Embed Size (px)
Citation preview

ABSTRACT
Purpose: To evaluate trends in health service delivery forcataract surgery at the Royal Victorian Eye and Ear Hospital,Melbourne, Australia.
Methods: A retrospective study was conducted of com-puterized hospital admissions for cataract surgery from July1994 through June 1999. Main outcome measures includedthe annual number of cataract surgeries, waiting time,percentage of patients hospitalized overnight, length of over-night hospitalization, type of cataract surgery, surgery duration and total time in the operating theatre.
Results: Although the annual number of patients under-going cataract surgery increased from 3395 to 4796 overthe 5-year study interval, there was a 13-day reduction inmean waiting time for public patients, a 30% reduction inovernight hospitalizations and a half-day reduction in lengthof hospitalization for all patients.There was also an increas-ing trend in use of phacoemulsification cataract extraction.
Conclusions: The health-care delivery for cataract surgeryappears to have improved during the past 5 years at theRoyal Victorian Eye and Ear Hospital.
Key words: Australia, cataract, epidemiology, health servicesresearch.
INTRODUCTION
Cataract is common in older Australians1,2 and cataractextraction is the most frequently performed ophthalmic surgical procedure in Australia.3 The technical aspects andoutcomes related to cataract surgery have been evaluatedmany times, and this procedure has a low rate of complica-tions and a high level of patient satisfaction.4–9 Within thenext 10–15 years, the number of Australians needing
cataract surgery is expected to double, primarily due to theageing of the Australian population.1,3,10
Improving cataract health service delivery is seen asessential to meet the anticipated increased demand forcataract surgery and to limit associated health-care costs.11
Patterns of health service delivery for cataract extractionhave been evaluated in several countries;12–15 however, fewstudies are available for Australia.3,16 To determine if healthservice delivery for cataract surgery is improving, we studiedtrends in cataract surgery at a large Australian ophthalmichospital.
METHODS
The study was conducted at the Royal Victorian Eye and EarHospital (RVEEH), the major ophthalmic tertiary referralhospital in Victoria, Australia. It is also one of the largestprimary training centres for ophthalmologists in Australia.
The RVEEH hospital computerized information system(PICK system) was searched to identify all admissions forcataract surgery that were performed from July 1994 throughJune 1999. The ICD-9-CM17 and ICD-10-AM18 procedurecodes (see Appendix I for list of codes) were used to identifycases. Patients who underwent other surgical procedures inaddition to cataract extraction (e.g. trabeculectomy) wereexcluded from this study.
Patient admissions were categorized as public, private orVeterans’ Affairs (VA) according to the patient’s paymentclassification. Surgery waiting time was defined as thenumber of days that elapsed from the date the patient wasplaced on the elective surgery waiting list until the date ofsurgery. Waiting times and operating times were definedconsistently over the study period. Continuous variableswere analysed to determine if they were normally distrib-uted. A square root transformation was applied to two variables (waiting time and length of stay) to make themnormally distributed and geometric means are presented forthese variables. χ2 tests were used to assess changes in
Clinical and Experimental Ophthalmology (2001) 29, 291–295
Original Article
Trends in health service delivery for cataract surgery at alarge Australian ophthalmic hospitalQing Yi MB MPH,1 Sandra J Flanagan DIT2 and Daniel J McCarty PhD1
1Centre for Eye Research Australia, Department of Ophthalmology, University of Melbourne and 2Royal Victorian Eye and Ear Hospital,Melbourne, Victoria, Australia
� Correspondence: Dr Qing Yi, Centre for Eye Research Australia, Royal Victorian Eye and Ear Hospital, 32 Gisborne Street, East Melbourne, VIC 3002,
Australia. Email: [email protected]

proportions over time and 95% confidence intervals (CI)were calculated for means and proportions.19 SPSS forWindows (release 9.0.1; SPSS, Chicago, IL, USA) was usedfor statistical analyses.
The validity of the computerized admissions data wasevaluated by comparing these data with results from anindependent review of 600 medical records.16 Variables evaluated included patient age, sex, postcode, payment classification, admission date, surgery date, percentage ofovernight hospital admissions, length of hospital stay, andtype of cataract procedure. For the 600 patients, there wasexcellent agreement between the two methods of data collection (percentage agreement ranged from 96.1% forpayment classification to 99.6% for sex).
RESULTS
A total of 23 512 admissions were identified from the hospi-tal computerized information system. Of these, 1950 (8.3%)admissions had another procedure in addition to cataractsurgery and 341 (1.5%) admissions had their cataractsurgery cancelled. Therefore, further analysis was restrictedto 21 221 admissions (18 220 patients).
