Embed Size (px)
Citation preview

1
Annual Members’ Meeting
Tuesday, 23rd September 2014 Between 1.00pm - 4.00pm
In the Nowgen Centre, Manchester Royal Infirmary
PRESENT: Executive Directors, Non-Executive Directors and Directors Lady Rhona Bradley – Non-Executive Director, Kathy Cowell – Non-Executive Director, Sir Michael Deegan – Chief Executive, Ursula Denton – Director of Financial Strategy, Cheryl Lenney – Director of Nursing (Adults), Anthony Leon - Deputy Chairman/Non-Executive Director, Anthony Middleton – Director of Performance, Peter Mount – Chairman, Steve Mycio – Non-Executive Director, Margot Johnson – Executive Director of Human & Corporate Resources, Professor Robert Pearson – Medical Director and Brenda Smith – Senior Independent Director/Non-Executive Director. Trust Secretary Alwyn Hughes – Director of Corporate Services/Trust Secretary

2
Council of Governors Ivy Ashworth-Crees – Public Governor (Greater Manchester), Bashir Chaudhry – New Public Governor (Manchester), David Edwards – Public Governor (Greater Manchester), Peter Gomm – Staff Governor (Non-Clinical & Support), Sharon Green – Staff Governor (Nursing & Midwifery), Angela Harrington – Re-appointed Nominated Governor (Manchester City Council), Beverley Hopcutt – Staff Governor (Other Clinical), Richard Jenkins – Public Governor (Rest of England & Wales), Professor Henry Kitchener - New Nominated Governor (Manchester University), Councillor Paul Lally – New Nominated Governor (Trafford Borough Council), Mary Marsden – Staff Governor (Nursing & Midwifery), Keith Paver – Lead & Public Governor (Manchester), Andrew Peel – Public Governor (Manchester), Sue Rowlands – Public Governor (Manchester), Carol Shacklady – New Public Governor (Greater Manchester), Geraldine Thompson – New Staff Governor (Other Clinical), Graham Watkins – New Nominated Governor (Volunteer Services) and Abebaw Yohannes – New Public Governor (Manchester). Members A total of 200 Public/Staff Members and members of the public attended. Notes Prepared By: Donna Beddows – Foundation Trust Membership Manager Apologies: Rabnawaz Akbar – Re-appointed Nominated Governor (Manchester City Council), Jayne Bessant – Re-elected Public Governor (Manchester), Isobel Bridges – Staff Governor (Non-Clinical & Support), Julia Bridgewater – Chief Operating Officer, Julie Cheetham – Nominated Governor (Central Manchester Clinical Commissioning Group), Professor Malcolm Chiswick – Public Governor (Trafford), Professor Rod Coombs – Non-Executive Director, George Devlin – Public Governor (Trafford), Peter Dodd – Public Governor (Manchester), Matthew Finnegan – Public Governor (Trafford), Michael Gregory – Nominated Governor (Trafford Clinical Commissioning Group), Gill Heaton – Deputy Chief Executive/Chief Nurse, Ariful Islam – Nominated Governor (Youth Forum), Alan Jackson – Public Governor (Rest of England & Wales), Patrick McGuinness – New Public Governor (Manchester), Dr Stephan Meyer – New Nominated Governor (Manchester University), Adrian Roberts - Executive Director of Finance, Mr John Vincent Smyth – Staff Governor (Medical & Dental), Barrie Warren – Public Governor (Greater Manchester) and Susan Webster – Re-elected Public Governor (Manchester).

