Embed Size (px)
Citation preview

Journal of Infection (1993) 26, I-7
LEADING ARTICLE
T r 6 s d i f f i c i l e
E d m u n d Wi lk ins
Regional Department of Infectious Diseases and Tropical Medicine, Monsall Hospital, Manchester MIO 8WR, U.K.
Accepted for publication 5 November 1992
Sixty years ago each and every person lived in almost daily contact with tubercle bacilli, became a little tuberculous, yet had a fair chance of enjoying a normal creative life. ~ The presence of Mycobacterium tuberculosis can bring about clinical disease, but moreoften does not. A balance between struggle and partnership evolves in which many factors influence the outcome; sometimes, under the slightest provocation, the alliance is broken and the mycobacterium gains the upper hand. The same appears to be true for Clostridium difficile where a delicate interplay exists between the micro-organism and the individual and where the gut hosts the struggle for dominance.
Pseudomembranous colitis was first reported as a pathological entity towards the end of the last century, 2 long before the discovery of C. difficile) This was an era when epidemics of erysipelas, gangrene, and septicaemia were occurring with regularity on the wards, spreading with heart-rending swiftness and exacting a high mortality. Antibiotics have done much to alter the face of hospital acquired infection and render pyogenic disease an enfeebled shadow of its former self. But it is these two considerations, antibiotics and nosocomial infection, that make C. difficile such a prominent pathogen of modern hospital medicine. Its name betrays its nature in more ways than just isolation and study.
During the first 8 months of 1992, the Public Health Laboratory Service received reports from IO hospitals concerning nosocomial C. difficile outbreaks involving significant numbers of patients: prior to then, only a few had been recorded (Dr R. Adak, personal communication). The largest of these occurred in hospitals in north Manchester where I75 patients developed C. difficile diarrhoea over a 6 month period and where infection contributed directly to the deaths of I7 patients. The outbreak began in one elderly ward but eventually spread to 34 wards in three hospitals resulting in major disruption to patient care in the district. Subsequently, nearly all isolates were found to be identical using two typing methods, pyrolysis mass spectrometry and immuno-fingerprinting. Environmental screening demonstrated that the clone was present throughout the hospital to the exclusion of other strains.
From being the stuff of case reports before I977, C. difficile has rapidly become the leading clostridium of human importance and is now recognised as an important and difficult nosocomial pathogen. 4 Managing C. difficile outbreaks has taxed Control of Infection Teams up and down the country. Unfortunately, there are no official guidelines and C. difficile refuses to behave
oi63-4453/93/OlOOOI +07 $08.00/0 © I993 The British Society for the Study of Infection

2 E. W I L K I N S
in a predictable manner ; much has had to be learnt by a process of trial and error. Dur ing an outbreak, several aspects of overall management are raised: clinical care of the patient; laboratory diagnosis; limiting spread of disease; and administrative management.
Clinically, C. difficile diarrhoea simulates diarrhoea produced by other enteric pathogens; the principal clue to aetiology is a history of antibiotics. Symptoms of disease typically start 5 - I0 days after commencing on antibiotics, but may occur as early as the first day or as late as 2 months after discontinuing therapy. To some extent, this reflects whether antibiotics have preceded exposure to C. difficile or carriage h a d antedated antibiotic administration. Where cases are observed many weeks after completing antibiotic therapy, this probably reflects prolonged susceptibility induced by the antimicrobial and new acquisition of C. difficile. 5 Where symptoms begin long after admission, but soon after commencing antibiotics, this probably reflects earlier col- onisation, al though one study indicated t h a t ' carriers' are not at increased risk of developing subsequent diarrhoea. 6 Nevertheless, patients do serve as reservoirs of the organism in a situation analogous to meningococcal carriage. For the majority of patients, acquisition of C. difficile and administration of antibiotics probably occur near enough together and within the first few days after arrival onto the ward. 7 Clusters of cases indicate exposure to an exogenous source of the organism at a t ime of susceptibility, usually through antimicrobial therapy.
