Embed Size (px)
Citation preview

8/3/2019 Tuberculosa Nasofaring Ftp
http://slidepdf.com/reader/full/tuberculosa-nasofaring-ftp 1/4
The LaryngoscopeLippincott Williams & Wilkins, Inc., Philadelphia © 2003 The American Laryngological,Rhinological and Otological Society, Inc.
Tuberculosis of the Nasopharynx: A Rare
Entity RevisitedGary M. K. Tse, FRCPC; Tony K. F. Ma, FRCPA; Amy B. W. Chan, MBChB; Fiona N. Y. Ho, FRCS; Ann D. King, FRCR; Kitty S. C. Fung, FRCPA; Anil T. Ahuja, FRCR
Objectives: Tuberculosis of the nasopharynx isuncommon. A large series of 17 cases is reported, andthe clinical and pathological features are discussed.Study Design: A retrospective review. Methods: Seven-teen archived cases of biopsy-proven nasopharyngealtuberculosis were reviewed for patient age and sex,presenting complaint and duration, systemic symp-toms, cervical lymphadenopathy, and chest x-rayfindings. These findings were compared with a com-pilation of 40 cases reported in the English literature. Results: There was a female predominance (13 womenand 4 men), with age range of 20 to 74 years (meanage, 38 y). The most common presentation was en-largement of the cervical lymph nodes (53%), followedby hearing loss (12%), tinnitus, otalgia, nasal obstruc-tion, and postnasaldrip (6%each). The duration of thepresenting symptoms ranged from 1 week to 1 year(mean duration, 16 wk). Ten patients (59%) had cervi-cal lymphadenopathy, two (12%) had systemic symp-toms (fever, weight loss, night sweats), and one pa-tient (6%) had miliary pulmonary tuberculosis. Directendoscopic examination showed nasopharyngeal mu-cosal irregularity or mass in the majority of patients(12 patients [70%]). These features were similar tothose reported in the literature. Conclusions: Naso-pharyngeal tuberculosis is uncommon, usually occur-ring without pulmonary or systemic involvement.Cervical lymphadenopathy occurs in more than half of the patients and is the most common presentingcomplaint; this, together with the nasopharyngealfindings of mass or mucosal irregularity, makes dif-ferentiation from carcinoma on clinical examinationdifficult, necessitating histological evaluation. KeyWords: Nasopharynx, tuberculosis, undifferentiatedcarcinoma, granuloma, granulomatous inflammation.
Laryngoscope, 113:737–740, 2003
INTRODUCTIONTuberculosis (TB) of the nasopharynx is rare. Al-
though the upper respiratory tract is the usual portal of entry for pulmonary TB, involvement of the upper respi-ratory tract either in isolation or as part of systemic (or
pulmonary) disease remains uncommon. In a large histor-ical series of 843 cases of TB, only 1.8% of cases showedupper respiratory tract involvement, with one case of na-sopharyngeal involvement. 1 In the English literature,only three large series described nasopharyngeal TB indetail, and these series, respectively, reported 7 to 14cases. 2– 4 The remainder of reports in the literature weresingle case reports, approximately 10 cases in all. 5–14 Inthe present case series, the authors reviewed 17 cases,with emphasis on the disease features as compared withthe previous series.
MATERIALS AND METHODS Archived material from the Department of Pathology was
searched for TB of nasopharynx from 1990 to 2002, yielding 20cases in all. Three patients had a history of concurrent undiffer-entiated carcinoma (nasopharyngeal carcinoma [NPC]) and wereexcluded from the present review. All the medical records wereretrieved. The information extracted, when available, includedage, sex, presenting complaint and duration, systemic symptoms,clinical examination findings including appearance of the naso-pharynx, and chest x-ray findings. The pathological materials of the nasopharyngeal biopsies were retrieved and reviewed, andthe diagnosis confirmed. Ziehl Neelsen staining was performed onthe biopsy material to detect acid-fast bacilli, and in some cases,multiple sections were examined.
