Embed Size (px)
Citation preview
Treatment as prevention: a new paradigm for HIV control?
Richard Hayes
Treatment as prevention
• Background and rationale• Design of PopART/HPTN071 trial• Other planned trials
ART for prevention: background
• HIV incidence continues to be unacceptably high in many countries in Africa
• Lack of proven effective HIV prevention strategies• Unless incidence can be reduced dramatically it will
become increasingly difficult over time to sustain effective ART services
Lancet 2009 373: 48-57
ART for prevention: background
• HIV incidence continues to be unacceptably high in many countries in Africa
• Lack of proven effective HIV prevention strategies• Unless incidence can be reduced dramatically it will
become increasingly difficult over time to sustain effective ART services
• Risk of HIV transmission closely correlated with HIV viral load and ART can be used to reduce HIV viral load and hence infectivity
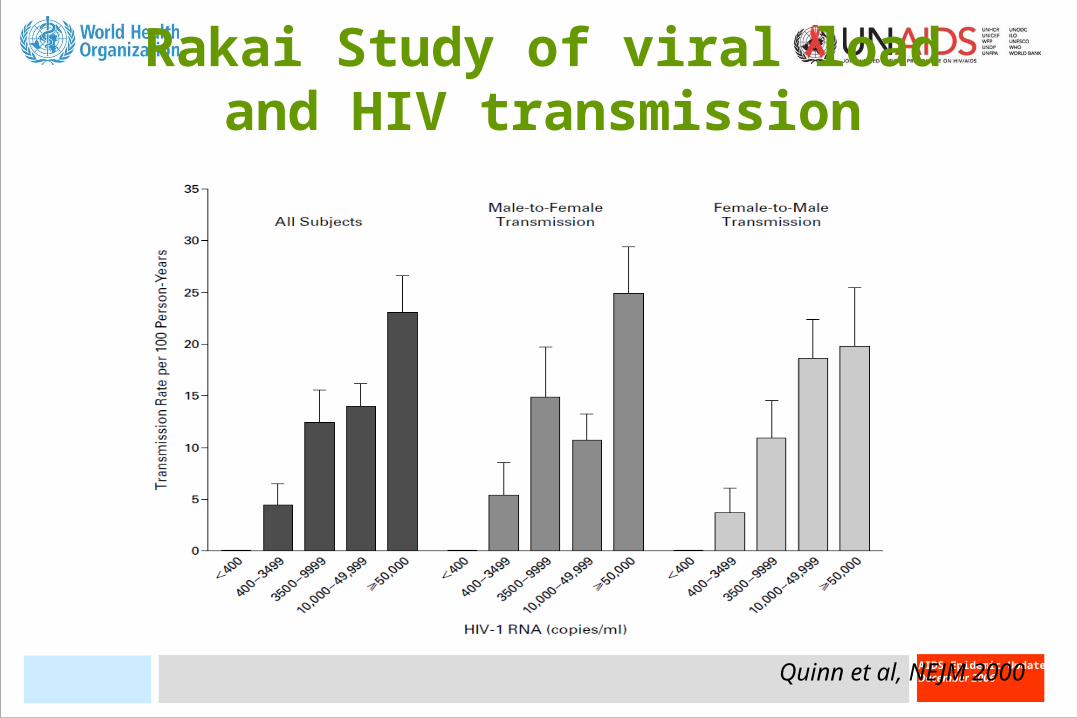
Rakai Study of viral load and HIV transmission
Quinn et al, NEJM 2000
Evidence from HPTN 052
• 1763 HIV-discordant couples in 9 countries, CD4=250-550• Randomized to immediate or deferred treatment• Stopped for efficacy• 39 HIV-ve partners were infected of which 29 were linked
virologically to the infected partner• Of these 29 only 1 was in the immediate treatment group• HR = 0.04 (95% CI: 0.01–0.27)• Also significant reduction in morbidity endpoints in treated
individuals – HR for serious clinical endpoints = 0.59 (95% CI: 0.40-0.88)
ART for prevention: background
• HIV incidence continues to be unacceptably high in many countries in Africa
• Lack of proven effective HIV prevention strategies• Unless incidence can be reduced dramatically it will
become increasingly difficult over time to sustain effective ART services
• Risk of HIV transmission closely correlated with HIV viral load and ART can be used to reduce HIV viral load and hence infectivity
• Current guidelines limit ART to those with late-stage HIV infection (CD4<200 or CD4<350) but most transmission occurs before that

Universal test and treat intervention
• Promote universal HIV voluntary counselling and testing at regular intervals
• All those diagnosed HIV positive are started on ART immediately
• Model shows immediate increase in numbers needing treatment but in medium-term, HIV incidence and prevalence are reduced dramatically
• In long-term, numbers needing ART are reduced.
