Embed Size (px)
Citation preview

MAIN RESEARCH ARTICLE
Trends in live births in the past 20 years in Zhengzhou, ChinaWEI HAN1, JIANGANG SONG1, AIQING LIU2,3, KAIMING HUO1, FALIN XU1,4, SHIHONG CUI2,3,XIAOYANG WANG1,4,5 & CHANGLIAN ZHU1,4
1Department of Pediatrics and 2Department of Obstetrics and Gynecology, the Third Affiliated Hospital of ZhengzhouUniversity, Zhengzhou, 3Department of Obstetrics and Gynecology, Henan Provincial Women and Children’s Hospital,Zhengzhou, 4Key Laboratory for Neonatal Brain Injury of Henan, Zhengzhou, China, and 5Perinatal Center, SahlgrenskaAcademy, University of Gothenburg, Gothenburg, Sweden
Key wordsAsphyxia, cesarean, neonatal death, pretermbirth, risk factor
CorrespondenceChanglian Zhu, MD, PhD, Professor ofPediatrics, Department of Pediatrics,the Third Affiliated Hospital of ZhengzhouUniversity, Kangfuqain Street 7,Zhengzhou 450052, China.E-mail: [email protected]
Conflict of interestThe authors have stated explicitly that thereare no conflicts of interest in connection withthis article.
Received: 9 June 2010Accepted: 18 December 2010
DOI: 10.1111/j.1600-0412.2010.01065.x
Abstract
Objective. To evaluate changing trends in neonatal births and deaths in a provin-cial women’s and children’s hospital over the past 20 years. Design: Retrospectivelongitudinal study. Setting. Henan Provincial Women’s and Children’s Hospital,China. Population. Live births in Henan Provincial Women’s and Children’s Hospi-tal from January 1987 to December 2006. Methods: Data was stratified by sex, birthweight, delivery type, maternal age, gestational age, and single or multiple births.The incidence of low Apgar scores and neonatal death was calculated for each fiscalyear. Main outcome measures: Trends in the fundamental status of hospital-born livebirths and risk factors for neonatal death. Results. 26 760 hospital live births were in-cluded. The ratio of males to females was 1.16:1. The mean gestational age decreasedfrom 39.5±1.4 weeks to 38.4±2.5 weeks (p <0.001) and multiple births increasedfrom 1.5 to 7.3% (p<0.001). The proportion of preterm births increased from 4.7to 18.9% (p<0.001), maternal age increased from 25.9±3.7 years to 29.0±4.4 years(p<0.001), and cesarean deliveries increased from 23.7 to 65.5% (p<0.001). Theincidence of low Apgar scores decreased from 12.9 to 1.1% (p<0.001). The inci-dence of neonatal death was 8.5/1 000 live births, with preterm births and low Apgarscores accounting for 72.8 and 16.2% of all neonatal deaths, respectively. Conclu-sion. Preterm births, multiple births, and cesarean deliveries increased dramatically.Preterm birth is the leading cause of neonatal death.
Introduction
Great progress has been made in improving child survivaland health globally due to improvements in socioeconomics,education, and healthcare conditions. However, of the 130million infants born every year worldwide, about 4 milliondie in the neonatal period (1), which constitutes over 40% ofall deaths in children under 5 years of age (2). Furthermore,about 75% of neonatal deaths happen in the early neonatalperiod (1). Reducing neonatal mortality is critical for reach-ing the Millennium development goal.
China has made great progress in child health in the pastfew decades. The infant mortality rate declined from 37/1 000live births in 1990 to 20/1 000 live births in 2006, and the mor-tality rate in children younger than 5 years of age decreasedfrom 46/1 000 live births to 24/1 000 live births during thatperiod (3). The incidence of hospitalized delivery increased
from 43.7% in 1985 to 88.4% in 2006 (4). There are approxi-mately 16 million infants born in China every year, of whichabout 1 million are born in Henan province, which has amortality rate of 7.45/1 000 live births (5). In China, the ma-ternity and child health care systems across the country areorganized in three vertical levels: community, county, andcity. There is one provincial women’s and children’s hospitalin each province that represents the top level of perinatal andneonatal health care in the province and takes the responsi-bility of training doctors and handling severe or complicatedcases.