3
WELCOME AND INTRODUCTION – PETER MOUNT, CHAIRMAN Presentation Slides Speaker’s Narrative
Peter Mount, Chairman opened the Annual Members’ Meeting by welcoming and thanking all present for attending. Just before we begin our Annual Members’ meeting, I’d like to share with you a short film clip. It illustrates just how passionately we all believe in working together to give the best possible care to all our patients. http://vimeo.com/110774391 - click link to view film clip
It’s good to see so many of your here today, and a very warm welcome to all our staff and public members. We’re very pleased to have staff side representatives here today, and thank them for their ongoing support in ensuring our hospitals are a great place to work. Welcome also to our Governors who will be hosting a question and answer session for members following closure of this formal presentation part of the meeting. I hope you’ve had chance to look at the very interesting information stands that our Trust teams and many of the partners we work with have put together. They highlight some of the excellent work going on in partnership to ensure patients and their families have access to safe, high quality care. Our thanks to them for their contribution. I'd also like to thank you on your behalf our fundraising team and all the many individuals, families and organisations who have contributed to our Trust Charity. We raised over £4.8 million last year, to support treatment, care and research across our hospitals and community services.

4
As a Trust, we are very proud to play a key role in delivering excellent NHS services to more than a million people each year. My colleagues will be speaking today about some of the major highlights of the past year.
• Chief Executive, Sir Michael Deegan will cover key achievements in 2013/14
• Director of Financial Strategy, Ursula Denton will tell you about our financial position
• Lead Governor, Dr Keith Paver will update you on Membership matters and the results of our recent Governor elections.
• Chief Executive, Sir Michael Deegan will look ahead over the next 12 months and then the floor will then be open for questions to our Board of Directors.
I would like to extend congratulations to our Chief Executive on behalf of all our staff, patients and members. He received a knighthood in the Queen’s Birthday Honours list in June, for services to the NHS. He will visit Buckingham Palace later this year to formally become Sir Michael Deegan – a fitting recognition of what he has achieved during his career in healthcare and particularly at this Trust.

5
REVIEW OF THE ANNUAL REPORT 2013/14 – SIR MICHAEL DEEGAN, CHIEF EXECUTIVE Presentation Slides Speaker’s Narrative
Sir Michael Deegan, Chief Executive presented the Review of the Annual Report 2013/14 I’m delighted to once again have the opportunity to reflect and share with you the wide range of excellent patient services this organisation, with close collaboration and support from its partners and stakeholders, delivered during 2013/14. But first, I’d like to quickly remind us all of the scale and breadth of our organisation which was established as an NHS Foundation Trust in 2009. We are a large teaching hospitals group located on several sites within the conurbation. The main campus, the Oxford Road site, comprises the:
• Manchester Royal Infirmary
• Saint Mary’s Hospital
• Manchester Royal Eye Hospital
• Royal Manchester Children's Hospital.
• The University Dental Hospital of Manchester is located just off-site.
• Trafford hospitals, acquired in 2012, includes Trafford Hospital (located in Urmston) and two out-patient hospitals in Stretford and Altrincham.
• The Trust also provides community services for adults and children in central Manchester and in addition, children’s community services for the whole of Manchester.
We are indeed one of the largest and most diverse hospital groups in the UK.

6
Across our hospitals, community and specialist services, we care for more than one million patients a year and in 2013/14 we saw:
• 290,505 patients in our A&E Departments - we witnessed an 11% increase in the number of patients attending our A&E Departments throughout the organisation
• 1,022,003 out-patient and 177,077 in-patients attendances - an
increase of 1.3% in the number of patients who attend our Out-patient
Departments (up to 1,022,0033) and 3.5% increase in the number of
in-patient attendances
• 8,642 babies delivered in Saint Mary’s Hospital - we saw 8,642
babies delivered at Saint Mary’s which is 324 more babies than the
previous year
• 178,700 operations/procedures carried out throughout our hospitals - we undertook 178,700 operations and procedures in all our hospitals, up 2% on the previous year
Some amazing statistics which clearly demonstrates how our Trust is at the very heart of healthcare delivery here in the North West

7
In our annual plan for 2013/14, the Board of Directors agreed our key priorities and these ranged from achieving the highest standards for patient safety & clinical quality to improving the patient experience whilst maintaining financial viability and stability through to implementing our research & innovation strategy in partnership with key partners such as the University and City Council. Throughout last year, our group of hospitals worked tirelessly to achieve and often exceed the key priorities set by our Board of Directors with many examples of what was achieved being outlined in our Annual Report 2013/14.

