Embed Size (px)
Citation preview

ava i l ab l e a t www.sc i enced i r ec t . com
C l i n i ca l Immuno logy
www.e l sev i e r . com / l o ca t e / y c l im
Clinical Immunology (2013) 149, 345 –355
REVIEW
Trials in type 1 diabetes:Antigen-specific therapies
a c a, b,
Ken T. Coppieters , Leonard C. Harrison , Matthias G. von Herrath ⁎a Type 1 Diabetes R&D Center, Novo Nordisk Inc., Seattle, WA, USAb Type 1 Diabetes Center, The La Jolla Institute for Allergy and Immunology, La Jolla, CA, USAc TheWalter and Eliza Hall Institute of Medical Research and Department of Clinical Immunology and Burnet Clinical Research Unit,
The Royal Melbourne Hospital, Melbourne, AustraliaReceived 1 February 2013; accepted with revision 5 February 2013Available online 15 February 2013
⁎ Corresponding author at: Type 1 DiE-mail address: [email protected] (
1521-6616/$ - see front matter © 2013http://dx.doi.org/10.1016/j.clim.201
KEYWORDSType 1 diabetes;Antigen-specific therapies;Immune intervention;Clinical trials
Abstract Type 1 diabetes (T1D) results from an aberrant immunological response against theinsulin-producing beta cells in the islets of the pancreas. The ideal therapy would restore immunebalance in a safe and lasting fashion, stopping the process of beta cell decay. The efficacy ofimmune suppressive agents such as cyclosporin underscores the notion that T1D can in principlebe prevented, albeit at an unacceptable long-term safety risk. Immune modulatory drugs such asmonoclonal anti-CD3 antibody, on the other hand, have recently had rather disappointing results in
phase 3 trials, possibly due to inadequate dosing or choice of inappropriate endpoints. Therefore, itis argued that striking the right balance between safety and efficacy, together with careful trialdesign, will be paramount in preventing T1D. Here we outline the concept of antigen-specifictolerization as a strategy to safely induce long-term protection against T1D, focusing on availableclinical trial data, key knowledge gaps and potential future directions.© 2013 Elsevier Inc. All rights reserved.abetes Center, The La Jolla InsM.G. von Herrath).
Elsevier Inc. All rights reserve3.02.002
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3462. Immune suppression versus immune modulation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3463. Antigen-specific tolerance: concepts and advantages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3474. Antigen-specific therapy trials in T1D . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 348
4.1. (Prepro)insulin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3484.2. Glutamic acid decarboxylase (GAD) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3504.3. 60 kDa heat-shock protein (HSP60, p277) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 351
5. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 351Conflict of interest statement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 352References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 352
titute for Allergy and Immunology, La Jolla, CA, USA.
d.

346 K.T. Coppieters et al.
1. Introduction
The development of dysglycemia in T1D represents the endstage of a period of silent, immune-mediated beta cell decay[1]. Around the time of diagnosis it is estimated that upto 90% of functional beta cell mass is destroyed, althoughmost patients still produce variable amounts of insulin asmeasured by C-peptide secretion. The natural course of T1Dprior to diagnosis remains elusive, but relatively accuraterisk predictions can be performed based on genetic screen-ing and detection of islet autoantibodies.
It is well established that effector mechanisms in T1D areprimarily T cell-driven, as attested to by the predominance ofT cells in the characteristic islet infiltrate after diagnosis [2]and the ability of certain T cell clones to directly kill beta cells[3]. Replenishing the functional beta cell pool by transplanta-tion or regeneration of insulin-producing cells does not offer alongstanding cure without prevention, since these cells will berecognized and attacked by persisting autoreactive memoryT cells [4]. Curing T1D will therefore require a preventativetreatment to keep autoreactive T cells in check.
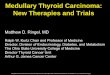
Figure 1 Staging of clinical trials in type 1 diabetes. The toppanel shows the different disease stages with correspondingrates of beta cell mass decline and associated trial terminology.Lower panel indicates the fact that prevention trials are morecostly, take more time but have a more clinically relevantendpoint (diabetes prevention) than intervention trials (C-peptidepreservation). Intervention trials tend to offer a more stringenttherapeutic setting yet are associated with easier recruitment andhigher patient motivation.
2. Immune suppression versusimmune modulation
The outcomes of several trials using immune suppressiveor immune modulating agents clearly indicate that interfer-ence with the immunological mechanisms of T1D can improvebeta cell survival. Immune-mediated interventions in T1D cangenerally be classified according to their timing relative toclinical diagnosis (Fig. 1). In primary prevention, the aim is toprevent the development of islet autoimmunity, usuallydefined as the occurrence of islet autoantibodies. In second-ary prevention the aim is to prevent healthy autoantibody-positive individuals from progressing to overt dysglycemia.Finally, in intervention studies (sometimes termed ‘tertiaryprevention’) the aim is to prevent loss of residual beta cellfunction after diagnosis, as measured by the primary endpointof C-peptide secretion, and the secondary endpoints ofglycemic indices such as fasting and post-prandial bloodglucose, HbA1c or insulin requirement.
Casting any potential therapy within these stages isparticularly difficult, as each has its own stringency parame-ters and ethical considerations (Fig. 1). Thus, primary andsecondary prevention may be mechanistically easier toachieve as compared to treatment of advanced disease atdiagnosis. From an ethical perspective, however, treatment ofhealthy individuals demands a zero sum side-effect profile.Animal models roughly support the idea that prevention isindeed easier to achieve earlier, in the pre-clinical stage.Literally hundreds of experimental treatments are known toreduce the incidence of diabetes in the NODmouse model, yetvery few can induce remission after the onset of hyperglyce-mia [5]. Those that have, e.g. anti-CD3 antibody and bonemarrow conditioning, are associated with significant safetyrisks.
Non-specific immune suppressive agents broadly inhibitthe components of the immune system that underlie T1D.Experience with the calcineurin inhibitor cyclosporin A hastaught us that preservation of beta cell function can indeed be
achieved, with many patients experiencing prolonged periodsof insulin independence [6,7]. However, the effect was notsustained upon treatment discontinuation and cyclosporintherapy resulted in accelerated renal dysfunction [8]. Similarrisk–benefit considerations apply to the use of autologoushematopoietic stem cell transplantation in T1D [9]. Evidently,these approaches are not suitable for prevention, especiallywith a target population that is predominantly pediatric.
Thus, the case can be made that chronic non-specificimmune suppression has an unacceptable risk–benefit ratiofor wide adoption in T1D. Immuno-modulatory treatments,such as biologicals directed against immune receptors, couldtheoretically curb pathogenic autoimmunity while avoidingmany of the risks associated with general immune suppres-sion. Examples from recent trials include CTLA-4Ig [10](abatacept), anti-CD20 [11] (rituximab) and anti-CD3 [12,13](teplizumab/otelixizumab). These agents are designedto block critical signaling pathways in disease-associatedleukocyte subsets and/or stimulate the function of regulatoryT cells in the hope that a short course will confer long-termtolerance and avoid the need for ongoing treatment. Indeed,it would be difficult to justify chronic co-stimulatoryinhibition, B or T cell depletion in T1D. Unfortunately, recentimmune modulation trials in recent-onset T1D have shownonly short-lasting preservation of C-peptide secretionfollowed by a decline parallel to placebo.
High hopes were initially held for non-mitogenic anti-CD3antibodies, based on animal studies indicating that theycould effectively reverse diabetes in several T1D models[14,15]. Mechanistically, benefit was achieved via effects on

347Trials in type 1 diabetes: Antigen-specific therapies
both autoreactive and regulatory T cell compartments andtreatment appeared to be reasonably safe. Early clinicaltrials confirmed these findings and two large phase 3 trialswere initiated, which unfortunately failed to meet theirprimary endpoints [16]. While we will not elaborate on thepotential reasons for these failures, we wish to highlightthat, as opposed to immune suppressive agents, the efficacyof these more subtle immunomodulatory approaches likelydepends on several pivotal parameters, such as dosing,timing, inclusion criteria and defined endpoints. Optimizationof these parameters is required lest a beneficial outcome isobscured. On a positive note, the favorable safety profile doesnot appear to preclude a secondary prevention setting, andTrialNet is currently recruiting for a trial of non-mitogenicanti-CD3 antibody in participants at high risk for T1D(NCT01030861).
