Embed Size (px)
Citation preview

Tuberculosis, HIV, malaria andneglected tropical diseasesStrengthening collaboration
to prevent and manage antimicrobialresistance

Tuberculosis, HIV, malaria andneglected tropical diseases
Strengthening collaborationto prevent and manage antimicrobial
resistance
AMR_brochure.indd 1 27/03/19 10:12 am

Tuberculosis, HIV, malaria and neglected tropical diseases: strengthening collaboration to preventandmanage antimicrobial resistance
ISBN 978-92-4-151545-0
©World Health Organization 2019
Some rights reserved. This work is available under the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO; https://creativecommons.org/licenses/by-nc-sa/3.0/igo).
Under the terms of this licence, youmay copy, redistribute and adapt the work for non-commercial purposes,provided the work is appropriately cited, as indicated below. In any use of this work, there should be nosuggestion thatWHO endorses any specific organization, products or services. The use of theWHO logo isnot permitted. If you adapt the work, then youmust license your work under the same or equivalent CreativeCommons licence. If you create a translation of this work, you should add the following disclaimer along withthe suggested citation: “This translation was not created by theWorld Health Organization (WHO). WHO isnot responsible for the content or accuracy of this translation. The original English edition shall be the bindingand authentic edition”.
Any mediation relating to disputes arising under the licence shall be conducted in accordance with themediation rules of theWorld Intellectual Property Organization.
Suggested citation. Tuberculosis, HIV, malaria and neglected tropical diseases: strengthening collaboration toprevent andmanage antimicrobial resistance. Geneva:World Health Organization; 2019. Licence:CC BY-NC-SA 3.0 IGO.
Cataloguing-in-Publication (CIP) data. CIP data are available at http://apps.who.int/iris.
Sales, rights and licensing. To purchaseWHO publications, see http://apps.who.int/bookorders. To submitrequests for commercial use and queries on rights and licensing, see http://www.who.int/about/licensing.
Third-party materials. If you wish to reuse material from this work that is attributed to a third party, such astables, figures or images, it is your responsibility to determine whether permission is needed for that reuseand to obtain permission from the copyright holder. The risk of claims resulting from infringement of anythird-party-owned component in the work rests solely with the user.
General disclaimers. The designations employed and the presentation of thematerial in this publication donot imply the expression of any opinion whatsoever on the part ofWHO concerning the legal status of anycountry, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries.Dotted and dashed lines onmaps represent approximate border lines for which there may not yet be fullagreement.
Themention of specific companies or of certain manufacturers’ products does not imply that they areendorsed or recommended byWHO in preference to others of a similar nature that are not mentioned. Errorsand omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken byWHO to verify the information contained in this publication.However, the publishedmaterial is being distributed without warranty of any kind, either expressed orimplied. The responsibility for the interpretation and use of thematerial lies with the reader. In no event shallWHO be liable for damages arising from its use.
Printed in France
AMR_brochure.indd 2 27/03/19 10:12 am

iiiSTRENGTHENING COLLABORATION TO PREVENT AND MANAGE ANTIMICROBIAL RESISTANCE
Contents
Abbreviations iv
Foreword v
Executive summary 1
1. Introduction 2
2. Background 3
2.1 Antimicrobial resistance 3
2.2 Sustainable Development Goals 3
2.3 How antimicrobial resistance aúects the achievement of the Sustainable Development Goals 3
2.4 Global Action Plan on Antimicrobial Resistance 4
2.5 Ad hoc United Nations Interagency Coordination Group on Antimicrobial Resistance 5
2.6 WHO 13th General Programme ofWork (2019–2023) 5
2.7 TB, HIV, malaria, neglected tropical diseases and antimicrobial resistance 6
3. Current antimicrobial resistance status: TB, HIV, malaria and relevant neglected tropical diseases 9
3.1 Factors driving antimicrobial resistance across disease areas 9
3.2 Tuberculosis 10
3.3 HIV 12
3.4 Malaria 13
3.5 Neglected tropical diseases 14
4. Preventing antimicrobial resistance related to TB, HIV, malaria and neglected tropical diseasesand theWHO response 15
4.1 Preventing antimicrobial resistance 15
4.2 Surveillance of antimicrobial resistance 16
4.3 Laboratory networks 21
4.4 Communication, awareness-raising, education and training 23
5. Future directions 25
5.1 Identify research and development gaps and new tools and approaches 26
5.2 Clinical and programmatic indicators associated with and predicting the emergenceof antimicrobial resistance 28
5.3 Joint support for countries 30
5.4 Identifying and optimizing synergy 31
5.5 Product pipelines 31
References 32
WHO antimicrobial resistance resources 34
Antimicrobial resistance – general 34
TB 34
HIV 35
Malaria 35
Neglected tropical diseases 36
AMR_brochure.indd 3 27/03/19 10:12 am

iv TUBERCULOSIS , HIV, MALARIA AND NEGLECTED TROPICAL DISEASES
Abbreviations
ACT artemisinin-based combination therapy
AIDS acquired immunodeficiency syndrome
AMR antimicrobial resistance
BBINS Bangladesh, Bhutan, India, Nepal, Sri Lanka
DNDi Drugs for Neglected Diseases initiative
FAO Food and Agriculture Organization of the United Nations
GAP Global Action Plan on Antimicrobial Resistance
GLASS Global Antimicrobial Resistance Surveillance System
HANMAT Horn of Africa Network for Monitoring Antimalarial Treatment
HIV human immunodeficiency virus
IACG Interagency Coordination Group on Antimicrobial Resistance
MDR-TB multidrug-resistant tuberculosis
MMV Medicines for Malaria Venture
NTD neglected tropical disease
OIE World Organisation for Animal Health
PEPFAR United States President’s Emergency Plan for AIDS Relief
PIAMNET Pakistan, Islamic Republic of Iran and Afghanistanmonitoring network
RAVREDRA Red Amazónica para la Vigilancia de la Resistencia a las Drogas Antimaláricas network
RR-TB rifampicin-resistant tuberculosis
TB tuberculosis
UNEP United Nations Environment Programme
USAID United States Agency for International Development
WHO World Health Organization
XDR-TB extensively drug-resistant tuberculosis
AMR_brochure.indd 4 27/03/19 10:12 am

vSTRENGTHENING COLLABORATION TO PREVENT AND MANAGE ANTIMICROBIAL RESISTANCE
Foreword
Antimicrobial resistance is one of the greatesthealth challenges of the 21st century, as recognizedin the 2015World Health Assembly resolutionon antimicrobial resistance and the 2016 PoliticalDeclaration of the High-level Meeting of theUnited Nations General Assembly on AntimicrobialResistance. If antimicrobial resistance is notaddressed, it may contribute to millions of deathsper year and cost the world economy US$ 1–3trillion per year after 2030 (1). Drug-resistant TB,HIV, malaria and some neglected tropical diseaseswill make a substantial contribution to this burden.Antimicrobial resistance threatens to take us backto a time when common infections could not betreated and often led to sustained illness and death.To preserve the health gains of the past century, wewill need to take eúective and coordinated action.
WHO has recognized the importance ofantimicrobial resistance in its 13th GeneralProgramme ofWork, which requires allprogrammes at all levels of the Organization toaddress antimicrobial resistance as a cross-cuttingissue. Antimicrobial resistance will impact theachievement of the triple billion targets, especiallyuniversal health coverage. The three objectives ofuniversal health coverage including equity, qualityand protection from financial risk will not bemetwithout also eúectively addressing antimicrobialresistance. Equally, universal health coverage alsooúers an excellent opportunity for preventing andmanaging antimicrobial resistance.
WHO is leading the fight to prevent and containantimicrobial resistance in human health and hasbeen working in close collaboration with the Foodand Agriculture Organization of the United Nations(FAO), theWorld Organization for Animal Health(OIE) (the FAO/OIE/WHO Tripartite Collaborationon Antimicrobial Resistance) and the United NationsEnvironment Programme (UNEP). The Tripartiteorganizations are working together through theInteragency Coordination Group on AntimicrobialResistance (IACG) and reaûrmed their commitment
to strengthen collaboration in amemorandum ofunderstanding signed inMay 2018. The IACGwillissue a final report to the United Nations Secretary-General in 2019 that re-emphasizes the urgency andthe need for a coordinated and stepped-up globalresponse.
The Tripartite and UNEP have developed aOne Health approach tomanaging antimicrobialresistance, as proposed in the Global Action Planon Antimicrobial Resistance (GAP), launchedin 2015. This plan focuses on the importanceof strengthening systems for preventing andmanaging infection, with more appropriate useof antimicrobial agents, as well as strengtheningsystems for surveillance. One of the core elementsof the GAP is to support countries to develop andimplement comprehensive, One Health-orientedantimicrobial resistance action plans. As of January2019, 117 countries have developed nationalantimicrobial resistance action plans with supportfrom partners. WHO has also developed GLASS, theGlobal Antimicrobial Surveillance System.
Antimicrobial resistance is also a major challengefor TB, HIV andmalaria and has the potentialto adversely aúect neglected tropical diseaseprogrammes. Sustainable Development Goal target3.3 calls for ending the epidemics of these diseasesby 2030.While antimicrobial resistance puts theachievement of many Sustainable DevelopmentGoals at risk, Sustainable Development Goaltarget 3.3 is especially aúected, with antimicrobialresistancemaking treating these diseases morediûcult and expensive.
TB, HIV, malaria and neglected tropical diseaseprogrammes have been working to address theantimicrobial resistance challenge for many yearsby focusing on supporting national and globalsurveillance networks, strengthening laboratorynetworks, optimizing diagnostic testing andtreatment, raising awareness of the dangersof antimicrobial resistance andworking withkey stakeholders to drive product and service
AMR_brochure.indd 5 27/03/19 10:12 am

vi TUBERCULOSIS , HIV, MALARIA AND NEGLECTED TROPICAL DISEASES
delivery innovation. These same interventionsare core components of strategies to preventandmanage antimicrobial resistance across thehuman health spectrum. Lessons learned and goodpractices gained from experience in preventingandmanaging antimicrobial resistance in thesediseases can be adapted and used to strengthenantimicrobial resistance approaches in othersettings.
Current opportunities exist to strengthenantimicrobial resistance collaboration at thecountry level by identifying and strengthening
programmatic synergies that underpin strategies forpreventing andmanaging antimicrobial resistance.This will require, for example, ensuring thatcountries develop and implement comprehensive,antimicrobial resistance action plans thatinclude TB, HIV, malaria and neglected tropicaldiseases where relevant. Achieving this requiresa coordinated eúort, working in partnership,involving all stakeholders at the global, regional,country and service delivery levels. Preventing andmanaging antimicrobial resistance will truly requiresustained eúorts and global collaboration.
RenMinghuiAssistant Director-General for Communicable Diseases
Raniero GuerraAssistant Director-General for Strategic Initiatives
AMR_brochure.indd 6 27/03/19 10:12 am

1STRENGTHENING COLLABORATION TO PREVENT AND MANAGE ANTIMICROBIAL RESISTANCE
Executive summary
There is global commitment to addressantimicrobial resistance through the Global ActionPlan on Antimicrobial Resistance. High-impactcommunicable diseases, including tuberculosis(TB), human immunodeficiency virus (HIV),malaria and neglected tropical diseases (NTDs),should be integrated into and aligned with globalantimicrobial resistance eúorts.
Antimicrobial resistance puts achievementof Sustainable Development Goal 3 and otherSustainable Development Goals at risk, makingeúectively treating diseases more diûcult and costlyand leading tomore illness and deaths.
Lessons learned from addressing antimicrobialresistance in TB and the other diseases during thepast 20 years provide useful guidance for otherantimicrobial resistance programmes in earlierstages of development, including:
ÿ recognizing at an early stage the antimicrobialresistance challenge and advocating andmobilizing global development partners toaddress it;
ÿ establishing a global antimicrobial resistancesurveillance system;
ÿ establishing direct drug resistance testingfor individual patients, providing data forpopulation-based surveillance;
ÿ expanding and strengthening national andregional laboratory networks;
ÿ strengthening country capacity for managingantimicrobial resistance;
ÿ reaching out to stakeholders at all levels througha public–private mix, including engagingpharmacies and health-care providers to providetraining on testing and treatment protocols; and
ÿ establishing product development partnershipsand research consortiums to facilitate theintroduction of new pipeline drugs, reviewnew drug formulations and develop improveddiagnostic tests to detect antimicrobialresistance.
AMR_brochure.indd 1 27/03/19 10:12 am

