Embed Size (px)
Citation preview

Tricuspid Stenosis with Pulmonary AtresiaA Cineangiographic-Pathologic Correlation
By MILTON H. PAUL, M.D., AND MAURICE LEV, M.D.
TRICUSPID stenosis associated with pul-monary atresia or stenosis is a relatively
uncommon complex that has been recognizedpathologically for mnaniy years.' More recentlythe clinical findings have beein docunmentedand summarized.2The course of the circulationi ii tricuspid
stenosis with pulmoinary atresia is essentiallysimnilar to that in tricuspid atresia with theright atrial blood being shunted into the leftcardiac chambers through a patent foramenovale. The henmodynamic role of the ob-structed, blind right velntricular chamber re-mains, however, inadequately defined. Thisreport deals with cineangiocardiographic andphysiologic observations in an infant withthis complex and presents a correlative anal-ysis of this material with the pathologic sub-stratum.
Clinical ExaminationA 15-week-old female infant, cvanotic since
birth, was admitted for study because of inereasingcvanosis and respiratorv distress.
Examnination revealed generalized slight cyano-sis. The liver was enlarged 4 cim. below the rightcostal margin and was pulsating. There was apronminent lower left sternal border systolic cardiacimpulse. No thrills were palpated. The first heartsound was of normal intenisity, and there was aloud earlv systolic click, masaximum at the upperleft sternal border, The second heart sound wassingle-sounding and of slightly increased intensityalong the left sternal border. A harsh short grade-III systolic murmur was maximum at the mid-left sternal border.The electrocardiogram (fig. 1) indicated right
atrial hypertrophv and severe left ventrieular pre-
From the Cardiovascular Laboratory and the De-partment of Pathology of the Children 's MemorialHospital, and the Congenital Heart Disease Researchand Training Center, Hektoen Institute, Chicago, Ill.
Supported in part by a researeh grant (H-3351)from the National Heart TIistitute, U.S. Public HealthService.
ponderance. The x-ray showed the heart to hemoderately enlarged, with an abnormallv promi-nent right atrial segment, decreased pulmnonarvvasculature, and left aortic areh.
Cyanotic spells and episodes of severe respira-tory distress recurred with increasing frequenecin the hospital, and the infant died 5 days aftercatheterization at 16 weeks of age.
Cardiac Catheterization andCineangiocardiograms
Cardiac catheterization was performed underiiild sedation (Demerol-Phenergan-sparine mix-ture) and the catheter was inserted via the rightsaphenous vein. From the right atrium it waspossible to enter a ventricular chamber located inthe right anterior portion of the cardiac silhouette.This chaniber was entered repeatedly, but at notinie could the catheter be manipulated to enteran outflow tract. No interatrial communicationcould be demonstrated by passage of the catheterinto the left atrium. Blood samples for oxygenianalysis and blood pressures were recorded (table1 and fig. 2).
Cineangiocardiograins were made at 48 framesper second with the rapid (.1 see.) injection of3 ml. of 90 per cent Hypaque, twice into the rightventricle and once into the right atrium (fig. 3).The right ventricular chamber remained opacifiedfor an unusually long period, over 480 frames (10see.), from the instant of injection. Regurgitatioifrom right ventricle to right atrium was clearly-demiionistrated throughout this period.
Postmortem Examination of HeartOn gross examination the heart (figs. 4 and 5)
weighed 39.5 Gm. (fixed) and was enlarged. Theapex was formed bv the left ventriele. From thebase 2 arteries emerged. The larger was situatedposteriorly and to the right; the smaller anteriorlvand to the left. The mutual relationships of thevarious chambers were normal. The cardiac meas-urements are given in table 2.The right atrium was markedlv enlarged and
thickened, being larger and thicker than the lefta-trium. The right atriunm received the superiorand inferior venae eavae and the coronary sinusin a normal manner. The limbus was well formed,and the foramen ovale was patent about 0.8 Cm.
8 C irculation, Volume XXII, Augu8t 1960198
by guest on July 23, 2018http://circ.ahajournals.org/
Dow
nloaded from

'I'le triculsp)i (ioifice was ver.y sriaiia (1 tihe ti-cuspid valve consisted of, 3 aittenuate(l (cusps, w ithvetIxN Smal11c |papilla 1 r11useles.
