Embed Size (px)
Citation preview

1
Treatment of Substance Use Disorders in Veterans with Post Traumatic Stress Disorder
(PTSD)
John P. Allen, PhD, MPASenior ScientistVISN 6 MIRECC
Durham, NC

2
Outline of the Presentation
• Context of the Issue• Warzone Stressors• Substance Use Disorder and PTSD in Service
Members and Veterans • Treatment Considerations• VA Services for OEF/OIF Veterans• Military Culture

Scope of the Issue
As of April 6, 2012http://www.defenselink.mil/news/casualty.pdf
USA – War Fatalities 6407 USA - Wounded in Action
47784
Iraq (OIF) 4422 Iraq (OIF) 31923
Iraq (OND) 66 Iraq (OND) 301
Afghanistan (OEF) 1919 Afghanistan (OEF) 15560
OVER 1.9 Million service members have been involved in the Global War on Terror (GWOT).
178,876 TBI’s and 1,621 amputations from 2000 through 2010 Q1
3

Influx of OEF/OIF Veterans
1.9 million have served so far in OEF/OIF 1.9 million have served so far in OEF/OIF
800,000 OEF/OIF Veterans are now VA Eligible800,000 OEF/OIF Veterans are now VA Eligible
300,000 OEF/OIF Veterans have enrolled300,000 OEF/OIF Veterans have enrolled
Former Active DutyFormer Active Duty Former Reserves/NGFormer Reserves/NG
96% of OEF/OIF Veterans have been seen in outpatient care
96% of OEF/OIF Veterans have been seen in outpatient care
4

Mental Health Issues Among OEF/OIF Veterans
• Approximately half of OEF/OIF/OND Veterans receiving VA care have provisional mental health diagnoses. The most common of these are PTSD, affective disorders, neurotic disorders, nondependent abuse of drugs or alcohol, and alcohol dependence.

6
Mental Health Problems in OEF/OIF Veterans
o 38% of Soldiers and 31% of Marines report psychological symptoms.
o Among the National Guard, the figure rises to 49%.
o Psychological concerns are significantly higher among those with repeated deployments.
o Psychological concerns among family members of deployed and returning OEF/OIF/OND Veterans are also of concern. Hundreds of thousands of children have experienced deployment of a parent.

7
Warzone Stressors

8
“In war, there are no unwounded soldiers.”
--Jose Narosky

9
Understanding the Experience of OEF/OIF/OND

10
There’s nothing normal about war. There’s nothing normal about seeing people losing their limbs, seeing your best friend die. There’s nothing normal about that, and that will never become normal…”
– Lt. Col. Paul Pasquina, MD from the movie "Fighting For Life"

11
Traumatic Events in OEF/OIF
Service Members (1)
• Multi-casualty incidents (suicide bombers, IEDs (improvised explosive devices), ambushes)
• Seeing the aftermath of battle• Handling human remains • Friendly fire• Witnessing or being involved in situations of
excessive violence

12
Traumatic Events in OEF/OIF/OND
Service Members (2)
• Witnessing death/injury of close friend/favored leader
• Witnessing death/injury of women and children
• Feeling helpless to defend or counter-attack• Being unable to protect/save another service
member or leader• Killing at close range• Killing civilians and avoidable casualties or
deaths

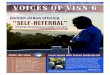
Exposure to traumatic warzone events(Hoge et al., 2004)
Receiv
ing inco
ming arti
llery,
morta
r, or r
ocket
fire
Knowing someo
ne seri
ously in
jured or k
illed
Being a
ttacke
d or ambush
ed
Seein
g dea
d bodies
Shooting o
r dire
cting fi
re at
the enem
y
Handlin
g human
remain
s0
20406080
100
98 92 81 75 63 43
Perc
ent R
epor
ting
13

14
“The most complex and dangerous conflicts, the most harrowing operations, and the most deadly wars, occur in the head.”
(Anthony Swafford, Jarhead from PBS video Operation Homecoming)