8
Some examples of our achievements in 2013/14: - Our hospital standardised mortality ratio (the number of deaths that would normally be expected) fell from 104.6 to 91.6 – the average is 100. I’m particularly pleased to note that the Hospital Standard Mortality Rate (HSMR) at Trafford has gone from being one of the highest in the country in the year before they became part of our Trust, to now being better than the average for the country. When we look at the unadjusted mortality figures, patients who are admitted to CMFT as an emergency have the lowest risk of dying across the North West. We witnessed significant improvement in our Harm Free Care campaign and behind the headline figures, there are some excellent achievements to report:
• For example, we have reduced catheter acquired urinary infections; the number of patient falls throughout the organisation fell 7.5% (from 2475 to 2290) along with a 12.5% reduction in pressure ulcers (from 1303 to 1140). Our performance was in the top 3 in the country when compared with similar Trusts
• There was an overall reduction in medication errors leading to harm and we had no medication related ‘never’ events in 2013/14
• Our Infection Control standards ensured that our infection rates continued to fall, despite increased demand and activity, for example, C. difficile – 54 cases – decrease of 20 from 2012/13
We saw an improvement in responses to some of the questions in the NHS national in-patient survey last year and in the Friends and Family Test, in our adult inpatient, A&E and assessment areas. Around 2,800 people gave feedback each month, with 74% extremely likely to recommend our hospital services to their friends and family if they needed similar treatment or care. There was clear indication of progress within the patient satisfaction survey around pain management and ward cleanliness which rose to 89% and almost 91% respectively.

9
Our commitment to ensuring we have Safe Staffing Levels throughout the organisation has resulted in an increase in nurse staffing levels on wards at night in acute medicine in the MRI. We’ve introduced a tool to determine safe staffing based on patient need. Increased recruitment to maintain safe staffing levels. Provided visible ward staffing information at ward entry – ‘Proud to Care’ initiative. Increased Health Visitor workforce in line with the National Call to Action to deliver the Healthy Child Programme and the integrated Early Years New Delivery Model. Our Health Visitor establishment in 2011, when services moved to CMFT was 89 whole time equivalent and currently, we have 128.97 whole time equivalent Health Visitors in post. This will increase to 160.37 in January 2015 when the Health Visitors that we’re supporting in training and our latest recruits come into post. Our final trajectory for the Health Visitor workforce is 173.6 whole time equivalents by April 2015. We value our people and what they do, and this is reflected in the annual NHS Staff Survey results. Staff have the opportunity to give anonymous feedback about their working environment and experience in the survey. It covers 28 different measures, and our results have improved from last year. We were delighted to see that our overall staff engagement score is now above the national average. This is all underpinned by the core attitudes and behaviours that everyone expects from their colleagues at every level of the organisation. Our core values are: Pride, Respect, Empathy, Consideration, Compassion and Dignity. One key element of our values is our commitment as an organisation to equality, diversity and human rights. Through training, activities and engagement with our staff and patients, we are developing a diverse workforce that meets the needs of our patients, service users and the wider community. An excellent example of this was our Equality and Diversity fortnight, in May 2013. This celebrated achievements, showcased good practice and raised awareness of equality, diversity and inclusion. The fortnight culminated in a hugely successful staff conference focused on diversity, attended by over 100 staff from different groups and backgrounds. The momentum from this was again evident this year with a hugely successful second E&D conference earlier this summer.

10
We successfully delivered a range of key national standards including the 62 day cancer referral standard (i.e. from GP to 1st treatment), the 4hrs maximum waiting time standard in our A&E Departments (3 out of 4 quarters) and referral to treatment standards.
The Trust’s income and expenditure for 2013/14 resulted in a surplus of £1m which means that we delivered our financial savings and balanced our books at the year end. More details are provided under the financial report 2013/14 section of the presentation.

