Embed Size (px)
Citation preview

CMPath Training 9 Feb 2018
in partnership with
Trial design and statistics for beginners
Professor Judith Bliss
Director ICR-Clinical Trials & Statistics Unit (ICR-CTSU), The Institute of Cancer
Research
NCRI Cancer CTU Group – Chair of Directors Group
https://www.youtube.com/watch?v=Hz1fyhVOjr4
(courtesy of Sue Hilsenbeck)

CMPath Training 9 Feb 2018
What is a clinical trial?
“A clinical trial may be defined as a carefully designed,
prospective medical study which attempts to answer a
precisely defined set of questions with respect to the effects of
a particular treatment or treatments.”
R. Sylvester 1984
Where is the laboratory?
The NHS & cancer centres worldwide
2

CMPath Training 9 Feb 2018
Phases of clinical trials 3
Phase 1: TOXICITY
What is the maximum tolerated dose (MTD)? safety, 3+3 vs. more complex dose escalation procedures eg
continual reassessment methods (CRM), size of expansion cohorts
Phase 2: ACTIVITY
Does it do anyone any good? establishing sufficient evidence of activity to justify phase III, formal
stop/go criteria, single group or randomised
Phase 3 THERAPEUTIC BENEFIT
Is it any better than existing treatment? efficacy comparison with standard of care, robust results with the
potential to change practice, choice of endpoints, risks & benefits
Ultimate goal is to change routine clinical practice & target
treatment towards those patients with the most to gain

CMPath Training 9 Feb 2018
Phase I Clinical Trials 4
Aim
Dose-finding: to determine Maximum Tolerated Dose (MTD)
Conduct
Common designs include 3+3, rolling six, continual reassessment
method (CRM)
Endpoints
Tolerability, pharmacodynamics, pharmacokinetics, bioavailability
First experiments in humans
For cancer treatment - usually in patients whose standard therapy has
failed i.e. those with late stage advanced disease

CMPath Training 9 Feb 2018
Phase II Clinical Trials 5
Aim
• To determine if drug has therapeutic activity
• To identify promising new agents / interventions / techniques for further
investigation / potential predictive biomarkers
Conduct
• Historically, single arm studies of 20-80 patients
• Single stage Fleming or A’Hern design
• Two stage - Simon, Gehan designs - allow trial to be terminated at end
of first stage if drug is clearly inactive
Endpoints
• Use quickly-available endpoints
• Usually “tumour response” (pCR or ORR) and/or safety
• Emergence of “biomarker” endpoints (molecular & imaging)

CMPath Training 9 Feb 2018
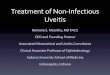
Phase II – Simon two-stage design 6
Identify boundaries of treatment utility:
p0: response level at which the treatment does not warrant further investigation
p1: expected (true) response level where the treatment warrants further
investigation (i.e. development of a phase III)
Stage 1:
Recruit N1 patients
if ≥n1/N1 responses seen,
continue to stage 2
if <n1/N1 responses seen,
STOP
Stage 2:
Recruit and additional N2
patients so that N1 + N2 = N
if ≥n/N responses seen,
treatment warrants
further investigation
if <n/N responses seen,
STOP

CMPath Training 9 Feb 2018
Phase II – Example: CORAL 7

CMPath Training 9 Feb 2018
Phase II Clinical Trials 8
Randomised phase II…
Move towards introduction of early randomised comparison against
current standard to assess feasibility + tolerability + activity - complex trial
designs: integrated phase II / phase III
Why not single group studies?
Single group trials prone to selection bias
No real allowance for imprecision in historical estimate of response used
to base phase II sample size on
“Modest” treatment effects may be lost in study bias or imprecision of
historical information
But….can be useful when cancer or subgroup of interest is uncommon or
for proof of principle studies