RESULTSSeventeen cases were reviewed, of which 13 were in
women and four were in men. The patient age range was20 to 74 years (mean age, 39 y). Ten patients (59%)presented with enlarged neck nodes, including eight(47%) with unilateral nodes and two (12%) with bilat-eral nodes. Two patients (12%) presented with hearingand one patient (6%) each presented with tinnitus, otal-gia, nasal obstruction, and postnasal drip. One patient(6%) did not have any symptoms referable to the headand neck region. The duration of the presenting symp-toms ranged from 1 week to 1 year (mean duration, 16wk). Only two patients (12%) had fever, night sweats,
From the Departments of Anatomical and Cellular Pathology(G.M .K .T., A.B.W.C.) and Surgery ( F .N . Y.H .), Division of Otorhinolaryngology,and the Departments of Diagnostic Radiology and Organ Imaging ( A.D.K ., A.T. A.) and Microbiology ( K .S.C.F .), Prince of Wales Hospital, Chinese Uni- versity of Hong Kong; and the Department of Pathology ( T.K .F .M.), Alice HoMin Ling Nethersole Hospital, Republic of China.
Editor’s Note: This Manuscript was accepted for publication Novem-ber 26, 2002.
Send Correspondence to Gary M. K. Tse, FRCPC, Department of Anatomical and Cellular Pathology, Ngan Shing Street, Shatin, NT, HongKong, Republic of China. E-mail: [email protected]
Laryngoscope 113: April 2003 Tse et al.: Nasopharyngeal Tuberculosis
737

8/3/2019 Tuberculosa Nasofaring Ftp
http://slidepdf.com/reader/full/tuberculosa-nasofaring-ftp 2/4
and weight loss. Endoscopic examination of the naso-pharynx showed mucosal irregularity, resembling lym-phoid hyperplasia in six (35%) patients, a nasopharyn-geal mass in six patients (35%), mucosal swelling in onepatient (6%), white patch on mucosa in one patient (6%),and ulceration in one patient (6%). In one patient (6%)
the nasopharynx appeared normal. In one case, thefinding was not recorded. Chest x-ray examinationshowed miliary TB in one patient (6%) and features of old lesions in four patients (24%). For the remaining 12patients, 4 (24%) had normal chest x-ray findings andthe results were not recorded in 8 patients.
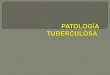
Fig. 1. Nasopharyngeal biopsy specimen with surface respiratory epithelium (short arrow) and multiple granulomas composed of epithelioidhistiocytes (long arrow) in the submucosa (H&E stain, original magnification 00). Inset: Acid-fast bacilli, consistent with Mycobacteriatuberculosis is seen (inset, Ziehl Neelsen, original magnification 400).
TABLE I.Clinical Features of All Patients.
CaseNo. Sex
Age(y)
Duration(wk)
PresentingSymptoms
SystemicSymptoms Nasopharyngeal Appearance Chest X-ray
1 F 24 8 Otalgia Yes Granular Not available2 M 20 Unknown Unknown Unknown Unknown Not available3 F 30 4 Neck node Yes Lymphoid hyperplasia Normal4 F 69 8 Right ear tinnitus No Roof mass Pleural thickening5 F 74 16 Neck node No Normal Apical pleural thickening6 F 28 12 Neck node No Rough right wall Normal7 F 19 52 Nasal
obstructionNo Large exophytic mass at all wall Not available
8 M 23 1 Neck node No Irregular Miliary TB9 F 22 24 Neck node No Central lymphoid hyperplasia Normal10 F 64 8 Neck node No Bulging mass Right upper lobe old granuloma11 F 29 Unknown Hearing loss No Lymphoid Not available12 F 49 Unknown Left hearing loss No Right whitish patch Not available13 F 29 16 Neck node (bilat) No Central swelling Not available14 F 31 Unknown Neck node No Mass Not available15 M 22 8 Neck node (bilat) No Irregular ulcer at right central NP Normal16 F 61 8 Neck node No Mass Right upper zone fibrocalcified change17 M 63 52 Nasal
obstructionNo Mass Not available
Laryngoscope 113: April 2003 Tse et al.: Nasopharyngeal Tuberculosis
738

8/3/2019 Tuberculosa Nasofaring Ftp
http://slidepdf.com/reader/full/tuberculosa-nasofaring-ftp 3/4
In all cases, nasopharyngeal biopsies were performedto rule out NPC, which has a similar presentation and ahigh incidence in this locality. The biopsy specimensshowed granulomatous inflammation with epithelioid his-tiocytes and multinucleated giant cells of Langerhanstype. Ziehl Neelsen staining for acid-fast bacilli was pos-itive in all cases (Fig. 1). All the patients responded totreatment for TB.