11
Another key area of our work which continues to help improve patient care is
our research and innovation activity. Our Trust brings together
internationally renowned researchers and clinicians who take discoveries
from the laboratory into our hospitals, community services and the wider
NHS. In 2013/14 saw: -
• 15,583 patients taking part in research
• 720 ongoing research studies
• 278 new research studies
• £13.9m of external research funding
• Active member of Manchester Academic Health Science Centre
(MAHSC) and continued close working partnerships with the
University, City Council, Clinical Commissioning Groups (CCGs) and
many more.
These figures show the extent of activity across our Research Division last
year, and patients are benefiting from our discoveries on a daily basis.
Exciting developments include:
• A new blood test to predict whether women in their first pregnancy
may be at risk of a serious condition called pre-eclampsia.
• Recruiting the first three patients in the world to a trial of a new
treatment for the eye condition, vitreomacular traction (VMT).

12
• Identifying that babies with an intermittent form of low blood sugar are
at risk of brain damage, not just babies with persistent low blood
sugar.
• Discovering 42 genetic risk markers associated with rheumatoid
arthritis, as part of an international research study.
• The creation of a new Peking-Manchester Centre for Genomic
Medicine, announced by Chancellor George Osborne in October.
As a member of the Manchester Academic Health Science Centre, along
with five other Trusts and the University of Manchester, we are bringing
direct benefits to patients by sharing research, education and innovation
excellence across the partnership.
This year saw our staff also collect three awards at the first ever Greater
Manchester Clinical Research Awards:
Principal Investigator of the Year; Research Nurse of the Year; Highest
Recruiting Trust into Clinical Research Trials.

13
When I started thinking about some of my personal highlights of 2013/14, I was first reminded of the wider NHS landscape in which we were operating. The Francis Inquiry into care at Mid Staffordshire Trust, plus the Keogh and Berwick Reviews of how care is delivered to patients, continued to have a major influence on the NHS. Government, regulators and NHS England understandably focusing on the quality and safety of care in an unprecedented way. The organisations that regulate us, the Care Quality Commission and Monitor, are both rigorous and challenging during their inspections. Clearly a very challenging and uncertain period for the NHS. However, everyone at CMFT is working extremely hard to meet and where possible, to exceed, all the national standards expected of us. To reinforce this commitment, in Autumn 2013 we introduced our own programme of Internal Quality Reviews. These were in addition to the statutory inspections. We invited staff and our Governors to form independent review teams, which visited wards and other patient areas and asked five key questions. They spoke to staff, patients and visitors, reviewed paperwork and built an understanding of the care environment. They also made unannounced, out of hours visits. By encouraging people to share their experiences openly, the result was a clear and objective picture of how a ward or service is performing. Each team put together a report, highlighting some of the wonderful and inspirational work our teams deliver but also some of the areas for improvement. This was fed back to the local management team, shared with the Board of Directors and findings published on the Trust website. The Quality Reviews are a major undertaking, and complement our existing ward accreditation programme. Both initiatives reinforce our Trust’s commitment to being open and honest about where we can improve and learn from each other. Your Governors have played a key role in these programmes, and I would like to thank them personally for their contribution. On behalf of my Board colleagues I also want to thank all our staff for their dedication and outstanding teamwork. In an environment where the NHS is under constant pressure to improve quality but also manage costs, we’re very proud of our 13,000 clinical, professional and support staff. They really do make a difference to patients and their families every day.