CMPath Training 9 Feb 2018
Phase III Clinical Trials 9
Reliable
• Large enough to give precision to estimate treatment benefit
• Study a group of patients who are broadly representative
• Experimental treatment differs sufficiently from control to have
reasonable chance of influencing chosen endpoint
• Trial may test superiority or non-inferiority of new treatment
Aim
• to determine how new treatment compares with existing therapy
Conduct
• Unbiased, reliable, clinically informative, randomised comparison
Endpoints
• Direct measure of patient benefit
• Disease-free survival, Progression-free survival, Overall Survival
• Identify adverse risk vs benefit profile (& cost effectiveness)
• Translational research to identify patients with most/least to gain

CMPath Training 9 Feb 2018
Treatment is allocated at random
Why randomise?
Randomisation avoids bias
Each subject has an equal chance
of receiving the experimental or
control treatment, regardless of
clinical / demographic
characteristics.
Treatment groups similar overall -
when sample size large enough to
avoid random errors
Randomisation – to balance for
the factors which cannot be
measured.
Only systematic difference between
groups is the treatment
If outcomes for group A better than B,
likely due to treatment, as two groups
similar
Results = improvement in treatment
10
Treatment A Treatment B

CMPath Training 9 Feb 2018
Common phase III trial designs 11
Parallel groups: “between-
patient” comparisons - each
patient receives 1 intervention
R
A
B
Compare A vs B
Compare A vs B and
C vs D
Interactions
Compare A vs B within
groups of patients
Interaction w/marker
R
A D
B D
A C B C
Factorial: ≥ 2 treatment
comparisons in same trial
without necessarily increasing
size
Stratified designs:
1 intervention,
comparison within
subgroup Str
atify
Marker +
Marker - R A
B
R A
B

CMPath Training 9 Feb 2018
Biomarker designs
Modified marker based design
Marker based strategy design
R
Marker based
strategy
Non-marker
based strategy
M+
M-
A
B
B
R
Marker based
strategy
Non-marker
based strategy
M- B
R A
B
Targeted design (enrichment)
Marker +
Marker -
R A
B
Off study
Marker stratified design (marker-treatment interaction)
M+ A
Str
ati
fy Marker +
Marker - R A
B
R A
B
12
M+ A

CMPath Training 9 Feb 2018
Biomarker trial - Example
A
B
B
A
B
A
A
B
B
A
B
Off study
FOCUS4: Molecularly stratified, multi-centre randomised trial programme
for patients with advanced/metastatic colorectal cancer
13

CMPath Training 9 Feb 2018
14 A randomised trial utilising ctDNA mutation tracking to detect minimal residual disease and trigger intervention in patients with moderate and high risk early stage triple negative breast cancer
14
c-TRAK TN
Background: • Circulating tumour DNA (ctDNA) is
released when tumour cells die. ctDNA detection in patients who have completed treatment for early BC may be highly predictive for future relapse.
• Pembrolizumab = anti PD-1 immunotherapy. Blocks interaction between PD-1 and it’s ligands which are often overexpressed in TNBC and therefore prevents immune system suppression.
• c-TRAK TN aims to show whether ctDNA tracking can predict relapse, and whether use of pembrolizumab may result in sustained clearance of ctDNA.
Recruitment duration: 18 months Number of centres: 17
Recruitment target:
ctDNA screening: 200 patients (~150 with trackable
mutations)
Randomised: 36-68 (dependant on rate of ctDNA positivity)

CMPath Training 9 Feb 2018
15
What are adaptive trials?
“use accumulating data to decide on how to modify aspects of the study
without undermining the validity or integrity of the trial” (Dragalin 2007)
• Adaptive by design not a license for adhoc changes of trial conduct &
analysis nor a remedy for poor planning
• Platform trials / umbrella protocols / basket trials
• Change trial based on early safety, activity or efficacy data / decision
rules
• Changes could include
Change dose of treatment (phase I)
Change allocation ratio of control:research
Early stopping for benefit
Early stopping for lack-of-(sufficient)-benefit
Adding in new treatments – via randomisation or as additional cohorts

CMPath Training 9 Feb 2018
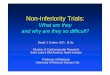
Multi-Arm Multi-Stage designs 16
Figure courtesy of STAMPEDE website
The MAMS design rolls the
phase 2 assessment of the
activity of combination
therapy into the same trial as
the phase 3 assessment of
effectiveness
Thus saving time and
resources