Perinatal mortality is reduced by improvements in obstet-ric and neonatal care (6), although it is still much higher inChina than in high-income countries (7). To further reduceneonatal deaths, it is essential to know the current status oflive births and the main causes of neonatal death. Henanis an agricultural province located in central China with
332c© 2011 The Authors
Acta Obstetricia et Gynecologica Scandinavica c© 2011 Nordic Federation of Societies of Obstetrics and Gynecology 90 (2011) 332–337
A C TA Obstetricia et Gynecologica

W. Han et al. Trends in live birth in Zhengzhou, China
98 million inhabitants. The average mortality rate, annualfamily income, and health expenditure in 2007 were verysimilar in Henan province to the average level for the wholecountry. Henan may thus represent the general healthcaresituation in China. The changes regarding births in this hos-pital could therefore help with understanding the recent ten-dencies with regard to deliveries in China. The aim of thisretrospective longitudinal study was to analyze the funda-mental status of hospital-born live children and the causesof neonatal death in this representative provincial maternaland child health care hospital over a 20-year period, and toprovide information for reducing neonatal deaths.
Material and methods
All data on live births came from the discharge databaseof Henan Provincial Women’s and Children’s Hospital fromJanuary 1987 to December 2006. Stillbirths and newbornsdelivered at other hospitals but transferred to the provin-cial hospital were not included. A live birth was defined asa newborn, whatever its gestational age, being delivered andshowing any sign of life. Stillbirth refers to any fetus of at least20 weeks’ gestational age who died in the uterus during laboror delivery. The data collected included sex, birth weight, ges-tational age, single or multiple births, maternal age, and deliv-ery type, and were calculated for each fiscal year. Gestationalage was estimated from the last menstrual period or by ultra-sound. Newborns were defined according to gestational ageas preterm (<37 weeks), term (37–42 weeks), and postterm(>42 weeks); or according to birth weight as very low birthweight (<1 500 g), low birth weight (1 500–2 500 g), normalbirth weight (2 500–4 000 g), and macrosomia (>4 000 g).Delivery modes were divided into natural labor, cesarean sec-tion, and assisted delivery.
Asphyxia was defined by Apgar scores: a score <7 at1 minute was defined as low; scores of 4–7 were definedas moderately low, and scores of 0–3 and depression at birthrequiring resuscitation with a mask and/or intubation weredefined as severely low. The annual incidence of low Apgarscores was calculated as the number of newborns with lowApgar scores divided by the total number of term infants. Casefatality rate was defined as the percentage of infants who hadlow Apgar scores and died before hospital discharge.
Statistical analysis
Trends in ratios and incidence rates were analyzed using thechi-squared test. Spearman’s rank relational coefficient wasused to analyze changes in birth weight, gestational age, andmaternal age. Low Apgar score incidence rates, stratified bygender, birth weight, delivery mode, maternal age, and mul-tiple births, were compared by calculating relative risk (RR)and the 95% confidence interval (CI) using univariate analy-sis. Multivariate RRs and 95%CIs were calculated by includ-
ing these variables in a logistic regression model. Case fatalityrates were similarly compared in univariate and multivariateanalyses. A value of p<0.05 was designated as the level of sig-nificance, and spss statistical software version 11.0 (Chicago,IL, USA) was used for analysis.
Results
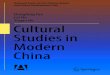
There were 26 760 live births between 1987 and 2006 inHenan Provincial Women’s and Children’s Hospital, consist-ing of 25 776 singleton, 866 twin and 118 triplet and higherorder pregnancies. Of these, 14 395 (53.8%) were male and12 365 (46.2%) female, with a mean male:female ratio of1.16:1 (range 1.03:1–1.33:1). The average birth weight was3 190±456 g for all newborns, 3 204±465 g for males, and3 174±446 g for females. The average birth weight decreasedfrom 3 227±281 g for males and 3 268±428 g for females in1987 to 3 051±618 g for males (p<0.001) and 3 027±618 gfor females (p<0.001) in 2006. The proportion of low birthweight and very low birth weight newborns increased, respec-tively, from 3.71 and 0.42% in 1987 to 11.67 (p=0.001) and4.22% (p<0.001) in 2006, respectively, while normal birthweight or macrosomia decreased (p<0.001). The percentageof preterm births rose steadily over the past two decades,from 4.7% in 1987 to 18.9% in 2006 (p<0.001), while therates of term and post-term infants decreased, respectively,from 89.3 and 6.0% in 1987 to 80.9 and 0.2% in 2006(Figure 1a). Gestational age decreased from 39.5±1.4 weeksin 1987 to 38.4±2.5 weeks in 2006 (p<0.001) (Figure 1b).At the same time, the twinning and triplet (including higherorder) rate tended to increase gradually from 1.5% in 1987to 7.3% in 2006 (p<0.001) (Figure 1c).