14
There have been so many other achievements which capture the spirit and resolve of our organisation and its workforce and make me feel so proud and privileged to lead our Trust with our Chairman Peter. Whilst you can find many more examples of our achievements in our Annual Report, I’d like to share just a few more personal highlights, for example: -
• The ‘We’re Proud of You’ Awards was a fantastic event, an opportunity to celebrate the hard work and dedication of our staff. Particular congratulations go to Gillian Lee, an Active Case Manager at Chorlton Health Centre, who won the Outstanding Achievement & Patient Choice awards. Very well done to all our winners.
• In addition to delivering excellent patient services we also aspire to excel in the area of research. We were delighted therefore when our Manchester Academic Health Science Centre (MAHSC) received re-designation as one of only six elite accredited partnerships in the country; we are the only one outside the South-East of England. MAHSC is a partnership between The University of Manchester and six NHS organisations, including ourselves. The MAHSC accreditation is a quality stamp for the world-class clinical research we do in Manchester which is subsequently translated into cutting edge clinical treatments for patients.
• Trafford Hospital had, in the past, been subject to close scrutiny
because of concern about the quality of its services. Last year we were able to report that standards of patient safety had been brought into line with national norms. As a result we received the decision by the Secretary of State to support the new clinical service model at Trafford General Hospital, which was implemented towards the end of 2013. We have worked in close collaboration with doctors, nurses and all partner organisations in Trafford to design future hospital services for the people of Trafford which are safe, affordable and high quality. The new model means that the sickest patients are cared for in specialist hospitals whilst retaining local access to a broad range of high quality services for patients with less serious needs.
• In August 2013, we opened the new Cardiac Critical Care Unit along with some additional relatives accommodation. This was the 3rd phase of the new, state-of-the-art Critical Care Unit in the MRI.

15
To summarise, this year has not been without its challenges as is the case for many NHS organisations. However our Trust continues to learn, progress and achieve excellence because of our dedicated staff to whom we are indebted. I would like to take the opportunity to sincerely thank all our hard working staff, partners, supporters and fundraisers for all your energy, professionalism and commitment throughout 2013/14. Thank you so much.

16
FINANCIAL REPORT 2013/14 – URSULA DENTON, DIRECTOR OF FINANCIAL STRATEGY Presentation Slides
Speaker’s Narrative
I would like to start by paying tribute to the incredible achievement of our Divisional leadership teams who grapple with the steep productivity and efficiency challenges that we face year on year, with unceasing commitment to ensure constant improvement in the services we provide for our patients. Their efforts, supported by the Corporate Teams, will help us continue to manage within the very challenging environment that we, and the rest of the NHS continues to face. In 2013/2014 the Trust was paid £919 million for the services that we provided and it cost us £918 million to provide those services so delivering a bottom line surplus of £1.2 million pounds at the end of the year. This meant that we achieved a risk rating of 3 (in line with our Plan) from our Regulator, Monitor – where 5 is the lowest risk and 1 is the highest.

17
What we get paid for: - £m Specialised Services 318 Planned & Other Care 264 Emergency & Critical Care 134 Outpatients 79 Research , Education and Training 68 Services to Other Bodies & Other Activity 56 Total 919 The income we received was generated from providing a full range of local hospital services for the residents of central Manchester and then specialist services for both local residents and patients from much further afield. This included planned, emergency and specialised care on an inpatient or daycase basis, outpatient services, community services, research and we also provide some services to other bodies. For context in terms of size, other UK organisations with a similar turnover to ours of nearly £1 billion pounds, which you may be familiar with, are Superdrug Stores Plc. and the B&M Retail Chain

18
We spend just over £2.5 million pounds a day in providing these services. Of that we pay £1.5 million pounds a day to employ circa 12,000 expert and dedicated staff and around £15 million a month buying clinical supplies and services for our patients.

19
In 2013/2014 the Trust delivered savings in excess of £40 million pounds. One area that the Trust continues to be a leader in the NHS is its Procurement Function. In 2013/2014 this team supported the Trust to deliver nearly £4 million of non-pay savings in a whole range of areas. A few facts: -
• We send out over 1,400 orders per week to suppliers and already 17% of our spend is with small to medium companies – we aim to achieve the Government’s target of 25% by 2017/2018.
• While you are sleeping, we receive 10,000 items per week from NHS supply chain between the hours of midnight and 6am.
• The Team have been nominated for 5 awards during the year.