A review of patient characteristics (Table 1) shows littlechange over the study interval in the mean age of patientsand the percentage of female patients. There was a slightdecrease in the percentage of rural patients (from 14.3% in1994 to 11.2% in 1998; χ2 = 44.391, d.f. = 4, P < 0.01).
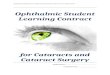
The number of public and private patients increased by51% and 59%, respectively, but the number of VA patientsdecreased by 23% (Fig. 1a). The overall mean waiting timewas significantly shorter for private patients (14.1 days, 95% CI = 13.7–14.5) and VA patients (14.7 days, 95%CI = 14.2–15.3) compared with public patients (92.3 days,95% CI = 91.2–93.5; Fig. 1b). There was a 13-day reductionin mean waiting time for public patients, from 94.0 days(95% CI = 91.1–97.0) to 80.8 days (95% CI = 78.9–82.7).There was no significant change in waiting time for privateand VA patients.
Over the study period, the percentage of overnight hospitalizations decreased by 29.0% in public patients(χ2 = 759.8, d.f. = 4, P < 0.01), 33.5% in private patients(χ2 = 364.2, d.f. = 4, P < 0.01), and 29.7% in VA patients(χ2 = 146.3, d.f. = 4, P < 0.01). In 1998, 27.5% of publicpatients, 29.5% of private patients, and 42.0% of VApatients were hospitalized overnight (Fig. 1c).
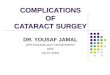
There was an increasing trend in use of phacoemulsifica-tion cataract extraction (PKE). In 1994, PKE was used in
55.6% of public, 55.9% of private and 74.6% of VA cataractsurgeries. By 1998, 90.5% of public patients, 95.6% ofprivate patients, and 97.0% of VA patients had PKE surgery(Fig. 2a).
A reduction in surgery time was observed over the studyperiod and this was strongly related to the procedure forcataract removal (PKE vs extracapsular cataract extraction[ECCE]). Among PKE cases, duration of surgery decreasedfor public patients (47 min to 35 min), private patients(40 min to 28 min) and VA patients (33 min to 26 min;
292 Yi et al.
Table 1. Characteristics of patients undergoing cataract surgery at the Royal Victorian Eye and Ear Hospital by financial year
Characteristic 1994 1995 1996 1997 1998 Total
Admissions (n) 3395 3826 4395 4836 4796 21 221Mean ± SD age (years) 72.9 ± 11.7 73.9 ± 11.1 73.5 ± 10.6 73.7 ± 10.7 73.6 ± 10.7 73.5 ± 10.9Female (%) 56.4 58.9 58.3 58.7 59.0 58.4Rural (%) 14.3 15.7 14.8 13.5 11.2 13.8
Figure 1. Patient classification and trends in (a) the annualnumber of cataract surgeries; (b) mean waiting time; and (c) percentage of patients who were hospitalized overnight. 95% confidence intervals are presented. ( ) Public; (— — —)private; ( ) Veterans’ Affairs.

Fig. 2b). Overall for PKE-treated eyes there was an 11 minreduction (95% CI 9–11) in surgery duration (from 43 minin 1994 to 32 min in 1998). Among patients who had ECCE,surgery duration remained fairly constant over the studyperiod.
Total patient time in theatre for PKE-treated patients alsodecreased. It decreased most in public patients from 211 min(95% CI = 206–216) in 1994 to 171 min (95% CI = 168–175)in 1998 (Fig. 2c).
Among patients who were hospitalized overnight, the per-centage of patients admitted the day before surgery droppedin public patients from 52.2% to 19.4% (χ2 = 438.3, d.f. = 4,P < 0.01), in private patients from 32.6% to 5.6% (χ2 = 175.0,d.f. = 4, P < 0.01), and in VA patients from 36.9% to 1.0%(χ2 = 194.1, d.f. = 4, P < 0.01; Fig. 3a). There was also a sig-nificant reduction in the length of stay (1.6 days to 1.2 daysin public patients, 1.3 days to 1.1 days in private patients,and 1.4 days to 1.0 days in VA patients) among patients whowere hospitalized overnight (Fig. 3b).
DISCUSSION
This study shows that despite increasing numbers of patientsundergoing cataract surgery annually at the RVEEH, therewere decreasing trends in patients’ waiting time, overnighthospitalization and length of hospitalization. There was alsoa significant change in the procedure used to extract cataractwith a marked increase in the use of PKE. During the last5 years, the number of operating theatres and the number ofsurgeons at the RVEEH have remained constant. Therefore,results from this study suggest that the efficiency of healthservice delivery for cataract has improved.