Fever, leucocytosis, abdominal pain, and mucus-containing stools are characteristic of clinical disease: yellow raised plaques on sigmoidoscopy are pathognomic. Disease may vary from a localised segment of non-specific colitis causing relatively trivial diarrhoea to a pancolitis with pseudomembranes and complicating toxic megacolon, perforation, or Gram-negative shock. Treat- ment is usually s traightforward--stop the offending antibiotic and, if the diarrhoea does not settle or the patient is sick, give either oral vancomycin or metronidazole. I f there is paralytic ileus, intravenous metronidazole should be added. The majority of patients improve within 2-4 days.
Clinical ' relapse ' , embracing both true relapse from the original infecting strain and reinfection (only typing can distinguish this), is a major problem. It occurs in I5-Z5 % of treated patients irrespective of which antibiotic was used. There is some evidence to suggest that shorter courses of initial therapy are associated with a lower risk of relapse. 8 In reality, relapse represents antibiotic- induced disease again, but in this case either vancomycin or metronidazole is the offending antibiotic. Hence, trivial or mild cases of C. difficile diarrhoea should not be treated with antimicrobial agents since relapse is rarely observed in untreated cases?
Relapsing patients typically respond well to initial therapy but symptoms recur I-3 weeks after discontinuing treatment without further antibiotic provocation. There is no reliable way of foretelling who will relapse; persistence of the toxin or organism is not predictive. 9,10 Retreatment may be followed by a further relapse in 30--50 % of patients (the record number for any one patient is said to be I8). Management of the patient with mult iple relapses is difficult. Regimens are based on fully treating C. difficile (at least 2-4 weeks of vancomycin or metronidazole) followed by tapering doses, 11

Trds difficile 3
trying to ' ca tch ' the germinating spores (intermittent 7-day pulse t reatment alternating with no treatment), 12 and re-establishing the normal colonic flora by either oral (Lactobacillus spp. preparations, non-toxigenic C. difficile) 13' 14 or rectal (polymicrobial normal faecal flora) 1~ administration.
The principal laboratory diagnostic methods have been directed towards detecting the organism by culture on selective med ium or identifying toxins (A or B) in faecal extracts. Cycloserine-Cefoxitin-Fructrose agar (CCFA) is the standard medium. Unfortunately, there is a lack of uniformity in culture methods between laboratories which makes it difficult to compare results. The predictive value of a positive culture is not good because approximately 3 % of healthy adults, 16-18 2- I 1% of hospitalised adults not receiving antibiotics, TM 19 and 21-46% of hospitalised adults receiving antibiotics and with no gastrointestinal complaints are found to be carrying C. difficilefl °-22 These figures may be higher in the outbreak context and where optimal recovery conditions are being used making it extremely difficult to base outbreak management decisions on stool culture results. Due to these diagnostic limitations and the 48 h delay for results of anaerobic culture, the value of culture is l imited to epidemiological investigations and subsequent typing of strains. Free toxin B, a potent cytotoxin, can be detected by monolayer tissue cell culture assay with neutralisation by antitoxin (either C. sordelii or C. difficile) and is currently the 'gold s tandard ' to which other assays are compared. It is present in 97 % of cases of pseudomembranous colitis and 25-4o% of patients with antibiotic-associated diarrhoea in which recto- sigmoid pseudomembranes cannot be detected. 4 It is not found in the stools of asymptomatic adults who have not received antibiotics but can be identified in t o-23 % of stools of asymptomatic antibiotic recipients. 16' 21 Nevertheless, the finding of specific cytotoxin in the stool of a symptomatic patient invariably indicates C. difficile disease. The major disadvantages of this test are general j lack of availability in hospitals without cell culture capability and the t ime delay of 24-72 h before obtaining a result.
Because of this, rapid immunoassays have been developed and evaluated for the detection of toxin. At least seven have become commercially available although one was later found not to detect either toxinfl a Four are enzyme immunoassays (Cytoclone, Cambridge Biotech Corp; Vidas, bioMerieux; Premier, Meridian; Tox-A-Tes t , Techlab) which demonstrate superior test characteristics over the three latex agglutination tests. Sensitivity approxi- mates 80% with a specificity nearing i o o % when compared to tissue cell culture. 24-26 This enables a reasonably predictive result to be available within 2½ h and, if set up simultaneously with the cytotoxin assay, allows a provisional result to be available on the same day to be followed by a confirmatory result 24-48 h later. Case management can then be applied (see algorithm).