2 TUBERCULOSIS , HIV, MALARIA AND NEGLECTED TROPICAL DISEASES
1. Introduction
The purpose of this report is to provide a briefoverview of the status of antimicrobial resistancein high-impact communicable diseases (TB, HIV,malaria and some neglected tropical diseases)and to present some areas in which strengthenedeúorts will be required in the future andmorecollaborative programme designmay generateeûciency and strengthened systems for addressingantimicrobial resistancemore widely. This overviewincludes a summary of the current antimicrobial
resistance situation by disease, current preventionand response eúorts in antimicrobial resistance anda future directions section examining opportunitiesfor strengthening collaboration among disease andother antimicrobial resistance programmes.
The report captures key messages in each areaand is aimed at technical and funding partners,global and national policy-makers and otherrelevant stakeholders.
AMR_brochure.indd 2 27/03/19 10:12 am

3STRENGTHENING COLLABORATION TO PREVENT AND MANAGE ANTIMICROBIAL RESISTANCE
2. Background
access to needed health-care services (includingdisease prevention, health promotion, treatment,rehabilitation and palliation) of suûcient qualityto be eúective while also ensuring that the use ofthese services does not expose the user to financialhardship.
2.3
How antimicrobial resistance aþectsthe achievement of the SustainableDevelopment Goals
Antimicrobial resistance is a substantial threatto several of the wider development goals, suchas economic growth, poverty reduction andsustainable production and consumption (Fig. 1).Progress towards other goals, such as SustainableDevelopment Goal 6 on water and sanitation andSustainable Development Goal 17 onworking inpartnership will make important contributions toaddressing antimicrobial resistance.
However, the greatest threat will be toSustainable Development Goal 3, human health.Antimicrobial resistance will make it harder totreat the diseases and lead to increased sickness,more protracted hospital stays andmore deaths.TheWorld Bank has estimated that health-care costs could increase by 25% in low-incomecountries in their worst-case scenario and reduceglobal gross domestic product (GDP) by 1–4%annually by 2050 (1). The spread of antimicrobialresistance could slow progress towards achievingSustainable Development Goal 3.3 targets for TB,HIV, malaria and potentially some specific neglectedtropical diseases if it is not managed or contained.Antimicrobial resistance will also dramaticallyincrease the costs of providing health-care services.For example, the second- and third-line HIVtreatments are 3 and 14 times more expensive,respectively, than first-line treatments (1) and leadtomore negative outcomes. Treating extensivelydrug-resistant TB (XDR-TB) takes up to two years,
2.1
Antimicrobial resistance
Antimicrobial resistance (AMR) occurs whenmicroorganisms such as bacteria, viruses, parasitesand fungi develop resistance to antimicrobialagents. Although this is a natural phenomenon, theinappropriate and excessive use of antimicrobialagents can increase the pace and spread ofantimicrobial resistance development. Diseasescaused by resistant microorganisms are morediûcult to treat.
Rising levels of drug resistance are a risk tothe success of human immunodeficiency virus(HIV), tuberculosis (TB) andmalaria programmes.Microorganisms that are resistant to antimicrobialagents threaten the successful management ofinfections, safe surgery and cancer treatment.Coinfection with resistant microorganisms posesheightened risks for people with TB and HIV (2).
2.2
Sustainable Development Goals
The United Nations adopted the SustainableDevelopment Goals (3) in September 2015.These reflect the growing complexity andinterdependence of the global developmentagenda. The Sustainable Development Goalsestablish 17 global goals that have 169 specifictargets, and if they are achieved by 2030 they willhelp to ensure the sustainability of economic andsocial development. Sustainable DevelopmentGoal 3 focuses on ensuring good health and well-being and covers infectious and noncommunicablediseases. Target 3.3 calls for ending by 2030 theepidemics of AIDS, TB, malaria and neglectedtropical diseases and reducing the incidenceof hepatitis, waterborne diseases and othercommunicable diseases. Sustainable DevelopmentGoal target 3.8 calls for universal health coverage(4), which is defined as ensuring that all people have
AMR_brochure.indd 3 27/03/19 10:12 am

4 TUBERCULOSIS , HIV, MALARIA AND NEGLECTED TROPICAL DISEASES
and the drugs and treatment required cost nearlysix times more than treatments for non-resistantTB (5). Among extensively drug-resistant TB casesstarting treatment globally in 2015, only 34%completed it or were cured (versus 82%with drug-sensitive strains), and in 45% the treatment failedor the person died (5). As noted in subsection 3.3and Fig. 10, the emergence of HIV drug resistancethreatens to reduce the gains in morbidity andmortality anticipated by a “treat all” approach andthe scale-up of pre-exposure prophylaxis.
2.4
Global Action Plan on Antimicrobial Resistance
TheWorld Health Assembly adopted the GlobalAction Plan on Antimicrobial Resistance (6) in May2015, and the Food and Agriculture Organizationof the United Nations (FAO) and theWorldOrganization for Animal Health (OIE) endorsed it.The Global Action Plan on Antimicrobial Resistancecovers antibiotic resistance in most detail but alsorefers, where appropriate, to existing action plansfor viral, parasitic and bacterial diseases, includingHIV, malaria and tuberculosis. The Global ActionPlan on Antimicrobial Resistance provides theframework for developingmultisectoral national
FIG. 1
Antimicrobial resistance and the Sustainable Development Goals
AMR hits the poor hardest with higher treatmentcosts and lost income due to illness
Untreatable infections in animalsthreatens sustainable foodproduction
Antimicrobial residues fromhospitals, pharmaceuticalcompanies and agriculturecontaminate water, spreadof resistant bacteria throughinadequate provision ofwater, sanitation andhygiene
AMR could increase healthcosts by 25% in low incomecountries and reduce globalGDP by 1 4% annually by 2050
Need tobalance access,innovation,conservation toprotectantimicrobialsto contain AMR Antimicrobials are essential for human
health
Addressing AMR requires multistakeholder approaches andone health partnerships
Addressing AMR requiresmulti-stakeholder approaches andOne
Health partnershipsAMRhits the poor hardest, with higher treatment
costs and lost income due to illness
Untreatable infections in animalsthreaten sustainable food
production
Antimicrobial residuesfromhospitals,pharmaceutical
companies and agriculturecontaminatewater and
spread of resistant bacteriathrough inadequateprovision of water,
sanitation and hygiene
AMR could increase health costsby 25% in low-income countriesand reduce global GDP by 1–4%
annually by 2050Antimicrobial agents are essentialfor human health
Need tobalance access,innovation,conservationto protect
antimicrobialagents to
contain AMR
AMR_brochure.indd 4 27/03/19 10:12 am

5STRENGTHENING COLLABORATION TO PREVENT AND MANAGE ANTIMICROBIAL RESISTANCE
action plans to combat antimicrobial resistance.It sets out the key actions that the various actorsinvolved should take to combat antimicrobialresistance, using an incremental approach over thenext 5–10 years. The TB, HIV, malaria and neglectedtropical diseases antimicrobial resistance work isaligned with the five objectives of the Global ActionPlan:
ÿ to improve awareness and understandingof antimicrobial resistance through eúectivecommunication, education and training;
ÿ to strengthen the knowledge and evidence basethrough surveillance and research;
ÿ to reduce the incidence of infection througheúective sanitation, hygiene and infectionpreventionmeasures;
ÿ to optimize the use of antimicrobial medicines inhuman and animal health; and
ÿ to develop the economic case for sustainableinvestment that takes account of the needs ofall countries and to increase investment in newmedicines, diagnostic tools, vaccines and otherinterventions.
2.5
Ad hoc United Nations Interagency CoordinationGroup on Antimicrobial Resistance
The United Nations Secretary-General hasestablished the United Nations InteragencyCoordination Group on Antimicrobial Resistance(IACG) (7) to improve coordination betweeninternational organizations and to ensureeúective global action against this threat tohealth security. The IACG is co-chaired by theUnited Nations Deputy Secretary-General andtheWHODirector-General and comprises high-level representatives of relevant United Nationsagencies, other international organizations andindividual experts across diúerent sectors. TheIACG’s mandate is to provide practical guidancefor approaches needed to ensure sustained,eúective global action to address antimicrobialresistance; and to report back to the UnitedNations Secretary-General in 2019.WHO hoststhe IACG Secretariat with contributions from theFood and Agriculture Organization of the UnitedNations (FAO) andWorld Organisation for AnimalHealth (OIE). WHO is responsible for addressing
antimicrobial resistance in relation to human healthincluding TB, HIV, malaria and relevant neglectedtropical diseases. The longstanding FAO/OIE/WHOTripartite Collaboration on Antimicrobial Resistancewas further strengthened through the signatureof a memorandum of understanding inMay 2018.The Tripartite agencies and the United NationsEnvironment Programme (UNEP) are activelyworking together to support a global multisectoralresponse to antimicrobial resistance, includingimplementing the IACG recommendations workingwithMember States, civil society and the privatesector.
2.6
WHO 13th General Programme of Work(2019–2023)
TheWHO 13th General Programme ofWorkfor 2019–2023 (8) is structured around threeinterconnected strategic priorities to ensure healthylives and well-being for all at all ages. The goals are:
ÿ 1 billion people benefiting from universal healthcoverage;
ÿ 1 billion more people better protected fromhealth emergencies; and
ÿ 1 billion more people enjoying better health andwell-being.
Addressing antimicrobial resistance will contributeto all three goals. The 13th General ProgrammeofWork provides the framework for positioningcommunicable diseases eúorts in support ofuniversal health coverage. Both ending theepidemics of high-impact communicablediseases (HIV, TB, malaria and neglected tropicaldiseases, Fig. 2–5) and preventing andmanagingantimicrobial resistance are priorities in the 13thGeneral Programme ofWork and need to beaddressed horizontally across all relevantWHOprogrammes at all levels of the Organization.The 13th General Programme ofWork ImpactFramework has specific targets for TB, HIV, malariaand neglected tropical diseases; a target to increasethe detection and treatment rates for rifampicin-resistant TB (includingmultidrug-resistant TB (MDR-TB) or combined resistance to at least rifampicin andisoniazid) to 80% by 2023, and targets to reduce theprevalence of resistant bloodstream infections and
AMR_brochure.indd 5 27/03/19 10:12 am

6 TUBERCULOSIS , HIV, MALARIA AND NEGLECTED TROPICAL DISEASES
improve the proportion of people with access toantibiotics.
2.7
TB, HIV, malaria, neglected tropical diseases andantimicrobial resistance
Antimicrobial resistance has long posed challengesfor managing TB, HIV, malaria and some neglectedtropical diseases. Drug-resistant TB is a public healthcrisis and a health security threat; drug resistancein HIV is a growing challenge and threatensprogress to end the epidemic as a public healththreat by 2030. In the past, widespread resistanceto chloroquine and other drugs led tomalariaresurgence and continuing epidemics in manycountries and areas. As a consequence of havingto address antimicrobial resistance challenges formany years, TB, HIV, malaria and neglected tropicaldisease programmes have refined their drugresistancemanagement and control strategies to
reflect reality on the ground and lessons learned.Unfortunately, strategies for managing andcontrolling drug resistance related to these diseaseshave sometimes been implemented separately inthe context of each individual disease programmeand not under the overall umbrella of antimicrobialresistance. Elements that underpin many of thedisease-specific interventions to prevent, detect andmanage drug resistance also apply to non-disease-specific antimicrobial resistancemanagementprogrammes. Better integrating TB, HIV, malariaand neglected tropical disease drug resistanceprogrammes into other antimicrobial resistanceeúorts would help to strengthen the overallresponse to antimicrobial resistance andmaximizesynergy in such areas as surveillance, laboratorystrengthening, monitoring and evaluation,procurement and supply chain management,developing human resource capacity and thequality of health services delivered.
FIG. 2
Estimated TB incidence rates by country, 2017
Source: Global tuberculosis report 2018 (5).
Incidence per 100 000population per year
0–24
25–99
100–199
200–299
≥300
No data
Not applicable
AMR_brochure.indd 6 27/03/19 10:12 am