In conclusion, the modest preservation of beta cellfunction achieved with immune modulation would implythat higher doses or longer treatment durations, or combi-nations with other agents, are required. It is uncertainwhether the risk–benefit ratio will remain favorable undersuch conditions.
3. Antigen-specific tolerance: conceptsand advantages
The default immune response to foreign protein antigens isactivation. This is unless the antigen is delivered andpresented to the immune system in a way that promotesignorance or tolerance. The mucosal immune system has longbeen known as a potent inducer of immunological tolerance.In 1911, H. Gideon Wells first described the effect of repeatedoral administration of proteins such as hen's egg protein toguinea pigs [17]:
‘Guinea-pigs fed upon a certain protein are at first renderedsensitive to this protein. After some time, however, if the
feeding is continued they become less sensitive, until they reachan immune or refractory condition so that they do not react totwo spaced injections of the fed protein.’
More than one hundred years later, this therapeuticconcept is still subject to intense investigation. Indeed, arecent phase 2 clinical trial on oral immunotherapy for eggallergy in children showed remarkable desensitizationfollowing daily feeding of high doses (gram range) of eggwhite [18].
The same concept of antigen-specific oral toleranceinduction has proven successful in a range of animal modelsfor autoimmunity, including arthritis [19], multiple sclerosis[20] and type 1 diabetes [21]. Other modes of mucosal (nasal[22,23]) and non-mucosal (subcutaneous [24]) antigen deliv-ery, alone or in combination with specific adjuvants, wereexplored and promising data were obtained showing thatantigen-specific tolerance induction can prevent and in someinstances even revert T1D. Despite the extensive dataset inmouse models, clinical translation has proven extremelydifficult in autoimmune diseases. In rheumatoid arthritis, amixed efficacy record was compiled throughout numeroustrials, of which many used different dosages and sources ofcollagen [25]. A recent phase 3 trial provides further evidence
for therapeutic efficacy of oral collagen administration withan advantage over the standard-of-care, methotrexate, andwith fewer side effects [26]. In multiple sclerosis, the oraladministration of myelin showed initial promise [27], yet aphase 3 trial by the company Autoimmune (Myloral; bovinemyelin) was unsuccessful. Here, the lack of proper dosefinding studies was criticized, which may have rendered thetreatment inefficacious due to suboptimal dosing [28].Collectively, these studies underscore that whereas antigen-specific therapy is reliably safe, its outcome critically dependson a variety of factors, such as disease stage and dosing, asdefined in detail in corresponding animal models. We willfurther argue below that, within the context of T1D, the pathtowards clinical translation of antigen-specific therapy forautoimmune disorders can be improved.
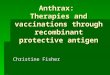
The cellular immunology of antigen-specific tolerance iswell-characterized in mice and typically involves the genera-tion and expansion of antigen-specific regulatory T cells (Treg)(Fig. 2) [29]. In oral tolerance, the importance of the Peyer'spatches as the immunological target should be mentioned, asmice lacking these structures fail to develop tolerance againstoral proteins [30]. Gamma delta T cells, the predominant T celltype in themucosa, are also crucial mediators of oral tolerance[31]. Once generated, antigen-specific Treg then circulate andare capable of regulating inflammatory responses locally wherethey again see their cognate antigen, e.g. within the pancreaticlymph nodes (PDLN) and islets in T1D (after oral or nasalinsulin). The specificity of these cells would theoreticallyrestrict their regulatory potential to the antigen that theyrecognize. However, a process termed linked suppression,originally discovered in the field of transplantation immunol-ogy, is thought to enable the antigen-specific Treg to controlresponses against antigens that are presented on the sameantigen presenting cell (APC). In transplantation, this meansthat once tolerance is established against antigens in atransplant, linked suppression will occur against any thirdparty antigen that is subsequently co-transplanted with theoriginal tissue [32]. In T1D, the implication is that antigen-specific therapy based on a single islet antigen would ensurethat ongoing autoimmune responses against other islet antigensare also regulated. The fact that any antigen other than the oneused for tolerization must be presented on the same APC asthe tolerizing antigen reduces the likelihood of unwantedsuppression of normal immune responses. This concept wouldexplain why mucosal immunization with for instance insulinalso regulates T cell responses in the PDLN against otherimmunodominant islet antigens such as GAD or IGRP. Thismechanism is particularly important because significant inter-individual variation exists in the autoreactive T cell repertoirein patients [2] and even in inbred NOD mice [33].
Before proceeding to an overview of clinical trials ofantigen-specific therapy in T1D we would like to emphasizethe importance of biomarker discovery and validation. Apertinent example is the measurement of autoantibodies inorder to predict the development of regulatory responsesagainst an autoantigen. In the NOD mouse, insulin autoanti-bodies are considered the most reliable marker of autoimmu-nity [34]. Bresson and coworkers [35] recently showed that inNOD mice the presence of insulin autoantibodies prior totreatment with oral insulin/anti-CD3 combination predicts abeneficial outcome. Other immune biomarkers such asregulatory cytokine responses to islet antigens [36–38] or

Figure 2 Antigen-specific tolerance induction and the concept of linked suppression. The mucosal immune system has the uniquecapacity to propagate the induction of antigen-specific regulatory T cells (Treg). These Treg subsequently regulate immune responsesas shown here in the pancreatic draining lymph nodes. In type 1 diabetes, islet antigens are constantly drained from the pancreas byantigen-presenting cells (APC). Treg subsequently recognize the tolerizing antigen (here antigen A) and promote a regulatoryresponse. Linked suppression would then account for a similar response to an unrelated antigen that is presented by the same APC(here antigen B). Treg are known to act via suppressive cytokines or contact-dependent mechanisms on both other T cells and APC.
348 K.T. Coppieters et al.
autoreactive T cell frequencies [39] could help to better assessthe efficacy of tolerization therapy in relation to parameterssuch as dose and administration route in small proof-of-concepttrials. An essential knowledge gap is the extent to which theseimmune markers vary by individual during the natural course ofT1D progression.
4. Antigen-specific therapy trials in T1D
4.1. (Prepro)insulin
Among islet autoantigens in T1D, insulin is the only proteinrestricted to beta cells (excluding the immune systemitself), all other known T1D autoantigens being producedby other non-immune cell types. It is well-known that insulin
is a major autoantigen in the NOD model [40,41] andevidence is mounting that insulin-reactive T cells playimportant roles in T1D. Insulin-specific CD4 [42] and CD8[43] T cells are found in increased frequencies in theperipheral blood of patients and certain patient-derivedPPI-specific CD8 T cells can directly kill beta cells in vitro[3]. Moreover, the insulin gene is second to only MHC class IIgenes in terms of genetic risk association, and its increasedexpression in the thymus confers protection [44]. Thus,plenty of reasons exist to assume a cardinal role for insulin asan autoantigen in T1D.
Several trials aimed at tolerizing the immune systemagainst insulin in T1D have been conducted (Table 1). Oraladministration of whole insulin has consistently resulted indisease prevention in spontaneous [21] and induced [45]animal models. One conclusion from these studies is that the

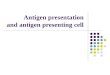
Table 1 Antigen-specific therapies described in this review article. This article almost solely focusses on larger controlled trials,some small proof-of-concept trials are included that are of particular interest. The trials are listed according to their order ofappearance in this article.