Having identified a patient with C. difficile toxin-positive diarrhoea and initiated specific treatment, how can one limit nosocomial spread? Several aspects of C. difficile epidemiology strike at the heart of effective infection control. The bacterium forms a spore under adverse conditions and as such quickly and heavily contaminates the local environment of a patient with diarrhoea, which is characteristically unannounced and explosive. The spores are highly resistant to standard disinfectants such as hypochlorite and survive

4 E. W I L K I N S
for many months: alkaline glutareldehyde and alkaline hypochlorite are the only effective sporicidal agents. Following acquisition, patients carry the organism for most of their hospital stay 7 and there is no effective treatment for the carriage state. During this time environmental contamination persists, albeit to a lesser degree. 27 The same is true for the significant proportion of patients who remain asymptomatic after infection but represent an infection risk (six for every symptomatic case), the 'silent majority'. 28 Community reservoirs of the organism exist where institutionalised patients may be reinfected or from where carriers may be readmitted to hospital. Lastly, health care workers can transiently carry the organism on their hands or in their gastrointestinal tract and can rarely develop clinical disease.
In this context, 'control ' of infection is more apposite than attempts at 'eradication'. Key areas in controlling spread are immediate isolation of diarrhoeal patients with strict enteric precautions, urgent sample collection and sameday toxin testing with close liaison with microbiology, and, if the outbreak is large, transfer ef patients with confirmed infection to an infectious diseases ward or designated isolation ward for cohort nursing. Treatment should be initiated with vancomycin reserving metronidazole for first relapse; further stool samples should be tested for toxin only if there is a recrudescence of diarrhoea. C. difficile culture-positive, toxin-negative patients with diarrhoea should not be treated as there is insufficient evidence that this course of action is beneficial .29.30
Immediate and rigorous cleaning of the patient's adjacent environment and any likely (e.g., sluice, bed-pan washers, commodes) or obviously soiled areas with neutral detergent and alkaline hypochlorite should be performed. The Infection Control Team may need to be strengthened in numbers to enable a 24 h service to be operated, to visit all ward areas to check on new cases daily or twice daily, to educate, and to reinforce handwashing, isolation principles, etc. Where clustering of cases has occurred the ward may need to be closed to new admissions while thorough cleaning takes place. However, emptying the ward and relocating patients to allow extraordinary 'spring ' cleaning should be avoided as this disseminates asymptomatic carriers around the hospital. Where diarrhoea has ceased for 48 h, patients can be returned to their ward. There is no advantage to be gained by continued isolation as persistent carriage after infection, whether treated or not, is common. 7,28 There is also the risk of reinfection on completion of treatment which will be greatest in the more heavily contaminated environment of the specially commissioned isolation ward.
Total antibiotic usage must be reviewed and measures taken to curb excessive or inappropriate prescribing. Weekly analysis of individual antibiotic consumption may identify a particular broad spectrum agent that can be removed from the antibiotic policy. Nearly all drugs with antibacterial activity and virtually all routes of administration have been linked with C. difficile diarrhoea but oral broad spectrum agents are those most frequently implicated. The antibiotic policy may need to be extensively rewritten so as to promote those antimicrobial agents less likely to predispose to C. difficile disease (e.g., gentamicin, co-trimoxazole, ciprofloxacin). This should be tackled immedi- ately; without antibiotics C. difficile is impotent. Additional prophylaxis of

Trds difficile 5
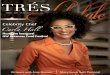
D I A R R H O E A in an in-patient on antibiotics or on
a ward with a confirmed case
Isolate in Side Ward with Strict Enteric Precautions
Send Stool for CD Toxin
Keep in Side Ward Repeat CD Toxin
Await Other Enteric Pathogen Screen
tIs CD Toxin Test Positive? [
t
Any More Diarrhoea? ]
<
1
Isolate * and Start Vancomycin
125 mg qds 10d
1 No Diarrhoea I for 48 hrs .
1
Return to Ward or [ Discharge home or [
to Institution ]
* Specially commissioned ward/part of ward with cohorted nur}ing etc., or Infectious Diseases Unit
Fig. I. Algor i thm for control of hospital outbreak of C. difficile.