7STRENGTHENING COLLABORATION TO PREVENT AND MANAGE ANTIMICROBIAL RESISTANCE
FIG. 3
HIV prevalence among people 15–49 years old by country, 2017
FIG. 4
Number of malaria cases by country, 2017
Source: World Health Organization, Global Malaria Programme, 2018.
Estimated casesper 1000 population
0–0.1
0.2–1
2–10
11–50
51–100
>100
Non-endemic or no ongoing malaria transmission
Not applicable
Source: WHO Global Health Observatory data repository (http://apps.who.int/gho/data/node.main.622?lang=en), last updated 17 July 2018.
<0.2%
0.2–0.5%
0.6–1.5%
>1.5%
No data
Not applicable
AMR_brochure.indd 7 27/03/19 10:12 am

8 TUBERCULOSIS , HIV, MALARIA AND NEGLECTED TROPICAL DISEASES
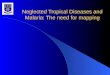
FIG. 5
Number of people requiring treatment and care for neglected tropical diseases by country, 2017
Source: World Health Organization, Department of Control of Neglected Tropical Diseases, 2019.
0–10
11–100
101–1 000
1 001–10 000
10 001–100 000
100 001–1 million
1 000 001–10 million
10 000 001–100 million
>100 million
AMR_brochure.indd 8 27/03/19 10:12 am

9STRENGTHENING COLLABORATION TO PREVENT AND MANAGE ANTIMICROBIAL RESISTANCE
3. Current antimicrobial resistance status:TB, HIV, malaria and relevant neglectedtropical diseases
KEY MESSAGESÿ TB drug resistance is a major cause of antimicrobial resistance mortality andmorbidityworldwide, and immediate action is required to prevent the further development and spreadof resistance.
ÿ Resistance of HIV to efavirenz and nevirapine, the most common first-line drugs, is acurrent global health threat leading to poor health outcomes such as treatment failure,mortality and increased programme costs and requires urgent action to be taken now toprevent the further development and spread of resistance.
ÿ Malaria drug resistance constitutes a challenge particularly in the Greater Mekongsubregion. Drug resistance has developed to artemisinin and some partner drugs used inartemisinin-based combination therapies, making treatment of people with Plasmodiumfalciparummalaria diûcult. The risk of importing or developing resistance in themalaria-endemic countries in the rest of the world is a concern, and surveillance of drug eûcacy is ahigh priority.
ÿ Some drug resistance has been identified in neglected tropical diseases caused by bacteria(leprosy and yaws) and a parasite (visceral leishmaniasis). The resistance observed has beenat low levels and does not apply to all available treatments. Drug resistance has not yet beenobserved in helminths that primarily infect humans.
ÿ Antimicrobial resistance is also a phenomenon in other pathogens (such as non-specificbacteria and fungi) that may cause secondary infection in people with TB and HIV. Risingdrug resistance levels in bacteria causing common acute infections in humans have been welldocumented, undermining the ability to treat these infections.
3.1
Factors driving antimicrobial resistance acrossdisease areas
Antimicrobial resistance occurs when drugs(antibiotics, antifungal agents, antiviral agents,antimalarial agents and anthelmintic agents)used to treat infections by microorganisms suchas bacteria (TB, leprosy and non-specific bacteria),fungi, viruses (HIV) and parasites (malaria, soil-transmitted helminths and trematodes) kill mostof the organisms, but sometimes not all, leavinga small subset of resistant microorganisms thatsurvive. The surviving populations can then
multiply, allowing infections to persist in the body,potentially leading to increasedmorbidity andmortality and increasing the risk of transmitting theresistant organisms to other people. Non-targetedorganisms are also aúected and can be exposedto antimicrobial residues in the environmentfrom hospitals, pharmaceutical production andagricultural activities. Genes for antimicrobialresistance can be transferred between bacteria inthe environment (such as from non-pathogenicspecies to pathogenic species). Antimicrobialresistance in populations of microorganisms isselected over time based on exposure to specificdrugs. Themisuse and overuse of antimicrobial
AMR_brochure.indd 9 27/03/19 10:12 am

10 TUBERCULOSIS , HIV, MALARIA AND NEGLECTED TROPICAL DISEASES
agents accelerate this process (2).Leading causes of antimicrobial resistance
related to these diseases include:
ÿ poor treatment practices, such as treatmentinterruption because of failure to adhere toprescribed treatment; stock-outs or interruptedaccess to key drugs; use of monotherapies orsubstandardmedicines; unregulated or informaluse of drugs without prescriptions; lack ofeúective drugs; use of inappropriate drugsto treat illnesses (such as artemisinin-basedcombination therapy to treat non-malarialfebrile illnesses and antibiotics to treat viralinfections); and non-optimal use of antibiotics(such as inadequate regimens or eúectivemonotherapy to treat TB);
ÿ failure to identify drug-resistant pathogens,resulting in ineúective treatment and delayedswitch tomore eúective drugs and the potentialspread of the resistant pathogens; and
ÿ inadequate disease prevention interventions,including poor infection control practices.
3.2
Tuberculosis
The TB bacteria can develop resistance to one,two or more antimicrobial drugs used to cure thedisease, leading to rifampicin-resistant TB (RR-TB),multidrug-resistant TB (MDR-TB) or extensivelydrug-resistant TB (XDR-TB). Extensively drug-resistant TB has been reported in 127 countries.MDR-TB is a public health crisis and global healthsecurity threat (5).
In 2017, MDR-TB or RR-TB caused 558 000 newcases (3.5% of new cases and 18% of previouslytreated cases) and 230 000 deaths (Fig. 6). Only25% of the estimatedMDR-TB cases (139 114)were treated, of which 55% that started treatmentcompleted it or were cured (5) (Fig. 6).
Three countries accounted for almost half of theworld’s cases of multidrug-resistant or rifampicin-resistant TB: India (24%), China (13%) and theRussian Federation (10%). Globally, 3.5% of newTB cases and 18% of previously treated cases hadmultidrug-resistant or rifampicin-resistant TB (Fig. 7and 8). The highest proportions (>50% in previouslytreated cases) are in countries of the former USSR.
Among cases of multidrug-resistant TB in 2017, anestimated 8.5% had extensively drug-resistant TB(5).
Multidrug-resistant TB is increasing as aproportion of all TB cases in some countries witha high burden of TB, with the burden eitherincreasing faster or decreasingmore slowly than theoverall TB burden (5).
FIG. 6
Drug-resistant TB treatment cascade
Source: Global tuberculosis report 2018 (5).
558 000ssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssss
Estimated newmultidrug-resistant orrifampicin-resistant TB cases in 2017
161 000ssssssssssssssss
Newmultidrug-resistant or rifampicin-resistant TB cases detected in 2017
139 000ssssssssssssss
People starting treatment formultidrug-resistant TB in 2017
55%Treatment success for people startingtreatment for multidrug-resistant or
rifampicin-resistant TB in 2015
AMR_brochure.indd 10 27/03/19 10:12 am

11STRENGTHENING COLLABORATION TO PREVENT AND MANAGE ANTIMICROBIAL RESISTANCE
FIG. 7
Percentage of new TB cases with multidrug-resistant or rifampicin-resistant TBa
a Figures are based on the most recent year for which data have been reported, which varies among countries. Data cover the period 2002–2018.Source: Global tuberculosis report 2018 (5).
a Figures are based on the most recent year for which data have been reported, which varies among countries. Data cover the period 2005–2018. The high percentagesof previously treated TB cases with RR-TB in Belize, Guam and Sao Tome and Principe refer to only a small number of notified cases
(range: 1–8 notified previously treated TB cases). Source: Global tuberculosis report 2018 (5).
FIG. 8
Percentage of previously treated TB cases with multidrug-resistant or rifampicin-resistant TB
Percentageof cases
0–5.9
6–11
12–29
30–49
≥50
No data
Not applicable
Percentageof cases
0–2.9
3–5.9
6–11
12–17
≥18
No data
Not applicable
AMR_brochure.indd 11 27/03/19 10:12 am

12 TUBERCULOSIS , HIV, MALARIA AND NEGLECTED TROPICAL DISEASES
3.3
HIV
HIV drug resistance is caused by a change(mutation) in the genetic structure of HIV thataúects the ability of a specific drug or combinationof drugs to block the replication of the virus. Allcurrent antiretroviral drugs are at risk of becomingpartly or fully inactive because of the emergenceof resistant virus. HIV drug resistance jeopardizesthe success of HIV treatment and endangers theattainment of the global targets to end the AIDSepidemic as a public health threat. The emergenceof HIV drug resistance threatens the success of the“treat all” approach for HIV because resistance ismore likely to lead to illness and potentially death(6).
HIV drug resistance is increasing across allWHO regions, with the yearly increases greatest ineastern and southern Africa (Fig. 9). Pretreatmentresistance to themost commonly used first-line
drugs (efavirenz and nevirapine) has reached thelevel of 10%1 or greater among people initiatingHIV treatment in many low- andmiddle-incomecountries assessed (6).
Women are at great risk of carrying a virus withpretreatment resistance, posing a challenge toeliminating themother-to-child transmission ofHIV and tomaternal and child health outcomes;about 50% of children newly diagnosed with HIVare infected with a virus resistant to commonly usedfirst-line drugs (6).
Modelling has predicted that, if resistance to themost common first-line drugs exceeds 10% amongpeople starting HIV therapy in sub-Saharan Africa,in 15 years pretreatment drug resistance could beresponsible for cumulatively 16% of deaths fromAIDS-related causes (890 000 deaths), 9% of the
1 WHO guidelines on HIV drug resistance recommend thatcountries with levels of pretreatment resistance to efavirenzor nevirapine at or above 10% urgently consider using otherHIV drugs in first-line regimens.
FIG. 9
Increasing levels of pretreatment resistance to efavirenz and nevirapine, the most commonly used drugs infirst-line HIV treatment
Source: HIV drug resistance report 2017 (11).
Southern Africa Western and central Africa Eastern Africa
Asia Latin America
1996 2000 2004 2008 2012 2016 1996 2000 2004 2008 2012 2016 1996 2000 2004 2008 2012 2016
1996 2000 2004 2008 2012 2016 1996 2000 2004 2008 2012 2016
Studies: 60 Patients: 11 855P-value for association: <0.00001
Studies: 51 Patients: 4 924P-value for association: 0.002
Studies: 50 Patients: 7 169P-value for association: <0.00001
Studies: 89 Patients: 16 088P-value for association: 0.01
Studies: 83 Patients: 16 008P-value for association: <0.00001
20
15
10
5
0
20
15
10
5
0
Prevalence
ofNNRTIresistance(%)
Prevalence
ofNNRTIresistance(%)
20
15
10
5
0
20
15
10
5
0
Prevalence
ofNNRTIresistance(%)
Prevalence
ofNNRTIresistance(%)
20
15
10
5
0
Prevalence
ofNNRTIresistance(%)
Fitted line
AMR_brochure.indd 12 27/03/19 10:12 am