20
Our nationally recognised stellar Procurement Service: -
• Regular visits from other Trusts who learn from our best practice • High level of qualification and professional development within the
team • The NHS wide Zero Inflation Policy was written by us • Recognised as a leader in Electronic Commerce • CMFT is the first Trust to be visited by NHS Procurement Tsar, Lord
Carter • Advised PM’s Enterprise Advisor, Lord Young, on SME access to the
NHS As outlined, we wrote the National policy on inflation resistance – I hope that you will have seen these signs around the Trust.
21
In 2014/2015 the challenge has proven to be more difficult than we had foreseen when I was speaking to you at this time last year. The Trust is addressing these issues and expects to achieve a breakeven position by year end. For many organisations the 2015/16 predicted challenge has come early and is presenting issues across the NHS which are being reported in the media

22
2015/16 is looking excruciatingly difficult at every level across the NHS. This graph shows that the public sector debt has continued to rise and still needs to be repaid so no-one should expect the financial challenges to reduce over the next decade. Indeed the Foundation Trust Network has said that “2015/16 will be the most financially challenging year for the NHS in over 15 years” and the Nuffield Trust predicts a funding gap of some £44 billion by 2021/2022. This is against the backdrop of Specialised Commissioning having an overspend on its budgets, the impact of the creation of the Better Care Fund on local commissioners budgets and in excess of 50% of NHS providers expected to be in deficit at the end of 2014/15. For this Trust, we will learn from the challenges of 2014/15, ensure that we have all the “basics” in place and then “up the pace” on our service redesign programme working in collaboration with our partners. With front line teams being fully involved in designing services to ensure that we get it right for patients first time, every time which also leads to financially sustainable services in the longer term. Also using technology to its greatest effect, for example in the coming year we will see the first electronic referral system in the dental hospital, we will be putting Chameleon (our in-house developed electronic patient record) into Outpatients and piloted in other areas such as a ward, the emergency department and in some community services.

23
And finally some highlights relating to the Trust’s charitable funds: -
The total income for the year from legacies, investments and donations was £4.8 million. Like last year I thought I would share with you just a few of the many activities that have generated some of the donations
• A team of fundraisers travelled from Lands’ End to John O’Groats on scooters taking 6 days to reach their destination and raising over £16 thousand pounds
• 17 people took part in a tandem skydive raising over £5 thousand pounds
• 4 teenage boys and their dads took on the coast to coast bike ride in heavy wind and rain and raised over £7 thousand pounds
• 200 people took part in the second “wiggle for women zumbathon” raising over £7 thousand pounds
• 30 people took part in a 12 hour karaoke session raising almost £9 thousand pounds
I would like, on behalf of the Trust, to say a very big thank you to all those people who support our Charity in so many different ways.
24
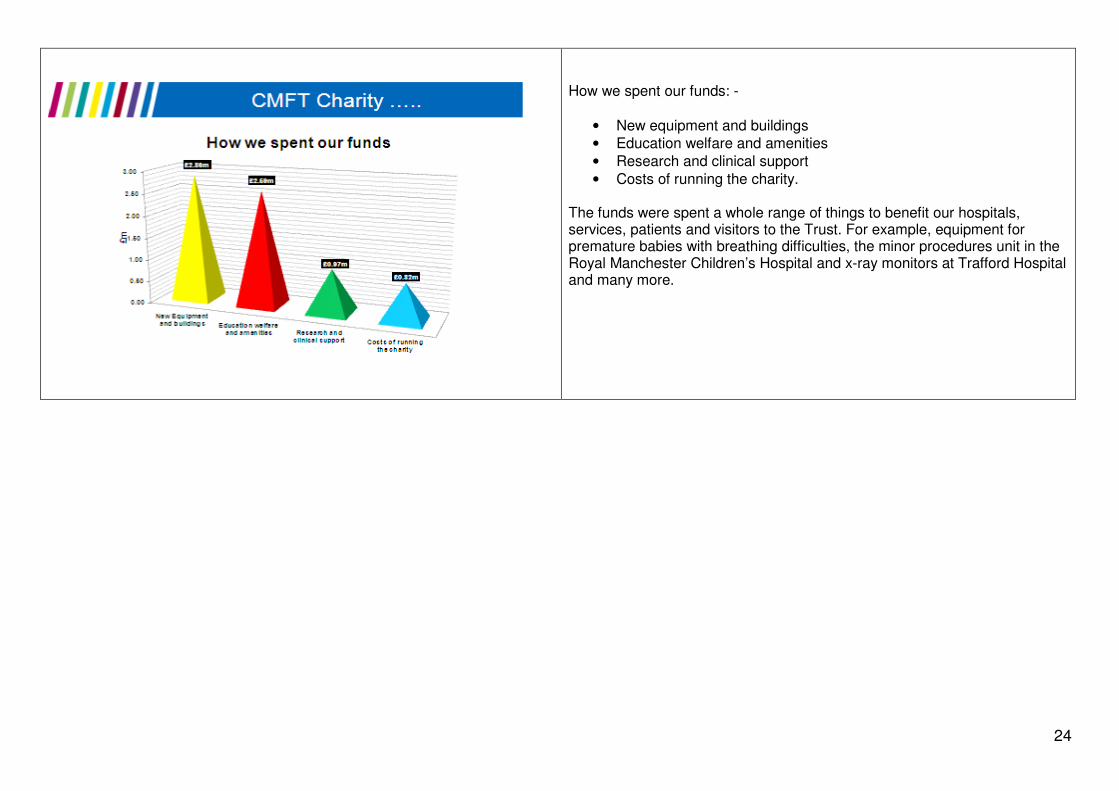
How we spent our funds: -
• New equipment and buildings
• Education welfare and amenities
• Research and clinical support
• Costs of running the charity. The funds were spent a whole range of things to benefit our hospitals, services, patients and visitors to the Trust. For example, equipment for premature babies with breathing difficulties, the minor procedures unit in the Royal Manchester Children’s Hospital and x-ray monitors at Trafford Hospital and many more.