high risk cases requiring broad spectrum antibiotics by adding in metro- nidazole or vancomycin does not work and should not be advised. 12
Administrative management of the outbreak will be set out in the hospital 'Major Outbreak Policy' which should be invoked. This will bring togeth~:r relevant local expertise, facilitate effective communication between the involved directorates, and provide the necessary working structure for effective control of the problem. Within this policy, a pre-agreed timetable for

6 E. WILKINS
contact ing outside agencies such as the Publ ic Hea l th Labora to ry Service can be followed. Genera l Pract i t ioners mus t be in formed of the outbreak and the significant risk of relapse if one of their patients has been infected. T h e y mus t also be made aware of the possibili ty that any recent inpat ient may be asymptomat ical ly carrying C. difficile which will only become manifest when antibiotics are prescr ibed. Patients mus t also be alerted to the possibil i ty of a relapse of symptoms and the need to contact the Genera l Pract i t ioner or hospital.
T h e last I5 years have seen C. difficile move f rom obscur i ty to high prominence . Ironically, it is dur ing this same per iod that Infect ion Control has rapidly gained in stature. Wi thou t a warning system in place to herald increasing C. difficile infections, a small cluster of cases may soon develop into a large and difficult to manage outbreak. Regular repor t ing of cases of diarrhoea by the nurs ing staff and f requent visits by the Infect ion Control T e a m is the key. A laissez-faire at t i tude is unlikely to work and with the new ethos of purchase r -p rov ide r contracts, will lead to auto-des t ruct ion. I t may be that low C. difficile carriage and infect ion rates will become the touchs tone of good infect ion control in the future.
R e f e r e n c e s
I. Dubos R. Mirage of health. Utopia, progress and biological change. London: George Allen and Unwin Ltd, I959: 57-8z.
2. Finney JMT. Gastroenterostomy for cicatrizing ulcer of the pylorus. Johns Hopkins Med J z893; 4: 53-55.
3. Hall JC, O'Toole E. Intestinal flora in new-born infants with a description of new pathogenic anaerobe, Bacillus difficilis. Am J Dis Child I935; 49: 39o-402.
4. Rolfe RD, Finegold SM, Eds. Clostridium difficile: its role in intestinal disease. London: Academic Press, I988.
5. Larson HE, Borriello SP. Quantitative study of antibiotic-induced susceptibility to Clostridium difficile eneterocecitis in hamsters. Antimicrob Agents Chemother I99O; 34: I348-I353.
6. Johnson S, Clabots CR, Linn FV, Olson MM, Peterson LR, Gerding DN. Nosocomial Clostridium difficile colonisation and disease. Lancet I99O; 336: 97-IOO.
7. McFarland LV, Mulligan ME, Kwok RYY, Stamm WE. Nosocomial acquisition of Clostridium difficile infection. N Engl J Med I989; 320: 204-210.
8. Bartlett JG, Tedesco FJ, Shull S, Lowe B, Chang T. Symptomatic relapse after oral vancomycin therapy of antibiotic-associated pseudomembranous colitis. Gastroenterology I98O; 78 : 431-434.
9. Young GP, Bayley N, Ward P, St John D J, McDonald MI. Antibiotic-associated colitis caused by Clostridium difficile: relapse and risk factors. Med J Aust I986; I44: 303-306.
IO. Finegold SM, George WL. Therapy directed against Clostridium difficile and its toxins: complications of therapy. In: Rolfe RD, Finegold SM, Eds. Clostridium difficile : its role in intestinal disease. London : Academic Press, I988 : 342-356.
rI. Tedesco FJ. Treatment of recurrent antibiotic-associated pseudomembranous colitis. Am J Gastroenterol I982; 77:220
I2 Fekety R. Antibiotic-associated colitis. In: Mandell GL, Douglas RG, Bennett JE, Eds. Principles and practice of infectious diseases. New York: Churchill Livingstone, I99O: 863-869.
