomes in mitral regurgitation to flail leaflets: a multicenter European study. JACC Cardiovasc. Imaging 1, 133–141 (2008).
31. Gillinov, A. M. et al. Valve repair versus valve replacement for degenerative mitral valve disease. J. Thorac. Cardiovasc. Surg. 135, 885–893 (2008).
32. Adams, D. H. et al. Large annuloplasty rings facilitate mitral valve repair in Barlow’s disease. Ann. Thorac. Surg. 82, 2096–2100 (2006).
33. Gammie, J. S., Bartlett, S. T. & Griffith, B. P. Small-incision mitral valve repair: safe, durable, and approaching perfection. Ann. Surg. 250, 409–415 (2009).
34. Holzhey, D. M. et al. Minimally invasive versus sternotomy approach for mitral valve surgery in patients greater than 70 years old: a propensity-matched comparison. Ann. Thorac. Surg. 91, 401–405 (2011).
35. Casselman, F. P. et al. Endoscopic mitral valve repair: feasible, reproducible, and durable. J. Thorac. Cardiovasc. Surg. 125, 273–282 (2003).
36. Chitwood, W. R. et al. Robotic mitral valve repairs in 300 patients: a single-center experience. J. Thorac. Cardiovasc. Surg. 136, 436–441 (2008).
37. Gammie, J. S., Bartlett, S. T. & Griffith, B. P. Small-incision mitral valve repair: safe, durable, and approaching perfection. Ann. Surg. 250, 409–415 (2009).
38. Flameng, W., Herijjers, P. & Bogaerts, K. Recurrence of mitral valve regurgitation after mitral valve repair in degenerative valve disease. Circulation 107, 1609–1613 (2003).
39. David, T. E. Artificial chordae. Semin. Thorac. Cardiovasc. Surg. 16, 161–168 (2004).
40. Alfieri, O. et al. The double-orifice technique in mitral valve repair: a simple solution for complex problems. J. Thorac. Cardiovasc. Surg. 122, 674–681 (2001).
41. Braunberger, E. et al. Very long-term results (more than 20 years) of valve repair with Carpentier’s techniques in nonrheumatic mitral valve insufficiency. Circulation 104 (Suppl. 1), I8–I11 (2001).
42. Crescenzi, G. et al. Management and decision-making strategy for systolic anterior motion after mitral valve repair. J. Thorac. Cardiovasc. Surg. 137, 320–325 (2009).
43. Saunders, P. C. et al. Anterior leaflet resection of the mitral valve. Semin. Thorac. Cardiovasc. Surg. 16, 188–193 (2004).
44. Gillinov, A. M. & Cosgrove, D. M. Chordal transfer for repair of anterior leaflet prolapse. Semin. Thorac. Cardiovasc. Surg. 16, 169–173 (2004).
45. Dreyfus, G. D., Souza Neto, O. & Aubert, S. Papillary muscle repositioning for repair of anterior leaflet prolapse caused by chordal elongation. J. Thorac. Cardiovasc. Surg. 132, 578–584 (2006).
46. von Oppell, U. O. & Mohr, F. W. Chordal replacement for both minimally invasive and conventional mitral valve surgery using premeasured Gore-Tex loops. Ann. Thorac. Surg. 70, 2166–2168 (2000).
47. Zussa, C. Different applications of ePTFE valve chordae: surgical technique. J. Heart Valve Dis. 5, 356–361 (1996).
48. David, T. E., Armstrong, S. & Sun, Z. Replacement of chordae tendineae with Gore-Tex sutures: a ten-year experience. J. Heart Valve Dis. 5, 352–355 (1996).
49. Chan, D. T., Chiu. C. S., Cheng, L. C. & Au, T. W. Artificial chordae: a simple clip and tie technique. J. Thorac. Cardiovasc. Surg. 136, 1597–1599 (2008).
50. Salvador, L. et al. A 20-year experience with mitral valve repair with artificial chordae in 608 patients. J. Thorac. Cardiovasc. Surg. 135, 1280–1287 (2008).