Events that provoke terror, horror, or helplessness
Events that provoke terror, horror, or helplessness
Death or injury of others who are loved and with whom one identifies
Death or injury of others who are loved and with whom one identifies
Accumulation of stress from all sources over time
Accumulation of stress from all sources over time
Events that contradict deeply held moral values and beliefs
Events that contradict deeply held moral values and beliefs
Life threatLife
threat
INTENSE OR PROLONGED STRESS
Wear & tear Loss Inner
conflict
Four Causes of Stress Injury
15

PTSD Symptoms Overview
Symptoms of PTSD, present for at least one month, and are divided into three symptom clusters:
• Reexperiencing of the traumatic event,
• Avoidance of trauma-relevant stimuli and numbing of general responsiveness, and
• Heightened physiological arousal.
16

Exposure Contributes to RiskHoge et al., 2006
Anxiety Depression PTSD Any MH Prob-lem
0
5
10
15
20
25
30
35
5 58
118 8
1417
13 12
2830
Low Combat Medium Combat High Combat
Per
cen
t sc
reen
ing
po
siti
ve
17

Millennium Cohort Study
• Largest prospective military health study personnel ever
• 21 year duration - began 2001
• 150,000 participants• Followed every 3 years
thru post-discharge• 35+ articles published
to date
18

Millennium Cohort Findings• Dose Response Relationship
– PTSD and Depression – The more trauma exposure – the more likely to develop problems
– Substance Use – Highest among younger Veterans and Reserve/National Guard
– Smoking initiation and recidivism– Aggressive Driving – Higher among deployed– Aggression and Domestic Violence – higher in PTSD– Hypertension – likely stress related– Eating problems in women with combat exposure
19

20
Common Themes and Presenting Problems in OEF/OIF/OND Veterans
• Marriage, relationship problems• Financial hardships • Endless questions from family and friends • Guilt, shame, anger • Feelings of isolation • Nightmares, sleeplessness• Lack of motivation• Forgetfulness • Anger• Feeling irritable, anxious, “on edge”

21
Military Deployment and Substance Use Disorder (SUD)
• Rate of alcohol behavioral problems doubles (25% vs 12%) before and after deployment (Wilk et al, 2010). (Among Reserve Component personnel there were twice as many new onsets of heavy weekly drinking, binge drinking, and alcohol-related behavioral problems among deployed personnel than among their non-deployed peers (Jacobson et al, 2008).)
• Post deployment military personnel with SUD problems are rarely referred for care (134 referrals/6669 positive alcohol screens on Post Deployment Health Reassessment (PDHRA) for active duty and 179/4787 for reserve component) (Milliken et al, 2007).

22
Combat Exposure and SUD
• Combat exposure is associated with increased rates of weekly heavy drinking, binge drinking, and alcohol-related problems. This is particularly true for personnel aged 24 or younger (Jacobson, et al, 2008).
• The threat of death or personal injury is most associated with post-deployment alcohol problems. This relationship is independent of the relationship of these threats to other mental health problems (Wilk et al, 2010).

23
2001 2002 2003 2004 2005 2006 2007 2008 20090.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
Percent of OEF/OIF Veterans with Diagnoses of Substance Use Disorder by Year Seen

24
Considerations in Treatment of Substance Use Disorder and PTSD

25
Dynamics of SUD and PTSD in OEF/OIF Veterans (1)
• 25-50% co-occurrence of SUD and PTSD
• The severity of SUD and PTSD tends to be greater and outcomes tend to be worse for both conditions in patients with both PTSD and SUD than in patients with only one of the conditions
• PTSD typically precedes SUD
• Exposure to trauma stimuli can trigger craving and substance use
• Symptoms of the two conditions co-vary. Diminution of PTSD symptoms precedes reduction in alcohol use