CMPath Training 9 Feb 2018
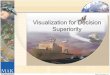
MAMS designs - Example 17
R
A
N
D
O
M
I
S
E
Hormone therapy (HT) aloneA
HT + zoledronic acidB
HT + docetaxelC
HT + celecoxibD
HT + zoledronic acid + docetaxelE
HT + zoledronic acid + celecoxibF
Control
Eligible patient with prostate cancer
R
A
N
D
O
M
I
S
E
Hormone therapy (HT) aloneA
HT + zoledronic acidB
HT + docetaxelC
HT + celecoxibD
HT + zoledronic acid + docetaxelE
HT + zoledronic acid + celecoxibF
Control
Eligible patient with prostate cancer
Figure from STAMPEDE trial website, MRC CTU
STAMPEDE: Systemic Therapy in Advancing or Metastatic
Prostate cancer: Evaluation of Drug Efficacy
Advantages and disadvantages of this design?

CMPath Training 9 Feb 2018
Actionable mutation identified in ctDNA screening
Blood sample sent to central laboratory for analysis by digital PCR using
ctDNA assays for hotspot mutations in ESR1, HER2, AKT1 and PIK3CA,
with HER2 copy number assessment
Platform trial: plasmaMATCH trial 18
PIK3CA mutation status
also reported to facilitate
entry into trials outside of
the context of
plasmaMATCH
Cohort A
ESR1 mutation
Treat with extended-
dose fulvestrant
Cohort B
HER2 mutation
Treat with neratinib
(plus fulvestrant in
ER+ BC)
Cohort C
AKT1 mutation in
ER+ BC
Treat with AZD5363
+ fulvestrant
Cohort D
AKT activation basket
mutation identified in ctDNA or
in tumour tissue sequencing
outside of plasmaMATCH
Treat with AZD5363
Future Cohorts
May be added by substantial
amendment in the case of
new
diagnostic/
therapeutic targets as the trial
progresses
Patients with metastatic or recurrent locally advanced breast cancer
eligible for ctDNA screening within plasmaMATCH are registered for
screening component
Eligible patients enter therapeutic component for treatment with targeted
agent until disease progression
Number of centres ~50 UK Screening Sites, of which ~25 sites will also be Treatment Sites
Recruitment target • ctDNA screening component: ~1000 patients with metastatic or recurrent locally
advanced BC who have received prior systemic treatment in the advanced setting
• Therapeutic component: Cohort A – 40 patients; Cohorts B–D – 16 patients in each

CMPath Training 9 Feb 2018
Trial considerations: Types of data 19
Clinical
• Baseline characteristics
• Treatment details
• Adverse events/side effects
• Disease related outcomes
PROMS
• QoL questionnaires
• Patient diaries
Translational
• Biomarkers using blood
(e.g. BRCA, ctDNA, CTCs)
• Biomarkers using tumour
tissue (e.g. Ki67, HRD)
• Gene expression data
• SNP arrays
• Whole exome sequencing
• PK/PD
Other
• Photographs
• Physics/dosimetry
• Imaging
• Health economics
• Qualitative

CMPath Training 9 Feb 2018
Trial considerations: effect size
Superiority
what is the minimum clinically important improvement in efficacy with new
treatment compared with standard treatment?
• e.g. treatment A is at least 6% better than treatment B
Non-inferiority
show that new treatment is not worse than standard by more than pre-
specified, small amount (non-inferiority margin)
• e.g. treatment A is no more than 3% worse than treatment B
20
Smaller effect size → larger sample size

CMPath Training 9 Feb 2018
Trial considerations: Analysis populations - Intention to treat (ITT) As a general rule (phase III), all patients randomised should be analysed by randomly allocated treatment.
Why?
• Avoids bias. People who receive non-allocated treatment likely to be a selected subset (e.g. side effects, more severe disease etc.) Ignoring them excludes this type of person from one treatment arm and not the other, which affects the comparison of treatment effect.
• Is more pragmatic. Gives an idea of what would happen if the treatment were to be adopted as standard practice in the real world.
21
‘What happens to the population on average if new drug becomes policy’ not ‘What happens to the average patient who gets the drug’