13STRENGTHENING COLLABORATION TO PREVENT AND MANAGE ANTIMICROBIAL RESISTANCE
people acquiring HIV infection (450 000 people)and a programme cost of US$ 6.5 billion in sub-Saharan Africa (Fig. 10). Several low- andmiddle-income countries are currently transitioning to newregimens in first-line treatment to which resistanceis expected to be low (6).
Drug resistancemay also be a challenge in someof the opportunistic infections that aúect peoplewith HIV, such as TB, cryptococcal meningitis (9),sexually transmitted infections and candidiasis (10).
3.4
Malaria
Malaria is caused primarily by the Plasmodiumfalciparum and P. vivax parasites. Artemisinin-based combination therapy (ACT) is used to treatP. falciparum and chloroquine-resistant strains ofP. vivax. Chloroquine- or ACTs, complemented withprimaquine, are recommended for treating P. vivaxin areas with chloroquine-susceptible infections (12).
The scale-up of ACTs has been integral tothe recent success of global malaria eúorts andprotecting their eûcacy in treatingmalaria is aglobal health priority. The eûcacy of artemisinin-
based combination therapy is threatened bythe emergence of both artemisinin and partnerdrug resistance. Partner drug resistance can ariseindependently of artemisinin partial resistance.Partner drug resistance with or without artemisininpartial resistance increases the risk of treatmentfailure, and association of artemisinin resistance willworsen the treatment failure rate (12).
Artemisinin partial resistance is currently limitedto five countries of the Greater Mekong subregion:Cambodia, the Lao People’s Democratic Republic,Myanmar, Thailand and Viet Nam (Fig. 11) andis suspected in Guyana, Papua NewGuinea andRwanda. Artemisinin partial resistance has notbeen confirmed in Africa; multi-drug resistance2 ispresent in Cambodia, the Lao People’s DemocraticRepublic, Thailand and Viet Nam (12).
P. vivax resistance is geographically widespread,but in many countries the parasite is still susceptibleto chloroquine, especially when primaquineis taken concurrently. P. vivax resistance to
2 Multidrug-resistant malaria is defined as resistance to morethan two antimalarial compounds of diúerent chemicalclasses. This term usually refers to P. falciparum resistanceto chloroquine, sulfadoxine-pyrimethamine and a thirdantimalarial compound.
FIG. 10
Predicted impact of HIV drug resistance in sub-Saharan Africa if levels of resistance to efavirenz andnevirapine, the most commonly used drugs in first-line HIV treatment, reach or exceed 10%
Source: Global action plan on HIV drug resistance 2017–2021 (6).
PROJECTED IMPACT IN SUB-SAHARAN AFRICAWHERE PPRETREATMENT HIV DRUG RESISTANCE ≥10%
2016–2021 2016–2030 2016–2021 2016–2030
2016–2021 2016–2030 FIRST LINE SECOND LINE THIRD LINE
NEWHIV INFECTIONS AIDS DEATHS
148 000
TREATMENT COST IN US$
450 000 150 000 890 000
$750million $6500 million $85 $1235$263
Cumulative cost Annual cost per person (2016)
AMR_brochure.indd 13 27/03/19 10:12 am

14 TUBERCULOSIS , HIV, MALARIA AND NEGLECTED TROPICAL DISEASES
artemisinin-based combination therapy has notbeen documented and thus artemisinin-basedcombination therapy can be used where there isextensive chloroquine resistance (12).
WHO recommends that countries change theirfirst-line treatments for P. falciparum and P. vivaxwhen treatment failure rates exceed 10% (12).
3.5
Neglected tropical diseases
Neglected tropical diseases (13) are a diverse groupof 20 diúerent diseases that mostly aúect low-income andmarginalized populations. For manyneglected tropical diseases, the risk of developing
resistance to treatment is considered low becauseof the nature of the diseases (such as parasites withrelatively long life cycles) or because no treatmentsare available to become resistant to (such asdengue, rabies, etc). Some drug resistance has beenidentified for neglected tropical diseases caused bybacteria – such as leprosy and yaws – and a parasite:visceral leishmaniasis. The resistance observedhas been at low levels and does not apply to allavailable treatments. Drug resistance has not yetbeen observed for helminths that primarily infecthumans.
Antibiotic resistance to at least one of the threeantibiotics used to treat leprosy has been detectedin 19 countries. Eight per cent of the bacteria wereresistant to at least one commonly used antibiotic.Resistance to two diúerent antibiotics wasidentified in 24 cases. Drug resistance was observedin 12 countries among 5.1% of relapses and 2.0%of new cases. Three countries (Brazil, Colombiaand India) reportedmore than five resistant cases.The numbers of resistant cases are still low, and nobacterial strain has yet shown resistance to all threeantibiotics simultaneously (14).
Drug resistance has been reported to some first-line medicines used to treat yaws (15) and visceralleishmaniasis (16).
The strategies for preventing and treatingtrachoma and yaws call for mass administration ofthe antibiotic azithromycin to populations at risk(17,18). This intervention can lead to increases indrug resistance related to non-targeted potentiallypathogenic bacteria (such as Streptococcuspneumoniae). Care is therefore required to plan themass drug administration tominimize the potentialfor increasing drug resistance related to non-targeted bacteria (19).
Anthelmintic resistance is not yet a public healthproblem in human helminthiasis, where mass drugadministration is a recommended intervention(schistosomiasis, onchocerciasis, lymphatic filariasisand soil-transmitted helminthiasis), but resistance isproblematic in helminths of veterinary importance,indicating that resistance could develop (20).
FIG. 11
Number of artemisinin-based combinationtherapies failing in the Greater Mekong Subregiona
a Countries are classified by numbers of ACTs failing (>10% treatment failure)after 2010. Source: World malaria report 2018 (12).
AMR_brochure.indd 14 27/03/19 10:12 am

15STRENGTHENING COLLABORATION TO PREVENT AND MANAGE ANTIMICROBIAL RESISTANCE
4. Preventing antimicrobial resistance relatedto TB, HIV, malaria and neglected tropicaldiseases and theWHO response
KEY MESSAGESÿ Achieving universal health coverage and strengthening health systems are key factors forpreventing antimicrobial resistance across all diseases and service delivery areas.
ÿ For TB, HIV, malaria and neglected tropical diseases, antimicrobial resistance often can bepredicted, prevented, managed and controlled bymaintaining focus on it and developingand implementing the right strategies.
ÿ Drug resistance is often amarker of poor-quality treatment service delivery, andidentifying and addressing quality gaps is important for preventing resistance.
ÿ Surveillance, laboratory strengthening and expansion of laboratory services, enhanceddata collection and use and better communication, awareness-raising, education andtraining are key components of all strategies for preventing andmanaging antimicrobialresistance and could be expanded to synergistically address antimicrobial resistance across alldisease and service delivery areas.
ÿ Addressing infectious diseases and antimicrobial resistance within the context of universalhealth coverage in amore integrated way oúers opportunities for eûciency and betteroutcomes.
4.1
Preventing antimicrobial resistance
Preventing drug resistance is a critical componentof any national communicable disease programmeand is achieved by optimizing service deliveryand eliminating programmatic gaps in diseaseprevention, treatment and care. WHO regularlyupdates its guidelines to optimize servicedelivery to prevent and treat TB, HIV, malariaand neglected tropical diseases. General diseaseprevention reduces both the overall diseaseburden and the transmission of sensitive andresistant pathogens – thus aúecting the spreadof antimicrobial resistance. WHO also producesspecific guidance for managing drug-resistantinfections. These include: policy recommendationson the overall public health response required;clinical and programmatic guidance on selectingthemost appropriate interventions and treatment
regimens, including diagnostic and drug resistancetesting; managing programmes and rationallyusingmedicines; and possible recommendationson restricting access to drugs by prescription orusing combination therapies. WHO policy andrecommendations are informed by programmaticdata on access to and use of preventive measures,resistance surveillance and eûcacy data and areroutinely updated on the prevention, diagnosisand treatment of TB, HIV, malaria and neglectedtropical diseases. WHO also produces guidance onother interventions and supporting programmes tobetter manage antimicrobial resistance in general,such as preventing and controlling infections inclinical settings, water, sanitation and hygiene inclinical settings, procurement and supply chainmanagement, prequalification of drugs and otherareas. Table 1 highlights examples ofWHO activitiesto identify, prevent andmanage antimicrobialresistance.
AMR_brochure.indd 15 27/03/19 10:12 am

16 TUBERCULOSIS , HIV, MALARIA AND NEGLECTED TROPICAL DISEASES
Preventing antimicrobial resistance also requiresstrengthening health systems to provide theneeded products and services to people at the timethey are required: for example, including critical,quality-assuredmedicines on lists of essentialmedicines; ensuring functioning supply chainsthat deliver the requiredmedicines to health-carefacilities; preventing stock-outs and treatmentdisruption; and ensuring that clinical personnelhave the necessary tools (such as treatmentalgorithms) to enable them to eúectively identifyand treat a wide range of illnesses with theappropriate drugs. For example, expanded useof malaria rapid diagnostic tests does not alwayslead to the right treatment outcome. Artemisinin-based combination therapy is sometimes stillgiven to patients with negative tests or antibioticsare provided to treat fever without confirmationthat bacteria are the cause (21). This leads topotential misuse and overuse of artemisinin-basedcombination therapy or antibiotics and increasedrisk of drug-resistant malaria parasites or non-specific bacteria. For chronic diseases such as HIV,resistance can be prevented by national and clinic-based strategies that support optimal adherence totreatment and retention in care.
4.2
Surveillance of antimicrobial resistance
Surveillance involves collecting, analysing andinterpreting epidemiological data on antimicrobialresistance. Data can be collected from surveys thatcover selected populations or at the individual levelfrom routine data provided by health facilities andlaboratories. Surveillance is critically importantfor monitoring trends and developing evidence-informed policies and interventions to prevent andmanage antimicrobial resistance.
In the past decades, WHO has helped toestablish global, regional and country-levelsurveillance systems tomonitor drug resistance andtherapeutic eûcacy trends in TB, HIV, malaria andneglected tropical diseases (Boxes 1–4). Overall,WHO supports drug resistance and therapeuticeûcacy surveillance activities in nearly all aúectedcountries: 160 countries for multidrug-resistantTB, 69 countries for HIV drug resistance and 64countries for malaria, representingmost of the
world’s population andmost of the burden of high-impact communicable diseases. Drug resistancestatus and trends for these diseases are routinelypublished in disease-specific reports and in peer-reviewed publications.
To support the second strategic objective ofthe Global Action Plan on Antimicrobial Resistanceto strengthen the knowledge and evidence basethrough surveillance and research, WHO launchedthe Global Antimicrobial Resistance SurveillanceSystem (GLASS) in October 2015 and startedcountry enrolment inMarch 2016. GLASS fosters thedevelopment of national antimicrobial resistancesurveillance systems and provides a standardizedapproach to collecting, analysing and sharingantimicrobial resistance data for bacteria causingcommon acute infections. To date, 72 countriesparticipate in GLASS (22).
As a core function of disease-specificprogrammes, WHO surveillance activities include:
ÿ developing standardizedmethods and toolsfor antimicrobial resistance surveillance, datacollection and analysis;
ÿ routinely collecting, quality assuring, analysingand disseminating surveillance data on drugresistance and therapeutic eûcacy andresistance trends at the global, regional andnational levels;
ÿ using surveillance data to informWHOguidelines and national treatment policies;
ÿ providing guidance on appropriate programmeindicators associated with and predictive ofresistance to be included in health informationsystems;
ÿ providing a framework for early detection andreporting of emerging antimicrobial resistance;
ÿ building global data repositories, countrydatabases and portals to support countries instoring, quality assuring and disseminating theirdata in a timely fashion; and
ÿ providing technical support to countries indesigning and conducting drug resistanceand therapeutic eûcacy studies and surveysand in collecting, quality assuring, analysing,interpreting and disseminating their data.
AMR_brochure.indd 16 27/03/19 10:12 am

