Embed Size (px)
Citation preview
Trigeminal AutonomicCephalalgias
Peter J. Goadsby, MD, PhD
ABSTRACTPurpose of Review: This article covers the clinical manifestations and differentialdiagnosis of the trigeminal autonomic cephalalgias (TACs).Recent Findings: TACs comprise a subgroup of primary headache disorders pres-enting with lateralized, often severe, pain accompanied by cranial autonomic fea-tures. The key syndromes are cluster headache, paroxysmal hemicrania, short-lastingunilateral neuralgiform headache attacks with conjunctival injection and tearing(SUNCT)/short-lasting unilateral neuralgiform headache attacks with cranial auto-nomic features (SUNA), and hemicrania continua. Lateralization of symptoms andsigns is the key feature differentiating the TACs and migraine. When diagnosing aTAC, it is appropriate to consider underlying pituitary or pituitary region pathology.Cluster headache responds to oxygen and parenteral triptans, with verapamil havingthe most success for prevention. Paroxysmal hemicrania responds to indomethacin.SUNCT/SUNA responds to lamotrigine and topiramate. Hemicrania continua re-sponds to indomethacin.Summary: TACs are a unique group of primary headache syndromes with indi-vidual features and specific responses to treatment that make their identification crucialfor optimum management.
Continuum Lifelong Learning Neurol 2012;18(4):883–895.
INTRODUCTIONCharacteristic symptoms of the trigem-inal autonomic cephalalgias (TACs) areunilateral head pain associated withprominent ipsilateral cranial autonomicfeatures, such as lacrimation, conjunc-tival injection, or nasal symptoms.1 TheTACs, primary headache disorders, in-clude cluster headache, paroxysmal hemi-crania (PH), and short-lasting unilateralneuralgiform headache attacks with con-junctival injection and tearing (SUNCT)/short-lasting unilateral neuralgiformhead-ache attacks with cranial autonomic fea-tures (SUNA). Section 3 of the InternationalClassification of Headache Disorders, Sec-ond Edition (ICHD-II) lists these syn-dromes.2 Hemicrania continua (HC) is notincluded among the TACs in the ICHD-II;
however, it shares clinical and patho-physiologic features with the TACs andtherefore might be considered a TAC.3
The TACs are distinguished fromeach other by their attack length, dura-tion, and frequency of occurrence. Theyalso respond to different treatments.Cluster headache is characterized by at-tacks of longer duration with relativelylow attack frequency. PH is interme-diate in duration and frequency of at-tacks. The shortest attack length andgreatest attack frequency is seen withSUNCT. In HC, the pain is continuouswith frequent exacerbations that may in-clude cranial autonomic symptoms.
TACs need to be distinguished fromother types of short-lasting headache(Table 10-1). It is important to diagnose
Address correspondence toDr Peter J. Goadsby,Headache GroupYDepartmentof Neurology, UCSF HeadacheCenter, 1701 Divisadero Street,San Francisco, CA 94115,[email protected].
Relationship Disclosure:
Dr Goadsby participates inactivities with Air Productsand Chemicals, Inc.; Allergan,Inc.; Autonomic Technologies,Inc.; Amgen, Inc.; BoehringerIngelheim; Boston ScientificCorporation; Bristol-MyersSquibb; CoLucid Pharmaceuticals,Inc.; Coherex Medical, Inc.;Eli Lilly and Company; eNeuraTherapeutics; Linde; MAPPharmaceuticals, Inc.;Medtronic, Inc.; Merck & Co.,Inc.; NeurAxon; and Pfizer,Inc.; and receives researchsupport from Amgen, Inc.;Boston Scientific Corporation;eNeura Therapeutics;GlaxoSmithKline; Miles forMigraine; and Merck & Co.,Inc. Dr Goadsby has providedheadache expert testimony.
Unlabeled Use ofProducts/InvestigationalUse Disclosure:
Dr Goadsby reports nodisclosure.
* 2012, American Academyof Neurology.
883Continuum Lifelong Learning Neurol 2012;18(4):883–895 www.aan.com/continuum
Review Article
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

the TACs accurately because each syn-dromehas a selective response to treat-ment (Case 10-1A).
Cranial Autonomic Symptoms,Sinus Headache, and theTrigeminal AutonomicCephalalgiasThe diagnosis of sinus headache, im-plying an erroneous infectious etiol-ogy and necessity for antimicrobials, iscommon in patients referred to neu-rologists, particularly those consultingheadache specialists. Cranial autonomicsymptoms are cardinal features of theTACs and the symptoms for which clus-ter headache is best known. These in-clude conjunctival injection, lacrimation,nasal congestion, and rhinorrhea. Theycan be elicited by inducing pain in thefirst division of the trigeminal nerve involunteers4 and are also common inmigraine.5 In the general populationof patients who believe they have si-nus headaches, more than 86% havemigraine and 56% have nasal conges-tion, which likely leads to this misdi-agnosis.6 The proportion is almost thesame in a headache clinic, where 88%of patients who have self- or physician-diagnosed sinus headache actually havemigraine.7 Not surprisingly, pain-free ratesfor sumatriptan in this sinus headachegroup are the same as for migraine.8
Similar confusion can lead patients withTACs to treatment for sinus pathology. In
Case 10-1AA 47-year-old man presented with a 9-year history of troublesomeheadaches. As a teenager, he had headache with nausea, during which hepreferred to retire to a darkened room. He reported daily headache forthe past 9 years. Some part of every day the headache was worsefor 2 to 3 hours. The pain was bilateral, although greater on the left.During exacerbations the pain throbbed, and photophobia localized to theleft and generalized phonophobia were present. Head movement hadno effect on the pain. He was treating with hydrocodone/acetaminophentablets 2 to 3 times per day. He also took thyroxine 100 2g daily. Familyhistory of headache included his mother, who associated her headacheswith her periods and drinking red wine. On examination he was euthyroid.General and neurologic examinations were normal.
Consider the differential diagnosis at this point. The case will continueon page 893.
TABLE 10-1 TrigeminalAutonomicCephalalgias andOther Short-LastingHeadaches
b Trigeminal AutonomicCephalalgiasa
Cluster headacheParoxysmal hemicraniaShort-lasting unilateralneuralgiform headacheattacks with conjunctivalinjection and tearing(SUNCT)/short-lastingunilateral neuralgiformheadache attacks with cranialautonomic features (SUNA)
Hemicrania continua
b Other Short-Lasting HeadachesPrimary stabbing headacheTrigeminal neuralgiaPrimary cough headachePrimary exertional headachePrimary sex headacheHypnic headache
a Consider pituitary tumorYrelated head-ache in the differential diagnosis of thesetrigeminal autonomic cephalalgias.