'lit right venitr icle was a minlulteI tutierlitits xvall was marikedi thickened, its thickness beillngequal to that of the left Ventricle. No) ar1terenerged f romi this (iamber.The lef't atriuill WaIS 1o11m111al ill size or s-lighti
larger than noraral and it was (listinctlv smiallertitan the right arinam. Its wa1ll was of normalthickness anti detfiiteil thlininler- th.-an thf.t (If tIerigt atr-ium. Ther initia-l or ifice was irorimaltl orsilitiv increased in size andi tire iritral vtave avsmtrirr'ralLk formed.
The left ventricula(r1. chamllber1 was mr1oraal ill size,but its wxall was thicker thail nonrial. Thiej ten1-tricular se])tum Was intact. Frorim tIis crIbererimerged tlief anor,ta. Tire aortie orifice was niormrailCirudlatiou, 'Volwume XXII, August 1960
199
Figure 1Elfecj 'e'Stroc( irdl(yoWzlmt. fJt'lolrvn Ituir.ft11,tet lot f> tt''0 f1'}?'/()hf 'fl{'.
or sfilitjriv illrareised it) size arid tie Valve xn,xI[ic1rsplTd With a.Ir'iht mrlrterior rrmtdl a left po)steriorcI-Is ). rjhe coronar\v o>stinl Wx1'err i -rrmral aInd tire(10oror11111Vx arteries wvere 11nor111ma11 iii dtirtributirl. Tired tilrts arterio()Slswas>ts llaitelit ari(d led ilto) tirepllnlrmoniary triniiik, w hricm wa rlistirmetlv sNrmallertim.iri time aorta. The ivall off tie piflimirmroim y trunikwas thirinrier' th,-ani norril. Thire iuhni)iit1oiVi tlririikeride tlhiirrdly at the hase of tie hreait, 1)ut, it gavx(Of tire 2 lLimilmmoitr^ ar^teries iIIil.1a0riorriml IIrarlirrer.Thbr'achimeplicldtalic ar1teries a'ro)se molrirnlriv
1i1 tire 1iglrt atriliurt there vas at- 11aeceeituatiormolf tire rorrloal enddoctmidiad tiickerinir ox-el tIrelirI1bius, tIre elittrx (f tIre ilnferiO verlrl-l (ca11vm, tirei)llsteio(lr crest, arid the (mdldocatdinra11 pr()oxilmll totire trienlspid ;miiiiiilus. l1m tire mi:lit ventricle tieeimtldmcrhrlmlill 'a1S diffuselx thrickermed arid wx hitenied,arid ai gro>ss diagnosis of fibrowbeiasto(.sis c-ould be
TRRA Si'll) WITH I't'l,Al()NA.'RY
by guest on July 23, 2018http://circ.ahajournals.org/
Dow
nloaded from

200 ~~~~~~~~~~~PAUL,LEV
RIGHTATRIUM
9 .., 9 - 9 -9''!J-t.;;;~j- .717-21 14¾i
ft
i.i K-
IK41CIi
rffII IIZt :i i:tci 222i.
fI-II.F -t-
4--
.--lo.4."I.I
I1
mm Hg100
'ii
5U
RIGHT
VENTRICLE.minmms S~~~~~~~~~~~~~4""-~.~,~,- ,,. Ii-I-
.I
Figure 2Prt .1/i/ic Iracitoia !'on,rgm at ri/f inid r-ig/it iveatricie.
Table 1Ct(a/turI.-(tiI/ji liti/ti
Oxygren Oxyg(en content,satuiration, % ~ ~Vol. %c
(5.5
4.1
7,/u
S.'1
21.8
1.8
ii9
5.2)
Pressure,mnm. Hg
:I tita v 1.4 ii/foa 7 ;)10l
90/1590/65
ititi,-ide. No ttl)ffolr ftl clf li 2i- s c'fill/ dletectedi ill
life tricuspid Hots ver dfilfuscly thic(~kened,
tihf tlii kettui il/v/fvix 1io thff edge.,l S ubstance, anid
ibtse. r'lf/,ev 1v/r ('fit teetd ibv ffti t/)orinaliv s hiort
/lfffild"te tof sliitit pm Ip ilt ry itit-itd s. rIT h .re Av s
f/a lk /d tiiickettiu f/ tift luff of (if/suite of the
ttitral vifiv/ tlat Wtfis tdtiftfft nodullitf inl nttItitre,
iti olvi n-tg ttfplte a tetior 1/taflet tttnd to a.
less extentt tiff il/leVi/ iefttet. Inl 1/lace of pul-
uf/utie val1vultir sttrcttu/f thfere w/l severtti fnsed
folds oif elidne,:fulu:fi ti-'-ue. -All the aortie enspts,//jpecit/iiy tli/f 1ig ft tftftelif01, ANT'iv tIhicker' titan-
Discussion
An opportunitly was presented during cair-
diac catheterization to stildv the Ifemodynanne, fun-ction of the obstruTcted righIt voni
tricuiar cthamber iM a hleart with tr-icuspid
stetios>,7 pulmonary atresia, anfd ani intact
ventricular septumn.
