Embed Size (px)
Citation preview

What’s new?
C Immunoglobulin G4-related (IgG4-related) disease is a newly
recognized multi-organ disorder that is associated with tubulo-
TUBULO-INTERSTITIAL DISORDERS
Tubulo-interstitial disordersAdnan Sharif
Simon Ball
interstitial disease
C The renal parenchymal changes associated with IgG4-related
disease are clinico-pathologically characteristic
C The pathogenesis of IgG4-related disease is poorly understood
C Recognition of this rare disorder is important as corticosteroid
therapy is often effective
AbstractChronic kidney disease (CKD) is accompanied by tubulo-interstitial
atrophy and fibrosis, regardless of the underlying cause. Disorders of
the renal vasculature, the glomeruli or urinary drainage all culminate in
chronic tubulo-interstitial damage, the severity of which is the histological
feature that correlates best with progression to end-stage renal failure
(ESRF). However, there are diverse conditions in which the tubulo-
interstitium is the primary site of damage; these may be considered
together without inferring a common aetiology or pathogenesis. The
diseases classified as tubulo-interstitial nephritis are considered in this
article.
Keywords acute renal failure; BK nephropathy; chronic renal failure;
drugs; IgG4-related disease; immune response; infection; interstitial
nephritis
Classification and pathology
Tubulo-interstitial disorders may be classified by their aetiology,
or according to their mode of presentation, into two broad
categories:
� acute interstitial nephritis (AIN)
� chronic interstitial nephritis (CIN).
AIN is characterized by an acute onset, often following a defined
insult (e.g. ingestion of a culprit drug). Tubulo-interstitial
inflammation occurs without significant atrophy or fibrosis1
(Figure 1). Conversely, CIN is characterized by tubulo-
interstitial atrophy and fibrosis, with varying degrees of inflam-
mation. The causes of CIN include direct toxicity, local
ischaemia, inflammation and, rarely, inherited disorders of
tubular proteins (nephronophthisis). Regardless of the cause,
a low-grade monocytic infiltrate may enter areas of atrophy and
fibrosis.2
Adnan Sharif MBChB is a Specialist Registrar in Renal Medicine at
University Hospital Birmingham, UK. He qualified from the University of
Edinburgh and has trained in Edinburgh and Cardiff before
commencing the West Midlands rotation. His special interests are
metabolic disorders post-transplantation and strategies to increase
organ procurement. Competing interests: none declared.
Simon Ball MA PhD FRCP is Consultant Nephrologist at University Hospital
Birmingham, UK. He qualified from Oxford University and University
College London. He trained in nephrology in London and Stevenage.
His main research interests include measuring the immune response to
HLA and blood group antigens. Competing interests: none declared.
MEDICINE 39:8 467
Clinical features
The precise mode of presentation differs between AIN and CIN,
and between different causes, but predominant tubulo-interstitial
damage has some typical effects. Patients often present with
renal impairment, uraemia and fluid overload but, occasionally,
presentation is with extra-renal manifestations such as fever,
skin rash and arthralgia, particularly in AIN.
Albuminuria is common but not large in amount (it may be
below the level of detection of conventional stick urinalysis), and
is generally not associated with the nephrotic syndrome (see
below). Low-molecular-weight proteinuria is common, but
seldom assessed.
Microscopic haematuria is variable and macroscopic haema-
turia uncommon with the exception of certain specific underlying
aetiologies, such as AIN caused by meticillin. In CIN it may
suggest a complicating uro-epithelial malignancy.
There may be defects in tubular handling of water, sodium
and hydrogen ions resulting in nephrogenic diabetes insipidus,
salt-losing nephropathy and renal tubular acidosis (RTA), which
can all lead to the initial presentation. Hypertension is variable.
Acute interstitial nephritis
Drug-induced AIN
AIN causes acute kidney injury (AKI). In the UK, the most
common cause is an idiosyncratic drug reaction; a thorough and
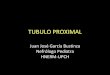
Figure 1 Renal biopsy showing tubulo-interstitial nephritis. Diffuse
monocytic infiltrate (with or without eosinophils) infiltration into tubules
and severe tubular damage. The glomerular structure is preserved with no
evidence of inflammation.
� 2011 Elsevier Ltd. All rights reserved.