17STRENGTHENING COLLABORATION TO PREVENT AND MANAGE ANTIMICROBIAL RESISTANCE
TABLE1
Pathog
enresistan
ce,resistancemon
itoringan
dWHOactivities
Pathogen
Status
ofresistance
a
Resistance
monito
ring
WHOactivities
toidentify,preventand
managedrug
resistance
Epidem
iologicalm
ethods
forpopulation-levelm
onito
ring
andsurveillanceofdrug
resistance
Laboratorymethods
for
resistance
detection
Literature
review
Nationally
andregionally
representative
surveys
Collection
anduseof
routinedrug
resistance
data
Therapeutic
eþcacy
studiesa
tsentinel
sites
(parasite
clearance)
Cultu
re
Molecular
methods
(gene
probes,
sequencing)
Global
monito
ring
and
reporting
Standardized
protocolsa
ndtoolsfordrug
resistance
surveillance,
datacollection,
analysisand
interpertatio
nGlobal
database
Global
laboratory
networks
with
WHO
designation
Technical
assistance
forcountries
toimplem
ent
drug
resistance
surveysa
ndstudies
Early
warning
indicators
fordrug
resistance
emergence
HIV
XX
XX
XX
XX
Mycob
acteriu
mtube
rculosis(TB)
XX
XX
XX
XX
XX
Plasmod
ium
(malaria)
XX
XX
XX
XX
Mycob
acteriu
mleprae
orleprom
atosis
(leprosy)
XX
X
Trep
onem
apa
llidu
m(yaw
s)b
X
Leish
man
iado
nova
ni(visceralleishmaniasis)
X
Chlamyd
iatracho
matis
(trachoma)
bX
XX
X
Helminths(soil-trans-
mitted
helminthiasis)
cX
XX
Xd
Xd
Helminths
(schistosomes)c
XX
Xd
Xd
aGreen
=nodocu
men
tedresistan
ce;o
range=drugresistan
cedocu
men
tedbutnotwidespread
orremainsregionallyco
nfined
;red
=drugresistan
ceas
curren
tglobal
hea
lththreat.
bInterven
tionsrequiremassdrugad
ministrationwiththesamean
tibioticaz
ithromycin;m
assuse
has
ledto
drugresistan
cein
yawsbac
teriaan
dother
pathogen
icbac
teriabutnottrac
homabac
teria.
cAnthelminthicdrugresistan
cehas
bee
nobserved
inhelminthsthat
infect
domestican
imalsbutnotye
tin
strainsthat
primarily
infect
human
s.dUnder
dev
elopmen
t.
HIV
AMR_brochure.indd 17 27/03/19 10:12 am

18 TUBERCULOSIS , HIV, MALARIA AND NEGLECTED TROPICAL DISEASES
BOX 1
Surveillance of resistance to TB
Established in 1994, the global surveillance system for TB drug resistance remains the oldest andlargest initiative on antimicrobial resistance surveillance in the world (Fig. 12). TB Surveillance dataare being collected either (1) through continuous surveillance systems based on routine testing ofeveryone with TB in countries with extensive laboratory capacity or (2) through periodic surveys,which are discrete studies measuring drug resistance among a selected sample of people who arerepresentative of an entire population of people with TB in countries with insuûcient laboratorycapacity for routine drug susceptibility testing of everyone with TB.
Standardizedmethods allow comparability of data within countries over time and between countries.Surveillance data on TB drug resistance are collected annually through a web-based data collectiontool that gathers notification data on everyone with TB worldwide. On average, 15 country surveysare conducted every year. Newmolecular technologies, including whole-genome sequencingtechnologies, have recently been incorporated into drug resistance surveys. Since 1994, data on drugresistance have been systematically collected and analysed from 165 countries (82% of the 194WHOMember States), which collectively represent more than 97% of the world’s population and TB cases(23,24).
FIG. 12
Global coverage of surveillance data on TB drug resistance
Source: Global tuberculosis report 2018 (5).
Year of mostrecent data
1995–1999
2000–2004
2005–2009
2010–2014
2015–2018
Ongoing in 2018
Subnational data
No data
Not applicable
AMR_brochure.indd 18 27/03/19 10:12 am

19STRENGTHENING COLLABORATION TO PREVENT AND MANAGE ANTIMICROBIAL RESISTANCE
BOX 2
Surveillance of HIV drug resistance
The emergence and transmission of some level of HIV drug resistance is inevitable, even whenappropriate regimens are prescribed and adherence to treatment is optimal. To address this challenge,WHO developed a global strategy for the surveillance andmonitoring of HIV drug resistance in 2004and updated it in 2015. The strategy includes four key activities: (1) annual monitoring of quality-of-care indicators of HIV drug resistance at all antiretroviral therapy clinics in a country; (2) surveillance ofpretreatment HIV drug resistance among adults initiating first-line antiretroviral therapy;(3) surveillance of acquired HIV drug resistance in adults and children receiving treatment; and(4) surveillance of HIV drug resistance among children younger than 18months newly diagnosed withHIV.
Survey data were generated from sentinel clinics from 2004 to 2014, but since 2014, nationallyrepresentative HIV drug resistancemethods have been recommended. The data generated fromthe HIV drug resistance surveys are representative of the entire population of individuals with HIVinitiating HIV treatment or receiving HIV treatment, respectively.
Since 2004, data from 271 surveys in 69 countries have been collected using standardizedepidemiological and laboratory methods, allowing comparability of data within countries over timeand across countries (Fig. 13).
The survey results have been used to inform policies and treatment guidelines at the national andglobal levels.
Quality assurance and dissemination of HIV drug resistance data are core activities ofWHO.Surveillance data for HIV drug resistance are entered and safely stored in theWHO global HIV drugresistance database, which has three main purposes: (1) supporting countries and genotypinglaboratories in the quality assurance of epidemiological and sequence data for the purpose ofgenerating high-quality country reports; (2) providing standardized resistance interpretations bylinking to themost recent algorithm for interpreting HIV drug resistance; and (3) providing countrieswith a long-term secure repository for their HIV drug resistance data (25,26).
A global network ofWHO-designated laboratories for HIV drug resistance supports the global eúortby producing reliable and quality-assured genotypic data.
AMR_brochure.indd 19 27/03/19 10:12 am

20 TUBERCULOSIS , HIV, MALARIA AND NEGLECTED TROPICAL DISEASES
BOX 3
Surveillance of antimalarial drug eÿcacy
WHO set up surveillance of antimalarial drug eûcacy in 1996 with the development of a standardprotocol to monitor antimalarial eûcacy through therapeutic eûcacy studies in collaboration withthe United States Centers for Disease Control and Prevention. The protocol was first implemented inareas with highmalaria transmission rates, mainly in Africa. Later the standard protocol was updatedtwice to include countries with low tomoderate malaria transmission rates. WHO has developeda series of tools (including in vitro tests, molecular analysis andmeasuring drug concentrations) tobetter define and detect drug resistance among treatment failures. The use of these standardizedprocedures facilitates the comparison of results within and across regions over time.WHO organizestraining at the regional and country levels on drug eûcacy monitoring and continually supportsregional networks on drug eûcacy (27).
WHO set up a global database in response to the challenges posed by the emergence of resistanceto antimalarial drugs. The contents of the database are extracted from published and unpublishedtherapeutic eûcacy studies and surveys of molecular markers on antimalarial drug resistanceconducted by partners at the country level. The database is the source forWHO’s onlineMalariaThreats Map, theWorld malaria report and update reports on antimalarial drug eûcacy and drugresistance.
WHO has provided support in creating subregional networks for monitoring antimalarial resistance.TheMekong network, the Red Amazónica para la Vigilancia de la Resistencia a las DrogasAntimaláricas (RAVREDRA) network, the Pacific network, the BBINS (Bangladesh, Bhutan, India, þ
FIG. 13
Global coverage of WHO-recommended surveillance surveys on HIV drug resistance
Source: Global Action Plan on HIV Drug Resistance 2017–2021: 2018 progress report (26).
2004–2013
2014–2017
2017–2018
Planned
No data
Not applicable
Year of most recent survey
AMR_brochure.indd 20 27/03/19 10:12 am

21STRENGTHENING COLLABORATION TO PREVENT AND MANAGE ANTIMICROBIAL RESISTANCE
þ Nepal, Sri Lanka) network, the Horn of Africa Network for Monitoring Antimalarial Treatment(HANMAT) and PIAMNET (Pakistan, Islamic Republic of Iran and Afghanistanmonitoring network)have successfully increased drug eûcacy surveillance in the regions and generated the data neededfor updating national treatment policies. Through these networks, WHO has oúered training forimplementing protocols, microscopy, analysing and validating data and preparing reports andpublications, which in turn improved the quality of the data.
BOX 4
Therapeutic eÿcacy testing for selected neglected tropical diseases
Threats of growing drug resistance related to some neglected tropical diseases has ledWHO to call formonitoring drug eûcacy and resistance at selected sentinel sites. TheWHO Strategic and TechnicalAdvisory Group on Neglected Tropical Diseases has created a subgroup to support themonitoring ofdrug resistance in neglected tropical diseases. WHO has developed standard protocols for monitoringthe eûcacy of the anthelminthic drugs used in preventive chemotherapy. Research is currentlyongoing to develop appropriate combinations of anthelminthics to prevent or respond to theemergence of resistance. Countries have been encouraged to use theWHO-recommended protocolsto monitor the local situation. TheWorking Group onMonitoring Neglected Tropical Diseases DrugEûcacy is working to establish a network of laboratories with experience evaluating anthelminthicdrug eûcacy and to developmore sensitive methods to measure anthelminthic eûcacy.
4.3
Laboratory networks
For TB, HIV, malaria and neglected tropical diseases,drug resistance cannot yet be directly detectedat the point of care. Samples (sputum, blood andfaeces) are collected from patients and analysed inlaboratories. In some cases, organisms are culturedand tested for resistance, or molecular methods(gene probes or sequencing) are used to detectresistance genes. For malaria and some neglectedtropical diseases (soil-transmitted helminths andtrematodes), therapeutic eûcacy tests are usedto screen for treatment failure, which may berelated to drug resistance. Support to strengthenand expand laboratory services is often needed todetect drug resistance (Box 5).
WHO’s role has been to support thedevelopment and expansion of national, regionalor specialized reference laboratories that monitorTB and HIV drug resistance (Fig. 14 and 15). WHOactivities include:
ÿ developing standardized drug resistance testingprotocols, assay validation, standard operating
procedures, tools and quality standards forinternal and external quality assurance;
ÿ undertaking quality assurance of resistance dataand therapeutic eûcacy testing data to ensureaccurate and reliable laboratory results and tofacilitate the comparison of data over time andacross countries;
ÿ designating specialized, regional and nationalreference laboratories that support resistancetesting for surveillance and diagnostic purposesfrom countries with limited or no testingcapacity;
ÿ identifying opportunities for eûcientlyintegrating drug resistance and therapeuticeûcacy monitoring into broader nationalantimicrobial resistance and laboratorystrengthening strategies and plans, includingusing shared health systems and laboratoryplatforms; and
ÿ training laboratory workers, facilitating South–South collaboration across laboratories andstrengthening laboratory capacity to detect andreport on drug resistance at the country andregional levels.
AMR_brochure.indd 21 27/03/19 10:12 am

22 TUBERCULOSIS , HIV, MALARIA AND NEGLECTED TROPICAL DISEASES
FIG. 14
WHO TB Supranational Reference Laboratory Network
Source: WHO TB Supranational Reference Laboratory Network [website] (24).
Supranational Reference Laboratory – Coordinating Centre
Supranational Reference Laboratory
National Centre of Excellence
Milan, ItalyRome, Italy
Santiago, Chile
Antwerp, Belgium
Atlanta, USA
Mexico City,Mexico
Guadeloupe, France
Buenos Aires, ArgentinaAdelaide, Australia
Brisbane, Australia
Bangkok, Thailand
Hong Kong SAR, China
Seoul, Republic of Korea
Tokyo, Japan
Chennai,India
Karachi,Pakistan
Delhi, IndiaCairo,Egypt
Johannesburg,South Africa
Kampala,Uganda
Cotonou,Benin
Le Hamma,Algeria
Porto, PortugalBarcelona, Spain
London, UK
Gauting, GermanyBorstel, Germany
Copenhagen, DenmarkStockholm, Sweden
Riga, Latvia
Zagreb, CroatiaPrague, Czech Republic
Moscow, Russian Federation
Yekaterinburg, Russian Federation
Novosibirsk, Russian Federation
FIG. 15
HIV Drug Resistance Laboratory Network as of July 2018
Source: Global Action Plan on HIV Drug Resistance 2017–2021: 2018 progress report (26).
WHO-designated national laboratory for HIV drug resistance testing
WHO-designated regional laboratory for HIV drug resistance testing
WHO-designated specialized laboratory for HIV drug resistance testing
WHO-designated laboratory for HIV drug resistance testing using dried blood spot
Laboratory with capacity for HIV drug resistance testing of integrase inhibitors
Kampala
Addis AbabaDakar
Johannesburg
Kisumu
Mexico City
Atlanta
Fort de France
Ponce
Rio de Janeiro (x2)
VancouverWinnipeg
Bordeaux
London
Montpellier
Utrecht
Bangkok (x2)Chennai
Pune
Beijing
Hanoi
Ho Chi Minh City
Shanghai
Shenyang
Sydney
AbidjanEntebbe
AMR_brochure.indd 22 27/03/19 10:12 am