'l'lic pa,"tiflo tify oir t1 i /reseiit cats(
fails iiito the tisinl i)atteirli of this com11plex.The tricuispid or-ifiec ini mtost cases is sm,iiall
clue to a s malIl a nnuiilar opeiiung rathier thian
tto a stetiosis- of the valve strutture itscif. rriie
vatlve tisuafllv consists of thic,keiied leaflet tis-
su,e Cotni1e eted li)v shio rt ehor01dae to s mail l)api)llariy niu11se'les. Thle wihuinoliii orifice is smtall1 or
c-omipletely absiuit. V/lieu. smiall, the auiiuilar
openling" is redluced iii s..ize wiithi a tylpical ring
type of ipulmtouiary. vaivular steiiosis.
WhIen the or.ifiee is obiitcratcd, aggclutinated
valvulair cusps miay- be reeogiiized or no dis-
tinect valve mi'ay be recognized. As ini all eases
of tricuspid sten d attresia,
atrial septal defTect (patenit foram-en ovale),
hyvpertrophyw of the righit atrium and left ven-
tricle, aCnd a dindii-untive, right venitricular
ehamnber. There is, in mnost eases, a markedly
Circ'ulationn, Volume XXII, August 1960
rm Hg9
201
10.
0
7-4
Catheter- site
-Sutperjotr velia c':vxlflght trittitaf
11/guflt vvcutrtiec (,1l'ettfor'.1;.lI it
'HM471-i Iii,
f :'f il ii I' F -., ili-` f-i-.'7,
200
"44:=11T,..
-t.
-,I
. " i"
44.414
44
rH
lit
-t-"i.J.
III 4.1.:I-, .. ... 1.1.1,
I!,11 ..;
by guest on July 23, 2018http://circ.ahajournals.org/
Dow
nloaded from

201TRICUSPID STENOSIS WITII PULMONARY ATRESIA
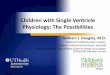
Figure 3Cineangiocardiograms (lateral) following injection of 3 il . of Hypaque (90 per cent)into right ventricle: A. Onset of injection into right venitricle (1). B and C. Completeopacification off riight ventricle (1) and?6 r-eguJtr'gita tiont in1to right atri-ani and atrial op-pencdage (2). U anid E. Opacificationl of left atr-iumin an2d left ventricle (3). PA. Opacifica-tion of aorta (4) fillinig front left ventricle, and pulm)onary artery (5) filling via patentductus arteriosus. Note that the right rentricle (1) remnains heavily opacified in F,approximattely 8 seconds after completion of dye injection.
tlhieneiied riglht ventiicular wall witlh diffusefibroelastosis of the en-cdocardiurn. Increasedfocal mydocardial hypertrophy is noted in the
Circulation, Volume XXII, Auguet 1960
ight atriumi ill most cases anid there arehiemitodyliam-iie chiang(res in the m:litral and aor-tic valves. The ventricular septum is usually
by guest on July 23, 2018http://circ.ahajournals.org/
Dow
nloaded from

PAUL, LEV
Figure 4 Figure 5It'lf'II t I/it1b)/ito Ii tt/ 11 1: of tIlt l ci/I litt/th I.
r
j.. t. ftisso /If; Itc-1111/ I~, It ft It Il / lit It 111, Ithe 1/111/ r1. lit tlet: 1- l(1 / slItf179/lI (t ittlitIt
ond~~~~~~ ~~~~~~~~~~~~~L[fEi f {ltochietn ca l r ; C, c tvi-o-wz fr} s 8 lol s; TV11-f 1cusfp>J#I /
fl/l] f't v'e}n}ttlrl'. l'bOte2, ondf It, por82ictaJl walre1 oJW f/he l'ighllt ,'1ti
intact. A platelit dlullltu1s arteriosiis of 1ode(r-ate ol small tal iber i usually iresenit canti itl'elP lt sec llts liet 1ri11118I llmitelotl' blood tlo IlIt
Il ellSe aliloiie fi iidiiigs take Onim
l .11 ".t hlel e ll li ,fr i,,t itcll\ h1 aXs lxth ei li
za titi .ll 111(1M iiil 'ahigiol .11'tli ogl'alidie fi dllin gs.