51. Fucci, C. et al. Improved results with mitral valve repair using new surgical techniques. Eur. J. Cardiothorac. Surg. 9, 621–626 (1995).
52. Kuduvalli, M. et al. Edge-to-edge technique for mitral valve repair: medium-term results with echocardiographic follow-up. Ann. Thorac. Surg. 82, 1356–1361 (2006).
53. Brinster, D. R. et al. Midterm results of the edge-to-edge technique for complex mitral valve repair. Ann. Thorac. Surg. 81, 1612–1617 (2006).
54. Bhudia, S. K. et al. Edge-to-edge (Alfieri) mitral repair: results in diverse clinical settings. Ann. Thorac. Surg. 77, 1598–1606 (2004).
55. Kherani, A. R. et al. Edge-to-edge mitral valve repair: the Columbia Presbyterian experience. Ann. Thorac. Surg. 78, 73–76 (2004).
56. De Bonis, M. et al. Similar long-term results of mitral valve repair for anterior compared with posterior leaflet prolapse. J. Thorac. Cardiovasc. Surg. 131, 364–368 (2006).
57. Gillinov, A. M., Shortt, K. G. & Cosgrove D. M. 3rd. Commissural closure for repair of mitral commissural prolapse. Ann. Thorac. Surg. 80, 1135–1136 (2005).
58. Lapenna, E. et al. Commissural closure for the treatment of commissural mitral valve prolapse or flail. J. Heart Valve Dis. 17, 261–266 (2008).
59. Maisano, F. et al. The double-orifice technique as a standardized approach to treat mitral regurgitation due to severe myxomatous disease: surgical technique. Eur. J. Cardiothorac. Surg. 17, 201–205 (2000).
60. Dreyfus, G., Corbi, P. J., Chan, K. M. & Bahrami, T. Secondary tricuspid regurgitation or dilatation: which should be the criteria for surgical repair? Ann. Thorac. Surg. 79, 127–132(2005).
61. Schaff, H. V., Dearani, J. A., Daly, R. C, Orszulak, T. A. & Danielson, G. K. Cox–maze procedure for atrial fibrillation: Mayo Clinic experience. Semin. Thorac. Cardiovasc. Surg. 12, 30–37 (2000).
62. Raanani, E., Albage, A., David, T. E., Yau, T. M. & Armstrong S. The efficacy of the Cox/maze procedure combined with mitral valve surgery: a matched control study. Eur. J. Cardiothorac. Surg. 19, 438–442 (2001).
REVIEWS
© 2012 Macmillan Publishers Limited. All rights reserved
NATURE REVIEWS | CARDIOLOGY VOLUME 9 | MARCH 2012 | 145
63. Cox, J. L. Intraoperative options for treating atrial fibrillation associated with mitral valve disease. J. Thorac. Cardiovasc. Surg. 122, 212–215 (2001).
64. Yun, K. L. & Miller, D. C. Mitral valve repair versus replacement. Cardiol. Clin. 9, 315–327 (1991).
65. Olson, L. J. et al. Surgical pathology of the mitral valve: a study of 712 cases spanning 21 years. Mayo Clin. Proc. 62, 22–34 (1987).
66. Gammie, J. S. et al. Influence of hospital procedural volume on care process and mortality for patients undergoing elective surgery for mitral regurgitation. Circulation 115, 881–887 (2007).
67. Gillinov, A. M. et al. Should patients with severe degenerative mitral regurgitation delay surgery until symptoms develop? Ann. Thorac. Surg. 90, 481–488 (2010).
68. Savage, E. B., Ferguson, T. B. Jr &. DiSesa, V. J. Use of mitral valve repair: analysis of contemporary United States experience reported to the Society of Thoracic Surgeons National Cardiac Database. Ann. Thorac. Surg. 75, 820–825 (2003).