Why is a trial needed?
• Not known whether a UTT intervention can be delivered with high uptake and acceptability
• Many uncertainties in model parameters• Population-level impact of (feasible) intervention package
is not known• Many potential adverse effects, such as toxicity, drug
resistance, sexual risk disinhibition, HIV-related stigma, overload of health services
• A rigorously designed trial can measure the costs and benefits of this strategy and provide reliable evidence on cost-effectiveness for health policy makers
HPTN 071 = PopART
Population effect of universal testing and immediate ART therapy to Reduce HIV Transmission
The PopART intervention package
• Universal voluntary HIV testing delivered through a house-to-house campaign
• Male circumcision offered to men who test HIV-negative• Immediate ART offered to all who test HIV-positive
• Counselling and condom provision• Strengthening of PMTCT services• Syndromic STI treatment at clinic
• CHiPs team (Community HIV Providers) to deliver testing, counselling, linkage to care and treatment support
Additional benefits of intervention – individual and public health
• Reduction of morbidity and mortality in those receiving ART through earlier onset of treatment
• Simplification of ART delivery and monitoring• Reduction of adverse effects of treatment• Reduction of clinic burden of TB and other illnesses• (Potential) elimination of mother to child HIV transmission• (Eventual) cost savings• Normalisation of HIV and reduction in HIV-related stigma• Reduces need for specially targeted interventions
Design of trial
• 24 clusters (15 in Zambia + 9 in S Africa)• Cluster = community served by a health facility• Variable population size but averages 50-60k• Clusters matched into triplets by HIV prevalence: 5 triplets
in Zambia, 3 in S Africa• Clusters randomly allocated to 3 study arms within each
matched triplet• Restricted randomisation used to ensure balance on ART
uptake, population size and HIV prevalence
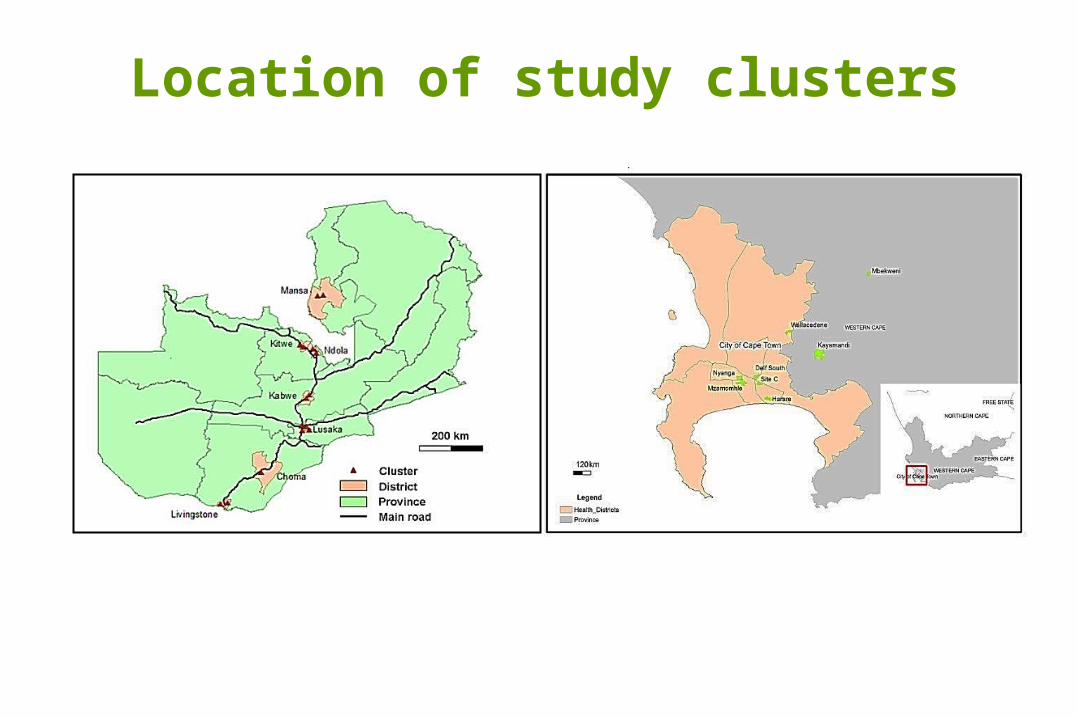
Location of study clusters
Study arms
• Arm A (8 clusters): Full PopART intervention including immediate ART irrespective of CD4 count
• Arm B (8 clusters): Full PopART intervention except that ART is initiated according to current national guidelines (CD4 < 350 or WHO stage 3/4)
• Arm C (8 clusters): Standard of care
Evaluation surveys
• Population cohort (All 3 arms)• 2,500 adults aged 18-44 sampled randomly from general
population of each cluster (1 adult per household)• Total size of cohort = 2,500 x 24 = 60,000• Followed up after 1 year and 2 years of intervention
• Population cross-sectional survey (All 3 arms)• 500 adults aged 18-44 sampled randomly from general
