Embed Size (px)
Citation preview
TUBERCULOUS LYMPHADINITIS
Prof. Abdul Majeed ChaudhryProf. Abdul Majeed Chaudhry FRCS(E), FRCS(G). FCPS, MHPE(Holland))FRCS(E), FRCS(G). FCPS, MHPE(Holland))
Head of Department of Surgery Head of Department of SurgerySIR GANGA RAM HOSPITAL, LahoreSIR GANGA RAM HOSPITAL, Lahore
LYMPHADENITISLYMPHADENITISLymphadenitis is the inflammation and/or
enlargement of a lymph node as a result of infection acquired of MBT from the draining area or directly as a lymphatogenous infection from a distant tubercle.
The increased size of a node may be caused by the following:
Inflammatory enlargement of the lymph nodesMultiplication of cells within the node,
including lymphocytes, plasma cells, monocytes, or histiocytes and central caseation necrosis
Cervical group of L.N’s is the commonest site among other L.N’s in the body.

LYMPH NODES-LYMPH NODES-Mated togetherMated together

POPULATION AT RISKPOPULATION AT RISK Low socioeconomic group Immunocompromisedi. Diabeticsii. On corticosteroidsiii. HIV
Young and old age group Excessive consumption of milk
and dairy products

EXTRAPULMONARY SITESEXTRAPULMONARY SITESAbdominal TBCervical L.N.Mediastinal L.N.Skeletal (Spine, bones & joints)SkinMeningies Surgical sitesUrogenital TB.Axillary L.N.Inguinal L.N.
MODES OF INFECTIONMODES OF INFECTIONAerosolization of organisms Ingestion of contaminated foodInoculationReactivation of old lesion
MODE OF SPREADMODE OF SPREADLymphatogenousHaematogenousLocal erosion

TONSIL
LYMPHADENOPATHY
TUBERCULAR BACILLI
CLINICAL FEATURESCLINICAL FEATURESLow grade feverAnorexia and weight lossNight sweats and lethargySingle or multiple neck swellings
Feature associated to the primary lesions
Single or multiple neck sinuses

PRESENTATIONPRESENTATIONAcute and chronic lymphadenopathy
Discharging sinusCold and collar stud abscessAs a differential diagnosis of neck masses



DIAGNOSISDIAGNOSISHistory & Clinical ExaminationFBC, ESR, x-Ray Chest & Neck,
PPD (tuberculin skin test) Fine needle aspiration
cytology/Excision biopsyM. tuberculosis (MTB) culture.PCR of blood and lymph node
CYTOLOGYCYTOLOGYThe diagnosis of
T.B.Lymphadenopathy is routinely performed by lymph node cytology or excision biopsy.
-HoweverIt lack specificity due to the
difficulty of distinguishing other granulomatous pathologies in the absence of acid-fast bacilli,
The process of biopsy is invasive