Trial designation+ref. Design Outcome
(prepro)InsulinDiabetes Prevention Trial (DPT-1) [47](oral insulin)
Secondary prevention No delay, post hoc subgroup effectidentified
NCT00419562 (oral insulin) Secondary prevention Currently recruiting, results expectedFebruary 2014
IMDIAB [48] Recent-onset No preservation of beta cell functionDiabète Insuline Orale group [49] Recent-onset No preservation of beta cell functionMacLaren et al. [50] Recent-onset No preservation of beta cell functionType 1 diabetes prediction and prevention(DIPP) [54] (nasal insulin)
Secondary prevention No delay
Intranasal insulin trial (INIT-1) [52] Safety trial in prevention Safe, no delay or acceleration, INIT-II trialongoing (NCT00336674)
Fourlanos et al. [55] Recent-onset No preservation of beta cell functionPrimary Oral/intranasal INsulin Trial(Pre-point) [56] (oral/nasal insulin)
Primary prevention Recruiting
Diabetes Prevention Trial (DPT-1) [58](parenteral insulin)
Secondary prevention No delay
Belgian Diabetes Registry [99](parenteral insulin)
Secondary prevention No delay
Proinsulin peptide vaccination [36] Safety trial in longstandingdisease
Safe, immunological tolerance signsobserved
Insulin B chain vaccination [37] Safety trial in recent-onset Safe, immunological tolerance signsobserved
GAD65GAD-alum [75,76] Dose-escalation study in LADA Safe, beta cell function preservation
with 20 μg doseGAD-alum [77] Recent-onset Beta cell function preservationGAD-alum (TrialNet) [82] Recent-onset No preservation of beta cell functionGAD-alum (Europe) [83] Recent-onset No preservation of beta cell functionGAD-alum (U.S., DIAPREVENT, NCT00751842) Recent-onset SuspendedDiabetes prevention — Immune Tolerance(DIAPREV-IT; NCT01122446)
Secondary prevention Ongoing, fully enrolled
HSP60 (p277)DiaPep277 pilot trial [89] Recent-onset Evidence of beta cell preservationHuurman et al. [91] Recent-onset Trend for beta cell preservationLazar et al. [92] Recent-onset No trend for beta cell preservationSchloot et al. [93] Recent-onset Trend for beta cell preservationBuzzetti et al. [94] Recent-onset Trend for beta cell preservationDiaPep277 phase III trial(www.andromedabio.com/news.php)
Recent-onset Evidence of beta cell preservation,confirmatory trial ongoing
349Trials in type 1 diabetes: Antigen-specific therapies
dose–efficacy curve is markedly bell-shaped [46], i.e. thatthe dose cannot be too low or too high and therefore needsto be carefully determined. Furthermore, the type of insulinsignificantly matters, as different optimal doses were foundfor porcine and human insulin, even though there is verylittle sequence difference. In addition, denaturing a proteingenerally abolishes its ability to induce oral tolerance,highlighting the requirement for intact whole protein.
Most mouse studies found an optimal dose within thesingle digit milligram range, given intra-gastrically twiceweekly in a relatively large (~0.5 ml) volume of buffer. Thelargest human trial that tested oral insulin in a secondaryprevention setting was the Diabetes Prevention Trial (DPT-1)
trial [47]. Here, a 7.5 mg dose of human insulin crystals wasgiven daily in non-enterocoated capsules with methylcellu-lose filler. Children who were unable to swallow the capsuleswere allowed to sprinkle the contents over their food or injuice. The investigators considered extensive breakdown ofinsulin in the GI tract as beneficial to avoid hypoglycemia,although insulin alone without an adsorption enhancingagent has never been shown to cross the mucosal barrier.The trial showed no overall protective effect, although asubgroup effect was seen in participants with pre-existinghigh circulating concentrations of insulin autoantibodies.A number of potential explanations exist for the apparentlack of efficacy. First, the dose was arbitrarily chosen and

350 K.T. Coppieters et al.
extrapolation from mouse studies would predict an optimaldose that is several hundred fold higher. Second, insulinis particularly prone to denaturation and degradation, andit can be questioned whether autoantigen would bebioavailable after GI passage. Third, patient inclusion mayneed to be based on the pre-existence of insulin autoanti-bodies, as demonstrated in mouse studies [35]. A TrialNetstudy (NCT00419562) is currently recruiting participants toassess this assumption. Other unsuccessful trials of oralinsulin in recent-onset T1D, including the IMDIAB [48],Diabète Insuline Orale group [49] and that by the MacLarengroup [50] used similar low doses of insulin, daily dosing andno enteroprotective delivery. Our studies in collaborationwith Entelos Inc. showed, at least for tolerization by nasalinsulin peptide, that high frequency dosing, used in mostmouse studies, is less effective than low frequency dosing[51]. In summary, clinical trials involving oral tolerance inT1D have so far largely disregarded what we think areimportant lessons from animal models.
An alternativemode of mucosal administration, nasal insulininhalation, was characterized in the NOD mouse model [22].Here, it was argued that, in contrast to oral insulin, nasaladministration preserves the antigenic structure up untilimmediate contact with the nasopharyngeal mucosa. Theintranasal insulin trial I (INIT I) in humans with islet autoanti-bodies at risk for T1D demonstrated both safety and biomarkereffects [52] and is the basis for the ongoing INIT II with clinicaldiabetes as the primary outcome measure (reviewed in [53]).However, in the meantime a large trial of daily nasal insulin inislet autoantibody-positive children at much higher risk for T1Dthan participants in INIT II found no effect on progression todiabetes [54]. A recent trial in new-onset patients also found alack of effect on C-peptide preservation, yet revealed im-munological changes suggestive of tolerance induction [55].The question therefore remains whether this immunologicaltolerance signature can be optimized and exploited to conferclinically relevant beta cell preservation. The Pre-POINT trialwhich is currently enrolling aims to identify optimal timing,disease stage, dose and route of administration by interveningwith oral insulin in genetically at-risk children before theappearance of islet autoantibodies [56].
Subcutaneous administration of insulin prior to diagnosis hasbeen explored as a secondary prevention strategy, based onencouraging data in animal models [24] and a small pilot trial[57]. Efficacy was however not substantiated in a large cohortof high-risk individuals in the DPT-1 study group [58]. Alter-native subcutaneous vaccination approaches include insulin Bchain administration in IFA [37], proinsulin peptide [36] andproinsulin DNA [59]; although some evidence was gathered insupport of tolerogenic capacity these remain to be assessed forefficacy in larger trials. So-called altered peptide ligands (APL),i.e. insulin peptides that have been designed to interact withTCRs in a tolerogenic manner, have also been considered, butdisease exacerbation with APL was seen in multiple sclerosisand extreme caution is obviously advised [60].
4.2. Glutamic acid decarboxylase (GAD)
More than two decades ago, the T1D-associated beta cellautoantigen, until then known by its molecular weight ‘64K’,was identified as GAD, an enzyme that catalyzes the
rate-limiting step in the biosynthesis of the inhibitoryneurotransmitter GABA (γ-aminobutyric acid) [61]. At leasttwo isoforms of GAD exist in mammals, with molecularweights of 65 kDa (GAD65) and 67 kDa (GAD67), of whichGAD65 is the main immunogenic isoform in T1D [62].Autoreactivity against this protein is associated withpreclinical and recent-onset T1D [63] and measurement ofGAD65 autoantibodies is a sensitive and specific diagnostictool for islet autoimmunity in modern day clinical practice.Evidence indicates however that GAD65 autoantibodies perse are associated with relatively indolent islet autoimmunityand, in the absence of other islet autoantibodies, have lowpredictive value [64,65]. GAD65 autoreactivity is also foundin a rare neurological condition called Stiff Person Syndrome(SPS), which is characterized by symmetrically increasedaxial muscle tone and a high prevalence of T1D [66]. Of note,GAD65 autoantibodies in SPS differ from those in T1D interms of isotype and epitope recognition [67]. GAD is widelydistributed in the nervous system but is also found in othertissues, including the pancreatic islets, specifically the betacells. The NOD mouse also exhibits humoral autoreactivity toendogenous GAD [68], and T cell reactivity to human GAD65was found to play an essential role in the disease process inthis model [69,70]. However, in a subsequent workshop, notall labs could not confirm these T cell results and Jaeckel et al.[71] could not show that transgenic GAD65, unlike proinsulin,prevented diabetes in the NOD mouse. Mouse beta cellsexpress mainly GAD67 while human beta cells express onlyGAD65. In agreement, various approaches to tolerize the NODmouse immune system against GAD have proved successful[23,72,73]
The formulation chosen by Diamyd for its clinical trialswas subcutaneous GAD65 in aluminum hydroxide (alum), aconventional adjuvant in childhood vaccines. This adjuvantwas included in order to steer away from a Th1-dominatedcellular immune response in T1D in favor of a Th2 humoralresponse, and to minimize the antigen dose required [74].Dose escalation studies performed in adults with T1Drevealed an optimal dose of 20 micrograms (given twice,four weeks apart) but not higher or lower, line with thenotion that correct dosing is pivotal in antigen-specifictolerance therapy [75]. The effect on insulin dependence inthe 20 microgram group was still evident after five years,suggesting long term tolerizing effects [76]. A phase II trial inrecently diagnosed children and adolescents with T1D wasthen conducted and reported delayed loss of C-peptidesecretion following a single course of therapy, especially inthose with short disease duration [77]. This beneficial effectand associated favorable safety profile was later reported tobe preserved after 4 years follow up [78]. Immunologicalevidence for tolerance induction was gathered, whichincluded the detection of GAD65-specific Treg [79], de-creased Ag-specific Th1 responses [80] and T cell inhibitorypathways upon Ag stimulation [81].
