Embed Size (px)
Citation preview
TPPIAA
TWiTe
Hiisftsptatie
ugptttuffisj
FS
Hk
©A
Case Report
reatment of Posttraumatic High-Flowriapism in 8-Year-Old Boy withercutaneous Ultrasound-Guided Thrombin
njectionndrás Kiss, Mária Polovitzer, Miklós Merksz, Attila Kardos, Péter Schaffer,sztrid Apor, and Kálmán Hüttl
reatment of high-flow priapism varies and has included transcatheter embolization when conservative approaches fail.e present the case of an 8-year-old boy with high-flow priapism, who was treated with ultrasound-guided thrombin
njection because of encouraging experience with the method obtained when treating aneurysms and pseudoaneurysms.his procedure appears to be a useful alternative to transcatheter embolization and results in no radiation
xposure. UROLOGY 69: 779.e7–779.e9, 2007. © 2007 Elsevier Inc.CAppibsll
paflrhccstcsHnpppttapucco
igh-flow priapism in a child is typically diag-nosed in association with a history of penile orperineal trauma, resulting in a pathologically
ncreased arterial blood influx into the cavernous bod-es caused by a shunt between the arterial and lacunarystems. Treatment of high-flow priapism has variedrom watchful waiting to mechanical compression,ranscatheter embolization of the shunt, or, even, openurgery. The first reported embolization for high-flowriapism in a child was reported in 1992. Superselec-ive arteriography and embolization has been suggesteds the therapy of choice if conservative options fail inhis condition.1– 4 This procedure includes the use ofonizing radiation, which can result in adverse events,specially in children.
Intravascular thrombin injections have been safelysed for several indications, including esophageal andastric varices, arterial aneurysms, and iatrogenicseudoaneurysms. Even though ultrasound-guidedhrombin injection is the initial treatment of choice inhe care of complications of inadvertent arterial punc-ure,5,6 to our knowledge, this technique has not beensed in the treatment of high-flow priapism resultingrom posttraumatic arteriovenous fistula. We describe therst report of a posttraumatic high-flow priapism treateduccessfully with ultrasound-guided single-thrombin in-ection.
rom the Heim Pál Children’s Hospital; and Clinics of Cardiovascular Surgery,emmelweis University, Budapest, Hungary