884 www.aan.com/continuum August 2012
Trigeminal Autonomic Cephalalgias
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

a clinic study, nearly one-fourth of pa-tients seen with cluster headache hadbeen treated by an ear, nose, and throatsurgeon.9
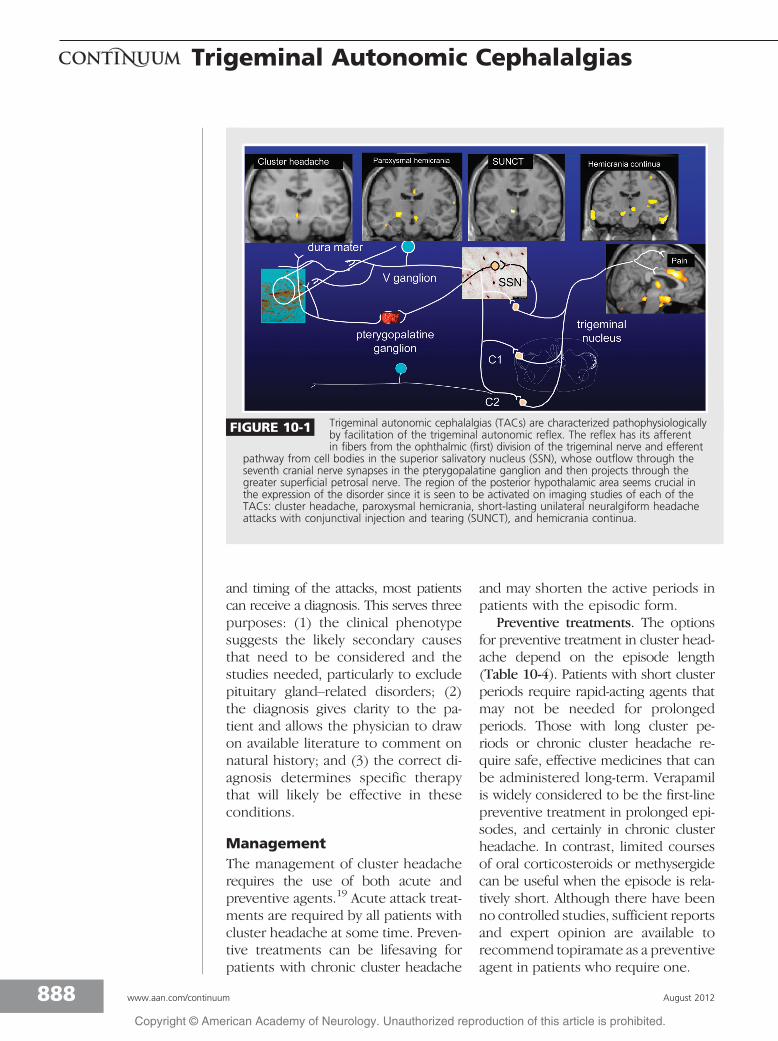
The patients and their physicians arecorrect in assigning part of the problemto sinus changes. However, the reasonfor the symptom is cranial parasympa-thetic activation related to pain ratherthan nasal congestion due to local in-flammation. The trigeminal autonomicreflex, which causes parasympatheticactivation triggered by nociceptive tri-geminal activation, consists of an af-ferent arc in the trigeminal nerve, mostprominently in the first division; a re-flex connection to the (parasympathetic)superior salivatory nucleus in the pons;and an efferent arc in the facial (seventhcranial) nerve. The efferent arc passesthrough the geniculate ganglion, syn-apsing mainly in the pterygopalatine(sphenopalatine) ganglion and proj-ecting through the greater superficialpetrosal nerve.10 This activation is veryprominent in TACs; however, it can beseen with any nociceptive input to thefirst division of the trigeminal nerve.This well-described physiology ex-plains why so many headaches aremisdiagnosed and provides a logicalbasis on which to rediagnose and cor-rectly manage these patients.
LateralizationAn important feature of TAC attacks islateralization of the symptoms and signs.In a group of consecutive patients, fewerthan 5% with unilateral migraine referredtheir photophobia or phonophobia ipsi-lateral to the pain. In the TAC popula-tion, as many as 10 times that numberreport photophobia or phonophobia,or both, ipsilateral to the pain.11 Whencomparing cranial autonomic symptomsbetween migraine and cluster head-ache, patients with cluster headacheare more likely to have lateralized symp-toms that are stereotypically associated
with painful paroxysms. In migraine,cranial autonomic symptoms are moreoften bilateral, less prominent, and var-iable in presentation.12 Recognizing thislateralization pattern is helpful in dis-tinguishing TACs from migraine.
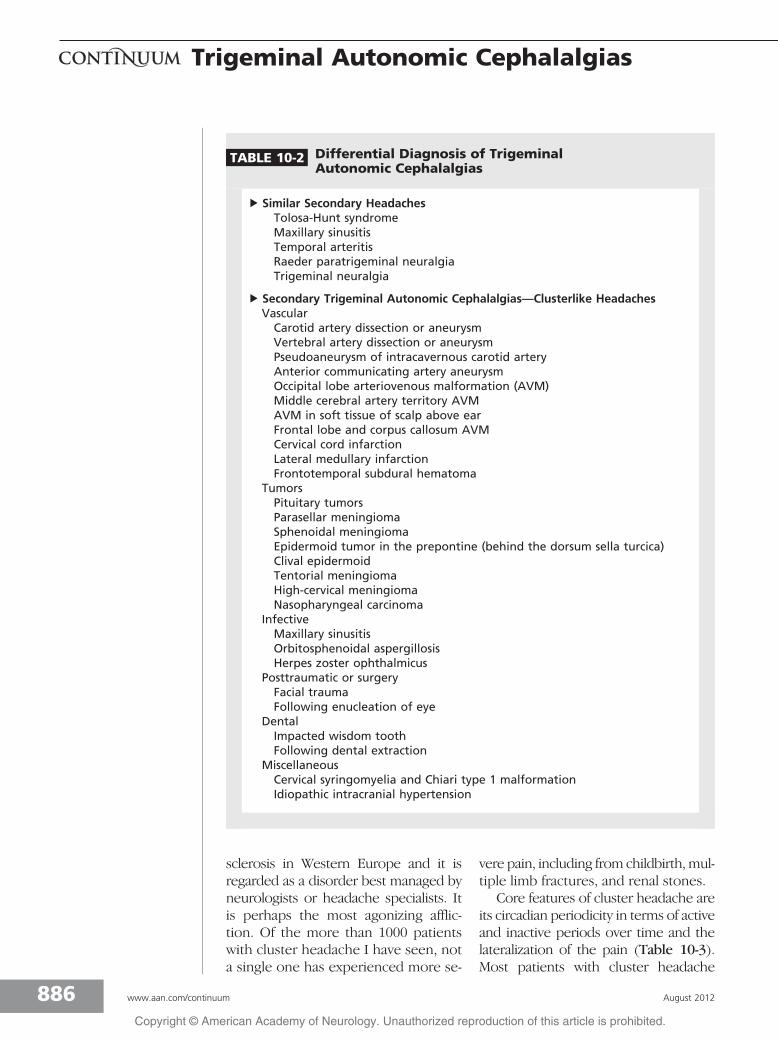
Role of the Pituitary GlandA spectrum of pathology is reportedto present with TAC-like headaches(Table 10-2), although it is likely thatsome of these cases are labeled ascluster headache solely on the pres-ence of cranial autonomic symptoms.Understanding the trigeminal auto-nomic reflex might reduce this ten-dency.10 An important theme that hasemerged recently is the propensity forpituitary and peripituitary gland path-ology to present as a phenotypic TAC.In a cohort of 84 patients with pituitarytumors and headache problems, 10%had a TAC-like headache.13 This isapproximately 100 times the expectednumber in the population, and whilemigraine was the most common head-ache type, the high prevalence of TACswas notable. Activity in the region ofthe hypothalamus on brain imaging inTACs14 supports this link to the pitui-tary, as do the associated neuroendo-crine disturbances well known to occurin cluster headache. MRI brain imagingwith pituitary views15 and pituitary func-tion tests are an appropriate part ofthe evaluation in all patients with TAC.Given that TACs are rare and lifelong,the treatment of a coexisting pituitarypathology may improve the headacheproblem. These studies may have im-portant therapeutic implications.