23STRENGTHENING COLLABORATION TO PREVENT AND MANAGE ANTIMICROBIAL RESISTANCE
BOX 5
Laboratory networks for TB, HIV and neglected tropical diseases
WHO established a global TB drug resistance surveillance programme in 1994, supported by anetwork of global TB supranational reference laboratories. As of December 2018, 155 countriesparticipated in the TB drug resistance surveillance programme, coveringmore than 95% of theworld’s population and TB cases. The network of supranational reference laboratories includes 36laboratories overseeing the drug resistance surveillance programme throughmore than 100 nationalTB reference laboratories (24).
A global HIV drug resistance laboratory network was established in 2005 to support HIV drugresistance surveillance activities. As of July 2018,WHO had designated 30 laboratories in five ofWHO’s six regions (Africa, the Americas, Europe, South-East Asia and theWestern Pacific) to conductHIV drug resistance testing for public health surveillance (26).
The first steps to establish a global neglected tropical disease drug resistance laboratory networkwere taken in February 2019: theWorking Group onMonitoring Neglected Tropical Diseases DrugEûcacy met to define the terms of reference of the networks and the characteristics, capacity andgeographical distribution of the laboratories that will be part of the network.
4.4
Communication, awareness-raising, educationand training
The first strategic objective of the Global ActionPlan on Antimicrobial Resistance is to improveawareness and understanding of antimicrobialresistance through eúective communication,education and training. As highlighted in Section3, antimicrobial resistance threatens sustainabledevelopment and is a major risk to ending the HIV,TB andmalaria epidemics. It is therefore criticallyimportant to maintain the issue of drug resistanceon the global and national development agendas.
WHO is working to improve awareness andunderstanding of drug resistance in countries,with diúerent audiences, as part of long-standingprogrammes in TB, HIV, malaria and neglectedtropical diseases. Ongoing activities include:
ÿ conveningMember States, civil society,researchers, implementing partners, donors,developers of drugs and diagnostics andother stakeholders to increase awareness andunderstanding around the status and impact ofresistance;
ÿ engaging and convening experts (throughstrategic and technical advisory groups,technical expert groups, global working groupsetc.) to ensure timely and appropriate responsesto elevated levels of resistance when they arise;
ÿ compiling, interpreting and disseminatinginformation and data on drug resistance tocountries and development partners andsupporting the strengthening of their situationanalyses;
ÿ using data generated by surveillance to informpolicy and recommendations;
ÿ providing regular updates about drug resistancetrends toMember States throughmeetings ofWHOGoverning Bodies and urging countries totake action;
ÿ using international days mandated by theWorldHealth Assembly (such asWorld TuberculosisDay, WorldMalaria Day, World AIDS DayandWorld Antibiotic AwarenessWeek) toraise awareness about the challenge of drugresistance;
ÿ supporting knowledge transfer, training andcapacity development ofWHO regional andcountry oûces as well as national diseaseprogrammes on prevention and clinical andprogrammatic management of drug-resistantTB, HIV, malaria and neglected tropical diseases;
AMR_brochure.indd 23 27/03/19 10:12 am

24 TUBERCULOSIS , HIV, MALARIA AND NEGLECTED TROPICAL DISEASES
ÿ engagingmanufacturers of diagnostics, drugsandmedical devices in dialogue to ensure thatkey medicines are aúordable and that drugs thatcontribute to antimicrobial resistance are takenoú the market (such as malaria monotherapies);
ÿ involving civil society and engaging communitiesin improving literacy on resistance and treatmentadherence;
ÿ engaging all relevant health-care providers indisease treatment, care and control throughpublic–private mix approaches; and
ÿ supporting countries in developing andimplementing comprehensive national actionplans to address antimicrobial resistance thatinclude TB, HIV, malaria and neglected tropicaldiseases where relevant.
AMR_brochure.indd 24 27/03/19 10:12 am

25STRENGTHENING COLLABORATION TO PREVENT AND MANAGE ANTIMICROBIAL RESISTANCE
5. Future directions
KEY MESSAGESÿ Addressing antimicrobial resistance is part of the agendas of universal health coverage,patient safety and the quality of health-care services.
ÿ Innovation and research in treatment and diagnostics will play key roles in reducing thedevelopment and spread of drug resistance related to TB, HIV, malaria and neglected tropicaldiseases and its risk to health.
ÿ Product development partnerships have demonstrated eúectiveness in identifying andfacilitating the development of new pipeline drugs for TB, malaria and neglected tropicaldiseases as drug resistance to current therapies spreads.
ÿ Sets of clinical and programmatic quality-of-care indicators that predict and are associatedwith developing drug resistance have been identified andmonitored for HIV. Similarapproaches might be explored to predict the emergence of resistance related to otherdiseases or at health-care delivery points, enabling early action to prevent andminimize thespread of antimicrobial resistance.
ÿ Antimicrobial resistance related to bacteria, TB, HIV, malaria and neglected tropicaldiseases is a critical issue and needs to be kept high on the global, regional and nationalhealth development agendas.
ÿ WHO has a key role to play in compiling and disseminating information on levels ofresistance and trends as well as innovative practices to prevent, manage and control thedevelopment and spread of antimicrobial resistance related to TB, HIV, malaria, bacteria,fungi and neglected tropical diseases.
ÿ WHO, working collaboratively with other development partners, will provide joint supportto countries in developing, implementing and tracking progress against comprehensive,evidence-informed national antimicrobial resistance action plans that include TB, HIV, malariaand neglected tropical diseases where relevant.
ÿ WHOwill work with countries to identify andmaximize synergy across programmesor service delivery areas and platforms to address TB, HIV, malaria and neglected tropicaldiseases antimicrobial resistance.
AMR_brochure.indd 25 27/03/19 10:12 am

26 TUBERCULOSIS , HIV, MALARIA AND NEGLECTED TROPICAL DISEASES
5.1
Identify research and development gaps and newtools and approaches
New products, technologies and service deliveryapproaches will be needed to address antimicrobialresistance related to TB, HIV, malaria, neglectedtropical diseases and across the whole spectrum ofantimicrobial resistance. Research and developmentwill play an important role in preventing andmanaging antimicrobial resistance.
WHO has a clear leadership role to play inidentifying prevention andmanagement gaps inantimicrobial resistance related to TB, HIV, malariaand neglected tropical diseases, which can includethe need for new products and approaches toservice delivery. WHO’s role includes:
ÿ monitoring antimicrobial resistance prevalenceand trends to assess needs and gaps;
ÿ identifying and setting global, regional andnational research agendas and priorities forantimicrobial resistance;
ÿ convening institutions and expert networks toaddress antimicrobial resistance gaps, includingcollaborative eúorts to identify antimicrobialresistancemanagement needs in the animalhealth and agricultural sectors (such as throughthe FAO/OIE/WHO Tripartite Collaboration onAntimicrobial Resistance and UNEP) and howthis aúects human health;
ÿ compiling and disseminating good practicesin preventing andmanaging antimicrobialresistance to facilitate changes in approaches toservice delivery to address gaps in service qualityand eúectiveness;
ÿ supporting countries in conductingimplementation research across a variety ofsettings and populations to improve approachesto service delivery (such as improving treatmentadherence, preventing drug stock-outs,
identifying drug resistance and optimizingtreatment protocols in the face of increasingresistance) or address other factors that leadto the emergence and spread of antimicrobialresistance;
ÿ assessing the burden of disease caused byantimicrobial resistance; and
ÿ advocating for increased research anddevelopment investment to strengthen productpipelines that address aspects of antimicrobialresistance.
To prevent andmanage drug resistance relatedto TB, HIV, malaria and neglected tropical disease,WHO can:
ÿ identify and advocate for the developmentof better andmore aúordable tools, suchas vaccines, eúective drugs with shorter orsimplified treatment protocols, point-of-usediagnostic tests, gene sequencing andmolecularmethods for surveillance of drug resistance;
ÿ recommendmodels of service delivery thatimprove the quality and follow-up of keyinterventions that influence antimicrobialresistance, such as treatment adherence,diagnostic testing and appropriate response,algorithms to ensure eúective treatmentand infection control to minimize diseasetransmission in hospital settings;
ÿ collaborate to further address antimicrobialresistance in the animal husbandry andagricultural sectors;
ÿ engage with product development partnerships,the private sector and other partners toadvocate for developing new drug candidates(Box 6) or diagnostics and other products (Box 7);and
ÿ support countries in rapidly adopting innovativepractices or new products to prevent or manageantimicrobial resistance for maximum impact.
AMR_brochure.indd 26 27/03/19 10:12 am

27STRENGTHENING COLLABORATION TO PREVENT AND MANAGE ANTIMICROBIAL RESISTANCE
BOX 6
Product development partnerships to identify and develop new candidate drugs
TheMedicines for Malaria Venture (MMV) and Drugs for Neglected Diseases initiative (DNDi) areproduct development partnerships that have identified and developed an innovative model todevelop new pipeline drugs to treat malaria and neglected diseases. These partnerships provide asystematic way for partners to work together to identify and develop newmedicines and/or betterformulations to increase the pipeline of available drugs to treat malaria and neglected tropicaldiseases. These partnerships facilitate the development of drugs that pharmaceutical companies maybe reluctant to pursue by themselves because of economic considerations.
Since it was created in 1999, MMV has built an extensive network of over 400 pharmaceutical,academic and endemic-country partners in more than 55 countries and has developed and broughtforward 10 newmedicines to treat malaria (28). Increasing the pipeline of available malaria drugs willhelp to mitigate the impact if current resistance to artemisinin-based combination therapy becomeswidespread. The product development partnership model has also been used to address drugresistance related to other diseases.
The Global Antibiotic Research and Development Partnership was established inMay 2016 as a jointinitiative byWHO and the DNDi. This not-for-profit research and development initiative addressesglobal public health needs by developing and delivering new or improved antibiotic treatments whileendeavouring to ensure sustainable access. It also harnessesWHO’s mandate to drive the globalresponse to antimicrobial resistance and set health priorities and DNDi’s expertise in maximizingpartnerships to build a pipeline for neglected diseases and deliver not-for-profit, needs-drivenresearch and development. Various partners and donors are contributing to this collaborative eúort.
In 2010, theWHODepartment of Control of Neglected Tropical Diseases established theWorkingGroup onMonitoring Neglected Tropical Diseases Drug Eûcacy to promote the testing of newanthelminthic drugs or combinations of existing drugs. The group identified several potential drugcandidates. ThreeWHO collaborating centres are participating in this working group.
BOX 7
Role of development partners in the response to antimicrobial resistance
In recent years, the work to respond to antimicrobial resistance has benefited from investment bytechnical agencies, donor initiatives and the private sector.
Unitaid, the United States Agency for International Development (USAID) and the Bill &MelindaGates Foundation have supported trials and other studies of newmedicines and novel regimensfor multidrug-resistant TB (such as the EndTB project coordinated by Partners in Health, MédecinsSans Frontières and Interactive Research and Development in Pakistan; the Global Alliance for TBDrug Development; and the STREAM trial of a shorter nine-monthmultidrug-resistant TB regimen).The initiatives of manufacturers of diagnostics (such as HAIN for line probe assay and CEPHEID forGeneXpert) andmedications (such as bedaquiline by Janssen and delamanid by Otsuka) have alsobeen critical to improvemultidrug-resistant TB care.
Unitaid has made critical contributions to support national TB laboratory networks to consolidatetheir work and implement new diagnostics for drug-resistant TB (EXPAND-TB project) and improveaccess to new TBmedicines. þ
AMR_brochure.indd 27 27/03/19 10:12 am