Drugs causing tubulo-interstitial nephritis
Antibiotics Non-steroidal
anti-inflammatory
drugs (NSAIDs)
Anticonvulsants Others
Penicillinsa Ibuprofena Phenytoin Allopurinola
Sulphonamidesa Indometacina Sodium
valproate
Cimetidinea
Rifampicina Diclofenac Lamotrigine Phenindionea
Quinolonesa Piroxicama Furosemide
Vancomycin Cox 2 inhibitors Proton pump
inhibitors
Salicylates
a Drugs associated with renal granulomata.
Table 1
TUBULO-INTERSTITIAL DISORDERS
careful drug history including alternative medications is critical
(see Table 1). Patients may present with renal failure, flank pain
or extra-renal manifestations. Macroscopic haematuria is excep-
tional and mainly reported to occur with meticillin. Urinalysis
may reveal blood and protein, but generally not in the amounts
typical of acutely presenting glomerulonephritis. Eosinophilia
may be present, but is variable. Renal ultrasonography and
autoantibody screening are generally normal. The diagnosis is
established by renal biopsy. The drug responsible must be
stopped, and there is evidence that the use of corticosteroids
accelerates and improves recovery.3 Rarely, non-steroidal anti-
inflammatory drugs (NSAIDs) cause a ‘minimal-change’
glomerular lesion in addition to AIN, which presents with
nephrotic syndrome.
Infections causing AIN
Pyelonephritis is an ascending bacterial infection, characterized
by neutrophil inflammation centred on tubules. Tubulo-
interstitial nephritis can complicate various systemic infections
Infections causing tubulo-interstitial nephritis
Virus Bacteria Others
Hantaviridae Legionella Leishmania
Leptospira Toxoplasmaa
EpsteineBarr (EBV)a Mycobacterium
tuberculosisa
HIV Streptococcus
Measles Salmonella
Adenovirus Campylobacter
Immunocompromised Mycoplasma
Polyomavirus Chlamydia
Cytomegalovirus (CMV)
Herpes simplex virus (HSV) Brucella
a Infections associated with renal granulomata.
Table 2
MEDICINE 39:8 468
(see Table 2). Hantavirus causes haemorrhagic fever with renal
syndrome and is an important cause of AIN outside the UK. The
typical presentation is with non-specific systemic symptoms,
followed by acute renal failure (ARF), thrombocytopenia and
elevated hepatic enzymes.
BK virus is a polyomavirus that causes interstitial nephritis in
renal transplant patients.4 It usually presents as acute or
subacute deterioration of transplant function. The main differ-
ential diagnosis is acute rejection, and the main risk factor for BK
nephropathy is the amount of immunosuppression. The diag-
nosis is established by renal biopsy (Figure 2), although urine
cytology for ‘decoy cells’ and quantification of viral DNA in the
plasma by polymerase chain reaction (PCR) provide non-
invasive means of predicting those at risk. The outcome is vari-
able; treatment requires reduction of immunosuppressive load.
The role of antiviral agent remains uncertain. There may be
additional benefit from replacing a standard immunosuppressive
agent with leflunomide or an mammalian target of rapamycin
(mTOR) inhibitor, but clinical trials data are not yet available.
Multi-system inflammatory diseases causing
tubulo-interstitial nephritis
Several non-infectious inflammatory diseases may cause AIN or
CIN. They often respond to corticosteroids.
Sarcoidosis is associated with renal granulomata in about 20%
of patients, but clinically manifest tubulo-interstitial nephritis
(TIN) is less common. More often, hypercalcaemia causes
abnormal renal function. A putative predisposition to glomerular
disease remains unproven.
Sj€ogren’s syndrome is associated with TIN manifest as renal
impairment or renal tubular acidosis.
Systemic lupus erythematosus and Wegener’s granu-
lomatosis, although both typically causes of glomerular lesions,
can present with predominant tubulo-interstitial inflammation.
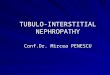
Figure 2 Renal transplant biopsy showing intranuclear basophilic viral
inclusions, chromatin clumping of infected cells and features of interstitial
nephritis.
� 2011 Elsevier Ltd. All rights reserved.

Practice points
C Tubulo-interstitial nephritis has many causes. The diagnosis is
usually made by renal biopsy, but determination of the precise
cause requires careful clinical assessment and the cause
frequently remains obscure
C Urinalysis may show little blood and protein
C Drug-induced acute interstitial nephritis (AIN) is a common
cause of acute renal failure, is an important differential diag-
nosis of acute tubular necrosis (ATN), and should be consid-
ered when recovery of renal function is delayed. (Patients with
ATN are generally in hospital and have commonly received
drugs that can provoke an AIN)
C Chronic interstitial nephritis (CIN) may complicate a recognized
disease or therapy; when this is not the case, there may be
extensive renal damage at presentation because symptoms
occur late
TUBULO-INTERSTITIAL DISORDERS
TIN with uveitis (TINU) is a syndrome in which uveitis gener-
ally coincides with or follows a TIN. TINU commonly presents in
childhood, but has been reported into late adulthood. The
differential diagnosis includes the multi-system diseases above.