CLUSTER HEADACHEDiagnosisCluster headache is a rare variety of pri-mary headache, having a population fre-quency of 0.1%.16 As a clinical anchor,it is about as common as multiple
KEY POINTS
h Photophobia orphonophobia isipsilateral to theheadache in trigeminalautonomic cephalalgiasand remains bilateral inmigraine even when thepain is lateralized.
h In trigeminal autonomiccephalalgias, cranialautonomic symptoms,such as lacrimation,conjunctival injection,and nasal congestion,tend to be lateralizedto the side of pain,prominent, andconsistent between oneattack and another.
h In migraine, cranialautonomic symptomsare often bilateral,mild, and do not alwaysparallel the severity ofattacks.
h Pituitary glandpathology mayaccompany trigeminalautonomic cephalalgias.
885Continuum Lifelong Learning Neurol 2012;18(4):883–895 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
sclerosis in Western Europe and it isregarded as a disorder best managed byneurologists or headache specialists. Itis perhaps the most agonizing afflic-tion. Of the more than 1000 patientswith cluster headache I have seen, nota single one has experienced more se-
vere pain, including from childbirth,mul-tiple limb fractures, and renal stones.
Core features of cluster headache areits circadian periodicity in terms of activeand inactive periods over time and thelateralization of the pain (Table 10-3).Most patients with cluster headache
TABLE 10-2 Differential Diagnosis of TrigeminalAutonomic Cephalalgias
b Similar Secondary HeadachesTolosa-Hunt syndromeMaxillary sinusitisTemporal arteritisRaeder paratrigeminal neuralgiaTrigeminal neuralgia
b Secondary Trigeminal Autonomic Cephalalgias—Clusterlike HeadachesVascularCarotid artery dissection or aneurysmVertebral artery dissection or aneurysmPseudoaneurysm of intracavernous carotid arteryAnterior communicating artery aneurysmOccipital lobe arteriovenous malformation (AVM)Middle cerebral artery territory AVMAVM in soft tissue of scalp above earFrontal lobe and corpus callosum AVMCervical cord infarctionLateral medullary infarctionFrontotemporal subdural hematoma
TumorsPituitary tumorsParasellar meningiomaSphenoidal meningiomaEpidermoid tumor in the prepontine (behind the dorsum sella turcica)Clival epidermoidTentorial meningiomaHigh-cervical meningiomaNasopharyngeal carcinoma
InfectiveMaxillary sinusitisOrbitosphenoidal aspergillosisHerpes zoster ophthalmicus
Posttraumatic or surgeryFacial traumaFollowing enucleation of eye
DentalImpacted wisdom toothFollowing dental extraction
MiscellaneousCervical syringomyelia and Chiari type 1 malformationIdiopathic intracranial hypertension
886 www.aan.com/continuum August 2012
Trigeminal Autonomic Cephalalgias
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
are men (a 3:1 predominance). Theyusually experience episodes of one ortwo attacks of relatively short duration(lasting 15 to 180 minutes with unilat-eral pain) which occur daily for 8 to 10weeks yearly. Patients are generallyasymptomatic between attacks. Duringattacks, patients move unceasingly,pacing, rocking, or even rubbing theirhead for relief. This is in contrast topatients with migraines, who prefer toremain still. The pain tends to beretro-orbital or temporal, boring inquality, and intense. Associated featuresinclude ipsilateral symptoms of cranial
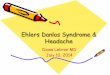
(parasympathetic) autonomic activa-tion: a red or watering eye, a blockedor running nose, or cranial sympatheticdysfunction such as partial ptosis. Clus-ter headache is thought to involveneurons in or around the centralpacemaker regions of the posterior hy-pothalamic graymatter (Figure 10-1).17,18
While patients with cluster headachemay also experience nausea, photopho-bia, and phonophobia, the latter two,particularly photophobia, tend to beipsilateral to the pain only in TACs.11
By defining the cycling pattern,length of attack, frequency of attack,
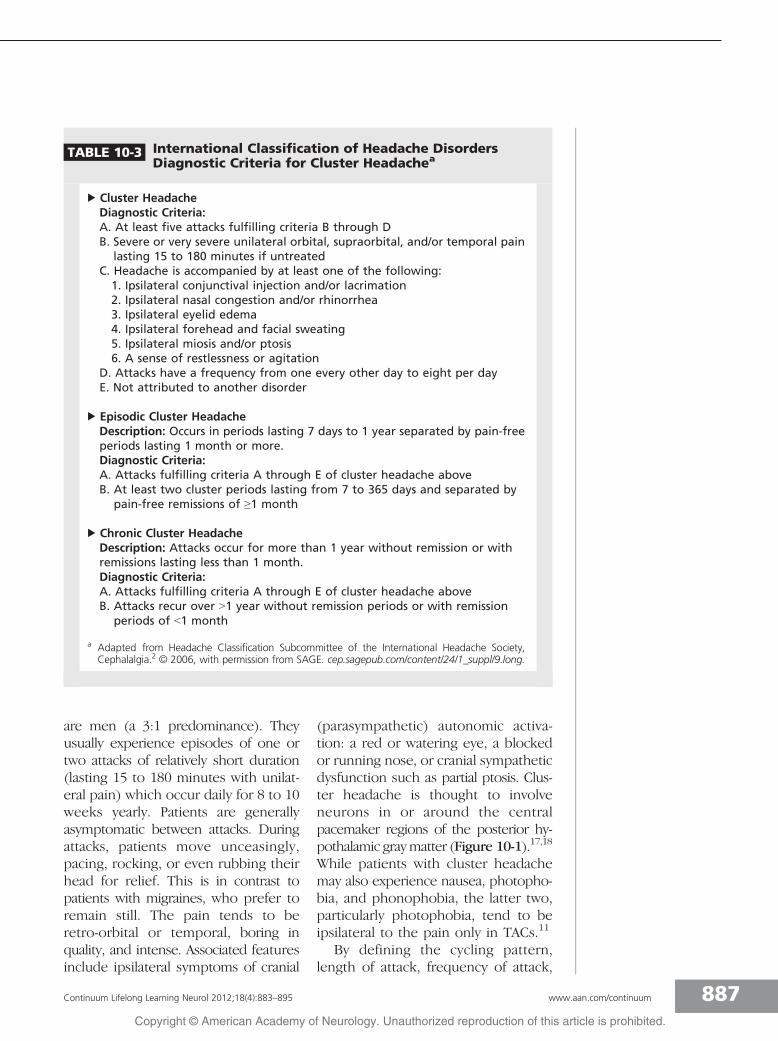
TABLE 10-3 International Classification of Headache DisordersDiagnostic Criteria for Cluster Headachea
b Cluster HeadacheDiagnostic Criteria:A. At least five attacks fulfilling criteria B through DB. Severe or very severe unilateral orbital, supraorbital, and/or temporal pain
lasting 15 to 180 minutes if untreatedC. Headache is accompanied by at least one of the following:1. Ipsilateral conjunctival injection and/or lacrimation2. Ipsilateral nasal congestion and/or rhinorrhea3. Ipsilateral eyelid edema4. Ipsilateral forehead and facial sweating5. Ipsilateral miosis and/or ptosis6. A sense of restlessness or agitation
D. Attacks have a frequency from one every other day to eight per dayE. Not attributed to another disorder
b Episodic Cluster HeadacheDescription: Occurs in periods lasting 7 days to 1 year separated by pain-freeperiods lasting 1 month or more.Diagnostic Criteria:A. Attacks fulfilling criteria A through E of cluster headache aboveB. At least two cluster periods lasting from 7 to 365 days and separated by