Address for correspondence: András Kiss, M.D., Ph.D., Department of Urology,eim Pál Children’s Hospital, Ullõi u. 86, Budapest H-1089, Hungary. E-mail:
Submitted: September 15, 2006; accepted (with revisions): February 8, 2007
2007 Elsevier Inc.ll Rights Reserved
ASE REPORTn 8-year-old boy presented with a 7-day history of a
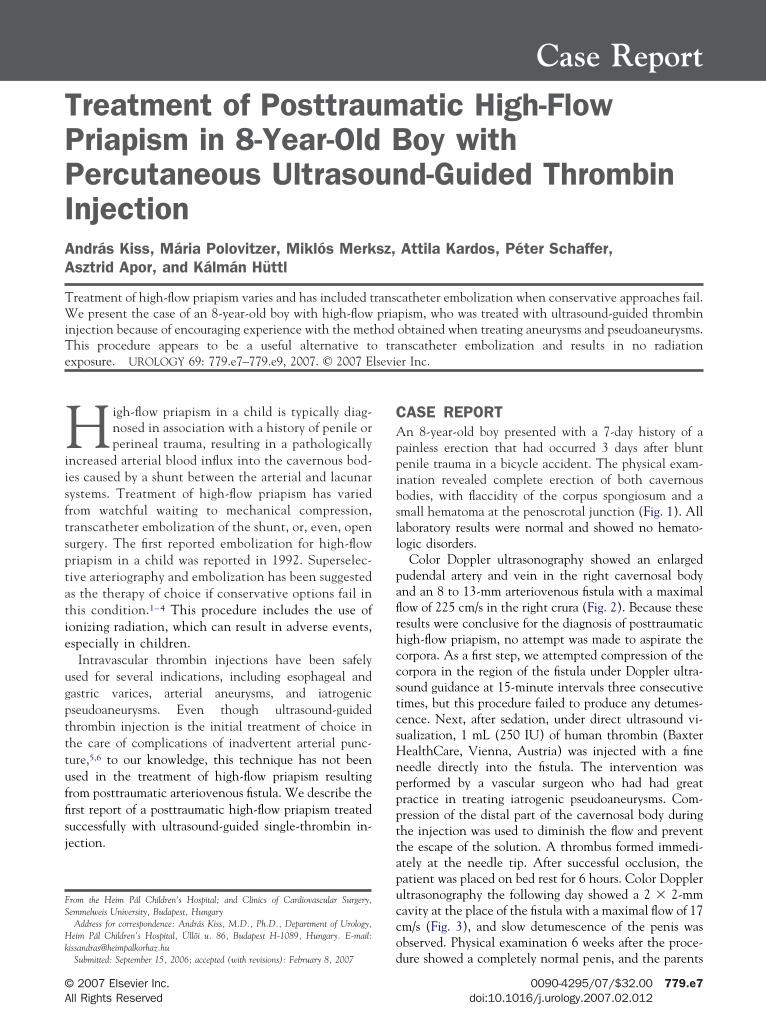
ainless erection that had occurred 3 days after bluntenile trauma in a bicycle accident. The physical exam-nation revealed complete erection of both cavernousodies, with flaccidity of the corpus spongiosum and amall hematoma at the penoscrotal junction (Fig. 1). Allaboratory results were normal and showed no hemato-ogic disorders.
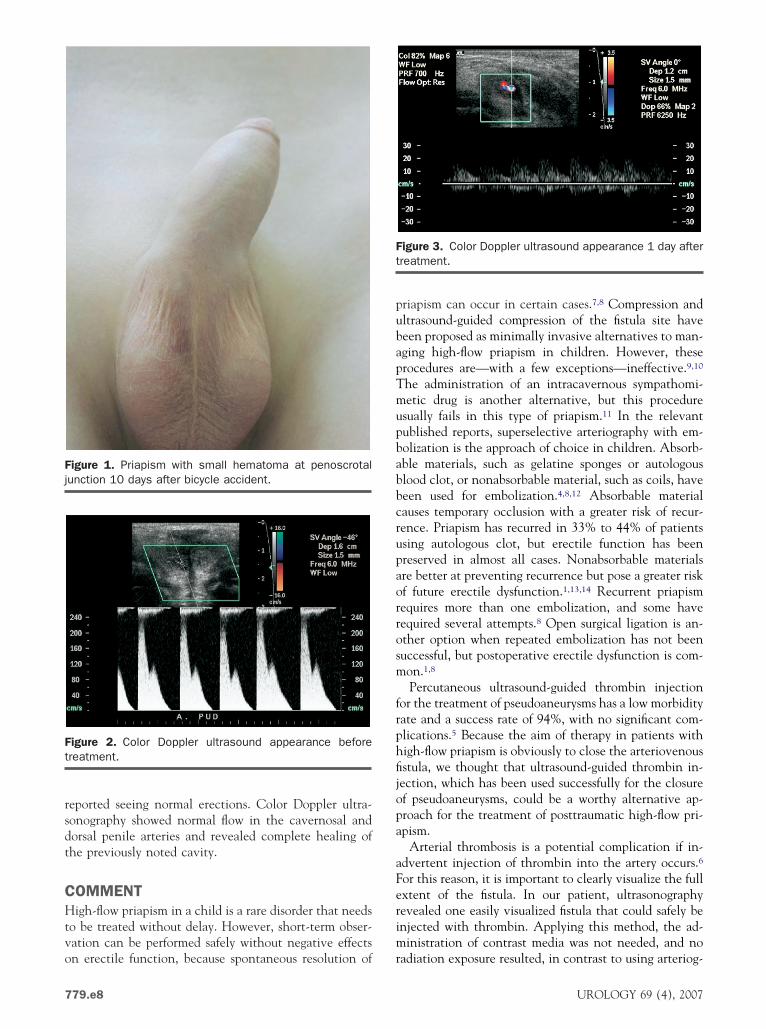
Color Doppler ultrasonography showed an enlargedudendal artery and vein in the right cavernosal bodynd an 8 to 13-mm arteriovenous fistula with a maximalow of 225 cm/s in the right crura (Fig. 2). Because theseesults were conclusive for the diagnosis of posttraumaticigh-flow priapism, no attempt was made to aspirate theorpora. As a first step, we attempted compression of theorpora in the region of the fistula under Doppler ultra-ound guidance at 15-minute intervals three consecutiveimes, but this procedure failed to produce any detumes-ence. Next, after sedation, under direct ultrasound vi-ualization, 1 mL (250 IU) of human thrombin (BaxterealthCare, Vienna, Austria) was injected with a fineeedle directly into the fistula. The intervention waserformed by a vascular surgeon who had had greatractice in treating iatrogenic pseudoaneurysms. Com-ression of the distal part of the cavernosal body duringhe injection was used to diminish the flow and preventhe escape of the solution. A thrombus formed immedi-tely at the needle tip. After successful occlusion, theatient was placed on bed rest for 6 hours. Color Dopplerltrasonography the following day showed a 2 � 2-mmavity at the place of the fistula with a maximal flow of 17m/s (Fig. 3), and slow detumescence of the penis wasbserved. Physical examination 6 weeks after the proce-
ure showed a completely normal penis, and the parents0090-4295/07/$32.00 779.e7doi:10.1016/j.urology.2007.02.012
rsdt
CHtvo
pubapTmupbabbcrupaorrosm
frphfijopa
aFerim
Fj
Ft
Ft
7