population of each cluster (all adults in selected households)• Total size of survey = 500 x 24 = 12,000• At final follow-up after 2 years of intervention
Evaluation surveys
• Clinic cohort (All 3 arms)• Sample of 300 HIV+ve patients presenting at clinic to register
for HIV treatment and care• Total size of cohort = 300 x 24 = 7,200• Followed up for 2 years
Primary outcome
Population cohort• HIV incidence over 2 years• Will also look at impact during first year and second year of
follow-up
Secondary outcomes
Population cohort• HSV-2 incidence (marker of risk behaviour)
Population cohort and Population cross-sectional survey• Sexual risk behaviour and HIV-related stigma• Community HIV viral load, CD4 count, drug resistance• Uptake of services
• HIV-free infant survival• TB prevalence
Secondary outcomes
Clinic cohort• HIV disease progression, CD4 count, morbid events• ART adherence and viral suppression• Drug resistance
Clinic and CHiPs records• Uptake of services• TB case notification, clinic burden by cause
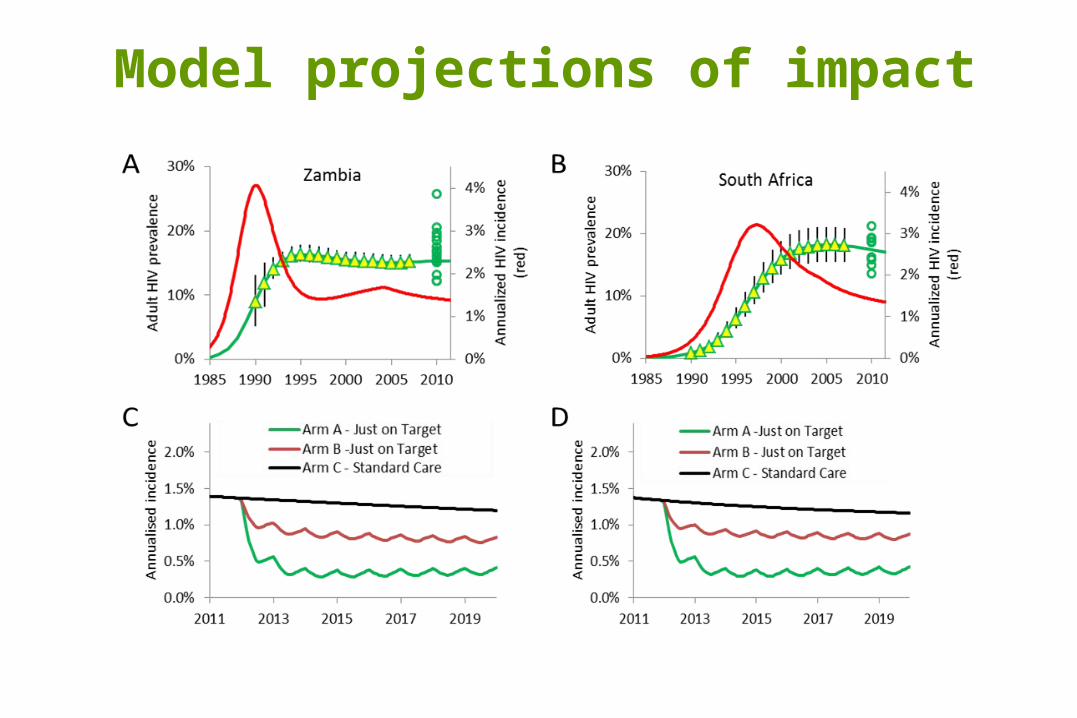
Model projections of impact
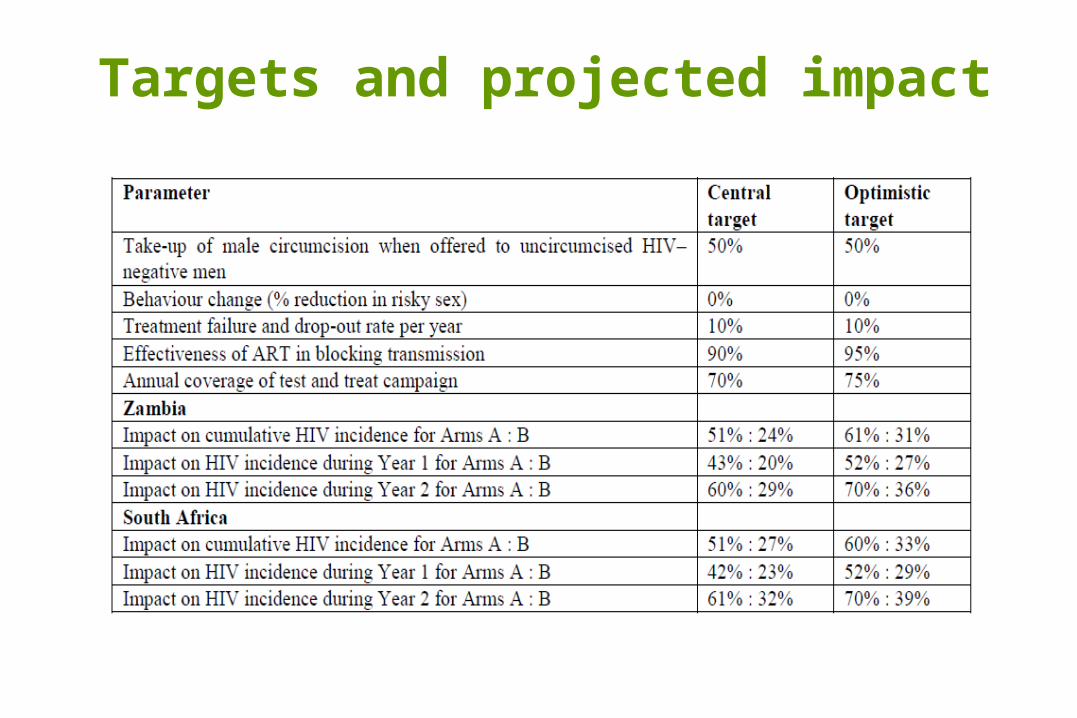
Targets and projected impact
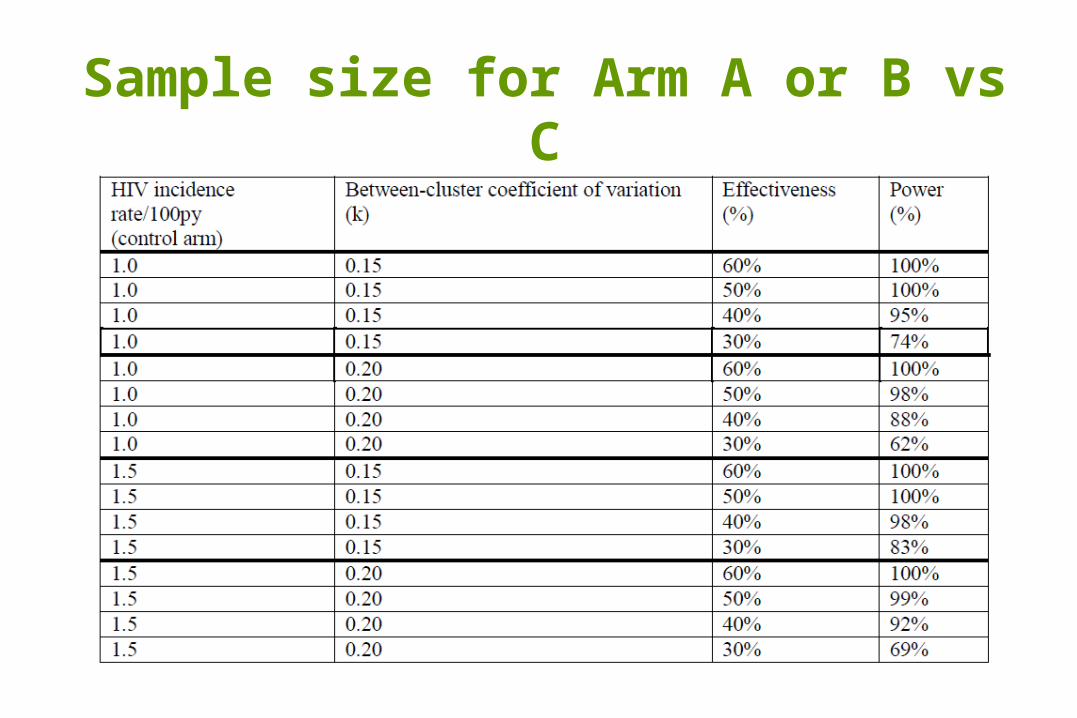
Sample size for Arm A or B vs C
Funding of PopART/HPTN071
• OGAC (PEPFAR)• Bill & Melinda Gates Foundation• NIH
• PopART is one of 3 trials of combination HIV prevention supported by OGAC