PCRPCRThe PCR is routinely used in
specimen from the site of infection, such as
sputum for pulmonary T.B.cerebrospinal fluid for
tuberculous meningitis, and Lymph node material for
T.B.Lymphadenitis (LN-PCR)
PBMC-PCRPBMC-PCRAn alternative approach is the
detection of M. tuberculosis or M. avium DNA with a PCR in peripheral blood mononuclear cells (PBMC-PCR) of patients with pulmonary TB.
The hypothesis is that patients with active infection harbor mycobacterial DNA in peripheral scavenging cells such as macrophages.
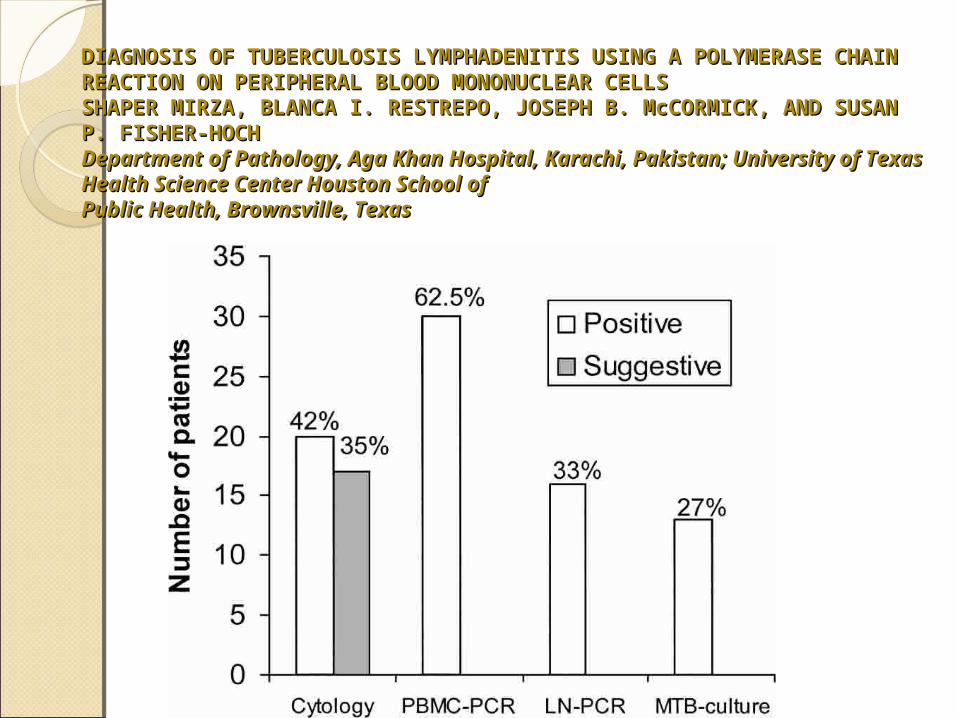
DIAGNOSIS OF TUBERCULOSIS LYMPHADENITIS USING A POLYMERASE DIAGNOSIS OF TUBERCULOSIS LYMPHADENITIS USING A POLYMERASE CHAINCHAINREACTION ON PERIPHERAL BLOOD MONONUCLEAR CELLSREACTION ON PERIPHERAL BLOOD MONONUCLEAR CELLSSHAPER MIRZA, BLANCA I. RESTREPO, JOSEPH B. McCORMICK, AND SHAPER MIRZA, BLANCA I. RESTREPO, JOSEPH B. McCORMICK, AND SUSAN P. FISHER-HOCHSUSAN P. FISHER-HOCHDepartment of Pathology, Aga Khan Hospital, Karachi, Pakistan; Department of Pathology, Aga Khan Hospital, Karachi, Pakistan; University of Texas Health Science Center Houston School ofUniversity of Texas Health Science Center Houston School ofPublic Health, Brownsville, TexasPublic Health, Brownsville, Texas
TUBERCULOUS LYMPHADENITIS: CLINICAL CHARACTERISTICS TUBERCULOUS LYMPHADENITIS: CLINICAL CHARACTERISTICS AND OUTCOME IN A COMMUNITY HOSPITAL AND OUTCOME IN A COMMUNITY HOSPITAL Tapan K. Gayen, MD*, Ravindra Hanumaiah, MD, Vijay Rupanagudi, MD, Tapan K. Gayen, MD*, Ravindra Hanumaiah, MD, Vijay Rupanagudi, MD, Karthikeyan Kanagarajan, MD and Santi Dhar, MD Karthikeyan Kanagarajan, MD and Santi Dhar, MD Coney Island Hospital, Coney Island Hospital, Brooklyn, NY Brooklyn, NY
Foreign born particularly immigrants from Indian subcontinent constituted the predominant patient subgroups with TB lymphadenitis.
Cervical lymphadenopathy constituted predominant lymph node group involved.
PPD was positive in only 60%, while only 8% had sputum growing MTB.
72% of patients had positive lymph node culture for MTB and in others pathology showing caseating granulomas was needed to establish diagnosis.
6 months of treatment was adequate in most of the patients.

TREATMENTTREATMENTHigh protein dietExcision of lesion followed by 9-12 months of
antituberculous chemotherapy.Cold abscess requires repeated aspirations
with chemotherapyVery large and mated lymph nodes may
require neck dissection preserving sternomastoid, accessory nerve and jugular vein if possible followed by chemotherapy.
Chronic sinuses heal spontaneously on anti-tuberculous chemotherapy.
Treatment of primary lesion
CONCLUSIONCONCLUSIONIn our setup patients with subacute to
chronic lymphadenitis , TB should be strongly considered even if PPD is negative and sputum is negative for MTB. Lymph node pathology showing caseating granuloma establishes the diagnosis even if culture is negative.
Uncomplicated tuberculous cervical lymphadenitis resolve completely on effective ATT for appropriate duration.
Disease can be well controlled by better vaccination, public education and consuming pasteurized milk

THANK YOUTHANK YOU