Embed Size (px)
Citation preview

Treatment of Opioid Dependency in Pregnancy and Strategies to Reduce
Neonatal Abstinence Syndrome

Over the last decade, increased attention has focused upon the parallel rise in two
trends: an increased prevalence of prescription opioid misuse and an increased
incidence of NAS.

Signs and Symptoms of NAS
• Neonatal Abstinence Syndrome (NAS) is neonatal withdrawal after exposure to certain illicit or prescription drugs in the womb, which occurs with the abrupt cessation of the exposure resulting from birth.
• Signs and symptoms can be different for every baby with NAS. Most appear within 3 days (72 hours) of birth, but some can appear right after birth or within a few weeks of birth.
• Symptoms are measured in the following categories:– Central nervous system disturbances– Metabolic/Vasomotor/Respiratory disturbances– Gastrointestinal disturbances

Incidence of NAS
• Approximately 55-94 percent of exposed newborns will experience NAS.
• Variability is explained by several factors:– Prenatal opioid exposure is a risk factor for but not a
predictor of NAS – Neither daily opioid dose nor total dose throughout
the pregnancy predict incidences nor severity of NAS
– Wide variability exists among institutions in the diagnosis of NAS in opioid-exposed populations

Rates of NAS
• NAS cases in the U.S. grew by 300% between 2000 and 2009– In 2000, there were 1.2 cases per 1,000
U.S. births. – In 2009, there were 3.3 cases per 1,000
U.S. births.
• In Texas, one out of four pregnant women admitted to DSHS-funded treatment services are dependent on opioids.

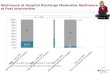
Texas Medicaid NAS Births
Series1750
800
850
900
950
1000
1050
2011 2012 2013

2013 Texas Medicaid NAS Births Data
• Average length of hospital stay was 24 days• Average cost for hospital stay was $33,000• Counties with highest incidence:– Bexar 32%– Dallas 12%– Harris 11%– Tarrant 10%– Nueces 5%– Travis 4%

http://www.astho.org/Prevention/NAS-Neonatal-Abstinence-Report/
asthoNeonatal Abstinence Syndrome: How States Can Help Advance the Knowledge Base for Primary Prevention and Best Practices of Care
A state-level approach to NAS can address several levels of intervention, including:
• Surveillance for NAS-affected infants and the sources of maternal opiate use.
• Reimbursement for utilizing screening protocols to detect substance abuse early in pregnancy and withdrawal signs in newborns.
• Developing better measures to ensure follow-up of opioid-dependent women and receipt of comprehensive services.
• Collaborative efforts to strengthen clinical standards for identification, management, and follow-up of NAS-affected infants and their families.
Although much is known about how to manage opioid dependency in pregnancy and NAS, manyresearch and operational questions remain regarding how to consistently provide good quality ofcare in an unbiased and compassionate manner. State health agencies, along with other agencies,professional networks, and community partners, have a unique contribution to make to the knowledge base and support of best practices in caring for women and their children affected by NAS.

http://www.acog.org/-/media/Departments/Government-Relations-and-Outreach/NASToolkit.pdf?dmc=1&ts=20150326T1453435852
ACOG

NAS Exceptional Item:
• This Exceptional Item (EI) would appropriate $17 million in General Revenue to DSHS over the course of the 2016-2017 biennium to fund new and existing services aimed at reducing incidence, severity, and costs associated with NAS.
• This EI would take a multi-pronged approach to addressing NAS by: – enhancing screening and outreach to women of
childbearing age to reduce the number of opioid dependent women that become pregnant
– increasing the availability of intervention and treatment services to pregnant and postpartum women to improve birth outcomes
– implementing specialized programs to reduce the severity of NAS

NAS EI Details:Purpose
• Provide a continuum of care for at-risk women by increasing: Screening, Brief Intervention, and Referral to Treatment (SBIRT) services; Opioid Substitution Therapy (OST); case management services; and Pregnant and Postpartum Intervention (PPI) services
• Target outreach services for over 1,000 pregnant women with substance abuse disorders
• Implement a residential substance use disorder treatment pilot program for over 150 clients
• Expand the “Mommies” program to hospitals with highest incidence of NAS, serving about 560 more families
• Ensure availability of best practices education for a broad array of providers about how to provide appropriate care for at-risk women
Outcomes
• Improved health outcomes for children born to women who receive services
• Reduced use of Neonatal Intensive Care Units (NICUs) for children born to women who receive assistance
• Fewer hospitalizations, arrests, and injuries for women who are referred to and receive services
• Reduced rate of removal by Child Protective Services due to parental substance abuse
Return on Investment: An estimated $1.4 million in General Revenue savings to Medicaid in FY 2017 ($3.95 savings for every $1 invested)

The “Mommies” Program: a Model of Integrated Care
The Center for Healthcare Services:
Methadone Clinic
University Health System (UHS):
County Hospital
The U.T. Health Science Center &
Department of State Health Services:
The “Mommies” Program

“Mommies”: A Healthcare Environment “Culture” Change
• “Mommies” are treated like any other patient with a chronic healthcare need such as diabetes or hypertension.
• During encounters, are referred to as “one of our Mommies” to reduce stigmatization
• The result of both educating the mothers and developing a therapeutic relationship prior to delivery has proven to reduce NICU lengths of stay and lowered DFPS removal rates.
• In addition, many newborns delivered by mothers in this program have symptoms that do not require hospitalization.

Contact
Lisa Ramirez M.A. LCDCWomen’s SUD Services Coordinator
Department of State Health Services512.206.5414
[email protected]://www.dshs.state.tx.us/sa/nas/