28 TUBERCULOSIS , HIV, MALARIA AND NEGLECTED TROPICAL DISEASES
þ For HIV, the Bill &Melinda Gates Foundation has supported the establishment of theWHOGlobalStrategy for the Surveillance andMonitoring of HIV Drug Resistance and the Global Action Plan onHIV Drug Resistance; the Global Fund to Fight AIDS, Tuberculosis andMalaria and the United StatesPresident’s Emergency Plan for AIDS Relief (PEPFAR) have supported countries in implementingnational HIV drug resistance surveys and in strengthening laboratory capacity for HIV drug resistancetesting. The United States Centers for Disease Control and Prevention has provided technicalassistance to PEPFAR-supported countries in activities related to surveillance of HIV drug resistance.The United States National Institutes of Health provide in-kind support to the quality assurance of theglobal HIV drug resistance laboratory network. Over the years, some specializedWHO-designatedHIV drug resistance laboratories (such as the University of British Columbia (Vancouver, Canada),Public Health Agency of Canada (Winnipeg, Canada); Center for Research in Infectious Diseases(CIENI, Mexico City, Mexico), United States Centers for Disease Control and Prevention/Global ActionPlan on Antimicrobial Resistance (Atlanta, USA) have provided HIV drug resistance testing free ofcharge to support HIV drug resistance surveillance in several low- andmiddle-income countrieswith limited financial and technical capacity. Other partners, including the Public Health Agency ofCanada, have contributed to diúerent aspects of HIV drug resistancemonitoring and surveillanceeúorts. HIVResNet, a large network of institutions and experts, has provided strategic guidance toWHO over the years and contributed to the global eúorts to monitor, respond to and prevent HIVdrug resistance. Unitaid is funding clinical trials for emerging antiretroviral medicines and supportstreatment monitoring to facilitate treatment optimization, including for children.
Partners have also played a key role in the work to develop newmalaria treatments, in supportingthe surveillance of the eûcacy of existing antimalarial drugs, and in the eúorts to contain resistanceand eliminate malaria in the Greater Mekong Subregion. The Bill &Melinda Gates Foundation,the Australian Department of Foreign Aúairs and Trade, the United KingdomDepartment forInternational Development, the Global Fund to Fight AIDS, Tuberculosis andMalaria and USAIDprovide essential support to the surveillance of eûcacy. The Global Fund to Fight AIDS, TuberculosisandMalaria is the main funder of the work to eliminate P. falciparummalaria in the Greater Mekongsubregion and thereby minimize the risk of future spread of drug-resistant parasites from this area.
Unitaid is also fundingmalaria projects to improve diagnostics and prevention for pregnant women.
The Bill &Melinda Gates Foundation and USAID have provided financial support for neglectedtropical diseases, identifying alternative anthelminthics and establishing a network of laboratorieswhile technical support was provided by three collaborating centres in Basel, Switzerland, Ghent,Belgium and Negrar, Italy and byMcGill University, the University of Texas, the University of Londonand Universidad de Valencia.
5.2
Clinical and programmatic indicators associatedwith and predicting the emergence ofantimicrobial resistance
Evidence from HIV programmes has shown thatit is possible to identify andmonitor a set ofprogrammatic quality-of-care indicators thatprovide an early warning for the emergence of drugresistance in certain populations or settings (see
Box 8 and Table 2). Monitoring this set of indicatorscan help to predict where resistancemay emerge,enabling corrective actions to be taken to preventthe emergence and subsequent spread of drugresistance (29). For several diseases (such as TB, HIVand leprosy) drug resistance is more likely to ariseamong people who have been previously treatedand stopped treatment or experienced treatmentfailure. This should prompt the use of a diúerentdrug combination for subsequent treatment
AMR_brochure.indd 28 27/03/19 10:12 am

29STRENGTHENING COLLABORATION TO PREVENT AND MANAGE ANTIMICROBIAL RESISTANCE
regimens in accordance withWHO treatmentguidelines. For neglected tropical diseases,the emergence of parasite resistance to someanthelminthics used to treat infections in livestocksignals that human pathogenic helminth strainsalso need to bemonitored for resistance, especiallygiven the scale of themass drug administration
approaches used to treat these parasites in humans.Future work across disease areas might help
to identify common sets of service delivery and/or quality-of-care indicators that can be routinelymonitored to prevent the emergence and spread ofdrug resistance.
BOX 8
Quality-of-care indicators associated with and predicting the emergence ofHIV drug resistance
Monitoring a subset of quality of care indicators – also known as early warning indicators of HIV drugresistance – is a key component of theWHO public health strategy to prevent HIV drug resistancein countries scaling up antiretroviral therapy. These quality-of-care indicators specifically assessfactors at individual antiretroviral therapy clinics associated with and predicting the emergence ofHIV drug resistance. Monitoring these quality-of-care indicators is designed to provide countrieswith actionable information to improve clinical and programmatic performance to prevent HIV drugresistance from emerging.
Many factors are associated with the emergence of HIV drug resistance. They include viral factors(such as subtype, replication capacity and pre-existing polymorphisms); drug-related factors (suchas drug potency, pharmacokinetics, drug–drug interactions, drug tolerability and genetic barriers toselecting resistance) and programme factors (such as patient adherence, drug stock-outs and supplycontinuity and retention in treatment). Although viral and drug-related factors are often beyondthe control of public health or programme action, monitoring the clinical or programmatic factorsassociated with HIV drug resistance can alert antiretroviral therapy programmes to situations thatmay favour the emergence of HIV drug resistance or failure to suppress viral load at the populationlevel.
This set of quality-of-care indicators monitors factors related to patient care (appropriate prescribingand viral load suppression at 12months); patient behaviour (adherence); and clinic-level andprogrammemanagement (follow-up, retention on antiretroviral therapy, procurement and supplymanagement of antiretroviral drugs and appropriately switching regimen among people with failureto suppress viral load).
Early warning indicators use internationally agreed standardized definitions and accompanyingtargets. Annual monitoring of early warning indicators enables the degrees of improvement ordecline over time to bemeasured, both within and between clinics
AMR_brochure.indd 29 27/03/19 10:12 am
(29).

30 TUBERCULOSIS , HIV, MALARIA AND NEGLECTED TROPICAL DISEASES
5.3
Joint support for countries
The Global Action Plan on Antimicrobial Resistanceoutlines a framework for action on antimicrobialresistance with supporting countries to develop,implement andmonitor antimicrobial resistancenational action plans as a priority. The OneHealth concept requires a perspective that coversantimicrobial resistance across all key components,including human health, animal health andagriculture because preventing andmanagingantimicrobial resistance requires activities across allrelevant sectors. As of January 2019, 117 countrieshad national action plans, but the extent to whichTB, HIV, malaria and neglected tropical diseaseprogrammes are involved varies. WHO and other
TABLE 2
WHO-recommended early warning indicators of HIV drug resistance and their respective targets
WHO-recommended early warning indicators of HIV drug resistance
Target (green: goodperformance; amber: fairperformance; red: poor
performance)
Retention on antiretroviral therapy at 12months (ART.5, antiretroviral therapyretention)% of patients retained on antiretroviral therapy 12months after initiatingantiretroviral therapy
Green: >85%
Amber: 75–85%
Red: <75%
On-time pill pick-up (ART.7, antiretroviral therapy adherence proxy)% of people who pick up antiretroviral therapy nomore than two days late at the firstdrug pick-up after a defined baseline pick-up
Green: >90%
Amber: 80–90%
Red: <80%
Pharmacy stock-outa (not collectable through the HIV patient monitoring system)% of months with any days of stock-out of any routinely dispensed antiretroviral drug
Green: 0%
Red: >0%
Viral load suppressionb (VLS.1, viral load suppression at 12months)% of people with viral load <1000 copies/mL 12months after initiating antiretroviraltherapy
Green: ≥90%
Amber: 80–<90%
Red: <80%
Viral load completionc (VLS.2, viral load testing coverage)% of people with a 12-month viral load test result available
Green: ≥70%
Red: <70%
a Stock-out refers to lack of availability of first-line antiretroviral drugs.b The denominator for the viral load suppression indicator is the number of people alive and receiving antiretroviral therapy 12 months afterinitiating treatment who have a viral load test result available.
c The denominator for the viral load completion indicator is the number of people alive and receiving antiretroviral therapy 12 months afterinitiating treatment, who are therefore, consistent with the policy, expected to have a viral load test result available in the primary medicalrecord. For all early warning indicators, a grey classification is applied in situations where a sampled antiretroviral therapy clinic is unable toreport on a specific indicator because more than 30% of the data are missing.
development partners need to collaborate betterandmakemore eúort in providing joint support tocountries to develop comprehensive national actionplans that include interventions to address TB, HIV,malaria and neglected tropical diseases whererelevant. Countries need coordinated supportin collecting and using data on antimicrobialresistance (national and subnational) for evidence-informed decision-making. Technical supportshould also target drug regulatory authorities toensure that new eúective medicines and otherrelevant products (such as diagnostic tests thatdetect drug resistance) are added to national listsof essential medicines and that treatment policiesare changed as soon as possible if antimicrobialresistance is reducing the eúectiveness of existingtreatment protocols.
AMR_brochure.indd 30 27/03/19 10:12 am
Source: WHO Consolidated guidelines on person-centred HIV patient monitoring and case surveillance (29).

31STRENGTHENING COLLABORATION TO PREVENT AND MANAGE ANTIMICROBIAL RESISTANCE
5.4
Identifying and optimizing synergy
As countries move to strengthen their primaryhealth care systems and towards achieving universalhealth coverage in the context of reduced relianceon external funding resources, they will need tolook for opportunities to increase the eûciencyof health services and reachmore people withessential services. For antimicrobial resistance,this might mean using diagnostic platforms thatcan detect drug-resistant strains of pathogens forseveral diseases and strengthening and expandingthe services oúered by laboratories to detect drugresistance. Synergy can also be found by traininghealth-care providers to prevent andmanageantimicrobial resistance across multiple diseasesand at various service delivery points, provide bettertreatment by using adapted treatment algorithmsand undertake infection control and preventioninterventions. Strengthening procurement andsupply chain management systems to reduce drugstock-outs is also an important intervention forpreventing antimicrobial resistance related to TBand HIV and to other diseases as well. Ensuringthat health-care facilities have clean waterand functioning sanitation facilities and thatwastewater is adequately treated before beingdischarged into the environment from health-carefacilities and drugmanufacturing facilities canstrongly reduce antimicrobial resistance.
5.5
Product pipelines
Collaboration is required to identify new drugcandidates. New drugs take a long time to develop,are expensive andmust go through at leastthree phases of clinical trials before they can beapproved for widespread use among humans.Pharmaceutical companies are often unwilling toinvest the time andmoney required to bring newdrugs to market unless they have a high probabilityof achieving adequate returns on investment. Thisis often a challenge for such diseases as TB, HIV,malaria and neglected tropical diseases, whichhave their greatest impact in low- andmiddle-income countries. As highlighted in Box 6, productdevelopment partnerships and other researchconsortiums can facilitate and fundwork to identifynew pipeline drugs.
Further research is also needed to developformulations for children, shorter durationtreatments, treatments with reduced side-eúects,more eúective combinations of existing drugs,lower cost treatments, medicines with greaterstability and long-acting formulations.
Point-of-care diagnostic tests that directlymeasure drug resistance are not currently available.Research and funding are also needed to developnew technologies and products and commondiagnostic platforms that can detect drug resistanceacross multiple diseases.
AMR_brochure.indd 31 27/03/19 10:12 am