pain-free remissions of Q1 month
b Chronic Cluster HeadacheDescription: Attacks occur for more than 1 year without remission or withremissions lasting less than 1 month.Diagnostic Criteria:A. Attacks fulfilling criteria A through E of cluster headache aboveB. Attacks recur over 91 year without remission periods or with remission
periods of G1 month
a Adapted from Headache Classification Subcommittee of the International Headache Society,Cephalalgia.2 B 2006, with permission from SAGE. cep.sagepub.com/content/24/1_suppl/9.long.
887Continuum Lifelong Learning Neurol 2012;18(4):883–895 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
and timing of the attacks, most patientscan receive a diagnosis. This serves threepurposes: (1) the clinical phenotypesuggests the likely secondary causesthat need to be considered and thestudies needed, particularly to excludepituitary glandYrelated disorders; (2)the diagnosis gives clarity to the pa-tient and allows the physician to drawon available literature to comment onnatural history; and (3) the correct di-agnosis determines specific therapythat will likely be effective in theseconditions.
ManagementThe management of cluster headacherequires the use of both acute andpreventive agents.19 Acute attack treat-ments are required by all patients withcluster headache at some time. Preven-tive treatments can be lifesaving forpatients with chronic cluster headache
and may shorten the active periods inpatients with the episodic form.
Preventive treatments. The optionsfor preventive treatment in cluster head-ache depend on the episode length(Table 10-4). Patients with short clusterperiods require rapid-acting agents thatmay not be needed for prolongedperiods. Those with long cluster pe-riods or chronic cluster headache re-quire safe, effective medicines that canbe administered long-term. Verapamilis widely considered to be the first-linepreventive treatment in prolonged epi-sodes, and certainly in chronic clusterheadache. In contrast, limited coursesof oral corticosteroids or methysergidecan be useful when the episode is rela-tively short. Although there have beenno controlled studies, sufficient reportsand expert opinion are available torecommend topiramate as a preventiveagent in patients who require one.
FIGURE 10-1 Trigeminal autonomic cephalalgias (TACs) are characterized pathophysiologicallyby facilitation of the trigeminal autonomic reflex. The reflex has its afferentin fibers from the ophthalmic (first) division of the trigeminal nerve and efferent
pathway from cell bodies in the superior salivatory nucleus (SSN), whose outflow through theseventh cranial nerve synapses in the pterygopalatine ganglion and then projects through thegreater superficial petrosal nerve. The region of the posterior hypothalamic area seems crucial inthe expression of the disorder since it is seen to be activated on imaging studies of each of theTACs: cluster headache, paroxysmal hemicrania, short-lasting unilateral neuralgiform headacheattacks with conjunctival injection and tearing (SUNCT), and hemicrania continua.
888 www.aan.com/continuum August 2012
Trigeminal Autonomic Cephalalgias
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

Verapamil is suggested as a usefuloption and is comparable in efficacy tolithium.20 Clinical practice has demon-strated the need to use high doses,higher than those used in cardiacconditions. Although most patients starton doses as low as 40 mg to 80 mgtwice daily, doses up to 960 mg dailymay be required. Side effects, such asgingival hyperplasia, constipation, andleg swelling, are recognized, as arecardiac dysrhythmias. Verapamil cancause heart block by slowing conduc-tion in the atrioventricular node that ismonitored clinically by the PR intervalon the ECG. Given that the effects onthe atrioventricular node take up to 10days to appear, 2-week intervals arerecommended between dose changeson the first exposure, with ECGsprior to the next escalation and rou-tine 6-month ECGs after the dose isestablished.21
Acute treatments. Cluster headacheattacks quickly reach full intensity andrequire treatment with a rapid onset.Many patients with acute cluster head-ache respond well to treatment withoxygen inhalation.22 This should be ad-ministered as 100% oxygen at 12 L/minto 15 L/min for 15 to 20 minutes. Itis important to have a high flow rateusing an appropriate mask. Injectablesumatriptan 6 mg is effective,23 rapidin onset, shows no evidence of tachy-phylaxis, and is the only US Food andDrug AdministrationYapproved treat-ment for cluster headache. Sumatrip-tan 20 mg24 and zolmitriptan 5 mg25
nasal sprays are effective in acute clus-ter headache in controlled trials andoffer a useful option. Preemptive treat-ment with sumatriptan 100 mg orally3 times daily is ineffective, and no evi-dence suggests that it is effective whenused orally in the acute treatment of clus-ter headache. It can be associated withmedication-overuse headache problems.