The average maternal age was 27.2±3.8 years during thestudy period and climbed from 25.9±3.7 in 1987 to 29.0±4.4in 2006 (p<0.001) (Figure 1d). The modes of delivery alsochanged dramatically during this period. Cesarean sectiondelivery increased sharply from 23.7% in 1987 to 65.5% in2006 (p<0.001), and by 1998 was the primary mode of de-livery (Figure 1e). The rate of cesarean section without indi-cation was 18.7% in 2001–2006. The percentage of inducedlabor decreased from 3.7 to 1.7% (p<0.001) (Figure 1f).
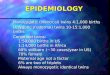
A total of 23 914 (89.4%) newborns were identified as termbabies, of whom 1 405 had low Apgar scores at birth, an in-cidence of 5.9%. Among newborns with low Apgar scores,1 193 cases (84.9%) were identified as “moderate” and 212cases (15.1%) as “severe”. The annual incidence of low Ap-gar scores in term infants decreased from 12.9% in 1987to 1.1% in 2006 (p<0.001) (Figure 2). Further analysis re-vealed that low Apgar scores occurred more frequently inmales (817/12 804, 6.4%) than in females (588/11 110, 5.3%)(RR=1.2, 95% CI 1.1–1.4, p<0.001) (Table 1). Term infantswith low birth weights were at higher risk for low Apgar scores(RR=3.1, 95% CI: 2.4–4.1, p<0.001) (Table 1). Cesarean
c© 2011 The AuthorsActa Obstetricia et Gynecologica Scandinavica c© 2011 Nordic Federation of Societies of Obstetrics and Gynecology 90 (2011) 332–337 333

Trends in live birth in Zhengzhou, China W. Han et al.
35
37
39
41
43
45
19861988199019921994199619982000200220042006
0
5
10
15
20
25
1987 1989 1991 1993 1995 1997 1999 2001 2003 2005
Pe
rce
nta
ge
of
pre
term
bir
th
Ge
sta
tio
na
l a
ge
(w
ee
ks
)
0
20
40
60
80
100
1987 1989 1991 1993 1995 1997 1999 2001 2003 2005
Ce
sa
rea
n d
eli
ve
ry (
%)
15
20
25
30
35
40
19861988199019921994199619982000200220042006
0
1
2
3
4
5
6
1987 1989 1991 1993 1995 1997 1999 2001 2003 2005
Pe
rce
nta
ge
of
ind
uc
ed
la
bo
r
0
3
6
9
12
15
1987 1989 1991 1993 1995 1997 1999 2001 2003 2005
Ttw
in /m
ult
iple
bir
ths
(%
)
Ma
tern
al a
ge
(ye
ars
)
Figure 1. Dynamic changes in live birthprofiles 1987–2006. a) The percentage ofpreterm births fluctuated between 1987and 1999, and increased gradually after1999. b) Gestational age decreased after2000. c) The proportion of twin /multiplebirths increased from 2001. d) Maternalage increased gradually from 1995. e) Theproportion of cesarean deliveries increasedfrom 1994 and remained at more than50% after 1998. f) The percentage ofinduced labor fluctuated between 1987and 2003, and decreased gradually after2003.
Pe
rce
nta
ge
of
low
ap
ga
r s
co
res
0
5
10
15
20
1987 1989 1991 1993 1995 1997 1999 2001 2003 2005
Term low Apgar scores
Figure 2. Incidence of term birth low Apgar scores by fiscal year,1987–2006.
section was not related to the incidence of low Apgar scores(p=0.14); however, a higher incidence of low Apgar scoreswas related to assisted delivery (RR=2.6, 95% CI: 2.4–2.9,p<0.001) (Table 1). Maternal age and multiple births werenot related to an increased risk of low Apgar scores.
In all, 228 hospital-born neonates died in the past 20 yearsin the hospital, a mortality rate of 8.5/1 000 live births. The an-nual newborn mortality rate was 11/1 000 live births in 1987and reached its highest level in 1989 at 30/1 000 live births.