26
Dynamics of SUD and PTSD in OEF/OIF Veterans (2)
• PTSD is a risk factor for SUD—Use of alcohol or drugs may reduce the anxiety component of PTSD and thus be reinforced
• Withdrawal from substances may exacerbate PTSD symptoms
• Prolonged exposure as a treatment for PTSD doesn’t increase craving or substance abuse
• Patients prefer that the two conditions be treated together

27
Evidence Based Treatments for PTSD
• Prolonged Exposure Therapy—Repeated verbalizations of the trauma experience to prompt reprocessing of the trauma. Training in coping skills, stress reduction strategies, cognitive restructuring, real world practice of skills (http://deploymentpsych.org/training/civilian-practice)
• Cognitive Processing Therapy—Education about the PTSD symptoms, challenge and modify beliefs about the trauma event, self-monitoring of thoughts and feelings (http://deploymentpsych.org/training/training-catalog/cognitive-processing-
therapy-cpt-for-ptsd-in-veterans-and-military-personnel)

Effective Alcoholism Treatments (1)
Psychosocial interventions that are well supported by research evidence:
• Motivational Enhancement Therapy• Cognitive Behavior Therapy for Relapse Prevention• Community Reinforcement Approach• Behavioral Couples Therapy• Twelve Step Facilitation

Effective Alcoholism Treatments (2)
• Medications that can serve as alcohol treatment adjuncts:
– Disulfiram (Antabuse®)– Naltrexone/Vivitrol®– Acamprosate– Topiramate (not approved for this indication by
FDA. Research is very encouraging on efficacy, especially for Type 2 alcoholics.)

30
Najavits’ Treatment Seeking Safety
• Safety has highest priority in the treatment.
• Safety is “abstinence from all substances, reduction in self-destructive behavior, establishment of a network of supportive people, and self-protection from dangers associated with the disorders” (Najavitz, 1998)

31
Seeking Safety (2)• Designed for integrated treatment of PTSD and SUD• Theme is to establish safety from substances, dangerous relationships, and
extreme symptoms (e.g. suicidality)• Can use in group or individual therapy sessions• Cognitive behavioral approach to develop skills to cope with stress also
includes psychoeducation• Present focus• Very popular in the Veterans Health Administration• Uses treatment manual and handouts• 25 modules in 4 content areas :
– Cognitive– Behavioral– Interpersonal– Case Management

32
Seeking Safety (3)
• Flexible—Use relevant modules and can vary order• Structured sessions for modules—check-in, quotation
to emotionally engage clients, reflect on and comment on relevant handouts/practice skills, check-out asking what clients got out of session and what commitment they are willing to make.
• Positive, compassionate tone and positive interactions among clients
• Can use with other treatments• Website: www.seekingsafety.org

33
Recommendations for Treatment of SUD in Veterans with PTSD
(Based on Findings of Subject Matter Expert Panel in November, 2009)
• Treatments for the two conditions should be coordinated and generally the treatments should be done simultaneously. There should be a single treatment plan.
• The VA-DoD Clinical Practice Guidelines should be followed for each condition.
• A community of practice for SUD-PTSD specialists should be created.
• Patients should be regularly monitored to ensure that the treatment plan is responsive to their needs.
• Family involvement can be very helpful to the treatment of both conditions.
• The Clinical Recommendations of the Panel should be revisited/ revised on the basis of new research and the actual experiences of the SUD-PTSD specialists.

34
Issues in Treating SUD in OEF/OIF/OND Veterans (1)
• Assessment should include both conditions. Systematic screening for PTSD in SUD programs results in four times as many patients being diagnosed with comorbid PTSD
• Establish solid working alliance.• Use term “warzone stress” rather than “combat
stress.”• “Normalize” reactions of Veteran and emphasize self
efficacy and hope. • Encourage relationships with other Veterans.
Encourage involvement with Vet Centers

35
Issues in Treating SUD in OEF/OIF/OND Veterans (2)
• Distinguish developmentally-related aspects of substance abuse from risk of chronic dependence and effects.
• Computerized aids to enhance SUD services.
• Integrate services to address complexity of problems - combinations of SUD with traumatic brain injury, chronic pain, homelessness, PTSD, nicotine dependence, community/family readjustment.
• Reduce concerns over confidentiality.