Tl'e i 1je( tioll (of iiil. of tontiast materialiiit t oe 8si111 11ted ve tit l l e ha nihe of
.pp1roxi7liiatelI 2 tot :3 iiil. vohititie. p1robahllyrepla('etl a larg"e( )Ptj)i'tntiin of thle ventrieu-Jarl bXelood lld.|e t1ellsl prov)\ided> *1 c#tetillUOus.bult (1i11lillis11ill0, Opac>Xeific.ation of tlse '}chambterI1lt'r a ot1(11 1()0 selmlilts (11' 25) eardiia< co itrae-
tiol1s. Tli (.i le lloJigiltardi rademllrateiionistratetl
t111t the al1lto lili l'-all steii0tite t1'illspi(I o 1i-file 11811W a s a ieg iur'gitailt orihfie. 1rThese o
serrvat io)i I s aare ecessarI'i I 1 11.a(11we-ithI thie
1't1.t'( l vat'ahitt'r traversillt thlec trie'uisi id valve
a1d11( the i'tole (of the (cathetet' ill iiidii'iliig 01
aignietithig thite regiritatiti is nlldefilled. Itsteal's quite liktelv. 111v ever, that there is 11su-
allv a b1)ilidireti(llall Iliovemllelit of btlood aeross
the triiespitl (iee ilt this con(litionl. It eala
be J)t0 11siilaicll that the bitdiieeltioIwal mniittve nicilt
(1 i)1()t)l a1sso)ciatedl w ithi the trieusipid reogur-
gitatiol rlreVellts the dIi imiinutive ventiwi thl (A)strucltedl oultflowX fi mll b)eeom)imn obl1it-elralet stasis .timd tIiroml b)osis. 1Il1iis latterfindinlg' IitsX 1eTell desellleed ill triculls)i(l Stel)-
sas 'ith pulmionary atresia.'4
rth1'1ti-1h at lriil jp'esstlr trlenillgs shlow very
lplro01i111'lit .itrial systolle "A w .\(es tfliat a1re( '1 M lv (eflectet ill he p 'esYstolit plilase ofIllet v-et ri'lt'ih.r t1l iiisil jllSthlf11l1a prIW5Ssure'X
the10 atial presstlit''s 1'et'01'tetl ill ('aly v(' I-
triit'ili. diastotle .rt Ilot tilli g'l'(r Iterl' thall't|(ltle larly di.id i tsi l ie J)ress1llres In. till'
1 ii-lg t Vetlltl e .(lld 1(11d)olo Ieflett llenliodv-ailitie.ll' sigiliietmieit Ivic-lisp)id stenosis. It
see' ns li el ho,w veVt'I', tli.t the usual trails-
val lvollpiI' CSr'58 I'T' g1ratient ti'aenimrs seen ill
isolcated tfrit'uspitl valvular stenlloFs. ainght i11t
he o1)tailletl ill tilns eoiM1lex because of till'
extreit'iely sii]si )lvollnes oIf lootl flo-wingo
tiross the sienoltie aitl regri'gitaiit tr'ieflps)itlotrifiel2. lr1'essi1're (t'iiiuvts rleor'ded fronit tille'ighlt -VIlltl'il'lt' i'it'th fron1 7 5/12 t-o 90/15
111111. Ig (1ll'illig ti' t cathete'rizaftiol, till'
tr'iallo{}1ifar e'jectt ionl ciirve'( is i)t tludikse thllto)bs1e tved ill tfl' Obstitletedi ('1ctal)t'Ib of Severe
i}mhiboniarIy valvular stenosis.
In tins eomiplex tIle triiuspind valve is pat
tllt 1lld( blootl elitel' s thle riglit veiitie]le. I11'8uset' tft tilte ot)hstiltr ilto at tIle outltet anti tIlt
sft'Ilosis at flit illht, lot veXtX ', 'olsi'derla.l )lt
jo'ight v I1Iit liSe ItlliiT l)h1't lt sit) i i l)1'l.St1 II t
l ihlt entl i]ll'r wall is eoltespondiuglythliekened. TIl'e eItvated righit te'ntricnlar
pr'es.s;re' 11m.1> lead1 to the dtvetop)lnllt of tri-en-spid 1't'gnrgitatimill. Tf]e right vt'ntrieular-volulne is siliall, probablv bmt'tause of thle siiall.