• 2 other trials in Botswana (Harvard) and Tanzania (JHU)
Other planned trials (1)
Iringa, Tanzania (2 arms)• Arm A: Expanded testing/linkage to care, ART at CD4<350, IEC,
male circumcision, conditional cash transfers, targeted outreach• Arm B: Standard of care• 24 clusters (12 vs 12)• Cohort of 500/cluster, total 12,000, 24m follow-up
Botswana (2 arms)• Arm A: Expanded testing/linkage to care, ART at CD4<350 OR
VL>10,000, male circumcision• Arm B: Standard of care• 20 clusters (10 vs 10)• Cohort of 500/cluster, total 10,000, 36-48m follow-up
Other planned trials (2)
KwaZulu Natal, S Africa (2 arms) – TasP trial• Arm A: Expanded testing, male circumcision, immediate ART,
IEC, STI treatment etc.• Arm B: As above but ART at CD4<350• 32 clusters (16 vs 16)• 1,250/cluster, total 40,000, 24m follow-up (total population)• Funding currently available for initial feasibility study in 4 of the
32 clusters
The HPTN 071 team
LSHTM ZambartRichard Hayes Helen AylesDebby Watson-Jones Virginia BondKalpana Sabapathy Nathaniel ChisingaSian Floyd Ab SchaapLucy Bradshaw
Imperial College Desmond Tutu TB CentreSarah Fidler Nulda BeyersChristophe Fraser Peter BockPeter Smith Lyn Horne
The HPTN 071 research team
HPTN/FHI360 HPTN Network LabSten Vermund Sue EshlemanAyana Moore Estelle Piwowar-ManningSam GriffithRhonda White
DAIDS SCHARPDavid Burns Deborah DonnellPeter Kim Lynda Emel