IgG4-related disease is characterized by elevated serum
immunoglobulin G4 (IgG4) and renal interstitial infiltration of
IgG4-positive plasma cells. Although often associated with auto-
immune pancreatitis, clinico-pathological data of IgG4-related
disease causing tubulo-interstitial nephritis are emerging.5
Chronic interstitial nephritis
Analgesic nephropathy results from the ingestion of large quantities
of compound analgesics containing phenacetin. The role of non-
phenacetin-containing analgesics is plausible, but unproven. The
typical pathology is centred on the medulla with overlying scarring,
calcification and papillary necrosis. (Papillary necrosis may also
complicate sickle cell nephropathy, which resembles CIN. There is
prominent tubular dysfunction arising from medullary ischaemia.)
Balkan nephropathy and Chinese herbs nephropathy: Balkan
nephropathy is a form of CIN, the cause of which remains unde-
terminedalthough there is increasingevidence that it is related to the
ingestion of food contaminated with aristolochic acid. Environ-
mental andgenetic factors are likely to contribute to its pathogenesis
and eponymous geography. Chinese herbs nephropathy was iden-
tified in 1992 in Belgian women in which the causal agent has been
clearly identified as aristolochic acid contaminating a slimming
agent. In both conditions, there is progressive renal failure, and,
becauseof the substantial risk of uro-epithelialmalignancy, patients
require long-termurological surveillance (see Drugs and toxins that
damage the kidney inMedicine 2011; 39(6): 356e361).
Lithium toxicity: use of lithium as a therapeutic agent may be
complicated by nephrogenic diabetes insipidus, acute tubular
necrosis and, in the long-term, CIN. Development of renal
dysfunction in a patient taking lithium requires careful collabo-
ration between psychiatrist and nephrologist.
Heavy-metal intoxication:CIN fromheavymetal intoxicationmay
arise following environmental or industrial exposure, and perhaps
as a consequence of their presence in traditional medicines.
Radiation nephritis: includes an acute thrombotic micro-
angiopathy and, in the long term, a CIN. It may be ameliorated
by shielding and dose fractionation.
Calcineurin inhibitor toxicity: calcineurin inhibitors often cause
nephrotoxicity with vascular and tubulo-interstitial damage,
which may be ameliorated by dose reduction or withdrawal.
Eating disorders: CIN may develop in patients with eating
disorders. It causes renal impairment, and contributes to the
MEDICINE 39:8 469
complex electrolyte disturbances seen in such individuals. Long-
standing hypovolaemia and hypokalaemia may contribute to its
development although the role of chronic hypokalaemia as
a causative factor is controversial.
Late presenting CIN: many patients presenting with advanced
chronic renal failure and small, unscarred kidneys exhibit
evidence of predominant tubulo-interstitial non-glomerular
damage. This presentation is particularly common in the Indo-
Asian population, but no cause has been identified.6
Idiosyncratic drug reactions, infections and multi-system
inflammatory disorders may all present as a CIN rather than an
AIN. A
REFERENCES
1 Praga M, Gonzalez E. Acute interstitial nephritis. Kidney Int 2010 Jun;
77: 956e61.
2 Nangaku M, Fujita T. Chronic interstitial nephropathy. In: Feehally J,
Floege J, Johnson R, eds. Comprehensive clinical nephrology. 3rd edn.
Mosby, 2007.
3 Gonzalez E, Gutierrez E, Galeano C, et al. Early steroid treatment
improves the recovery of renal function in patients with drug-induced
acute interstitial nephritis. Kidney Int 2008 Apr; 73: 940e6.
4 Dall A, Hariharan S. BK virus nephritis after renal transplantation. Clin J
Am Soc Nephrol 2008 Mar; 3: S68e75.
5 Saeki T, Nishi S, Imai N, et al. Clinicopathological characteristics of
patients with IgG4-related tubulointerstitial nephritis. Kidney Int 2010
Nov; 78: 1016e23.
6 Ball S, Lloyd J, Cattell V, et al. Why is there so much end stage renal
failure of undetermined cause in the Indo-Asian population? Q J Med
2001; 94: 187e93.
� 2011 Elsevier Ltd. All rights reserved.