From 1989 to 2004, it fluctuated between 3 and 15/1 000 livebirths (Figure 3). The ratio of preterm deaths was 76.9% in1987, with the lowest level appearing in 1994 (16.7%). Al-though preterm deaths accounted for a large proportion ofoverall deaths, preterm mortality decreased during the past20 years (p<0.001).
The death rate in term infants with low Apgar scoreswas 2.63% and remained unchanged over the past 20 years(p=0.612). Low Apgar scores were the second leading cause,accounting for 16.2% of total neonatal deaths in this study.Neonates with low birth weight had a fivefold (95% CI:2.1–11.8, p<0.001) increased risk of death before dischargecompared with newborns who weighed >2 500 g (Table 2).Sex and the mode of delivery, which were related to theincidence of low Apgar scores, were not related to fatality(Table 2).
Discussion
In this retrospective investigation, we found that the ratioof males to females slightly favored males at an average ra-tio of 1.16:1, which was similar to the Chinese populationcensus results (1.19:1) from the same period (8). The latest
334c© 2011 The Authors
Acta Obstetricia et Gynecologica Scandinavica c© 2011 Nordic Federation of Societies of Obstetrics and Gynecology 90 (2011) 332–337

W. Han et al. Trends in live birth in Zhengzhou, China
Table 1. Risk factors for term low Apgar scores.
n/N (%) Univariate Adjusted∗
RR 95% CI P-value RR 95% CI p-value
GenderFemale 588/11 110 (5.3) 1.0Male 817/12 804 (6.4) 1.2 1.1–1.4 <0.001 1.2 1.1–1.4 <0.001
Birth weight2 500 g–4 000 g 1274/22 193 (5.7) 1.0<2 500 g 73/495 (14.7) 2.8 2.2–3.7 <0.001 3.1 2.4–4.1 <0.001>4 000 g 58/1226 (4.7) 0.8 0.6–1.1 0.14 0.9 0.8–1.0 0.15
Delivery modeNatural labor 589/11 543 (5.1) 1.0Cesarean section 520/11 295 (4.6) 0.9 0.8–1.0 0.08 0.9 0.8–1.0 0.14Assisted delivery 296/1 076 (27.5) 7.1 6.0–8.3 <0.001 2.6 2.4–2.9 <0.001
Maternal age≤35 years 1357/23 163 (5.9) 1.0>35 years 48/751 (6.4) 1.1 0.8–1.5 0.53 1.0 0.8–1.4 0.86
Multiple birthsSingle 1385/23 594 (5.9) 1.0Twin/multiple 20/320 (6.3) 1.1 0.7–1.7 0.80 1.6 1.0–2.5 0.06
∗Multivariate RRs are adjusted for gender, birth weight, delivery mode, maternal age, and multiple births.n, death number of term infants with low Apgar score; N, total number of term infants with low Apgar score.
0
20
40
60
80
100
1987 1989 1991 1993 1995 1997 1999 2001 2003 2005Ne
on
ata
l d
ea
ths
/ 1
00
0 liv
e b
irth
s
Figure 3. Incidence of neonatal deaths by fiscal year 1987–2006.
report showed the ratio of males to females is 1.23:1 (9).The imbalance of sex ratio is a potential problem in China,which is likely related to the one-child policy, illegal prenatalscreening, and sex-selective abortion (8).
We found a recent, dramatic increase in preterm births,similar to another report from China (10). Preterm birthhas been the main cause of neonatal death since 1999, inkeeping with the situation in high-income countries (1,11).Previous studies demonstrated that assisted reproduction,maternal and neonatal complications, and antenatal smok-ing can increase the risk of preterm delivery (11). We foundthat multifetal pregnancy increased the risk of preterm de-livery, which is approximately 3.6 times the risk associatedwith singleton pregnancy (p<0.001, data not shown). Fur-thermore, more severe and complicated maternal cases trans-
ferred to the hospital may be one reason for a high rate ofpreterm births. Preterm infants have higher mortality ratescompared with term infants (6) and an increased incidenceof preterm births may have influenced the overall neonatalmortality rate. The multiple birth rate increased graduallyand was much higher than figures released previously (12).Fertility treatments such as in vitro fertilization or other as-sisted reproductive therapies may contribute to the increaseof multiple births (13). In this study, we found that maternalage (RR=1.7, p<0.01) (data not shown) was a risk factor ofmultiple births, which is likely related to assisted reproductivetreatment. In vitro fertilization has been strictly controlled bythe national health department and was approved for clinicalapplication in 1999 in a few provincial or university hospitalsin Henan Province, which was coincident with the increasein multiple births.