Circulation, Volume XXII, August 1960
202
1.1 Jill/Ill1)111/h/Irf OrJ'clit,! 1 lit/IJ ll
It 11111t
I ot'
by guest on July 23, 2018http://circ.ahajournals.org/
Dow
nloaded from

203TRICUSPID STENOSIS WITH PULMONARY ATRESIA
Table 2Heart Me(surements (Fixed Heart)
Wall thickness
Right ventricle
Pulmoniic area
Tricuspid area
Apical area
Left ventricle
Maximum
Apex
Circumference of orifices
Tricuspid
Mitral
Aortic
Internal wall nmeasuremiientsRight ventricle
Inlet length
Inlet perimeter
Outlet length
Outlet perimeter
Left venltrieleInlet length
Outlet length
Perinieter
SummaryAn opportunity was presented during car-
diac catheterization to study the hemodynamicfunction of the obstructed right ventricularchamber in a heart with tricuspid stenosis,pulmonary atresia, and an intact ventricularseptum.
Cineangiocardiograms demonstrated thatthe anatomically steuotic tricuspid orifice was
also a regurgitant orifice and it is postulatedthat the bidirectional flow of blood associatedwith the tricuspid regurgitation prevents theobstructed ventricle from becoming obliter-ated by stasis-thrombosis.
3.6
3.0
3.2
1.6
3.2
0.6
2.4
3.3
4.1
volume of blood entering and leaving thischamber. The fibroelastosis in the right ven-tricle may be the result of stasis, increasedendomyocardial tension, or some other unde-fined factor.5The right atrium is large and thick-walled
due to the large volume and high pressurepresent in this chamber as a result of the tri-cuspid stenosis and the relative functionalstenosis of the patent foramen ovale.
Summario in InterlinguaSe presentava le opportuiiitate, durante catheteri-
sation cardiac, de studiar le function hemodynamicdel obstruite camera dextero-ventricular in un cordecon stenose tricuspidic, atresia pulmonar, e un in-tacte septo ventricular.
Cineangiocardiogrammas demonstrava que le ana-
tomicamente stenotic orificio tricuspidic esseva etiamun orificio regurgitante, e ii es postulate que le fluxobidirectional de sanguine associate con le regurgita-tion tricuspidic preveni que le obstruite ventriculoes oblitterate per stase e thrombose.
References1. LEv, M.: Autopsy Diagnosis of Congenitally Mal-
formed Hearts. Springfield, Ill., Charles CThomas, 1933.
2. KEITH, J. D., ROWE, R. D., AND VLAD, P.: HeartDisease in Infancy and Childhood. New York,The MAacMillan Co., 1958.
3. LEV, M\., AND ROWLATT, V.: A Semiquantitativegross and Ihistopathologic method of studyingthe congenitally malformed heart for clinicaland physiologic correlation. To be published.
4. GLABOFF, J. J., GOHMANN, J. T., AND LITTLE,J. A.: Atresia of the pulmonary artery withintact interventricular septum. J. Pediatrics37: 396, 1950.
5. BLACK-SCIIAFFER, B.: Infantile endocardial fibro-elastosis: A suggested etiology. Arch. Path.63: 281, 1957.
Circulation, Volume XXII, August 1960
by guest on July 23, 2018http://circ.ahajournals.org/
Dow
nloaded from

MILTON H. PAUL and MAURICE LEVCorrelation
Tricuspid Stenosis with Pulmonary Atresia: A Cineangiographic-Pathologic
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1960 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.22.2.198
1960;22:198-203Circulation.
http://circ.ahajournals.org/content/22/2/198located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. and Rights Question and Answer
Permissionsthe Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle column ofClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on July 23, 2018http://circ.ahajournals.org/
Dow
nloaded from


![[JCC] 日本心臓病学会 Japanese College of Cardiology...Tricuspid atresia Mitral atresia Aortic atresia Cardiomyopathy Complete AV block 2: 1 AV block Atrial flutter DIFFICULT](https://img.pdfslide.net/doc/110x75/60813d015e28bb5176058121/jcc-oefec-japanese-college-of-cardiology-tricuspid-atresia.jpg)