69. David, T. E., Ivanov, J, Armstrong, S., Christie, D. & Rakowski H. A comparison of outcomes of mitral valve repair for degenerative disease with posterior, anterior, and bileaflet prolapse. J. Thorac. Cardiovasc. Surg. 130, 1242–1249 (2005).
70. Russo, A. et al. Thromboembolic complications after surgical correction of mitral regurgitation incidence, predictors, and clinical implications. J. Am. Coll. Cardiol. 51, 1203–1211 (2008).
71. Markar, S. R., Sadat, U., Edmonds, L. & Nair S. K. Mitral valve repair versus replacement in the elderly population. J. Heart Valve Dis. 20, 265–271 (2011).
72. Nloga, J. et al. Mitral valve surgery in octogenarians: should we fight for repair? A survival and quality-of-life assessment. Eur. J. Cardiothorac. Surg. 39, 875–880 (2011).
73. Enriquez-Sarano, M. et al. Echocardiographic prediction of survival after surgical correction of organic mitral regurgitation. Circulation 90, 830–837 (1994).
74. Heikkinen, J. et al. Quality of life after mitral valve repair. J. Heart Valve Dis. 14, 722–726 (2005).
75. Gillinov, A. M. et al. Durability of mitral valve repair for degenerative disease. J. Thorac. Cardiovasc. Surg. 111, 734–743 (1998).
76. Suri, R. M. et al. Survival advantage and improved durability of mitral repair for leaflet prolapse subsets in the current era. Ann. Thorac. Surg. 82, 819–826 (2006).
77. Bolling, S. F. et al. Predictors of mitral valve repair: clinical and surgeon factors. Ann. Thorac. Surg. 90, 1904–1911 (2010).
78. Hueb, A. C. et al. Ventricular remodeling and mitral valve modifications in dilated cardiomyopathy: new insights from anatomic study. J. Thorac. Cardiovasc. Surg. 124, 1216–1224 (2002).
79. Flynn, M. et al. Regional wall motion abnormalities and scarring in severe functional ischemic mitral regurgitation: a pilot cardiovascular magnetic resonance imaging study. J. Thorac. Cardiovasc. Surg. 137, 1063–1070 (2009).
80. Lancellotti, P., Gérard, P. & Piérard, L. Long term outcome of patients with heart failure and dynamic mitral regurgitation. Eur. Heart J. 26, 1528–1532 (2005).
81. Bolling, S. F. et al. Early outcome of mitral valve reconstruction in patients with end-stage cardiomyopathy. J. Thorac. Cardiovasc. Surg. 109, 676–682 (1995).
82. Bolling, S. F. et al. Intermediate-term outcome of mitral reconstruction in cardiomyopathy. J. Thorac. Cardiovasc. Surg. 115, 381–386 (1998).
83. Bach, D. & Bolling, S. Early improvement in congestive heart failure after correction of secondary mitral regurgitation in end-stage cardiomyopathy. Am. Heart J. 129, 1165–1170 (1995).
84. Silberman, S. et al. Repair of ischemic mitral regurgitation: comparison between flexible and rigid annuloplasty rings. Ann. Thorac. Surg. 87, 1721–1726 (2009).
85. Spoor, M. T., Geltz, A. & Bolling, S. F. Flexible versus nonflexible mitral valve rings for congestive heart failure: differential durability of repair. Circulation 114 (Suppl. 1), I67–I71 (2006).
86. Bax, J. J. et al. Restrictive annuloplasty and coronary revascularization in ischemic mitral regurgitation results in reverse left ventricular remodeling. Circulation 110 (Suppl. 1), II103–II108 (2004).
87. Braun, J. et al. Restrictive mitral annuloplasty cures ischemic mitral regurgitation and heart failure. Ann. Thorac. Surg. 85, 430–436 (2008).
88. Wu, A. H. et al. Impact of mitral valve annuloplasty on mortality risk in patients with mitral regurgitation and left ventricular systolic dysfunction. J. Am. Coll. Cardiol. 45, 381–387 (2005).