CMPath Training 9 Feb 2018
Intention to treat analysis - Example 22
• RCT comparing nurse-led vs. conventional medical follow-up for patients
with lung cancer
• Primary outcome measures: patient satisfaction & quality of life
• Followed-up to 1 year after randomisation
• In practice, many patients allocated to nurse-led follow-up were referred
back to medical team for symptom control or further palliative treatment
What would be the result of not analysing these data according to ITT?
Conventional medical follow-up group included severely ill patients who had
been referred from nurse-led group → patients who had only received nurse-
led follow-up would generally be those with better prognosis
BIAS!

CMPath Training 9 Feb 2018
Trial considerations: Analysis populations – Per Protocol (PP)
23
Usually excludes patients who have any major protocol violations and
analysis is by treatment actually received
Often used for safety analyses – better estimate of absolute risks
Often used for non-inferiority trials because
including data for patients who did not receive protocol treatment (ITT)
• tends to bias results toward equivalence
• could make a truly inferior treatment appear non-inferior
But bias! – excluding patients fails to maintain the integrity of randomisation
Non-inferiority trials should be analysed both by ITT & PP
• Want to see the same result in both analyses

CMPath Training 9 Feb 2018
Statistical considerations in clinical trials
At the concept/design stage (pre-funding application)
Trial design:
Treatment allocation method – randomisation / blinding
Stratification variables - centre / biomarkers
Protecting against other sources of bias
Endpoints – clinically informative, reliable & valid measurement?
Sample size – study appropriately powered random error
• Power (1-β) = probability of detecting a difference if such a difference truly exists
• Significance level (α) = probability of concluding there is a treatment effect when
no true effect exists
Power = 80%- 90% α = 0.05 (usual)
s
24

CMPath Training 9 Feb 2018 Clinical Trials - Lucy Kilburn & Holly Tovey – 12/01/2018
Statistical considerations in clinical trials
Statistical Analysis Plan defines plans and scope for During the running of the trial Trial monitoring • Data quality & completeness Interim analyses (for review by Independent Data Monitoring Committee)
• Review of emerging data - safe & ethical to continue? • Futility assessment Analysis
Analysis of primary endpoint
• maturity of data, ITT or PP populations
Estimate of treatment effect & of precision of estimate
• 95% confidence interval
Subgroups/exploratory or hypothesis generating analyses
• Multiplicity Adjustment
25

CMPath Training 9 Feb 2018
Trial considerations: Null hypothesis 26
• It is simpler to set out to disprove a hypothesis than to prove it
e.g. in a metastatic breast cancer trial of A vs B:
Response rate A = 53% Response rate B = 20%
The null hypothesis is that the treatments are equally effective in the
population of all metastatic breast cancer patients (there is no true
difference in response rates)
The alternative hypothesis is that there is a true difference in response
rates for A & B.
Note: difference could be in either direction; alternative hypothesis is “2-
sided”
• The declaration of a null hypothesis (often a statement that there is no
difference) is the first step in any statistical test of significance

CMPath Training 9 Feb 2018
Statistical fundamentals: Significance test 27
• After defining the null hypothesis, the main question is:
If the null hypothesis were true, what are the chances of getting a
difference at least as big as that observed?
e.g. in the breast cancer trial, if there really is no true difference
between the 2 drugs in terms of tumour response, what is the
probability of observing a treatment difference as large (or even
larger than) 53% versus 20%?
• This probability (the p-value) is determined by applying an
appropriate statistical significance test
• There are different significance tests for different types of data, but
the principle is the same

CMPath Training 9 Feb 2018
Statistical fundamentals: What is a p-value? 28
• p-value: probability of obtaining data as extreme (or more extreme)
than that observed, if null hypothesis is true
• The smaller the p-value, the less likely the sample results could have
occurred by chance if the null hypothesis were true (greater statistical
significance)
• Statistical tables provide p-values for statistical test values
“Degrees of freedom“ relates
to number of observations,
number of categories being
compared etc (depends on the
test)