32 TUBERCULOSIS , HIV, MALARIA AND NEGLECTED TROPICAL DISEASES
References
1. Adeyi OO, Baris E, Jonas OB, Irwin A, Berthe FCJ, Le Gall FG et al. Drug-resistant infections: a threat toour economic future (Vol. 2). Washington (DC): World Bank; 2017(http://documents.worldbank.org/curated/en/323311493396993758/final-report, accessed4 February 2019).
2. Antimicrobial resistance. Geneva: World Health Organization; 2018(https://www.who.int/en/news-room/fact-sheets/detail/antimicrobial-resistance, accessed4 February 2019).
3. Sustainable Development Goals [website]. New York: United Nations; 2019(https://sustainabledevelopment.un.org/sdgs, accessed 4 February 2019).
4. What is health financing for universal health coverage? [website]. Geneva: World Health Organization;2019 (https://www.who.int/health_financing/universal_coverage_definition/en, accessed4 February 2019).
5. Global tuberculosis report 2018. Geneva: World Health Organization; 2018(https://www.who.int/tb/publications/global_report/en, accessed 4 February 2019).
6. Global action plan on HIV drug resistance 2017–2021. Geneva: World Health Organization; 2017(http://apps.who.int/iris/bitstream/handle/10665/255883/9789241512848-eng.pdf, accessed4 February 2019).
7. United Nations Interagency Coordination Group on Antimicrobial Resistance (IACG) [website]. Geneva:World Health Organization; 2019(https://www.who.int/antimicrobial-resistance/interagency-coordination-group/en, accessed4 February 2019).
8. Thirteenth General Programme ofWork 2019–2023. Geneva: World Health Organization; 2018(https://www.who.int/about/what-we-do/gpw-thirteen-consultation/en, accessed 4 February2019).
9. Mpoza E, Rhein J, Abassi M. Emerging fluconazole resistance: implications for themanagement ofcryptococcal meningitis. MedMycol Case Rep. 2017;19:30–2.
10. Pankhurst CL. Candidiasis (oropharyngeal). BMJ Clin Evid. 2009;2009:1304.11. HIV drug resistance report 2017. Geneva: World Health Organization; 2017
(http://www.who.int/hiv/pub/drugresistance/hivdr-report-2017/en, accessed 4 February 2019).12. World malaria report 2018. Geneva: World Health Organization; 2018
(https://www.who.int/malaria/publications/world-malaria-report-2018/en, accessed 4 February2019).
13. Neglected tropical diseases [website]. Geneva: World Health Organization; 2019(https://www.who.int/neglected_diseases/diseases/en, accessed 4 February 2019).
14. Cambau E, Saunderson P, MatsuokaM, Cole ST, Kai M, Suúys P et al. Antimicrobial resistance in leprosy:results of the first prospective open survey conducted by aWHO surveillance network for the period2009–15. Clin Microbiol Infect. 2018;24:1305–10.
15. Mitjà O, Godornes C, Houinei W, Kapa A, Paru R, Abel H et al. Re-emergence of yaws after single massazithromycin treatment followed by targeted treatment: a longitudinal study. Lancet. 2018;391:1599–1607.
AMR_brochure.indd 32 27/03/19 10:12 am

33STRENGTHENING COLLABORATION TO PREVENT AND MANAGE ANTIMICROBIAL RESISTANCE
16. Ponte-Sucre A, Gamarro F, Dujardin J-C, Barrett MP, Lopez-Vélez R, Garcia-Hernandez R et al. Drugresistance and treatment failure in leishmaniasis: a 21st century challenge. PLoS Negl Trop Dis.2017;11:e0006052.
17. Trachoma fact sheet. Geneva: World Health Organization; 2018(https://www.who.int/en/news-room/fact-sheets/detail/trachoma, accessed 4 February 2019).
18. Yaws fact sheet. Geneva: World Health Organization; 2018(https://www.who.int/news-room/fact-sheets/detail/yaws, accessed 4 February 2019).
19. O’Brien KS, Emerson P, Hooper PJ, Reingold AL, Dennis EG, Keenan JD et al. Antimicrobial resistancefollowingmass azithromycin distribution for trachoma: a systematic review. Lancet Infect Dis.2019;19:e14–e25.
20. Seventhmeeting of theWorking Group onMonitoring of Neglected Tropical Diseases Drug Eûcacy.Geneva: World Health Organization; 2018(https://apps.who.int/iris/bitstream/handle/10665/273620/WHO-CDS-neglected tropicaldisease-PCT-2018.06-eng.pdf, accessed 4 February 2019).
21. Bruxvoort KJ, Leurent B, Chandler CIR, Ansah EK, Baiden F, Björkman A et al. The impact of introducingmalaria rapid diagnostic tests on fever case management: a synthesis of ten studies from the ACTConsortium. Am J TropMed Hyg. 2017;97:1170–9.
22. Global Antimicrobial Resistance Surveillance System (GLASS) [website]. Geneva: World HealthOrganization; 2019 (https://www.who.int/glass/en, accessed 4 February 2019).
23. Tuberculosis: surveillance of drug-resistant TB [website]. Geneva: World Health Organization; 2019(https://www.who.int/tb/areas-of-work/monitoring-evaluation/mdr-tb-surveillance/en,accessed 4 February 2019).
24. WHO TB Supranational Reference Laboratory Network [website]. Geneva: World Health Organization;2010 (available at https://www.who.int/tb/areas-of-work/laboratory/srl-network/en, accessed4 February 2019).
25. HIV drug resistance surveillance guidance: 2015 update. Geneva: World Health Organization; 2015(https://apps.who.int/iris/bitstream/handle/10665/204471/9789241510097_eng.pdf, accessed4 February 2019).
26. Global Action Plan on HIV Drug Resistance 2017–2021: 2018 progress report. Geneva: World HealthOrganization; 2018 (https://www.who.int/hiv/pub/drugresistance/gap-hivdr-progress2018/en,accessed 4 February 2019.
27. Malaria: drug resistance and response [website]. Geneva: World Health Organization; 2019(https://www.who.int/malaria/areas/drug_resistance/en, accessed 4 February 2019).
28. An overview of our work. Geneva: Medicines for Malaria Venture; 2019(https://www.mmv.org/about-us/about-mmv, accessed 4 February 2019).
29. Consolidated guidelines on person-centred HIV patient monitoring and case surveillance. Geneva:World Health Organization; 2017(https://www.who.int/hiv/pub/guidelines/person-centred-hiv-monitoring-guidelines/en,accessed 4 February 2019).
AMR_brochure.indd 33 27/03/19 10:12 am

34 TUBERCULOSIS , HIV, MALARIA AND NEGLECTED TROPICAL DISEASES
WHO antimicrobial resistance resources
Antimicrobial resistance – general
WHO antimicrobial resistance websitehttp://www.who.int/topics/antimicrobial_resistance/en
Global Action Plan on Antimicrobial Resistancehttp://www.who.int/antimicrobial-resistance/publications/global-action-plan/en
Global Framework for Development & Stewardship to Combat Antimicrobial Resistance – Draft roadmaphttp://www.who.int/entity/antimicrobial-resistance/global-action-plan/UpdatedRoadmap-Global-Framework-for-Development-Stewardship-to-combatantimicrobial resistance_2017_11_03.pdf
Global Antimicrobial Resistance Surveillance System: Manual for Early Implementationhttp://www.who.int/antimicrobial-resistance/publications/surveillance-system-manual/en
Worldwide country situation analysis: response to antimicrobial resistancehttp://www.who.int/antimicrobial-resistance/publications/situationanalysis/en
Antimicrobial resistance: global report on surveillance 2014http://www.who.int/antimicrobial-resistance/publications/surveillancereport/en
Global Antimicrobial Resistance Surveillance System –manual for early implementationhttps://www.who.int/antimicrobial-resistance/publications/surveillance-system-manual/en
Global Antimicrobial Resistance Surveillance System (GLASS) report – early implementation 2016–2017https://www.who.int/glass/resources/publications/early-implementation-report/en
TB
Drug-resistant TB:WHOwebsitehttp://www.who.int/tb/areas-of-work/drug-resistant-tb/en
The End TB Strategyhttp://www.who.int/tb/strategy/en
Global tuberculosis report 2018http://www.who.int/tb/publications/global_report/en
WHO treatment guidelines for drug-resistant tuberculosishttp://apps.who.int/iris/bitstream/handle/10665/250125/9789241549639-eng.pdf
Companion handbook to theWHO guidelines for the programmatic management of drug-resistanttuberculosishttp://www.who.int/tb/publications/pmdt_companionhandbook/en
Guidelines for surveillance of drug resistance in tuberculosis – 5th editionhttp://www.who.int/tb/publications/2015/drs_guidelines/en
Compendium ofWHO guidelines and associated standards: ensuring optimum delivery of the cascade ofcare for patients with tuberculosishttp://apps.who.int/iris/bitstream/10665/259180/1/9789241512572-eng.pdf
AMR_brochure.indd 34 27/03/19 10:12 am

35STRENGTHENING COLLABORATION TO PREVENT AND MANAGE ANTIMICROBIAL RESISTANCE
HIV
Global Health Sector Strategy on HIV, 2016–2021http://apps.who.int/iris/bitstream/handle/10665/246178/WHO-HIV-2016.05-eng.pdf
HIV drug resistance: WHOwebsitehttp://www.who.int/hiv/topics/drugresistance/en/
Global Action Plan on HIV Drug Resistance 2017–2021http://apps.who.int/iris/bitstream/handle/10665/255883/9789241512848-eng.pdf
Global Action Plan on HIV Drug Resistance 2017–2021: 2018 progress reporthttps://www.who.int/hiv/pub/drugresistance/gap-hivdr-progress2018/en/
HIV drug resistance surveillance guidancehttp://apps.who.int/iris/bitstream/handle/10665/204471/9789241510097_eng.pdf
Guidelines on the public health response to pretreatment HIV drug resistancehttp://www.who.int/hiv/pub/guidelines/hivdr-guidelines-2017/en
HIV drug resistance report 2017http://www.who.int/hiv/pub/drugresistance/hivdr-report-2017/en
Consolidated guidelines on person-centred HIV patient monitoring and case surveillancehttp://www.who.int/hiv/pub/guidelines/person-centred-hiv-monitoring-guidelines/en
Tackling HIV drug resistance: trends, guidelines and global action.http://apps.who.int/iris/bitstream/handle/10665/255881/WHO-HIV-2017.21-eng.pdf
Malaria
Global technical strategy for malaria 2016–2030http://www.who.int/malaria/publications/atoz/9789241564991/en
Malaria drug resistance: WHOwebsitehttp://www.who.int/malaria/areas/drug_resistance/en
World malaria report 2018https://www.who.int/malaria/publications/world-malaria-report-2018/report/en
WHO status reports on Plasmodium falciparum drug eûcacy and resistancehttp://www.who.int/entity/malaria/areas/drug_resistance/updates/en/index.html
Eliminatingmalaria in the Greater Mekong Subregion: united to end a deadly diseasehttp://www.who.int/entity/malaria/publications/atoz/eliminating-malaria-greater-mekong/en/index.html
Methods for surveillance of antimalarial drug eûcacyhttp://www.who.int/entity/malaria/publications/atoz/9789241597531/en/index.html
Q&A on artemisinin resistancehttp://www.who.int/entity/malaria/publications/atoz/9789241597531/en/index.html
Guidelines for the treatment of malaria. Third editionhttp://www.who.int/malaria/publications/atoz/9789241549127/en
AMR_brochure.indd 35 27/03/19 10:12 am

36 TUBERCULOSIS , HIV, MALARIA AND NEGLECTED TROPICAL DISEASES
Neglected tropical diseases
Neglected tropical diseases: WHOwebsitehttp://www.who.int/neglected_diseases/en
Seventhmeeting of theWorking Group onMonitoring of Neglected Tropical Diseases Drug Eûcacyhttp://apps.who.int/iris/bitstream/handle/10665/273620/WHO-CDS-neglected tropical disease-PCT-2018.06-eng.pdf
AMR_brochure.indd 36 27/03/19 10:12 am



World Health Organization20 Avenue Appia1211 Geneva 27Switzerlandwww.who.int
ISBN 978-92-4-151545-0