89. McGee, E. C. et al. Recurrent mitral regurgitation after annuloplasty for functional ischemic mitral regurgitation. J. Thorac. Cardiovasc. Surg. 128, 916–924 (2004).
90. Hung, J. et al. Mechanism of recurrent ischemic mitral regurgitation after annuloplasty: continued LV remodeling as a moving target. Circulation 110 (Suppl. 1), II85–II90 (2004).
91. Magne, J. et al. Preoperative posterior leaflet angle accurately predicts outcome after restrictive mitral valve annuloplasty for ischemic mitral regurgitation. Circulation 115, 782–791 (2007).
92. Lee, A. P. et al. Mechanisms of recurrent functional mitral regurgitation after mitral valve repair in nonischemic dilated cardiomyopathy: importance of distal anterior leaflet tethering. Circulation 119, 2606–2614 (2009).
93. Braun, J. et al. Preoperative left ventricular dimensions predict reverse remodelling following restrictive mitral annuloplasty in ischaemic mitral regurgitation. Eur. J. Cardiothorac. Surg. 27, 847–853 (2005).
94. Roshanali, F., Mandegar, M. H., Yousefnia, M. A., Rayatzadeh, H. & Alaeddini, F. A prospective study of predicting factors in ischemic mitral regurgitation recurrence after ring annuloplasty. Ann. Thor. Surg. 84, 745–749 (2007).
95. Ciarka, A. et al. Predictors of mitral regurgitation recurrence in patients with heart failure undergoing mitral valve annuloplasty. Am. J. Cardiol. 106, 395–401 (2010).
96. Borger, M. A. et al. Initial results of the chordal-cutting operation for ischemic mitral regurgitation. J. Thorac. Cardiovasc. Surg. 133, 1483–1492 (2007).
97. Hvass, U., Tapia, M., Baron, F., Pouzet, B. & Shafy, A. Papillary muscle sling: a new functional approach to mitral repair in patients with ischemic left ventricular dysfunction and functional mitral regurgitation. Ann. Thorac. Surg. 75, 809–811 (2003).
98. Kron, I. L., Green, G. R. & Cope, J. T. Surgical relocation of the posterior papillary muscle in chronic ischemic mitral regurgitation. Ann. Thorac. Surg. 74, 600–601 (2002).
99. Menicanti, L. et al. Ischemic mitral regurgitation: intraventricular papillary muscle imbrication without mitral ring during left ventricular restoration. J. Thorac. Cardiovasc. Surg. 123, 1041–1050 (2002).
100. De Bonis, M. et al. Mitral valve repair for functional mitral regurgitation in end-stage dilated cardiomyopathy: role of the “edge-to-edge” technique. Circulation 112 (Suppl. 9), I402–I408 (2005).
101. Mann, D. L. et al. Clinical evaluation of the CorCap Cardiac Support Device in patients with dilated cardiomyopathy. Ann. Thorac. Surg. 84, 1226–1235 (2007).
102. Tulner, S. A. et al. Clinical efficacy of surgical heart failure therapy by ventricular restoration and restrictive mitral annuloplasty. J. Card. Fail. 13, 178–183 (2007).
103. Vassileva, C. M., Boley, T., Markwell, S. & Hazelrigg, S. Meta-analysis of short-term and long-term survival following repair versus replacement for ischemic mitral regurgitation. Eur. J. Cardiothorac. Surg. 39, 295–303 (2011).
104. Gillinov, A. M. et al. Is repair preferable to replacement for ischemic mitral regurgitation? J. Thorac. Cardiovasc. Surg. 122, 1125–1141 (2001).
105. De Bonis, M. & Alfieri, O. Mitral regurgitation should be corrected in patients with dilated cardiomyopathy. Nat. Clin. Pract. Cardiovasc. Med. 5, 452–453 (2008).
106. Bach, D. S., Awais, M., Gurm, H. S. & Kohnstamm, S. Failure of guideline adherence for intervention in patients with severe mitral regurgitation. J. Am. Coll. Cardiol. 54, 860–865 (2009).