WHO has recommended an optimal cesarean section rateof around 5–10%, and rates exceeding 15% seem to be moreharmful (14). In this investigation, the rate of cesarean sectionsharply increased from 23.7 to 65.5% with a mean cesareanrate of 48.9%, far exceeding the level set by WHO and slightlyhigher than the survey results from WHO (46.2%) (15). Therate of cesarean section without indication was also high(18.7%) during 2001–2006, which indicates that many preg-nant women asked for a cesarean birth although they metthe criteria for natural birth. The reasons for the high ratioof cesarean section are complex; increasing maternal age andmultiple births (as indicated in this investigation) are someof the causes. However, the one-child policy may have an
c© 2011 The AuthorsActa Obstetricia et Gynecologica Scandinavica c© 2011 Nordic Federation of Societies of Obstetrics and Gynecology 90 (2011) 332–337 335

Trends in live birth in Zhengzhou, China W. Han et al.
Table 2. Risk factors for case fatality.
n/N (%) Univariate Adjusted∗
RR 95% CI p-value RR 95% CI p-value
GenderFemale 15/588 (2.6) 1.0Male 22/817 (2.7) 1.1 0.5–2.1 0.87 1.2 0.6–2.3 0.65
Birth weight>2500 g 29/1332 (2.2) 1.0<2500 g 8/73 (11.0) 5.5 2.4–12.6 <0.001 5.0 2.1–11.8 <0.001
Delivery modeNatural labor 12/589 (2.0) 1.0Cesarean Section 18/520 (3.5) 1.7 0.8–3.6 0.15 1.6 0.8–3.5 0.20Assist delivery 7/296 (2.4) 1.2 0.5–3.0 0.75 1.1 0.7–1.8 0.65
Maternal age≤35 years 35/1 357 (2.6) 1.0>35 years 2/48 (4.2) 1.6 0.4–7.0 0.50 1.3 0.3–5.9 0.72
Multiple birthsSingle 36/1 385 (2.6) 1.0Twin/Multiple 1/20 (5.0) 2.0 0.3–15.1 0.51 1.5 0.2–13.0 0.66
∗Multivariate RRs are adjusted for gender, birth weight, delivery mode, maternal age, and multiple births.
effect on pregnant women’s insistence on choosing cesareansection.
The incidence of low Apgar scores dropped dramaticallyfrom 1995 to 1999, and continued to decrease slightly there-after. In this investigation, only term infants were includedwhen calculating the incidence of low Apgar scores becausethe use of Apgar scores is limited in preterm infants. Theincidence declined dramatically after 1996, when implemen-tation of the ABCDE resuscitation (16,17) protocol beganin the hospital; this protocol significantly improved the 1-minute Apgar score and thereby reduced the morbidity rate(18). In this study, we found that males are more likely toexperience low Apgar scores than females. The imbalance offetal sex has also been reported in previous studies (19,20).However, there was no difference in mortality rate betweenthe sexes.
In agreement with a previous study (21), low birth weightwas the only risk factor related to both low Apgar scores andcase fatality. Birth weight is a sensitive predictor for infantdeath (22) because it is secondary to utero-placental insuffi-ciency, which can result in decreased energy stores and sup-ply. In this study, low Apgar scores were the second leadingcause of neonatal deaths, related to 16.2% of neonatal deaths,which is in agreement with a survey conducted during thesame period in China (23). The neonatal death rate was stillmuch higher than that of high-income countries (7), withpreterm birth and asphyxia the leading causes. Additionalefforts to improve perinatal care are required to reduce ratesof multiple fetus pregnancy, cesarean section, preterm birth,and neonatal death.
Funding
This study was supported by a grant from Henan Medi-cal Science Academy, the Department of Education, and theMinistry of Health of China.
References
1. Lawn JE, Cousens S, Zupan J. 4 million neonatal deaths:
when? Where? Why? Lancet. 2005;365:891–900.
2. Bryce J, Boschi-Pinto C, Shibuya K, Black RE. WHO
estimates of the causes of death in children. Lancet.
2005;365:1147–52.