!3 Gorbach SL, Chang TW, Goldin B. Successful treatment of relapsing Clostridium difficile colitis with lactobacillus GG. Lancet I987; ii: z519.
I4. Seal D, Borriello SP, Barclay F, Welch A, Piper M, Bonnycastle M. Treatment of relapsing Clostridium difficile diarrhoea by administration of a non-toxigenic strain. Eur J Microbiol x987; 6: 51-53.

Trds difficile 7
r 5. Tvede M, Rask-Masden J. Bacteriotherapy for chronic relapsing Clostridium difficile diarrhoea in six patients. Lancet I989; i i : I I56-I I6o.
I6. Rolfe RD. Asymptomatic intestinal colonisation by Clostridium difficile. In: Rolfe RD, Finegold SM, Eds. Clostridium difficile : its role in intestinal disease. London: Academic Press; I988 : zoI -zz5 .
I7. Brettle RP, Wallace E. Clostridium difficile-associated diarrhoea. J Infect I984; 8: I23-I28. I8. Varki NM, Aquino TI . Isolation of Clostridium difficile from hospitalised patients without
antibiotic-associated diarrhoea or colitis. J Clin Microbiol x982; 16: 659-662. I9. Chang TW, Lauermann M, Bartlett JG. Cytotoxicity assay in antibiotic-associated colitis.
J Infect Dis I979; I4O: 765-77 o. 2o. Viscidi R, Willey S, Bartlett JG. Isolation rates and toxigenic potential of Clostridium
difficile isolates from various patient populations. Gastroenterology I98I ; 8x: 5-9- 2I. George WL, Rolfe RD, Finegold SM. Clostridium difficile and its cytotoxin in feces of
patients with antimicrobial agent-associated diarrhea and miscellaneous conditions. J Clin Microbiol I982; I5: IO49-IO53.
22. George WL, Rolfe RD, Harding G K M , Klein R, Putnam CW, Finegold SM. Clostridium difficile and cytotoxin in feces of patients with antimicrobial agent-associated pseudo- membranous colitis. Infection I982; IO: 205--208.
23. Lyerly DM, Wilkins TD. Commercial latex test for Clostridium difficile toxin A does not detect toxin A. J Clin Microbiol I986; 23: 622-623.
24. Borriello SP, Vale T, Bi"azier JS, Hyde S, Chippeck E. Evaluation of a commercial enzyme immunoassay kit for the detection of Clostridium difficile toxin A. Eur J Clin Microbiol Infect Dis I992; I i ; 36o--363.
25. Delmee M, Mackey T, Hamitou A. Evaluation of a new commercial Clostridium difficile toxin A enzyme immunoassay using diarrhoeal stools. E u r J Clin Microbiol Infect Dis I992; IX : 246-249.
26. Barbut F, Kazjer C, Planas N, Petit JC. Comparison of four laboratory methods for the detection of Clostridium difficile (CD) toxins. Abstract I252, The 32nd Interscience Conference on Antimicrobial Agents and Chemotherapy. American Society of Micro- biology I992.
27. Fekety R, Kyung-Hee K, Brown D, Batts DH, Cudmore M, Silva J. Epidemiology of antibiotic-associated colitis. Isolation of Clostridium difficile from the hospital environment. A m J Med I98I ; 70: 906-908.
28. Johnson S, Homann SR, Bettin K M et al., Treatment of asymptomatic Clostridium difficile carriers (fecal excretors) with vancomycin or metronidazole. Ann Int Med I992; I I 7 : 297-302.
29. Lashner BA, Todorczuk J, Sahm DF, Hananer SB. Clostridium difficile culture-positive toxin-negative diarrhoea. Am ff Gastroent I986; 8x: 940-943 .
3o. Bender BS, Bennett R, Laughon BE et al. Is Clostridium difficile endemic in chronic-care facilities? Lancet I986; i i : I I - I 3 .