36
Some Good Assessment Questions for OEF/OIF/OND Veterans
1. Why did you join the Army, Marine Corps, Navy, etc.? What did you hope to accomplish?
2. Combat tours – Number? When? Where? Military job? Duties in combat zone?
3. Satisfaction with training and deployment preparation
4. Satisfaction with leadership and equipment
5. How do family members feel about the military?

37
Eligibility for VA Care

38
Who is Eligible for VA Health Care Benefits?
• Served in the Active military and discharged or released under conditions other than dishonorable
• Former Reservists may be eligible if they served full-time and for operational or support (excludes training) purposes
• Former National Guard members may be eligible if they were mobilized by a Federal order

39
Minimum Duty Requirements
• Persons enlisting in the Armed Forces after 9/7/80 or who entered on active duty after 10/16/81 are not eligible for VHA benefits unless they completed:
– 24 months continuous active service, or
– the full period for which they were called or ordered to active duty

40
Excluded from the Minimum Duty Requirements
Minimum active duty requirements do not apply to persons discharged or released from active duty for:
– Early out
– Hardship
– Disability that was incurred or aggravated in line of duty or Veterans with compensable service-connected disability

41
Combat Veteran (CV) Authority• Title 38, U.S.C., Section 1710(e)(1)(D) gave authority to
provide hospital, medical and nursing home care to Combat Veterans despite insufficient medical evidence to conclude that the condition is attributable to such service.
• Veterans who served on active duty in a theater of combat operations during a period of war after the Persian Gulf War or in combat against a hostile force during a period of hostilities after November 11, 1998.
• The National Defense Authorization Act of 2008 extended the period in which a combat-theater Veteran may enroll for VA health care and services to five years post discharge/release date. (Please note that this includes Reserve and National Guard Personnel mobilized for Operation Enduring Freedom (OEF), Operation Iraqi Freedom (OIF) and Operation New Dawn (OND).)

42
Combat Veteran Eligibility DefinitionsCombat Zones Designated by an Executive Order from the President as areas in which the U.S. Armed Forces are engaging or have engaged in combat.
Hostilities Defined as conflict in which the members of the Armed Forces are subjected to danger comparable to the danger to which members of the Armed Forces have been subjected in combat with enemy armed forces during a period of war.
“Hostile Fire or Imminent Danger Pay” Hostile fire pay refers to pay to anyone exposed to hostile fire or mine explosion. Imminent danger pay is paid to anyone on duty outside the United States area who is subject to physical harm or imminent danger due to wartime conditions, terrorism, civil insurrection, or civil war.

43
Criteria for Combat Veteran Eligibility
• Must first meet the definition of a “Veteran” for VA health care benefits.
• Combat-theater Veterans who are ineligible to enroll for VA care are referred to a Vet Center for readjustment counseling services, if appropriate, or to a community provider to obtain services at the Veteran's expense.
• If a health care emergency exists for an ineligible Veteran, treatment is provided under VA’s humanitarian treatment authority.

44
Beyond Mental Health Diagnosis
Many problems faced by returning combat Veterans and their families are not so much clinical as they are functional:– Work Stress/Unemployment– Educational/Training Needs– Housing Needs– Financial and/or Legal Problems)– Family Issues
• Lack of Social Support• Estrangement• Family Breakup• Kids in trouble

45
Positive Aspects of Deployment
• Foster maturity• Encourage independence• Strengthen family bonds

46
Identifying/Treating Post Deployment Mental Health Problems Among New Combat Veterans and their Families
• OEF/OIF/OND Veterans often seek care outside DoD/VA systems– It is estimated that 50% of those seen in DoD/VA
may also receive part of their care in the community
• Family members are also dealing with deployment-related stress and look for help in the community