In recent years, similar trends of increasing need forcataract surgery, sharp rise of PKE, shorter length of hospi-talization and increasing proportion of day surgery have alsobeen demonstrated in other countries.13–15 In England,Dunn et al. suggested that public patients consider waitingtime for cataract surgery of 3 months or less as acceptable,and waits exceeding 6 months to be excessive.20 The samedefinition of waiting time has been used in a national studyto identify patients’ access to cataract surgery in 1990 in theUK.12 In this study, the median waiting time was 144 days,with 30% of patients waiting less than 90 days, and 43% ofpatients waiting more than 180 days. In the present study,the mean waiting time for public patients was 94 days (3.1months) in 1994, with 48% of patients waiting less than 3months and 13% waiting more than 6 months. By 1999, themean waiting time had dropped to 80 days (2.6 months),with 58% of patients waiting less than 3 months and only
Health service delivery for cataract surgery 293
Figure 2. Patient classification and trends in (a) the use of phaco-emulsification cataract extraction (PKE) procedure; (b) mean dura-tion of PKE surgery; and (c) mean duration of time in theatre ofPKE surgery. 95% confidence intervals are presented. ( ) Public;(— — —) private; ( ) Veterans’ Affairs.
Figure 3. Patient classification and trends in (a) the percentage ofpatients admitted the day before surgery; and (b) mean length ofstay. Data shown are for patients who were hospitalized overnight.95% confidence intervals are presented. ( ) Public; (— — —)private; ( ) Veterans’ Affairs.

5% of patients waiting more than 6 months. Our resultscompare favourably to the UK data; however, differences instudy periods and methodologies make comparisons amongstudies difficult.
The differences in mean waiting time among public,private and VA patients should be cautiously interpreted.Booking for a public cataract surgery session usually occursshortly after diagnosis of a cataract requiring removal.However, scheduling private and VA patients in theatre ismore flexible and can occur longer after diagnosis depend-ing on the availability of a time during private surgery ses-sions. Therefore, the recorded waiting time for private andVA patients may not reflect actual waiting time.
The majority of cataract surgery (70%) at the RVEEHinvolves ambulatory admissions (day surgeries). Ambulatorycare has been shown to be safe and cost-effective forcataract surgery in patients without significant comorbidi-ties.21,22 We recently reported that only 2.0% of patientsrequiring overnight hospitalization at the RVEEH receivedan active medical intervention. Furthermore, the mainfactors associated with overnight stay were country residenceand the lack of a carer at home.16 Given these data, it maybe possible to further reduce the percentage of patients whoare hospitalized overnight without compromising level ofcare. This might be achieved by ensuring that cataractsurgery is available at regional medical centres or alterna-tively providing for overnight accommodation in nearbymotels as an alternative to hospitalization.23
Finally, PKE appears to be a major factor in the increasein efficiency of cataract service delivery. Currently, morethan 90% of cataract surgeries at the RVEEH are performedunder local anaesthesia with PKE, a technically moreadvanced procedure than ECCE.6,7 The combination of localanaesthesia with PKE procedure appears to have resulted inreduced theatre times and increased rates of ambulatory surgeries.24,25
In conclusion, this study shows improvements in health-care delivery for cataract surgery at a large Australian oph-thalmic hospital. Clinical outcomes such as surgery compli-cations, final postoperative visual acuity and patients’functional improvements were not measured in this study.Continued monitoring of cataract health service delivery isimportant to meet the anticipated increased demand forcataract surgery and to limit associated health-care costs.However, clinical outcomes from cataract surgery will alsohave to be monitored to ensure quality is not sacrificed forincreased efficiency.
REFERENCES
1. McCarty CA, Mukesh BN, Fu CL, Taylor HR. The epidemiol-ogy of cataract in Australia. Am. J. Ophthalmol. 1999; 128:446–65.
2. Mitchell P, Cumming RG, Attebo K, Panchapakesan J.Prevalence of cataract in Australia: The Blue Mountains EyeStudy. Ophthalmology 1997; 104: 581–8.
3. Keeffe JE, Taylor HR. Cataract surgery in Australia 1985–1994.Aust. N.Z. J. Ophthalmol. 1996; 24: 313–17.
4. Mangione CM, Phillips RS, Lawrence MG, Seddon JM, Orav EJ, Goldman L. Improved visual function and attenu-ation of declines in health-related quality of life after cataractextraction. Arch. Ophthalmol. 1994; 112: 1419–25.