A subsequent TrialNet phase 2 trial of GAD-alum in patientswith newly diagnosed T1D did not show any clinical benefit.Here, two or three doses of subcutaneous GAD-alum across4–12 weeks were given to patients within 100 days ofdiagnosis [82]. The results from a Diamyd phase 3 trial weresimilarly disappointing, with no significant effects onC-peptide preservation, insulin dose, glycated hemoglobinlevel, or hypoglycemia rate [83]. A significant problem with

351Trials in type 1 diabetes: Antigen-specific therapies
these studies has been the lack of proof of concept in mousemodels with the GAD-alum drug, which in hindsight makes itimpossible to address such issues as dosing and the develop-ment of appropriate biomarkers for efficacy. In addition,these stories should caution us about over-interpretingpositive phase 2 trials, in which the number of patients isrelatively small and the observations might not hold up inlarger cohorts, in which greater heterogeneity can beexpected. The heterogeneity of T1D natural history, presum-ably reflecting a range of genetically- and environmentally-determined pathological mechanisms, is an importantreason why we need to develop a ‘personalized’ approachto biomarkers. Nevertheless, the GAD-alum vaccine mightstill be beneficial for prevention of T1D or could become acomponent of a combination therapy protocol in recent-onsetT1D. An ongoing secondary prevention trial (DIAPREV-IT;NCT01122446) may provide more information.
4.3. 60 kDa heat-shock protein (HSP60, p277)
The role of HSP60 as a putative autoantigen in the NODmouse was first reported by Elias and coworkers [84]. Later,a specific HSP60-derived peptide (p277) was identified thathad the ability to confer protection in mice [85,86] and toinduce disease in non-susceptible strains after vaccination[87]. Some support exists for an antigenic role for hsp60 inpatients with T1D [88], yet the available data indicate a lessimmunodominant role in comparison to insulin and possiblyGAD65.
The compound tested in clinical trials (DiaPep277, TEVAPharmaceuticals) contains two amino acid substitutions in thenative p277 sequence to stabilize the peptide, but does notfunction as an APL. A pilot trial in 2001 tested the effect ofthree subcutaneous 1 mg p277 injections in a 10% lipidsolution, at entry, 1 month, and 6 months in recentlydiagnosed T1D patients [89]. Positive outcomes were recordedpertaining to glucagon-stimulated (GST) C-peptide preserva-tion and exogenous insulin requirements. Interestingly, atemporary increase of glucagon-stimulated C-peptide in thetreatment group was observed after each P277 injection.These data generated support for the idea that a highly safeantigen-specific treatment could reverse the natural course ofT1D even after clinical diagnosis. The mechanism of actionwas proposed to involve altered (Th2-skewed) T cell reactivityto hsp60 and p277, and also direct binding to TLR2 on Treg,enhancing their regulatory potential [90]. A number of othersmall trials were conducted, which all showed excellentsafety, yet were not powered to provide conclusive evidencefor efficacy [91–94]. In the trial by Huurman et al. [38]the clinical response to p277 was associated with proliferationof T cells to p277, which might serve as a biomarker.
TEVA Pharmaceuticals has now completed a phase 3 trial, inwhich preservation of C-peptide secretion to glucagon (but notto a mixed meal tolerance test) showed reduction in thefrequency of hypoglycemia and in insulin usage (http://www.andromedabio.com/news.php). It is interesting to note thatthe dose that was used (1 mg s.c. at monthly intervals inoil-based adjuvant) was associated with reduction of hypogly-cemia frequency but preservation of C-peptide secretion wasoptimal at higher doses, as in Huurman et al. (lowest decreaseof C-peptide at 2.5 mg) [91]. A further phase 3 trial has recently
completed recruitment. Taken together, these data offersubstantial grounds for the hypothesis that antigen-specifictherapies are safe and powerful enough to tackle even theadvanced stages of disease. The immune biomarkers need to befurther developed but preliminary data suggest that efficacy atleast in part correlates with an altered immune responseagainst the immunizing antigen.
5. Conclusions
There is now reason to be cautiously optimistic that immuneintervention can alter the course of beta cell decline in T1D.However, we have yet to find a therapy that strikes the rightbalance between safety and efficacy. The risks associated withchronic immune suppression clearly outweigh the benefits andthese drugs have failed to stably restore immune tolerance.Immune modulatory agents such as anti-CD3 antibody have sofar not fulfilled their potential in large clinical trials and otherbiologicals have provided only temporary stabilization ofC-peptide secretion. We have argued here that antigen-specific therapies may represent a more suitable approach inT1D, in particular given the excellent safety record compiledacross various clinical studies.
Has the clinical potential of antigen-specific therapy forT1D been unequivocally demonstrated in the clinic? Certainlynot. The trial data with p277 in recent-onset T1D actuallyrepresents the first and only available phase 3 evidence of atolerizing effect after antigen-specific therapy. The efficacyrecord of oral and nasal antigen delivery in animal modelshas thus far failed to move forward from bench to bedside. Ofnote, many antigen-specific therapies tend only to workprior to onset in pre-clinical models, whereas most clinicaltesting occurs in a recent-onset setting. Quite clearly, ethicalconsiderations and the shorter trial duration are at play but thechoice to treat very advanced disease also sets the bar forclinical efficacy very high. Here, we believe that combinationtherapies may be the answer. One important advantage couldbe that the complementary action of two drugs may allow dosereductions and thereby the risk for side-effects. Additionally,it is easy to envision how two drugs with unrelated modesof action could impact the immune system more broadly,confer better protection and perhaps even induce remission.There is pre-clinical evidence to support this line of thought,for instance showing improved efficacy after combiningnasal insulin and anti-CD3 [95]. Promising new formulationapproaches, such as antigen-coated microparticles [96],peptide-MHC-based nanovaccines [97] or antigen-linked au-tologous cell transfer [98], could serve as alternatives toimprove the efficacy of antigen-specific tolerization.
Finally, it can be argued that better informed decisions arerequired on the important variables of antigen dose-formulationand frequency, and disease stage, of administration. Despitethe shortfalls of animal models, they are undeniably still thebest available means of evaluating the aforementioned param-eters. Finally, to better position and assess the outcome ofantigen-specific interventions, we require suitable immunebiomarkers to identify the most appropriate target populationand correlate immune function with clinical benefit. Failure toconsider the importance of these variables in past trials is alesson for the future that may eventually allow the translationof antigen-specific therapies from mouse to man.

352 K.T. Coppieters et al.
Conflict of interest statement
KTC and MTvH are both employed by Novo Nordisk.
References
[1] T.L. van Belle, K.T. Coppieters, M.G. von Herrath, Type 1diabetes: etiology, immunology, and therapeutic strategies,Physiol. Rev. 91 (2011) 79–118.
[2] K.T. Coppieters, F. Dotta, N. Amirian, P.D. Campbell, T.W. Kay,M.A. Atkinson, B.O. Roep, M.G. von Herrath, Demonstration ofislet-autoreactive CD8 T cells in insulitic lesions from recentonset and long-term type 1 diabetes patients, J. Exp. Med. 209(2012) 51–60.
[3] A. Skowera, R.J. Ellis, R. Varela-Calvino, S. Arif, G.C. Huang,C. Van-Krinks, A. Zaremba, C. Rackham, J.S. Allen, T.I. Tree,M. Zhao, C.M. Dayan, A.K. Sewell, W.W. Unger, J.W. Drijfhout,F. Ossendorp, B.O. Roep, M. Peakman, CTLs are targeted to killbeta cells in patients with type 1 diabetes through recognitionof a glucose-regulated preproinsulin epitope, J. Clin. Invest.118 (2008) 3390–3402.
[4] G. Tyden, F.P. Reinholt, G. Sundkvist, J. Bolinder, Recurrenceof autoimmune diabetes mellitus in recipients of cadavericpancreatic grafts, N. Engl. J. Med. 335 (1996) 860–863.
[5] L.K. Shoda, D.L. Young, S. Ramanujan, C.C. Whiting, M.A.Atkinson, J.A. Bluestone, G.S. Eisenbarth, D. Mathis, A.A.Rossini, S.E. Campbell, R. Kahn, H.T. Kreuwel, A comprehensivereview of interventions in the NOD mouse and implications fortranslation, Immunity 23 (2005) 115–126.