eported seeing normal erections. Color Doppler ultra-onography showed normal flow in the cavernosal andorsal penile arteries and revealed complete healing ofhe previously noted cavity.
OMMENTigh-flow priapism in a child is a rare disorder that needs
o be treated without delay. However, short-term obser-ation can be performed safely without negative effects
igure 1. Priapism with small hematoma at penoscrotalunction 10 days after bicycle accident.
igure 2. Color Doppler ultrasound appearance beforereatment.
n erectile function, because spontaneous resolution of r
79.e8
riapism can occur in certain cases.7,8 Compression andltrasound-guided compression of the fistula site haveeen proposed as minimally invasive alternatives to man-ging high-flow priapism in children. However, theserocedures are—with a few exceptions—ineffective.9,10
he administration of an intracavernous sympathomi-etic drug is another alternative, but this procedure
sually fails in this type of priapism.11 In the relevantublished reports, superselective arteriography with em-olization is the approach of choice in children. Absorb-ble materials, such as gelatine sponges or autologouslood clot, or nonabsorbable material, such as coils, haveeen used for embolization.4,8,12 Absorbable materialauses temporary occlusion with a greater risk of recur-ence. Priapism has recurred in 33% to 44% of patientssing autologous clot, but erectile function has beenreserved in almost all cases. Nonabsorbable materialsre better at preventing recurrence but pose a greater riskf future erectile dysfunction.1,13,14 Recurrent priapismequires more than one embolization, and some haveequired several attempts.8 Open surgical ligation is an-ther option when repeated embolization has not beenuccessful, but postoperative erectile dysfunction is com-on.1,8
Percutaneous ultrasound-guided thrombin injectionor the treatment of pseudoaneurysms has a low morbidityate and a success rate of 94%, with no significant com-lications.5 Because the aim of therapy in patients withigh-flow priapism is obviously to close the arteriovenousstula, we thought that ultrasound-guided thrombin in-ection, which has been used successfully for the closuref pseudoaneurysms, could be a worthy alternative ap-roach for the treatment of posttraumatic high-flow pri-pism.