107. Mirabel, M. et al. What are the characteristics of patients with severe, symptomatic, mitral regurgitation who are denied surgery? Eur. Heart J. 28, 1358–1365 (2007).
108. Seiffert, M. et al. Series of transcatheter valve-in-valve implantations in high-risk patients with degenerated bioprostheses in aortic and mitral position. Catheter. Cardiovasc. Interv. 76, 608–615 (2010).
109. Nuñez-Gil, I. J. et al. Transapical mitral valve-in-valve implantation: a novel approach guided by three-dimensional transoesophageal echocardiography. Eur. J. Echocardiogr. 12, 335–337 (2011).
110. Cheung, A. W. et al. Transcatheter transapical mitral valve-in-valve implantations for a failed bioprosthesis: a case series. J. Thorac. Cardiovasc. Surg. 141, 711–715 (2011).
111. de Weger, A., Ewe, S. H., Delgado, V. & Bax, J. J. First-in-man implantation of a trans-catheter aortic valve in a mitral annuloplasty ring: novel treatment modality for failed mitral valve repair. Eur. J. Cardiothorac. Surg. 39, 1054–1056 (2011).
112. Kawata, M., Vasilyev, N. V., Perrin, D. P. & del Nido, P. J. Beating-heart mitral valve suture annuloplasty under real-time three-dimensional echocardiography guidance: an ex vivo study. Interact. Cardiovasc. Thorac. Surg. 11, 6–9 (2010).
113. Swaans, M. J., Post, M. C. & ten Berg, J. M. Transapical repair of mitral valve paravalvular leakage using 3-D transesophageal guidance. Catheter. Cardiovasc. Interv. 77, 121–123 (2011).
114. Forleo, G. B. et al. Real-time integration of intracardiac echocardiography and 3D electroanatomical mapping to guide catheter ablation of isthmus-dependent atrial flutter in a patient with complete situs inversus and interruption of the inferior vena cava with azygos continuation. J. Interv. Card. Electrophysiol. 30, 273–277 (2011).
115. Maisano, F. et al. Beating-heart implantation of adjustable length mitral valve chordae: acute and chronic experience in an animal model. Eur. J. Cardiothorac. Surg. 40, 840–847 (2011).
REVIEWS
© 2012 Macmillan Publishers Limited. All rights reserved
146 | MARCH 2012 | VOLUME 9 www.nature.com/nrcardio
116. Condado, J. A. et al. Percutaneous edge-to-edge mitral valve repair: 2-year follow-up in the first human case. Catheter. Cardiovasc. Interv. 67, 323–325 (2006).
117. Feldman, T. et al. Percutaneous repair or surgery for mitral regurgitation. N. Engl. J. Med. 364, 1395–1406 (2011).
118. Franzen, O. et al. Acute outcomes of MitraClip therapy for mitral regurgitation in high-surgical- risk patients: emphasis on adverse valve morphology and severe left ventricular dysfunction. Eur. Heart J. 31, 1373–1381 (2010).
119. Maisano, F. European percutaneous mitral valve therapy experience: acute results in the first 1,000 patients. Data from the European ACCESS Registry: what patients have been treated in Europe? Presented at TCT 2010.
120. Tamburino, C. et al. Percutaneous mitral valve repair with the MitraClip system: acute results from a real world setting. Eur. Heart J. 31, 1382–1389 (2010).
121. Maisano, F. et al. Surgical isolated edge-to-edge mitral valve repair without annuloplasty: clinical proof of the principle for an endovascular approach. EuroIntervention 2, 181–186 (2006).
122. Schofer, J. et al. Percutaneous mitral annuloplasty for functional mitral regurgitation results of the CARILLON Mitral Annuloplasty Device European Union Study. Circulation 120, 326–333 (2009).
123. Webb, J. G. et al. Percutaneous transvenous mitral annuloplasty: initial human experience with device implantation in the coronary sinus. Circulation 113, 851–855 (2006).