5. Desai P, Reidy A, Minassian DC, Vafidis G, Bolger J. Gainsfrom cataract surgery. visual function and quality of life. Br. J.Ophthalmol. 1996; 80: 868–73.
6. Ohrloff C, Zubcov AA. Comparison of phacoemulsificationand planned extracapsular extraction. Ophthalmologica 1997;211: 8–12.
7. Chang-Godinich A, Ou RJ, Koch DD. Functional improve-ment after phacoemulsification cataract surgery. J. CataractRefract. Surg. 1999; 25: 1226–31.
8. Desai P, Minassian DC, Reidy A. National cataract surgerysurvey 1997–8. A report of the results of the clinical outcomes.Br. J. Ophthalmol. 1999; 83: 1336–40.
9. McCarty CA, Nanjan MB, Taylor HR. Operated and unoper-ated cataract in Australia. Clin. Exp. Ophthalmol. 2000; 28: 77–82.
10. McCarty CA, Keeffe JE, Taylor HR. The need for cataractsurgery: projections based on lens opacity, visual acuity, andpersonal concern. Br. J. Ophthalmol. 1999; 83: 62–5.
11. Wormald R. Cataract surgery – quantity and quality. Br. J.Ophthalmol. 1999; 83: 889–90.
12. Courtney P. The national cataract surgery survey: I. Methodand descriptive features. Eye 1992; 6: 487–92.
13. Hansen TE. Current trends in cataract surgery in Denmark –1997 survey. Acta Ophthalmol. Scand. 1998; 76: 707–10.
14. Oshika T, Amano S, Araie M, Majima Y, Leaming DV. Currenttrends in cataract and refractive surgery in Japan: 1997 survey.Jpn. J. Ophthalmol. 1999; 43: 139–47.
15. Lee SY, Tan D. Changing trends in cataract surgery inSingapore. Singapore Med. J. 1999; 40: 256–9.
16. Atalla ML, Wells KK, Peucker N, Yi Q, McCarty DJ, Louis D,Taylor HR. Cataract extraction in a major ophthalmic hospi-tal: day case or overnight stay? Clin. Exp. Ophthalmol. 2000; 28:83–8.
17. National Coding Centre. The Australian Version of The InternationalClassification of Diseases 9th Revision Clinical Modification (ICD-9-CM), Vol. 3, 2nd edn. Sydney: National Coding Centre, 1996.
18. National Centre for Classification in Health. The InternationalStatistical Classification of Diseases, Related Health Problems, 10thRevision Australian Modification (ICD-10-AM), Vol. 3, 1st edn.Sydney: National Centre for Classification in Health, 1998.
19. Fleiss JL. Statistical Methods for Rates and Proportions, 2nd edn.New York: John Wiley and Sons, 1981; 138–43.
20. Dunn E, Black C, Alonso J, Norregaard JC, Anderson GF.Patients’ acceptance of waiting for cataract surgery: whatmakes a wait too long? Soc. Sci. Med. 1997; 44: 1603–10.
21. Strong NP, Wigmore W, Smithson S, Rhodes S, Woodruff G,Rosenthal AR. Daycase cataract surgery. Br. J. Ophthalmol.1991; 75: 731–3.
22. Fan YP, Boldy D, Bowen D. Comparing patient satisfaction,outcomes and costs between cataract day surgery and inpatientsurgery for elderly people. Aust. Health Rev. 1997; 20: 27–39.
23. La Nauze J. Cataract, the community and care: are we pre-pared? Clin. Exp. Ophthalmol. 2000; 28: 75.
24. Sindhu K, Colrain I, Buttery R, Gordon W. A survey of localanaesthesia use in cataract surgery in Australia. Aust. N.Z. J.Ophthalmol. 1991; 19: 43–8.
25. Bellucci R. Anesthesia for cataract surgery. Curr. Opin.Ophthalmol. 1999; 10: 36–41.
294 Yi et al.

APPENDIX I
List of codes used to identify cases
ICD-9-CM codes17
13.11, 13.19, 13.2, 13.3, 13.41, 13.42, 13.43, 13.51, 13.69,13.59, 13.71.
ICD-10-AM codes18
42698–00, 42698–01, 42698–02, 42698–03, 42698–04,42698–05, 42702–00, 42702–01, 42702–02, 42702–03,42702–04, 42702–05, 42702–06, 42702–07, 42702–08,42702–09, 42702–10, 42702–11, 42716–00.
Health service delivery for cataract surgery 295