47
Recommendations for Community Mental Health Care Providers
• Know something about US military history and about our present military conflicts– Military Culture as a major (yet often invisible)
American subculture– Know the different Service Branches and respect the
difference!
• Know something about DoD and VA– Services, Best practices, Access, Benefits
• Ask each patient if he/she has ever served in the Armed Forces or is close to someone who has

48
Examples of VA Services Relevant for OEF/OIF Veterans
• PTSD Treatment Teams• SUD-PTSD Specialist• Military Sexual Trauma • Homelessness Services• Veterans Justice Outreach Program• Vet Centers• Suicide Prevention Program• Deployment Health Clinics• OEF/OIF Coordinators

49
Frequency of VHA Mental Health Screenings
• At-risk drinking (annual)• Post-traumatic stress disorder (every year for first
five years and once every five years thereafter)• Depression (annual)• Suicide risk (if depression screen is positive)• Military sexual trauma (once)• Traumatic brain injury (once)

50
VHA Care Access Points(As of November 3, 2010)
• 153 medical centers--At least one in each state, Puerto Rico and the District of Columbia
• 951 ambulatory care/community-based outpatient clinics
• 47 residential rehabilitation treatment programs
• 271 Veterans Centers
• Suicide Prevention Hotline:
1-800-273-TALK

51
Key Aspects of VHA Mental Health Care Services
• Recovery Orientation• Evidence-Based Practices and Treatments• Continuum of Care• Integration of Mental Health Services with Each Other and
with Physical Health Care Services• Role of Principal Mental Health Care Provider• Maximal Access to Care• Continuing Care• Measurement-Based Outcome Indicators• Automated Treatment Adjuncts
(e.g. MyHealtheVet)

Prevalence of SUD / PTSD Diagnoses in Veteran Patients in FY 2010
• In FY2010, 5,536,526 patients were seen in VA. Around 7% of these are OEF/OIF Veterans.
• 465,262 Veterans (8.4 %) were diagnosed with SUD. Of these 28% also had PTSD.
• 553,045 Veterans (10 %) were diagnosed with PTSD. Of these 23% also had SUD.

Treatment Services Offered by VA SUD Programs at VA Facilities FY08-FY10 (N=140)
Treatment ServiceFY 2008 % of
FacilitiesFY2010
% of Facilities% Increase
OEF/OIF-specific groups or services
39% 50% 11%
Seeking Safety 58%
71% 13%
Pharmacotherapy and psychosocial intervention for PTSD and SUD 76% 78%
2%

Availability of Evidence-Based SUD Psychotherapy Treatment within General Mental Health Clinics at VHA Facilities (N=140)
Therapy Modalities % of Facilities
Cognitive Behavioral Therapy for Relapse Prevention 57%
12-Step Facilitation 33%
Contingency Management 14%
Seeking Safety 53%
Behavioral Couples/Family Therapy 37%

55
Public Health Model (1)
• Most war fighters/Veterans will not develop a mental illness but all war fighters/Veterans and their families face important readjustment issues
• This population-based approach is less about making diagnoses than about helping individuals and families retain a healthy balance despite the stress of deployment

56
Public Health Model (2)
• Incorporates the Recovery Model and other principles of the President’s New Freedom Commission on Mental Health– There is a difference between having a
problem and being disabled
• The public health approach requires a progressively engaging, phase-appropriate integration of services

57
Public Health Model (3)
• This program must: – Be driven by the needs of the Service
Member/Veteran and his/her family rather than by DoD and VA traditions
– Meet prospective users where they live rather than wait for them to find their way to the right mix of our services
– Increase access and reduce stigma

•Offers each state its own page•Includes VA facilities and Vet Centers•Over 1500 providers nationally• Over 1200 providers in NC including 96 of 100
NC counties• A model for further populating the National
Resource Directory on a state-by-state basis
https://www.nationalresourcedirectory.gov
58

59
http://www.ptsd.va.gov/professional/ptsd101/course-modules/af-am-vets.asp