124. Sack, S. et al. Percutaneous transvenous mitral annuloplasty: initial human experience with a novel coronary sinus implant device. Circ. Cardiovasc. Interv. 2, 277–284 (2009).
125. Lansac, E. et al. Percutaneous mitral annuloplasty through the coronary sinus: an anatomic point of view. J. Thorac. Cardiovasc. Surg. 135, 376–381 (2008).
126. Webb, J. G. et al. Percutaneous suture edge-to-edge repair of the mitral valve. EuroIntervention 5, 86–89 (2009).
127. Bajona, P., Katz, W. E., Daly, R. C., Zehr, K. J. & Speziali, G. Beating-heart, off-pump mitral valve repair by implantation of artificial chordae tendineae: an acute in vivo animal study. J. Thorac. Cardiovasc. Surg. 137, 188–193 (2009).
128. Panic, G. et al. A novel technique for treatment of mitral valve prolapse/flail. J. Thorac. Cardiovasc. Surg. 137, 1568–1570 (2009).
129. Williams, J. L. et al. Feasibility of myxomatous mitral valve repair using direct leaflet and chordal radiofrequency ablation. J. Interv. Cardiol. 21, 547–554 (2008).
130. Kim, J. H. et al. Mitral cerclage annuloplasty, a novel transcatheter treatment for secondary mitral valve regurgitation: initial results in swine. J. Am. Coll. Cardiol. 54, 638–651 (2009).
131. Raman, J., Hare, D., Storer, M. & Hata M. Epicardial cardiac basal annuloplasty: preliminary findings on extra-cardiac mitral valve repair. Heart Lung Circ. 18, 401–406 (2009).
132. Rahman, S., Eid, N., Murarka, S. & Heuser R. R. Remodeling of the mitral valve using radiofrequency energy: review of a new treatment modality for mitral regurgitation. Cardiovasc. Revasc. Med. 11, 249–259 (2010).
133. Heuser, R. R., Witzel, T., Dickens, D. & Takeda, P. A. Percutaneous treatment for mitral regurgitation: the QuantumCor system. J. Interv. Cardiol. 21, 178–182 (2008).
134. Jilaihawi, H. et al. Mitral annular reduction with subablative therapeutic ultrasound: pre-clinical
evaluation of the ReCor device. EuroIntervention 6, 54–62 (2010).
135. Lozonschi, L. et al. Transapical mitral valved stent implantation: A survival series in swine. J. Thorac. Cardiovasc. Surg. 140, 422.e1–426.e1 (2010).
136. Lutter, G. et al. Mitral valved stent implantation. Eur. J. Cardiothorac. Surg. 38, 350–355 (2010).
137. Grossi, E. A. et al. Ischemic mitral valve reconstruction and replacement: comparison of long-term survival and complications. J. Thorac. Cardiovasc. Surg. 122, 1107–1124 (2001).
138. Braun, J. et al. Preoperative left ventricular dimensions predict reverse remodelling following restrictive mitral annuloplasty in ischaemic mitral regurgitation. Eur. J. Cardiothorac. Surg. 27, 847–853 (2005).
139. Magne, J. et al. Preoperative posterior leaflet angle accurately predicts outcome after restrictive mitral valve annuloplasty for ischemic mitral regurgitation. Circulation 115, 782–791 (2007).
140. Lee, A. P. et al. Mechanisms of recurrent functional mitral regurgitation after mitral valve repair in nonischemic dilated cardiomyopathy: importance of distal anterior leaflet tethering. Circulation 119, 2606–2614 (2009).
141. Gelsomino, S. et al. Left ventricular reverse remodeling after undersized mitral ring annuloplasty in patients with ischemic regurgitation. Ann. Thorac. Surg. 85, 1319–1330 (2008).
Author contributionsAll authors contributed equally to researching data for the article, made substantial contributions to the discussion of content, wrote, and reviewed and edited the manuscript before submission.
REVIEWS
© 2012 Macmillan Publishers Limited. All rights reserved