Arterial thrombosis is a potential complication if in-dvertent injection of thrombin into the artery occurs.6or this reason, it is important to clearly visualize the fullxtent of the fistula. In our patient, ultrasonographyevealed one easily visualized fistula that could safely benjected with thrombin. Applying this method, the ad-inistration of contrast media was not needed, and no
igure 3. Color Doppler ultrasound appearance 1 day afterreatment.
adiation exposure resulted, in contrast to using arteriog-
UROLOGY 69 (4), 2007

ratsrogl
CUaee
R
1
1
1
1
1
U
aphy. Unlike in adults, in children, bilateral or multiplerterial lacerations are more frequent. In these cases, theechnique we have described cannot be expected to beuccessful. However, multiple arterial lacerations oftenequire more than one angiography session; therefore, ifnly one well-visualized fistula is present, ultrasound-uided thrombin injection could be used, with superse-ective angiography only for the unsuccessful cases.
ONCLUSIONSltrasound-guided thrombin injection for high-flow pri-
pism appears to be a useful alternative to transcathetermbolization and results in no radiation exposure; how-ver, more data are needed to confirm our experience.
eferences1. Ciampalini S, Savoca G, Butazzi L, et al: High-flow priapism:
treatment and long-term follow-up. Urology 59: 110–113, 2001.2. Marotte JB, Brooks JD, Sze D, et al: Juvenile posttraumatic high-
flow priapism: current management dilemmas. J Pediatr Surg 40:E25–E28, 2005.
3. Visvanathan K, Burrows PE, Schillinger JF, et al: Posttraumaticarterial priapism in a 7-year-old: successful management by percu-taneous transcatheter embolization. J Urol 148: 382–383, 1992.
4. Volkmer BG, Nesslauer T, Kraemer SC, et al: Prepubertal high flowpriapism: incidence, diagnosis and treatment. J Urol 166: 1018–
1022, 2001.ROLOGY 69 (4), 2007
5. Perna LL, Olin JW, Goines D, et al: Ultrasound-guided thrombininjection for the treatment of postcatheterization pseudoaneurysms.Circulation 102: 2391–2395, 2000.
6. McConell PI, Rehm J, Oltman DL, et al: Thrombin injection fortreating a subclavian pseudoaneurysm. Surgery 127: 716–718,1999.
7. Ilkay AK, and Levine LA: Conservative management of high-flowpriapism. Urology 46: 419–424, 1999.
8. Hatzichristou D, Salpiggidis G, Hatzimouratidis K, et al: Manage-ment strategy for arterial priapism: therapeutic dilemmas. J Urol168: 2074–2077, 2002.
9. Mabjeesh NJ, Shamesh D, and Abramiwitz HB: Posttraumatichigh-flow priapism: successful management using duplex guidedcompression. J Urol 161: 215–216, 1999.
0. Imamoglu A, Bakirtas H, Conkbayir I, et al: An alternative non-invasive approach for the treatment of high-flow priapism in achild: duplex ultrasound-guided compression. J Pediatr Surg 41:446–448, 2006.
1. Bastuba MD, Tejada S, Dinlenc CZ, et al: Arterial priapism: diag-nosis, treatment and long-term follow-up. J Urol 151: 1230–1237,1994.
2. Callewaert P, Stockx L, Bogaert G, et al: Post-traumatic high-flowpriapism in a 6-year-old boy: management by percutaneous place-ment of bilateral vascular coils. Urology 52: 234–237, 1998.
3. Park JK, Jeong YB, and Han YM: Recanalization of embolizedcavernosal artery: restoring potency in the patient with high flowpriapism. J Urol 165: 2002–2003, 2001.
4. O’Sullivan P, Browne R, McEniff N, et al: Treatment of “high-flow”priapism with superselective transcatheter embolization: a usefulalternative to surgery. Cardiovasc Intervent Radiol 29: 198–201,
2006.779.e9





