[6] G. Feutren, L. Papoz, R. Assan, B. Vialettes, G. Karsenty, P.Vexiau, R.H. Du, M. Rodier, J. Sirmai, A. Lallemand, Cyclosporinincreases the rate and length of remissions in insulin-dependentdiabetes of recent onset. Results of a multicentre double-blindtrial, Lancet 2 (1986) 119–124.
[7] Cyclosporin-induced remission of IDDM after early intervention.Association of 1 yr of cyclosporin treatment with enhancedinsulin secretion. The Canadian–European Randomized ControlTrial Group, Diabetes 37 (1988) 1574–1582.
[8] H.H. Parving, L. Tarnow, F.S. Nielsen, P. Rossing, T.Mandrup-Poulsen, R. Osterby, J. Nerup, Cyclosporine nephro-toxicity in type 1 diabetic patients. A 7-year follow-up study,Diabetes Care 22 (1999) 478–483.
[9] J.C. Voltarelli, C.E. Couri, A.B. Stracieri, M.C. Oliveira, D.A.Moraes, F. Pieroni, M. Coutinho, K.C. Malmegrim, M.C. Foss-Freitas, B.P. Simoes, M.C. Foss, E. Squiers, R.K. Burt, Autologousnonmyeloablative hematopoietic stem cell transplantation innewly diagnosed type 1 diabetes mellitus, JAMA 297 (2007)1568–1576.
[10] T. Orban, B. Bundy, D.J. Becker, L.A. DiMeglio, S.E. Gitelman,R. Goland, P.A. Gottlieb, C.J. Greenbaum, J.B. Marks, R.Monzavi, A. Moran, P. Raskin, H. Rodriguez, W.E. Russell, D.Schatz, D. Wherrett, D.M. Wilson, J.P. Krischer, J.S. Skyler,Co-stimulation modulation with abatacept in patients withrecent-onset type 1 diabetes: a randomised, double-blind,placebo-controlled trial, Lancet 378 (2011) 412–419.
[11] M.D. Pescovitz, C.J. Greenbaum, H. Krause-Steinrauf, D.J.Becker, S.E. Gitelman, R. Goland, P.A. Gottlieb, J.B. Marks,P.F. McGee, A.M. Moran, P. Raskin, H. Rodriguez, D.A. Schatz,D. Wherrett, D.M. Wilson, J.M. Lachin, J.S. Skyler, Rituximab,B-lymphocyte depletion, and preservation of beta-cell func-tion, N. Engl. J. Med. 361 (2009) 2143–2152.
[12] K.C. Herold, W. Hagopian, J.A. Auger, E. Poumian-Ruiz, L.Taylor, D. Donaldson, S.E. Gitelman, D.M. Harlan, D. Xu,R.A. Zivin, J.A. Bluestone, Anti-CD3 monoclonal antibodyin new-onset type 1 diabetes mellitus, N. Engl. J. Med. 346(2002) 1692–1698.
[13] B. Keymeulen, E. Vandemeulebroucke, A.G. Ziegler, C. Mathieu,L. Kaufman, G. Hale, F. Gorus, M. Goldman, M. Walter, S.Candon, L. Schandene, L. Crenier, B.C. De, J.M. Seigneurin, P.P.De, D. Pierard, I. Weets, P. Rebello, P. Bird, E. Berrie, M. Frewin,H. Waldmann, J.F. Bach, D. Pipeleers, L. Chatenoud, Insulinneeds after CD3-antibody therapy in new-onset type 1 diabetes,N. Engl. J. Med. 352 (2005) 2598–2608.
[14] L. Chatenoud, E. Thervet, J. Primo, J.F. Bach, Anti-CD3antibody induces long-term remission of overt autoimmunityin nonobese diabetic mice, Proc. Natl. Acad. Sci. U. S. A. 91(1994) 123–127.
[15] M.G. von Herrath, B. Coon, T. Wolfe, L. Chatenoud,Nonmitogenic CD3 antibody reverses virally induced (rat insulinpromoter-lymphocytic choriomeningitis virus) autoimmunediabetes without impeding viral clearance, J. Immunol. 168(2002) 933–941.
[16] N. Sherry, W. Hagopian, J. Ludvigsson, S.M. Jain, J. Wahlen,R.J. Ferry Jr., B. Bode, S. Aronoff, C. Holland, D. Carlin, K.L.King, R.L. Wilder, S. Pillemer, E. Bonvini, S. Johnson, K.E.Stein, S. Koenig, K.C. Herold, A.G. Daifotis, Teplizumab fortreatment of type 1 diabetes (Protege study): 1-year resultsfrom a randomised, placebo-controlled trial, Lancet 378 (2011)487–497.
[17] H.G. Wells, Studies on the Chemistry of Anaphylaxis (III),Experiments with Isolated Proteins, Especially Those of theHen's Egg (1911).
[18] A.W. Burks, S.M. Jones, R.A. Wood, D.M. Fleischer, S.H.Sicherer, R.W. Lindblad, D. Stablein, A.K. Henning, B.P.Vickery, A.H. Liu, A.M. Scurlock, W.G. Shreffler, M. Plaut,H.A. Sampson, Oral immunotherapy for treatment of eggallergy in children, N. Engl. J. Med. 367 (2012) 233–243.
[19] C. Nagler-Anderson, L.A. Bober, M.E. Robinson, G.W. Siskind,G.J. Thorbecke, Suppression of type II collagen-inducedarthritis by intragastric administration of soluble type IIcollagen, Proc. Natl. Acad. Sci. U. S. A. 83 (1986) 7443–7446.
[20] P.J. Higgins, H.L. Weiner, Suppression of experimental autoim-mune encephalomyelitis by oral administration of myelin basicprotein and its fragments, J. Immunol. 140 (1988) 440–445.
[21] Z.J. Zhang, L. Davidson, G. Eisenbarth, H.L. Weiner, Suppres-sion of diabetes in nonobese diabetic mice by oral administra-tion of porcine insulin, Proc. Natl. Acad. Sci. U. S. A. 88 (1991)10252–10256.
[22] L.C. Harrison, M. Dempsey-Collier, D.R. Kramer, K. Takahashi,Aerosol insulin induces regulatory CD8 gamma delta T cells thatprevent murine insulin-dependent diabetes, J. Exp. Med. 184(1996) 2167–2174.
[23] J. Tian, M.A. Atkinson, M. Clare-Salzler, A. Herschenfeld, T.Forsthuber, P.V. Lehmann, D.L. Kaufman, Nasal administrationof glutamate decarboxylase (GAD65) peptides induces Th2responses and prevents murine insulin-dependent diabetes, J.Exp. Med. 183 (1996) 1561–1567.
[24] M.A. Atkinson, N.K. Maclaren, R. Luchetta, Insulitis anddiabetes in NOD mice reduced by prophylactic insulin therapy,Diabetes 39 (1990) 933–937.
[25] G.J. Macfarlane, A. El-Metwally, S. De, V.E. Ernst, G.L. Dowds,R.J. Moots, Evidence for the efficacy of complementary andalternative medicines in the management of rheumatoidarthritis: a systematic review, Rheumatology. (Oxford) 50(2011) 1672–1683.
[26] W.Wei, L.L. Zhang, J.H. Xu, F. Xiao, C.D. Bao, L.Q. Ni, X.F. Li, Y.Q.Wu, L.Y. Sun, R.H. Zhang, B.L. Sun, S.Q. Xu, S. Liu, W. Zhang, J.Shen, H.X. Liu, R.C. Wang, A multicenter, double-blind, random-ized, controlled phase III clinical trial of chicken type II collagen inrheumatoid arthritis, Arthritis Res. Ther. 11 (2009) R180.
[27] H.L. Weiner, G.A. Mackin, M. Matsui, E.J. Orav, S.J. Khoury,D.M. Dawson, D.A. Hafler, Double-blind pilot trial of oraltolerization with myelin antigens in multiple sclerosis, Science259 (1993) 1321–1324.

353Trials in type 1 diabetes: Antigen-specific therapies
[28] S. Quinn, Human trials scientists, investors, and patients in thequest for a cure, 2001.
[29] M. Peakman, H.M. von, Antigen-specific immunotherapy fortype 1 diabetes: maximizing the potential, Diabetes 59 (2010)2087–2093.