When extensive pharmacologic op-tions have been attempted but areunsuccessful, surgery may be consid-ered. Patients must be carefully se-lected. With the increasing exploration ofstimulator approaches, modern therapyhas no place for destructive procedures.Each has important morbidity, andsome have mortality, such as trigeminalsensory rhizotomy via a posterior fossaapproach, which is unacceptable. Poste-rior hypothalamic region neurostim-ulation is initiated based on neu-roimaging findings of diencephalicactivation in attacks of cluster head-ache.17 There is now a reasonableamount of experience with that ap-proach, suggesting about two-thirds ofpatients benefit.26 An alternative ap-proach is occipital nerve stimulation,which is also effective in about two-thirds of patients.27 Most recently,sphenopalatine (pterygopalatine) gan-glion stimulation has been proposed
KEY POINTS
h Verapamil can prolongthe PR interval of theECG. An ECG should beperformed 2 weeksafter increasingverapamil to check thePR interval.
h Oxygen 100% shouldbe given at a rate of12 L/min to 15 L/min.
TABLE 10-4 PreventiveManagement ofCluster Headache
b Short-Term Prevention ofEpisodic Cluster HeadacheGreater occipital nerveinjection
PrednisoloneMethysergidea
VerapamilTopiramate
b Long-Term Prevention ofEpisodic Cluster Headache andProlonged Chronic ClusterHeadacheVerapamilLithiumMelatoninTopiramateGabapentinMethysergidea
a Care is needed toavoid complications, andbreaks in therapy are essential. Methy-sergide is not available in the United Statesbut is still licensed.
889Continuum Lifelong Learning Neurol 2012;18(4):883–895 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
as another way to control medicallyrefractory cluster headache.
PAROXYSMAL HEMICRANIAPH is a rare variety of TAC (Table10-5),28Y30 marked by relatively shortattacks (2 to 30 minutes) of severe lat-eralized pain associated with cranial au-tonomic features and responding toindomethacin.28
Clinical FeaturesAttacks usually recur several times daily,with a mean of 11 in one series.28 Thepain characteristically involves the oph-thalmic division of the trigeminal nerve
and is always unilateral, although it mayshift sides. Attacks have a medianlength of 19 minutes.28 Typically de-scribed as a disorder occurring mainlyin women, this assumption was ques-tioned in a recent cohort study inwhich a clear female preponderancewas not evident.28 Two-thirds ofpatients in a large series had photo-phobia and phonophobia, which areoften lateralized to the side of the pain.In the same series, 80% of patientswere restless or agitated duringattacks.11 In contrast to cluster head-ache, the attacks of PH do not charac-teristically occur at night.
KEY POINT
h Paroxysmal hemicraniais effectively treatedwith indomethacin.
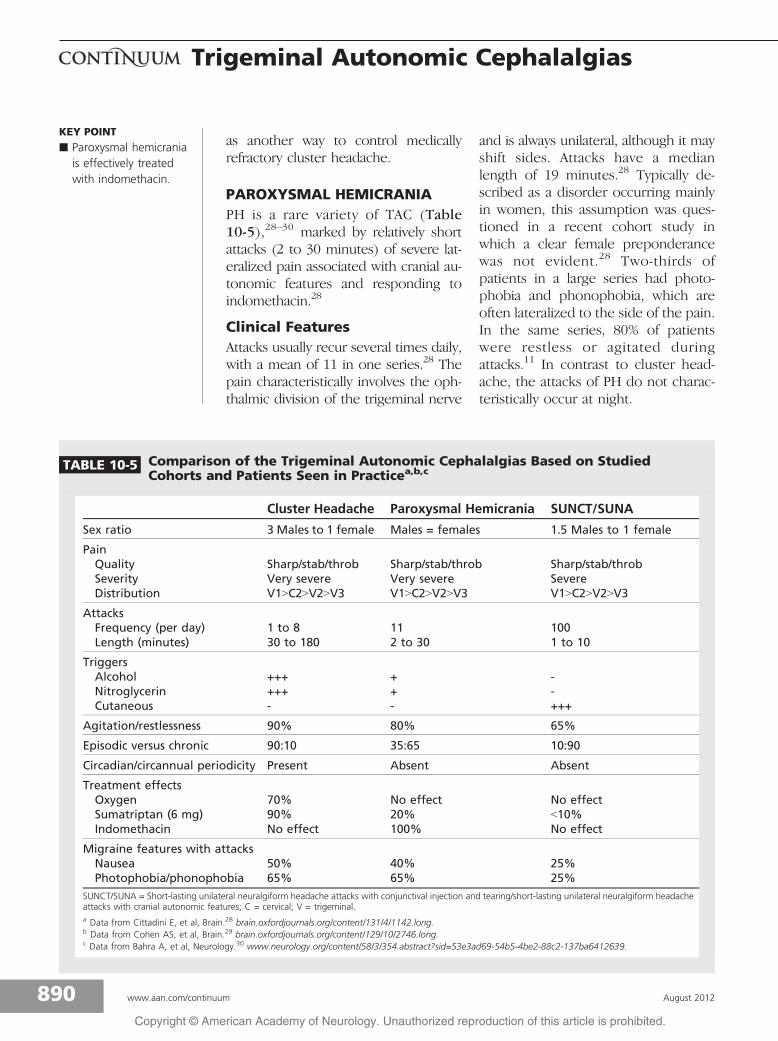
TABLE 10-5 Comparison of the Trigeminal Autonomic Cephalalgias Based on StudiedCohorts and Patients Seen in Practicea,b,c
Cluster Headache Paroxysmal Hemicrania SUNCT/SUNA
Sex ratio 3 Males to 1 female Males = females 1.5 Males to 1 female
PainQuality Sharp/stab/throb Sharp/stab/throb Sharp/stab/throbSeverity Very severe Very severe SevereDistribution V19C29V29V3 V19C29V29V3 V19C29V29V3
AttacksFrequency (per day) 1 to 8 11 100Length (minutes) 30 to 180 2 to 30 1 to 10
TriggersAlcohol +++ + -Nitroglycerin +++ + -Cutaneous - - +++
Agitation/restlessness 90% 80% 65%
Episodic versus chronic 90:10 35:65 10:90
Circadian/circannual periodicity Present Absent Absent
Treatment effectsOxygen 70% No effect No effectSumatriptan (6 mg) 90% 20% G10%Indomethacin No effect 100% No effect
Migraine features with attacksNausea 50% 40% 25%Photophobia/phonophobia 65% 65% 25%
SUNCT/SUNA = Short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing/short-lasting unilateral neuralgiform headacheattacks with cranial autonomic features; C = cervical; V = trigeminal.a Data from Cittadini E, et al, Brain.28 brain.oxfordjournals.org/content/131/4/1142.long.b Data from Cohen AS, et al, Brain.29 brain.oxfordjournals.org/content/129/10/2746.long.c Data from Bahra A, et al, Neurology.30 www.neurology.org/content/58/3/354.abstract?sid=53e3ad69-54b5-4be2-88c2-137ba6412639.