DISCUSSION
Nasopharyngeal TB represents an uncommon andunique form of TB infection. This disease is rare, and thenumber of reported cases in the English literature is low.The current report represents the largest series. Beforethe present report, there were three large series reportedin the English literature, being written 6, 10, and 30 years
ago, respectively. 1 – 3 Hence, it is of great interest to com-pare the clinical features of the current cases (Table I) inthe present series with the historical compilation (Table II).
In our series, neck lymph node enlargement as apresenting symptom accounted for 53% of cases, whereassymptoms referable to the ear and nose area in terms of tinnitus, nasal obstruction, hearing loss, and otalgia ac-counted for most of the remainder. These findings weresimilar to those in the literature, in which enlarged lymphnodes was the most common (58%) presenting symptomfollowed by nasal obstruction (10%) and pain around thehead and neck region, tinnitus, and hearing loss. Directexamination of the nasopharynx revealed a combination of mass and irregularity, which, together, accounted for amajor proportion (70%) in our series and 75% of cases inthe literature. More important, findings on direct exami-
TABLE II.Clinical Features of All Patients Reported in the Literature.
PatientNo. Year Reference Sex/Age (y) Complaint Duration (wk) NP Appearance LN NP Biopsy Lung
1 1992 2* M/37 Neck node 12 Irregularity Yes Neg No
2 1992 2 M/35 Neck node 16 Mass Yes Pos No
3 1992 2 F/26 Decrease hearing 12 Irregularity No Pos No
4 1992 2 F/38 Unknown 12 Mass No Pos Active TB
5 1992 2 F/25 Nasal obstruction 4 Mass Yes Pos No
6 1992 2 F/76 Nasal obstruction 20 Mass Yes Pos No
7 1992 2 M/48 Neck node 4 Irregularity Yes Neg No
8 1992 2 M/41 Neck node 12 Irregularity Yes Neg Old TB
9 1992 2 F/27 Neck node 8 Mass Yes Neg No
10 1972 3 M/18 Neck node 25 Mass Yes Pos No
11 1972 3 M/26 Headache 4 Mass No Pos No
12 1972 3 F/59 Neck node 16 White discoloration Yes Pos No
13 1972 3 F/22 Neck node 25 Mass Yes Neg No
14 1972 3 F/36 Neck node 16 Mass Yes Pos No
15 1972 3 F/57 Neck node 12 Irregularity Yes Neg No
16 1972 3 F/47 Sore throat 25 Mass Yes Pos No
17 1999 5 F/20 Chronic otitis media 52 Unknown Unknown Pos Old TB18 1984 6 M/35 Neck node 4 Irregular, right Yes Pos No
19 1986 7 F/54 Facial pain 1 Mass Unknown Pos Active TB ondrug for 1year
20 1992 8 F/58 Otalgia 12 Slough No Neg No
21 1999 9 F/64 Pharyngeal pain 8 Swelling No Neg Micronodules,nodes pos
22 1994 10 F/42 Nasal obstruction Unknown Mass, midline Unknown Neg No
23 2002 11 F/58 Snoring Unknown Swelling No Neg No
24 1997 12 F/70 Altered taste/smell 16 Unknown Unknown Neg Old TB
25 1985 13 F/18 Neck LN 3 Unknown Yes Neg No
26 1981 14 M/62 Nasal obstruction Unknown Mass Unknown Pos No
27–40† 1996 4 M 12 Neck node 11 16 wk 12 Mass 11 Yes 12 Pos 14 Active TB 7
F 2 Post nasal drip 2 or 16 wk 2 Normal 2 No 2 No 7
Range 17–61 Brisk epistasis 2
Mean 34
*This series reported 10 cases, but one patient had NPC and TB and was thus excluded from this review.†This series reported 14 cases, but individual patients’ data were not reported or tabulated separately.LN cervicallymphadenopathy; NP biopsy nasopharyngeal biopsy; neg granulomatous inflammation but direct stain for acidfast bacilli negative;pos
granulomatous inflammation and positive direct Ziehl Neelsen stain for acid fast bacilli.