[30] K. Fujihashi, T. Dohi, P.D. Rennert, M. Yamamoto, T. Koga, H.Kiyono, J.R. McGhee, Peyer's patches are required for oraltolerance to proteins, Proc. Natl. Acad. Sci. U. S. A. 98 (2001)3310–3315.
[31] N.R. Locke, S. Stankovic, D.P. Funda, L.C. Harrison, TCRgamma delta intraepithelial lymphocytes are required forself-tolerance, J. Immunol. 176 (2006) 6553–6559.
[32] J.D. Davies, L.Y. Leong, A. Mellor, S.P. Cobbold, H. Waldmann,T cell suppression in transplantation tolerance through linkedrecognition, J. Immunol. 156 (1996) 3602–3607.
[33] K.T. Coppieters, N. Amirian, M.G. von Herrath, Incidental CD8T cell reactivity against caspase-cleaved apoptotic self-antigensfrom ubiquitously expressed proteins in islets from prediabetichuman leucocyte antigen-A2 transgenic non-obese diabeticmice, Clin. Exp. Immunol. 165 (2011) 155–162.
[34] E. Bonifacio, M. Atkinson, G. Eisenbarth, D. Serreze, T.W. Kay,E. Lee-Chan, B. Singh, International workshop on lessons fromanimal models for human type 1 diabetes: identification ofinsulin but not glutamic acid decarboxylase or IA-2 as specificautoantigens of humoral autoimmunity in nonobese diabeticmice, Diabetes 50 (2001) 2451–2458.
[35] A.A. Mamchak, Y. Manenkova, W. Leconet, Y. Zheng, J.R. Chan,C.L. Stokes, L.K. Shoda, H.M. von, D. Bresson, Preexistingautoantibodies predict efficacy of oral insulin to cure autoim-mune diabetes in combination with anti-CD3, Diabetes 61 (2012)1490–1499.
[36] S.L. Thrower, L. James, W. Hall, K.M. Green, S. Arif, J.S. Allen,C. Van-Krinks, B. Lozanoska-Ochser, L. Marquesini, S. Brown,F.S. Wong, C.M. Dayan, M. Peakman, Proinsulin peptideimmunotherapy in type 1 diabetes: report of a first-in-manPhase I safety study, Clin. Exp. Immunol. 155 (2009) 156–165.
[37] T. Orban, K. Farkas, H. Jalahej, J. Kis, A. Treszl, B. Falk, H.Reijonen, J. Wolfsdorf, A. Ricker, J.B. Matthews, N. Tchao, P.Sayre, P. Bianchine, Autoantigen-specific regulatory T cellsinduced in patients with type 1 diabetes mellitus by insulinB-chain immunotherapy, J. Autoimmun. 34 (2010) 408–415.
[38] V.A. Huurman, P.E. van der Meide, G. Duinkerken, S. Willemen,I.R. Cohen, D. Elias, B.O. Roep, Immunological efficacy of heatshock protein 60 peptide DiaPep277 therapy in clinical type Idiabetes, Clin. Exp. Immunol. 152 (2008) 488–497.
[39] J.H. Velthuis, W.W. Unger, J.R. Abreu, G. Duinkerken, K.Franken, M. Peakman, A.H. Bakker, S. Reker-Hadrup, B.Keymeulen, J.W. Drijfhout, T.N. Schumacher, B.O. Roep,Simultaneous detection of circulating autoreactive CD8+ T-cellsspecific for different islet cell-associated epitopes using combi-natorial MHC multimers, Diabetes 59 (2010) 1721–1730.
[40] M. Nakayama, N. Abiru, H. Moriyama, N. Babaya, E. Liu, D. Miao,L. Yu, D.R. Wegmann, J.C. Hutton, J.F. Elliott, G.S. Eisenbarth,Prime role for an insulin epitope in the development of type 1diabetes in NOD mice, Nature 435 (2005) 220–223.
[41] P. Narendran, S.I. Mannering, L.C. Harrison, Proinsulin-apathogenic autoantigen in type 1 diabetes, Autoimmun. Rev.2 (2003) 204–210.
[42] V. Oling, J. Marttila, J. Ilonen, W.W. Kwok, G. Nepom, M. Knip,O. Simell, H. Reijonen, GAD65- and proinsulin-specific CD4+T-cells detected by MHC class II tetramers in peripheral bloodof type 1 diabetes patients and at-risk subjects, J. Autoimmun.25 (3) (Nov 2005) 235–243 (Epub 2005 Nov 2).
[43] G.G. Pinkse, O.H. Tysma, C.A. Bergen, M.G. Kester, F.Ossendorp, P.A. van Veelen, B. Keymeulen, D. Pipeleers,J.W. Drijfhout, B.O. Roep, Autoreactive CD8 T cells associatedwith beta cell destruction in type 1 diabetes, Proc. Natl. Acad.Sci. U. S. A. 102 (2005) 18425–18430.
[44] A. Pugliese, M. Zeller, A. Fernandez Jr., L.J. Zalcberg, R.J.Bartlett, C. Ricordi, M. Pietropaolo, G.S. Eisenbarth, S.T.Bennett, D.D. Patel, The insulin gene is transcribed in thehuman thymus and transcription levels correlated with allelicvariation at the INS VNTR-IDDM2 susceptibility locus for type 1diabetes, Nat. Genet. 15 (1997) 293–297.
[45] M.G. von Herrath, T. Dyrberg, M.B. Oldstone, Oral insulintreatment suppresses virus-induced antigen-specific destruc-tion of beta cells and prevents autoimmune diabetes intransgenic mice, J. Clin. Invest. 98 (1996) 1324–1331.
[46] J.S. Petersen, S. Bregenholt, V. Apostolopolous, D. Homann, T.Wolfe, A. Hughes, J.K. De, M. Wang, T. Dyrberg, M.G. vonHerrath, Coupling of oral human or porcine insulin to the Bsubunit of cholera toxin (CTB) overcomes critical antigenicdifferences for prevention of type I diabetes, Clin. Exp.Immunol. 134 (2003) 38–45.
[47] J.S. Skyler, J.P. Krischer, J. Wolfsdorf, C. Cowie, J.P. Palmer,C. Greenbaum, D. Cuthbertson, L.E. Rafkin-Mervis, H.P. Chase,E. Leschek, Effects of oral insulin in relatives of patients withtype 1 diabetes: the diabetes prevention trial — type 1,Diabetes Care 28 (2005) 1068–1076.
[48] P. Pozzilli, D. Pitocco, N. Visalli, M.G. Cavallo, R. Buzzetti, A.Crino, S. Spera, C. Suraci, G. Multari, M. Cervoni, M.L. MancaBitti, M.C. Matteoli, G. Marietti, F. Ferrazzoli, M.R. CassoneFaldetta, C. Giordano, M. Sbriglia, E. Sarugeri, G. Ghirlanda,No effect of oral insulin on residual beta-cell function inrecent-onset type I diabetes (the IMDIAB VII). IMDIAB Group,Diabetologia 43 (2000) 1000–1004.
[49] L. Chaillous, H. Lefevre, C. Thivolet, C. Boitard, N. Lahlou, C.Atlan-Gepner, B. Bouhanick, A. Mogenet, M. Nicolino, J.C. Carel,P. Lecomte, R. Marechaud, P. Bougneres, B. Charbonnel, P. Sai,Oral insulin administration and residual beta-cell function inrecent-onset type 1 diabetes: a multicentre randomised con-trolled trial. Diabete Insuline Orale group, Lancet 356 (2000)545–549.
[50] B. Ergun-Longmire, J. Marker, A. Zeidler, R. Rapaport, P.Raskin, B. Bode, D. Schatz, A. Vargas, D. Rogers, S. Schwartz,J. Malone, J. Krischer, N.K. Maclaren, Oral insulin therapy toprevent progression of immune-mediated (type 1) diabetes,Ann. N. Y. Acad. Sci. 1029 (2004) 260–277.
[51] G. Fousteri, J.R. Chan, Y. Zheng, C. Whiting, A. Dave, D.Bresson, M. Croft, H.M. von, Virtual optimization of nasalinsulin therapy predicts immunization frequency to be crucialfor diabetes protection, Diabetes 59 (2010) 3148–3158.
[52] L.C. Harrison, M.C. Honeyman, C.E. Steele, N.L. Stone, E.Sarugeri, E. Bonifacio, J.J. Couper, P.G. Colman, Pancreaticbeta-cell function and immune responses to insulin afteradministration of intranasal insulin to humans at risk for type1 diabetes, Diabetes Care 27 (2004) 2348–2355.