3. UNICEF. China statistics. http//:wwwuniceforg/
infobycountry/china statistichtml (last accessed September
2009).
4. Ministry of Health of the People’s Republic of China. China
Health Yearbook 2008. (http://wwwmohgovcn/publicfiles/
business/htmlfiles/mohbgt/s9605/listhtm).
5. Huo K, Zhao Y, Feng H, Yao M, Savman K, Wang X, et al.
Mortality rates of children aged under five in Henan
province, China, 2004–2008. Paediatr Perinat Epidemiol.
2010;24:343–8.
6. Mathews TJ, MacDorman MF. Infant mortality statistics
from the 2003 period linked birth/infant death data set. Natl
Vital Stat Rep. 2006;54:1–29.
7. WHO. World Health Statistics 2008. (http://www.who.int/
whosis/whostat/EN)
8. Zhu WX, Lu L, Hesketh T. China’s excess males, sex selective
abortion, and one child policy: analysis of data from 2005
national intercensus survey. Br Med J. 2009;338:b1211.
336c© 2011 The Authors
Acta Obstetricia et Gynecologica Scandinavica c© 2011 Nordic Federation of Societies of Obstetrics and Gynecology 90 (2011) 332–337

W. Han et al. Trends in live birth in Zhengzhou, China
9. National Bureau of Statistics of the People’s Republic of
China. China Statistical Yearbook 2009.
(http://wwwstatsgovcn/tjsj/ndsj/2009/indexehhtm).
10. Wei K, Yang Y, Yao Y, Du L, Sun J. An initial epidemiologic
investigation of preterm infants in cities of China. Chin J
Contemp Pediatr. 2005;7:25–8.
11. Tucker J, McGuire W. Epidemiology of preterm birth. BMJ.
2004;329:675–8.
12. Chen ZL, He RZ, Peng Q, Guo KY, Zhang YQ, Yuan HH,
et al. Prenatal risk factors for neonatal asphyxia: how risk for
each? (in Chinese). Chin J Contemp Pediatr. 2009;11:161–5.
13. Hegyi T, Carbone T, Anwar M, Ostfeld B, Hiatt M, Koons A,
et al. The apgar score and its components in the preterm
infant. Pediatrics. 1998;101(1 Pt 1):77–81.
14. WHO. Appropriate technology for birth. Lancet.
1985;2:436–7.
15. Lumbiganon P, Laopaiboon M, Gulmezoglu AM, Souza JP,
Taneepanichskul S, Ruyan P, et al. Method of delivery and
pregnancy outcomes in Asia: the WHO global survey on
maternal and perinatal health 2007–08. Lancet.
2010;375:490–9.
16. Zhu XY, Fang HQ, Zeng SP, Li YM, Lin HL, Shi SZ. The
impact of the neonatal resuscitation program guidelines
(NRPG) on the neonatal mortality in a hospital in Zhuhai,
China. Singapore Med J. 1997;38:485–7.
17. Elliott RD. Neonatal resuscitation: the NRP guidelines. Can J
Anaesth. 1994;41:742–52.
18. Patel D, Piotrowski ZH, Nelson MR, Sabich R. Effect of a
statewide neonatal resuscitation training program on Apgar
scores among high-risk neonates in Illinois. Pediatrics.
2001;107:648–55.
19. Bekedam DJ, Engelsbel S, Mol BW, Buitendijk SE, Van Der
Pal-de Bruin KM. Male predominance in fetal distress during
labor. AJOG. 2002;187:1605–7.
20. Clarke CA, Mittwoch U. Changes in the male to female ratio
at different stages of life. Br J Obstet Gynaecol.
1995;102:677–9.
21. Wu YW, Backstrand KH, Zhao S, Fullerton HJ, Johnston SC.
Declining diagnosis of birth asphyxia in California:
1991–2000. Pediatrics. 2004;114:1584–90.
22. Swamy GK, Ostbye T, Skjaerven R. Association of preterm
birth with long-term survival, reproduction, and
next-generation preterm birth. J Am Med Assoc.
2008;299:1429–36.
23. Yang Y. Epidemiologic survey for hospitalized neonates in
China (in Chinese). Chin J Contemp Pediatr. 2009;11:15–20.
c© 2011 The AuthorsActa Obstetricia et Gynecologica Scandinavica c© 2011 Nordic Federation of Societies of Obstetrics and Gynecology 90 (2011) 332–337 337