Laryngoscope 113: April 2003 Tse et al.: Nasopharyngeal Tuberculosis
739

8/3/2019 Tuberculosa Nasofaring Ftp
http://slidepdf.com/reader/full/tuberculosa-nasofaring-ftp 4/4
nation may be normal, as was shown in one case (6%) inour series and two cases (5%) in the literature.
The relation among TB of the nasopharynx, cervicallymph nodes, and pulmonary infection merits further dis-cussion. In primary nasopharyngeal TB, involvement of the cervical nodes is common, occurring in more than 50%of cases. Co-existing active or old pulmonary involvementor systemic disease is less common, with 30% (five cases)occurring in our series and 25% in the literature. Con- versely, nasopharyngeal involvement in TB cervicallymphadenopathy and pulmonary TB is exceeding rare. Inan elegant study of 75 patients with excision-proven TB of cervical nodes, the nasopharynx was shown to be the onlyprimary focus of infection in one patient (1%), withoutpulmonary or systemic involvement. 15 The same was truefor pulmonary TB, with a reported incidence of nasopha-ryngeal involvement in 1.8% of cases only. 1 The inferenceis that TB of the nasopharyngeal is usually primary andisolated; the chance of co-existing lung infection is low.The mechanism for such a phenomenon remains unclear.Involvement of TB of the upper airways was by contiguousspread from the active lung lesion through infected spu-
tum or other secretion. In a large series of cases of laryn-geal TB, abnormal findings on chest x-ray examinationwere noted in 95% of patients. 16 However, the rate of lunginvolvement in nasopharyngeal TB is low, suggesting thatcontiguous spread would have to occur from ongoing orreactivation of subclinical pulmonary TB, or the nasophar-ynx truly represents the primary portal of transmissionfrom inhalation of TB in airborne droplets. Cervicallymphadenopathy in nasopharyngeal TB is common anddoes not imply systemic spread of the disease. The com-mon scenario of enlarged cervical lymph nodes with anasopharyngeal mass or irregularity, but without sys-temic symptoms, makes the disease virtually indistin-guishable from NPC, making histological evaluation im-perative in endemic areas such as southern China.
The contribution of TB in the causation of granulo-matous diseases in the head and neck region remainsdifficult to estimate. Other causes of granulomas includesarcoidosis, vasculitic diseases such as Wegener ’s granu-lomatosis, fungal infections or reactive changes in re-sponse to carcinoma or lymphoma (particularly Hodgkin ’sdisease), and radiotherapy. Because positive identificationof the acid-fast bacilli in smears or cultures is a prerequi-site for diagnosis of TB, its incidence is likely to be under-estimated. In a study of 22 cases of tonsillar granulo-mas, 17 no underlying cause was identified in one-third of the cases, and the possibility of undiagnosed TB has to be
considered. With the improvement of techniques for de-tecting TB, including polymerase chain reaction for thebacterial DNA, and increased awareness, particularly in view of the resurgence of TB, the incidence of TB of theupper aerodigestive tract is likely to increase.