[53] L.C. Harrison, Vaccination against self to prevent autoimmunedisease: the type 1 diabetes model, Immunol. Cell Biol. 86(2008) 139–145.
[54] K. Nanto-Salonen, A. Kupila, S. Simell, H. Siljander, T.Salonsaari, A. Hekkala, S. Korhonen, R. Erkkola, J.I. Sipila, L.Haavisto, M. Siltala, J. Tuominen, J. Hakalax, H. Hyoty, J.Ilonen, R. Veijola, T. Simell, M. Knip, O. Simell, Nasal insulin toprevent type 1 diabetes in children with HLA genotypes andautoantibodies conferring increased risk of disease: adouble-blind, randomised controlled trial, Lancet 372 (2008)1746–1755.
[55] S. Fourlanos, C. Perry, S.A. Gellert, E. Martinuzzi, R. Mallone,J. Butler, P.G. Colman, L.C. Harrison, Evidence that nasalinsulin induces immune tolerance to insulin in adults withautoimmune diabetes, Diabetes 60 (2011) 1237–1245.
[56] P. Achenbach, J. Barker, E. Bonifacio, Modulating the naturalhistory of type 1 diabetes in children at high genetic risk bymucosal insulin immunization, Curr. Diab. Rep. 8 (2008)87–93.

354 K.T. Coppieters et al.
[57] R.J. Keller, G.S. Eisenbarth, R.A. Jackson, Insulin prophylaxisin individuals at high risk of type I diabetes, Lancet 341 (1993)927–928.
[58] Effects of insulin in relatives of patients with type 1 diabetesmellitus, N. Engl. J. Med. 346 (2002) 1685–1691.
[59] Peter Gottlieb, Peter G. Colman, Nanette Solvason, Kelly Otto,Bart Roep, Leonard C. Harrison, George Eisenbarth, WilliamRobinson, Paul J. Utz, Lawrence Steinman, Hideki Garren,Joanne Quan, One-Year Results from a Phase 1/2 Clinical Trialof BHT-3021, a DNA Plasmid Vaccine for Type 1 Diabetes (T1D),70th Scientific Sessions, June 25–29, 2010, Orlando, Florida2010.
[60] B. Bielekova, B. Goodwin, N. Richert, I. Cortese, T. Kondo, G.Afshar, B. Gran, J. Eaton, J. Antel, J.A. Frank, H.F. McFarland,R. Martin, Encephalitogenic potential of the myelin basicprotein peptide (amino acids 83–99) in multiple sclerosis:results of a phase II clinical trial with an altered peptide ligand,Nat. Med. 6 (2000) 1167–1175.
[61] S. Baekkeskov, H.J. Aanstoot, S. Christgau, A. Reetz, M.Solimena, M. Cascalho, F. Folli, H. Richter-Olesen, C.P. De,Identification of the 64K autoantigen in insulin-dependentdiabetes as the GABA-synthesizing enzyme glutamic aciddecarboxylase, Nature 347 (1990) 151–156.
[62] L.A. Velloso, O. Kampe, A. Hallberg, L. Christmanson, C.Betsholtz, F.A. Karlsson, Demonstration of GAD-65 as the mainimmunogenic isoform of glutamate decarboxylase in type 1diabetes and determination of autoantibodies using a radioligandproduced by eukaryotic expression, J. Clin. Invest. 91 (1993)2084–2090.
[63] H.J. De Aizpurua, Y.M. Wilson, L.C. Harrison, Glutamic aciddecarboxylase autoantibodies in preclinical insulin-dependentdiabetes, Proc. Natl. Acad. Sci. U. S. A. 89 (1992) 9841–9845.
[64] L.C. Harrison, M.C. Honeyman, H.J. DeAizpurua, R.S. Schmidli,P.G. Colman, B.D. Tait, D.S. Cram, Inverse relation betweenhumoral and cellular immunity to glutamic acid decarboxylasein subjects at risk of insulin-dependent diabetes, Lancet 341(1993) 1365–1369.
[65] W.A. Hagopian, C.B. Sanjeevi, I. Kockum, M. Landin-Olsson, A.E.Karlsen, G. Sundkvist, G. Dahlquist, J. Palmer, A. Lernmark,Glutamate decarboxylase-, insulin-, and islet cell-antibodies andHLA typing to detect diabetes in a general population-basedstudy of Swedish children, J. Clin. Invest. 95 (1995) 1505–1511.
[66] M. Solimena, F. Folli, R. Aparisi, G. Pozza, C.P. De, Autoanti-bodies to GABA-ergic neurons and pancreatic beta cells instiff-man syndrome, N. Engl. J. Med. 322 (1990) 1555–1560.
[67] T. Lohmann, M. Hawa, R.D. Leslie, R. Lane, J. Picard, M.Londei, Immune reactivity to glutamic acid decarboxylase 65 instiffman syndrome and type 1 diabetes mellitus, Lancet 356(2000) 31–35.
[68] H.J. De Aizpurua, M.B. French, N. Chosich, L.C. Harrison,Natural history of humoral immunity to glutamic acid decar-boxylase in non-obese diabetic (NOD) mice, J. Autoimmun. 7(1994) 643–653.
[69] R. Tisch, X.D. Yang, S.M. Singer, R.S. Liblau, L. Fugger, H.O.McDevitt, Immune response to glutamic acid decarboxylasecorrelates with insulitis in non-obese diabetic mice, Nature 366(1993) 72–75.
[70] D.L. Kaufman, M. Clare-Salzler, J. Tian, T. Forsthuber, G.S.Ting, P. Robinson, M.A. Atkinson, E.E. Sercarz, A.J. Tobin, P.V.Lehmann, Spontaneous loss of T-cell tolerance to glutamic aciddecarboxylase in murine insulin-dependent diabetes, Nature366 (1993) 69–72.
[71] E. Jaeckel, L. Klein, N. Martin-Orozco, B.H. von, Normalincidence of diabetes in NOD mice tolerant to glutamic aciddecarboxylase, J. Exp. Med. 197 (2003) 1635–1644.
[72] J.S. Petersen, A.E. Karlsen, H. Markholst, A. Worsaae, T.Dyrberg, B. Michelsen, Neonatal tolerization with glutamicacid decarboxylase but not with bovine serum albumin delays
the onset of diabetes in NOD mice, Diabetes 43 (1994)1478–1484.
[73] R. Tisch, B. Wang, D.J. Weaver, B. Liu, T. Bui, J. Arthos, D.V.Serreze, Antigen-specific mediated suppression of beta cellautoimmunity by plasmid DNA vaccination, J. Immunol. 166(2001) 2122–2132.
[74] J. Ludvigsson, Therapy with GAD in diabetes, Diabetes MetabRes. Rev. 25 (2009) 307–315.
[75] C.D. Agardh, C.M. Cilio, A. Lethagen, K. Lynch, R.D. Leslie, M.Palmer, R.A. Harris, J.A. Robertson, A. Lernmark, Clinicalevidence for the safety of GAD65 immunomodulation inadult-onset autoimmune diabetes, J. Diabetes Complications19 (2005) 238–246.
[76] C.D. Agardh, K. Lynch, M. Palmer, K. Link, A. Lernmark,GAD65 vaccination significantly reduces insulin dependenceat five years follow-up in a dose escalating study inadult-onset autoimmune diabetes patients, Diabetologia 51(2008) S230.
[77] J. Ludvigsson, M. Faresjo, M. Hjorth, S. Axelsson, M. Cheramy,M. Pihl, O. Vaarala, G. Forsander, S. Ivarsson, C. Johansson, A.Lindh, N.O. Nilsson, J. Aman, E. Ortqvist, P. Zerhouni, R.Casas, GAD treatment and insulin secretion in recent-onsettype 1 diabetes, N. Engl. J. Med. 359 (2008) 1909–1920.
[78] J. Ludvigsson, M. Hjorth, M. Cheramy, S. Axelsson, M. Pihl, G.Forsander, N.O. Nilsson, B.O. Samuelsson, T. Wood, J. Aman,E. Ortqvist, R. Casas, Extended evaluation of the safety andefficacy of GAD treatment of children and adolescents withrecent-onset type 1 diabetes: a randomised controlled trial,Diabetologia 54 (2011) 634–640.