CMPath Training 9 Feb 2018
Statistical fundamentals: Significant or not significant?
29
Arbitrary cut-off of p<0.05 often used to indicate statistical significance,
but better to present exact p-values & interpret accordingly
e.g. would you interpret p=0.04 very differently from p=0.06?
Note!!!
“Not significant” does not automatically mean that there is no actual
difference (we can’t prove the null hypothesis), but merely that we have
been unable to show evidence of a difference with certainty
i.e. “No evidence of an effect” is NOT the same as “evidence of no effect”
– this is subtle but important
Reasons for non-significant results include: no true difference in the
population, sample size may be too small, estimates too imprecise, bias

CMPath Training 9 Feb 2018
Statistical fundamentals: Statistical versus clinical significance
30
Size of the p-value depends on observed difference & sample size
• If sample size is small, results may produce a p-value which is not
statistically significant, even if there is actually a large true difference
• If sample size is large, small observed differences (which may be
clinically irrelevant) may achieve statistical significance
• Need to think about what size differences are clinically important in
order to interpret statistical significance results sensibly
e.g. supposing we found a mean difference in age of 5 years between 2
groups of patients
In a small study, this difference might not be statistically significant, but in
a much larger study might be highly statistically significant. So what?!
Need to use clinical judgement to decide whether 5 years is clinically
important (not a statistical decision)

CMPath Training 9 Feb 2018
Statistical fundamentals: Confidence intervals & hypothesis testing (1)
31
Significance tests help us decide whether or not study results are compatible
with a hypothesis
BUT they provide no information on the size of the difference
e.g. in the breast cancer trial, the 33% difference in tumour response rates
was statistically significant with p<0.001
Confidence intervals help us to estimate the size of the difference with some
measure of precision
e.g. 95% CI for the 33% difference in response rates in the breast cancer
trial is:
95% Confidence Interval (20.5% to 45.5%)
i.e. we are 95% confident that real difference between A & B tumour
response is between 20.5% & 45.5%

CMPath Training 9 Feb 2018
Statistical fundamentals: Confidence intervals & hypothesis testing (2)
32
• There is a link between p-values & CIs
• If 95% CI for a difference does not include the null hypothesis value of 0,
p<0.05
• If this CI includes the null hypothesis value, p>0.05
In the e.g., the null hypothesis is that there is no difference between the
tumour response rates in the population (i.e. the null hypothesis value = 0)
Does the 95% CI for the 33% difference in response rates include 0?
No (20.5% to 45.5%), so we can infer that p<0.05

CMPath Training 9 Feb 2018

CMPath Training 9 Feb 2018

CMPath Training 9 Feb 2018
Statistics is …about understanding data
It is NOT just about hypothesis testing and p-values - a statistically significant result may not be clinically important or vice versa
Confidence Intervals (95%) give information on the precision and clinical significance of an observed effect
Subgroup analyses
– open to abuse and mis-interpretation “the more you look the more you find” – adjustment for multiple testing, biological plausibility,
– quantitative vs qualitative treatment interactions - if overall trial no effect, identification of sensitive subgroup implies subgroup where treatment confers harm
And finally…..
Correlation is a measure of association – not of agreement (Bland-Altman methods required for Method Comparison analyses)
35
Statistics – the fundamentals

CMPath Training 9 Feb 2018
Further reading Books:
Clinical Trials. A Practical Approach. Stuart J Pocock. Wiley 1983
Cancer Clinical Trials. Methods and Practice. Edited by Marc Buyse, Maurice Staquet, Richard Sylvester. Oxford Medical Publications. 1984
Internet:
www-users.york.ac.uk/~mb55/pubs/pbstnote.htm BMJ Statistics Note series (Doug Altman & Martin Bland) OR on BMJ website (Research methods & reporting section)
www.ct-toolkit.ac.uk/ MRC DoH Clinical Trials Toolkit
http://csg.ncri.org.uk/portfolio/portfolio-maps/ cancer clinical studies within the NIHR portfolio
www.clinicaltrials.gov US NIH service – general information
And finally…….. (Power, P-values, publication bias, statistical evidence)
https://www.youtube.com/watch?v=kMYxd6QeAss
36