890 www.aan.com/continuum August 2012
Trigeminal Autonomic Cephalalgias
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

TriggersWhile most attacks are spontaneous,approximately 10% of attacks have me-chanical triggers, such as bending orrotating the head. Attacks may also beprecipitated by pressure against thetransverse processes of C4-C5, the C2root, or the greater occipital nerve.Alcohol triggers attacks in one-fifth ofpatients, but cutaneous triggers, such astouching the skin, chewing, or talking,are not seen with PH, unlike in SUNCT/SUNA. Menstruation does not appear toinfluence attacks, and pregnancy doesnot seem to terminate attacks.
SubtypesPH is classified as either episodic orchronic. About 35% of patients haveepisodic paroxysmal hemicrania, diag-nosed when remissions last 1 month orlonger. The remaining patients havechronic paroxysmal hemicrania, diag-nosed when no remission occurs with-in 1 year. Therefore, the chronic formof PH predominates, whereas in clus-ter headache the episodic form pre-dominates. The explanation for this isunknown.
TreatmentWhile the response to indomethacinis characteristic and long-lasting,31 pa-tients who develop gastrointestinal prob-lems present an important clinicalchallenge. Some patients intolerant to in-domethacin respond to cyclooxygenase2 (COX2) selective inhibitors, althoughlong-term safety issues make this optionproblematic. No controlled studies areavailable for PH management in patientsintolerant to indomethacin. Topiramateis reported to be useful.32 While mostattacks are too brief to be aborted bytriptans, subcutaneous sumatriptan isreported to be useful in 20% of patientswith longer attack duration. Greateroccipital nerve injection with lidocaineand methylprednisolone is effective in
some patients with PH.33 Neuromodu-lation devices are used for some pa-tients with PH, and these may play amore prominent role in the future treat-ment of these patients.
SHORT-LASTING UNILATERALNEURALGIFORM HEADACHEATTACKS WITH CONJUNCTIVALINJECTION AND TEARING/CRANIAL AUTONOMICSYMPTOMSSUNCT/SUNA is a relatively rare TACmarked by short-lasting attacks of lat-eralized severe head pain associatedwith prominent cranial autonomic fea-tures and often triggered by cutane-ous stimuli.29
Clinical FeaturesAlthough the International HeadacheSociety identifies the site of pain inSUNCT as unilateral orbital, supraor-bital, or temporal, the pain maybe experienced anywhere in the head.29
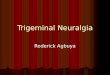
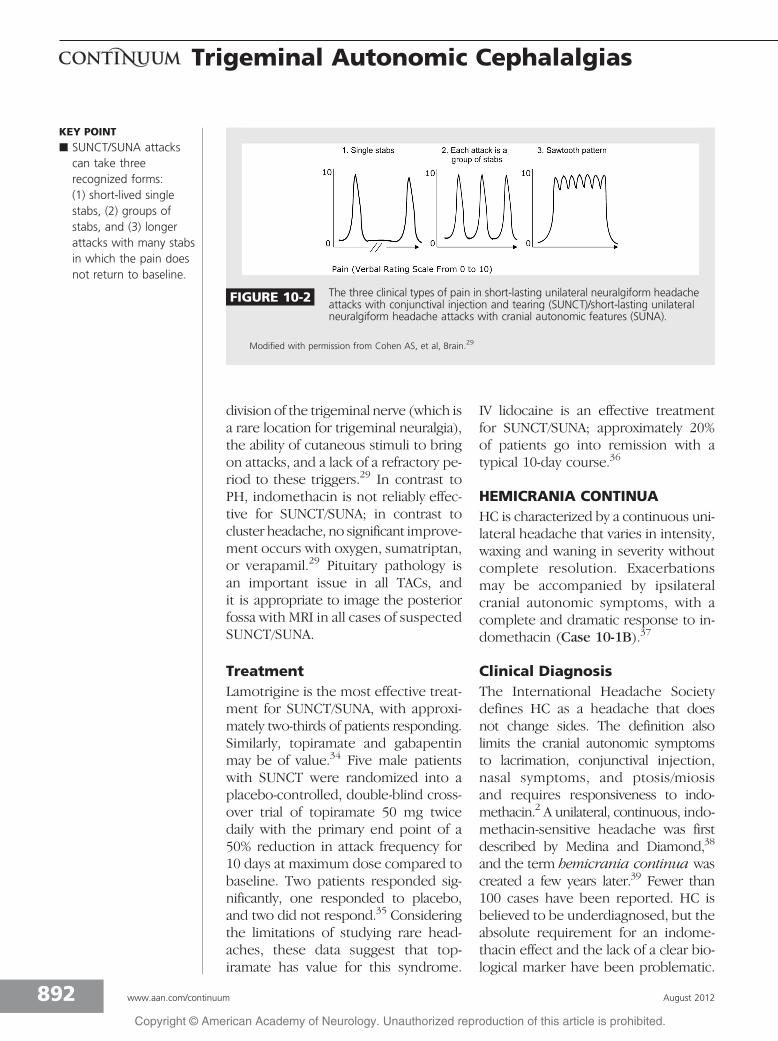
Three temporal profiles have been iden-tified: (1) single stabs, which are usu-ally short-lived, (2) groups of stabs, and(3) longer attacks comprised of manystabs between which the pain does notreturn to baseline, thus giving a saw-tooth pattern with attacks lasting manyminutes (Figure 10-2).29 The termSUNA is applied when both conjunc-tival injection and tearing are absent,although in practice the two condi-tions likely represent a spectrum of thesame disorder.
Differential Diagnosisand TriggersWhen typical, the short-lasting attacksof SUNCT/SUNA are clinically character-istic and the major differential diagnosisis trigeminal neuralgia. Features favor-ing SUNCT/SUNA as opposed to trige-minal neuralgia include the prominentdistribution of pain in the ophthalmic
891Continuum Lifelong Learning Neurol 2012;18(4):883–895 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
division of the trigeminal nerve (which isa rare location for trigeminal neuralgia),the ability of cutaneous stimuli to bringon attacks, and a lack of a refractory pe-riod to these triggers.29 In contrast toPH, indomethacin is not reliably effec-tive for SUNCT/SUNA; in contrast tocluster headache, no significant improve-ment occurs with oxygen, sumatriptan,or verapamil.29 Pituitary pathology isan important issue in all TACs, andit is appropriate to image the posteriorfossa with MRI in all cases of suspectedSUNCT/SUNA.