The authors have reported a large series of cases of nasopharyngeal TB, which showed a female predomi-nance, as well as neck node enlargement as the mostcommon presentation. In the majority of cases, examina-tion showed a mass lesion or mucosal irregularity in thenasopharynx, making differentiation from carcinoma dif-ficult. This poses a particular diagnostic problem in someregions of the world such as Southeast Asia and Africa,where NPC and TB are endemic, particularly becauseenlarged cervical lymph nodes are a common presentingsymptom in both diseases. Furthermore, nasopharynx TBis usually isolated, without pulmonary or systemic symp-toms. The similar clinical features of patients included inthe current series and those reported 10 to 30 years agohas suggested that little progress has been made in theearly detection of the disease. With the recent resurgenceof TB, it is imperative to be aware of the rare cases of nasopharyngeal TB.
BIBLIOGRAPHY
1. Rohwedder JJ. Upper respiratory tract tuberculosis: sixteencases in a general hospital. Ann Intern Med 1974;80:708 –713.
2. Waldron J, van Hasselt CA, Skinner DW, Arnold M. Tuber-culosis of the nasopharynx: clinicopathological features.Clin Otolaryngol 1992;17:57 –59.
3. Sim T, Ong BH. Primary tuberculosis of the nasopharynx. Singapore Med J 1972;13:39 – 43.
4. Eng HL, Su CY, Chen WJ. Nasopharyngeal tuberculosis.Chang Gung Med J 1996;19:149 –153.
5. Case records of the Massachusetts General Hospital: case 13. N Engl J Med 1999;340:1349 –1354.
6. Raizada RM, Behl R, Bhongsade V, Khan N. Primary naso-pharyngeal tuberculosis. Ear Nose Throat J 1984;63:70 –74.
7. Narendran K, Chan R, Poh WT. Nasopharyngeal tuberculosispresenting as a mass. Singapore Med J 1986;27:170 –172.
8. Bath AP, O ’Flynn P, Gibbin KP. Nasopharyngeal tuberculo-sis. J Laryngol Otol 1992;106:1079 –1080.
9. Percodani J, Braun F, Arrue P, et al. Nasopharyngeal tuber-culosis. J Laryngol Otol 1999;113:928 –931.10. Chopra RK, Kerner MM, Calcaterra TC. Primary nasopha-
ryngeal tuberculosis: a case report and review of this rareentity. Otolaryngol Head Neck Surg 1994;111:820 – 823.
11. Atkan B, Selimoglu E, Ucuncu H, Sutbeyaz Y. Primary na-sopharyngeal tuberculosis in a patient with the complaintof snoring. J Laryngol Otol 2002;116:301 –303.
12. Butt AA. Nasal tuberculosis in the 20th century. Am J Med Sci 1997;313:332 –335.
13. Lesser THJ, Jefferis AS, Shaw HJ. Pseudotumoral mycobac-terial infections of the head and neck. J Laryngol Otol1985;99:277 –283.
14. Goodman RS, Mattel S, Kaufman D, Grant JM. Tuberculomaof the nasopharynx. Laryngoscope 1981;91:194 –197.
15. Lau SK, Kwan S, Lee J, Wei WI. Source of tubercle bacilli incervical lymph nodes: a prospective study. J Laryngol Otol
1991;105:558 –561.16. Rupa V, Bhanu TS. Laryngeal tuberculosis in the eighties: an
Indian experience. J Laryngol Otol 1989;103:864 – 868.17. Kardon DE, Lester DR, Thompson MD. A clinicopathologic
series of 22 cases of tonsillar granulomas. Laryngoscope2000;110:476 – 481.
Laryngoscope 113: April 2003 Tse et al.: Nasopharyngeal Tuberculosis
740