[79] M. Hjorth, S. Axelsson, A. Ryden, M. Faresjo, J. Ludvigsson,R. Casas, GAD-alum treatment induces GAD65-specificCD4+CD25highFOXP3+ cells in type 1 diabetic patients, Clin.Immunol. 138 (2011) 117–126.
[80] S. Axelsson, M. Hjorth, J. Ludvigsson, R. Casas, DecreasedGAD(65)-specific Th1/Tc1 phenotype in children with Type 1diabetes treated with GAD-alum, Diabet. Med. 29 (2012)1272–1278.
[81] S. Axelsson, M. Cheramy, M. Hjorth, M. Pihl, L. Akerman, E.Martinuzzi, R. Mallone, J. Ludvigsson, R. Casas, Long-lastingimmune responses 4 years after GAD-alum treatment inchildren with type 1 diabetes, PLoS One 6 (2011) e29008.
[82] D.K. Wherrett, B. Bundy, D.J. Becker, L.A. DiMeglio, S.E.Gitelman, R. Goland, P.A. Gottlieb, C.J. Greenbaum, K.C.Herold, J.B. Marks, R. Monzavi, A. Moran, T. Orban, J.P.Palmer, P. Raskin, H. Rodriguez, D. Schatz, D.M. Wilson, J.P.Krischer, J.S. Skyler, Antigen-based therapy with glutamic aciddecarboxylase (GAD) vaccine in patients with recent-onsettype 1 diabetes: a randomised double-blind trial, Lancet 378(2011) 319–327.
[83] J. Ludvigsson, D. Krisky, R. Casas, T. Battelino, L. Castano, J.Greening, O. Kordonouri, T. Otonkoski, P. Pozzilli, J.J. Robert,H.J. Veeze, J. Palmer, U. Samuelsson, L.H. Elding, J. Aman, G.Kardell, H.J. Neiderud, G. Lundstrom, E. Albinsson, A.Carlsson, M. Nordvall, H. Fors, C.G. Arvidsson, S. Edvardson,R. Hanas, K. Larsson, B. Rathsman, H. Forsgren, H. Desaix, G.Forsander, N.O. Nilsson, C.G. Akesson, P. Keskinen, R. Veijola,T. Talvitie, K. Raile, T. Kapellen, W. Burger, A. Neu, I.Engelsberger, B. Heidtmann, S. Bechtold, D. Leslie, F.Chiarelli, A. Cicognani, G. Chiumello, F. Cerutti, G.V.Zuccotti, G.A. Gomez, I. Rica, R. Barrio, M. Clemente, M.J.Lopez Garcia, M. Rodriguez, I. Gonzalez, J.P. Lopez, M.Oyarzabal, H.M. Reeser, R. Nuboer, P. Stouthart, N. Bratina,N. Bratanic, K.M. de, J. Weill, N. Ser, P. Barat, A.M. Bertrand,J.C. Carel, R. Reynaud, R. Coutant, S. Baron, GAD65 antigentherapy in recently diagnosed type 1 diabetes mellitus, N.Engl. J. Med. 366 (2012) 433–442.
[84] D. Elias, D. Markovits, T. Reshef, R. van der Zee, I.R.Cohen, Induction and therapy of autoimmune diabetes in

355Trials in type 1 diabetes: Antigen-specific therapies
the non-obese diabetic (NOD/Lt) mouse by a 65-kDa heatshock protein, Proc. Natl. Acad. Sci. U. S. A. 87 (1990)1576–1580.
[85] D. Elias, T. Reshef, O.S. Birk, R. van der Zee, M.D. Walker, I.R.Cohen, Vaccination against autoimmune mouse diabetes with aT-cell epitope of the human 65-kDa heat shock protein, Proc.Natl. Acad. Sci. U. S. A. 88 (1991) 3088–3091.
[86] D. Elias, I.R. Cohen, Peptide therapy for diabetes in NOD mice,Lancet 343 (1994) 704–706.
[87] D. Elias, H. Marcus, T. Reshef, V. Ablamunits, I.R. Cohen,Induction of diabetes in standard mice by immunization withthe p277 peptide of a 60-kDa heat shock protein, Eur. J.Immunol. 25 (1995) 2851–2857.
[88] R. Abulafia-Lapid, D. Elias, I. Raz, Y. Keren-Zur, H. Atlan, I.R.Cohen, T cell proliferative responses of type 1 diabetespatients and healthy individuals to human hsp60 and itspeptides, J. Autoimmun. 12 (1999) 121–129.
[89] I. Raz, D. Elias, A. Avron, M. Tamir, M. Metzger, I.R. Cohen,Beta-cell function in new-onset type 1 diabetes andimmunomodulation with a heat-shock protein peptide(DiaPep277): a randomised, double-blind, phase II trial, Lancet358 (2001) 1749–1753.
[90] A. Zanin-Zhorov, L. Cahalon, G. Tal, R. Margalit, O. Lider, I.R.Cohen, Heat shock protein 60 enhances CD4+ CD25+ regulatoryT cell function via innate TLR2 signaling, J. Clin. Invest. 116(2006) 2022–2032.
[91] V.A. Huurman, K. Decochez, C. Mathieu, I.R. Cohen, B.O.Roep, Therapy with the hsp60 peptide DiaPep277 in C-peptidepositive type 1 diabetes patients, Diabetes Metab. Res. Rev. 23(2007) 269–275.
[92] L. Lazar, R. Ofan, N. Weintrob, A. Avron, M. Tamir, D. Elias, M.Phillip, Z. Josefsberg, Heat-shock protein peptide DiaPep277treatment in children with newly diagnosed type 1 diabetes: arandomised, double-blind phase II study, Diabetes Metab. Res.Rev. 23 (2007) 286–291.
[93] N.C. Schloot, G. Meierhoff, C. Lengyel, G. Vandorfi, J.Takacs, P. Panczel, L. Barkai, L. Madacsy, T. Oroszlan, P.
Kovacs, G. Suto, T. Battelino, N. Hosszufalusi, G. Jermendy,Effect of heat shock protein peptide DiaPep277 on beta-cellfunction in paediatric and adult patients with recent-onsetdiabetes mellitus type 1: two prospective, randomized,double-blind phase II trials, Diabetes Metab. Res. Rev. 23(2007) 276–285.
[94] R. Buzzetti, S. Cernea, A. Petrone, M. Capizzi, M. Spoletini, S.Zampetti, C. Guglielmi, C. Venditti, P. Pozzilli, C-peptideresponse and HLA genotypes in subjects with recent-onset type1 diabetes after immunotherapy with DiaPep277: an explor-atory study, Diabetes 60 (2011) 3067–3072.
[95] D. Bresson, L. Togher, E. Rodrigo, Y. Chen, J.A. Bluestone, K.C.Herold, H.M. von, Anti-CD3 and nasal proinsulin combinationtherapy enhances remission from recent-onset autoimmunediabetes by inducing Tregs, J. Clin. Invest. 116 (2006)1371–1381.
[96] D.R. Getts, A.J. Martin, D.P. McCarthy, R.L. Terry, Z.N.Hunter, W.T. Yap, M.T. Getts, M. Pleiss, X. Luo, N.J. King,L.D. Shea, S.D. Miller, Microparticles bearing encephalitogenicpeptides induce T-cell tolerance and ameliorate experimentalautoimmune encephalomyelitis, Nat. Biotechnol. 30 (12) (Dec2012) 1217–1224, http://dx.doi.org/10.1038/nbt.2434 (Epub2012 Nov 18).
[97] X. Clemente-Casares, S. Tsai, Y. Yang, P. Santamaria,Peptide-MHC-based nanovaccines for the treatment of auto-immunity: a “one size fits all” approach? J. Mol. Med. (Berl) 89(2011) 733–742.
[98] X. Luo, K.L. Pothoven, D. McCarthy, M. DeGutes, A. Martin,D.R. Getts, G. Xia, J. He, X. Zhang, D.B. Kaufman, S.D. Miller,ECDI-fixed allogeneic splenocytes induce donor-specific toler-ance for long-term survival of islet transplants via two distinctmechanisms, Proc. Natl. Acad. Sci. U. S. A. 105 (2008)14527–14532.
[99] E. Vandemeulebroucke, F.K. Gorus, K. Decochez, I. Weets, B.Keymeulen, B.C. De, J. Tits, D.G. Pipeleers, C. Mathieu, Insulintreatment in IA-2A-positive relatives of type 1 diabeticpatients, Diabetes Metab. 35 (2009) 319–327.