TreatmentLamotrigine is the most effective treat-ment for SUNCT/SUNA, with approxi-mately two-thirds of patients responding.Similarly, topiramate and gabapentinmay be of value.34 Five male patientswith SUNCT were randomized into aplacebo-controlled, double-blind cross-over trial of topiramate 50 mg twicedaily with the primary end point of a50% reduction in attack frequency for10 days at maximum dose compared tobaseline. Two patients responded sig-nificantly, one responded to placebo,and two did not respond.35 Consideringthe limitations of studying rare head-aches, these data suggest that top-iramate has value for this syndrome.
IV lidocaine is an effective treatmentfor SUNCT/SUNA; approximately 20%of patients go into remission with atypical 10-day course.36
HEMICRANIA CONTINUAHC is characterized by a continuous uni-lateral headache that varies in intensity,waxing and waning in severity withoutcomplete resolution. Exacerbationsmay be accompanied by ipsilateralcranial autonomic symptoms, with acomplete and dramatic response to in-domethacin (Case 10-1B).37
Clinical DiagnosisThe International Headache Societydefines HC as a headache that doesnot change sides. The definition alsolimits the cranial autonomic symptomsto lacrimation, conjunctival injection,nasal symptoms, and ptosis/miosisand requires responsiveness to indo-methacin.2 A unilateral, continuous, indo-methacin-sensitive headache was firstdescribed by Medina and Diamond,38
and the term hemicrania continua wascreated a few years later.39 Fewer than100 cases have been reported. HC isbelieved to be underdiagnosed, but theabsolute requirement for an indome-thacin effect and the lack of a clear bio-logical marker have been problematic.
KEY POINT
h SUNCT/SUNA attackscan take threerecognized forms:(1) short-lived singlestabs, (2) groups ofstabs, and (3) longerattacks with many stabsin which the pain doesnot return to baseline.
FIGURE 10-2 The three clinical types of pain in short-lasting unilateral neuralgiform headacheattacks with conjunctival injection and tearing (SUNCT)/short-lasting unilateralneuralgiform headache attacks with cranial autonomic features (SUNA).
Modified with permission from Cohen AS, et al, Brain.29
892 www.aan.com/continuum August 2012
Trigeminal Autonomic Cephalalgias
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Cases with bilateral pain have beenreported, and patients with unilateralattacks that change sides have beendescribed. Nausea, photophobia, pho-nophobia, and cranial autonomic symp-toms are rare during the backgroundpain but more common with ex-acerbations.40 Four cases have beendescribed with a typical migrainous vi-sual aura occurring in association withthe exacerbation of HC. Generally, thebackground pain of HC is greater thanthe interparoxysmal pain of the otherTACs, and the exacerbations in HC arelonger than the paroxysms of theother TACs. This helps to differentiateHC from PH.
TreatmentAs with PH, the essential managementproblem arises when indomethacin pro-duces peptic ulcer disease. The COX2inhibitors appear to be an alternativebut are no longer recommended. Top-iramate is reported to be useful inHC,41,42 and its success is confirmed inpractice. Greater occipital nerve injec-tion with lidocaine and methylprednis-olone are also reported to be helpful.33
The most promising approach is oc-cipital nerve stimulation.43
REFERENCES1. Goadsby PJ, Lipton RB. A review of
paroxysmal hemicranias, SUNCT syndromeand other short-lasting headaches withautonomic feature, including new cases.Brain 1997;120(1):193Y209.
2. Headache Classification Subcommittee ofthe International Headache Society. TheInternational Classification of HeadacheDisorders. 2nd edition. Cephalalgia2004;24(suppl 1):9Y160.
3. Goadsby PJ, Cittadini E, Burns B, Cohen AS.Trigeminal autonomic cephalalgias:diagnostic and therapeutic developments.Curr Opin Neurol 2008;21(3):323Y330.
4. Frese A, Evers S, May A. Autonomicactivation in experimental trigeminalpain. Cephalalgia 2003;23(1):67Y68.
5. Obermann M, Yoon M-S, Dommes P,et al. Prevalence of trigeminal autonomicsymptoms in migraine: a population-basedstudy. Cephalalgia 2007;27(6):504Y509.
6. Eross E, Dodick D, Eross M. The Sinus,Allergy and Migraine Study (SAMS).Headache 2007;47(2):213Y224.
7. Schreiber CP, Hutchinson S, Webster CJ,et al. Prevalence of migraine in patientswith a history of self-reported orphysician-diagnosed ‘‘sinus’’ headache.Arch Intern Med 2004;164(16):1769Y1772.
KEY POINT
h Hemicrania continuaresponds absolutely toindomethacin.
Case 10-1BThe patient was admitted for medication withdrawal. Prior to admission,treatment had changed from opioids to daily sumatriptan use, 50 mgonce to twice daily. He stated that this took the edge off his headaches.Sumatriptan was withdrawn. Oxygen 15 L/min was administered on threeoccasions for at least 20 minutes, but it was not useful. He was given acourse of IV dihydroergotamine by a published protocol over a 5-dayperiod.44 At discharge he had some left-sided headache, and theright-sided headache had remitted. Six weeks after discharge he still hadleft-sided headache and noted that over-the-counter naproxen wassomewhat useful. Indomethacin 50 mg 3 times daily with a proton-pumpinhibitor rendered him completely pain free.
Comment. The patient has hemicrania continua (HC). He has a history ofmigraine and a family history likely positive for migraine, which probablyprogressed to medication-overuse headache that remitted on medicationwithdrawal and dihydroergotamine.45 The differential diagnosis after theindomethacin response would be either HC or paroxysmal hemicrania.Because he has no increase in headache intensity, his phenotype is that of HC.
893Continuum Lifelong Learning Neurol 2012;18(4):883–895 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
8. Schreiber CP, Cady RK, Billings C. Oralsumatriptan for self-described ‘‘sinus’’headache. Cephalalgia 2001;21:291.
9. Bahra A, Goadsby PJ. Diagnostic delaysand mis-management in cluster headache.Acta Neurol Scand 2004;109(3):175Y179.
10. May A, Goadsby PJ. The trigeminovascularsystem in humans: pathophysiologicimplications for primary headachesyndromes of the neural influences onthe cerebral circulation. J Cereb BloodFlow Metab 1999;19(2):115Y127.
11. Irimia P, Cittadini E, Paemeleire K, et al.Unilateral photophobia or phonophobiain migraine compared with trigeminalautonomic cephalalgias. Cephalalgia2008;28(6):626Y630.
12. Lai T-H, Fuh J-L, Wang S-J. Cranial autonomicsymptoms in migraine: characteristicsand comparison with cluster headache.J Neurol Neurosurg Psychiatry 2009;80(10):1116Y1119.
13. Levy M, Matharu MS, Meeran K, et al.The clinical characteristics of headachein patients with pituitary tumours. Brain2005;128(pt 8):1921Y1930.
14. Sprenger T, Goadsby PJ. What hasfunctional neuroimaging done for primaryheadacheIand for the clinical neurologist?J Clin Neurosci 2010;17(5):547Y553.
15. Favier I, van Vliet JA, Roon KI,et al. Trigeminal autonomic cephalgiasdue to structural lesions: a review of31 cases. Arch Neurol 2007;64(1):25Y31.
16. Olesen J, Tfelt-Hansen P, Ramadan N,et al. The Headaches. Philadelphia,PA: Lippincott Williams & Wilkins, 2005.
17. May A, Bahra A, Buchel C, et al.Hypothalamic activation in clusterheadache attacks. Lancet 1998;352(9124):275Y278.
18. May A, Ashburner J, Buchel C,et al. Correlation between structuraland functional changes in brain in anidiopathic headache syndrome.Nat Med 1999;5(7):836Y838.
19. May A, Leone M, Afra J, et al. EFNSguidelines on the treatment of clusterheadache and other trigeminal-autonomiccephalalgias. Eur J Neurol 2006;13(10):1066Y1077.
20. Bussone G, Leone M, Peccarisi C,et al. Double blind comparison oflithium and verapamil in clusterheadache prophylaxis. Headache1990;30(7):411Y417.
21. Cohen AS, Matharu MS, Goadsby PJ.Electrocardiographic abnormalities inpatients with cluster headache on verapamiltherapy. Neurology 2007;69(7):668Y675.
22. Cohen AS, Burns B, Goadsby PJ.High-flow oxygen for treatment ofcluster headache: a randomized trial.JAMA 2009;302(22):2451Y2457.
23. Treatment of acute cluster headachewith sumatriptan. The SumatriptanCluster Headache Study Group. N EnglJ Med 1991;325(5):322Y326.
24. van Vliet JA, Bahra A, Martin V,et al. Intranasal sumatriptan in clusterheadache: randomized placebo-controlleddouble-blind study. Neurology 2003;60(4):630Y633.
25. Cittadini E, May A, Straube A,et al. Effectiveness of intranasalzolmitriptan in acute cluster headache:a randomized, placebo-controlled,double-blind crossover study. ArchNeurol 2006;63(11):1537Y1542.
26. Leone M, Proietti Cecchini A, Franzini A,et al. Lessons from 8 years’ experience ofhypothalamic stimulation in clusterheadache. Cephalalgia 2008;28(7):787Y797.
27. Burns B, Watkins L, Goadsby PJ. Successfultreatment of medically intractable clusterheadache using occipital nerve stimulation(ONS). Lancet 2007;369:1099Y1106.
28. Cittadini E, Matharu MS, Goadsby PJ.Paroxysmal hemicrania: a prospectiveclinical study of 31 cases. Brain2008;131(pt 4):1142Y1155.
29. Cohen AS, Matharu MS, Goadsby PJ.Short-lasting unilateral neuralgiformheadache attacks with conjunctivalinjection and tearing (SUNCT) or cranialautonomic features (SUNA)—a prospectiveclinical study of SUNCT and SUNA. Brain2006;129(pt 10):2746Y2760.
30. Bahra A, May A, Goadsby PJ. Clusterheadache: a prospective clinical studywith diagnostic implications. Neurology2002;58(3):354Y361.
31. Sjaastad O. Chronic paroxysmal hemicrania,hemicrania continua and SUNCT: thefate of the three first described cases.J Headache Pain 2006;7(3):151Y156.
32. Cohen AS, Goadsby PJ. Paroxysmal hemicraniaresponding to topiramate. J Neurol NeurosurgPsychiatry 2007;78(1):96Y97.
33. Afridi SK, Shields KG, Bhola R, Goadsby PJ.Greater occipital nerve injection inprimary headache syndromes—prolonged
894 www.aan.com/continuum August 2012
Trigeminal Autonomic Cephalalgias
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
effects from a single injection. Pain2006;122(1Y2):126Y129.
34. Cohen AS, Matharu MS, Goadsby PJ.Suggested guidelines for treating SUNCTand SUNA. Cephalalgia 2005;25:1200.
35. Cohen A, Matharu MS, Goadsby PJ.Double-blind placebo-controlled trial oftopiramate in SUNCT. Cephalalgia2007;27:758.
36. Matharu MS, Cohen AS, Goadsby PJ.Intravenous lidocaine is effective inthe treatment of SUNCT syndrome.Cephalalgia 2003;23:738.
37. Cittadini E, Goadsby PJ. Hemicraniacontinua: a clinical study of 39 patientswith diagnostic implications. Brain2010;133(pt 7):1973Y1986.
38. Medina JL, Diamond S. Cluster headachevariant. Spectrum of a new headachesyndrome. Arch Neurol 1981;38(11):705Y709.
39. Sjaastad O, Spierings EL. ‘‘Hemicraniacontinua’’: another headache absolutelyresponsive to indomethacin. Cephalalgia1984;4(1):65Y70.
40. Newman LC, Lipton RB, Solomon S.
Hemicrania continua: ten new casesand a review of the literature.Neurology 1994;44(11):2111Y2114.
41. Brighina F, Palermo A, Cosentino G, Fierro B.Prophylaxis of hemicrania continua:two new cases effectively treated withtopiramate. Headache 2007;47(3):441Y443.
42. Camarda C, Camarda R, Monastero R.Chronic paroxysmal hemicrania andhemicrania continua responding totopiramate: two case reports. Clin NeurolNeurosurg 2008;110(1):88Y91.
43. Burns B, Watkins L, Goadsby PJ.Treatment of hemicrania continua byoccipital nerve stimulation with a novelbion device: long-term follow-up ofa crossover study. Lancet Neurol2008;7(11):1001Y1012.
44. Nagy AJ, Gandhi S, Bhola R, Goadsby PJ.Intravenous dihydroergotamine forinpatient management of refractoryprimary headaches. Neurology2011;77(20):1827Y1832.
45. Goadsby PJ. Is medication-overuseheadache a distinct biological entity?Nat Clin Pract Neurol 2006;2(8):401.
895Continuum Lifelong Learning Neurol 2012;18(4):883–895 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.