25
MEMBERSHIP REPORT – DR KEITH PAVER, LEAD & PUBLIC GOVERNOR Presentation Slides Speaker’s Narrative
Having exceeded our public membership target (set by Monitor, the independent regulator of Foundation Trusts), our focus has been to sustain and actively engage with our membership community. We now have around 14,000 public members including nearly 700 young people (aged 11-16 years), and 13,000 staff members. Overall therefore we have a membership community of more than 27,000 members. A key element of our membership recruitment activity is to reflect the diverse nature of the communities we serve. Data taken from our membership community reveals that: -
• 22% of our members are from ethnic minority groups – against an average of 14% for the England and Wales population
• 32% of our Manchester members are from ethnic minority groups – against an average of 33% for the Manchester population
• 13% of our Governors are from ethnic minority groups.

26
To ensure we listen to you and take on board your ideas and concerns, we have a programme of member engagement. This includes events such as today’s interactive meeting, plus our careers and health event for young people which this year was attended by over 300 students, teachers and staff from Greater Manchester schools and colleges. 24 stand holders promoted NHS careers and offered health advice to our young attendees. We were delighted that our Youth and Volunteer Governors attended which also helped to enhance links between our young members and Governors. In addition, we have regular Staff Member Engagement Sessions to get feedback and suggestions, led by the Chairman and Staff Governors. Where possible, these are followed up and have generated ideas leading to real improvements for patients and staff. Invitations were sent to members to attend key Health Events including Movember Men’s Health Awareness Event and Living Longer, Living Better (integrated health and social care programme) Event. In addition, members were also invited to participate in the Trust’s Patient Led Assessments of the Care Environment (PLACE). Governors are also holding a new series of member engagement events with their constituents. They are joining events ranging from patient meetings run by local GPs to social and community group sessions, to talk about what Governors do, highlight the Trust’s forward plans and promote membership of our NHS Foundation Trust.

27
Our Council of Governors meets 3 times a year, and represents the views of patients, carers, the public, stakeholders and staff to our Board of Directors. The Governors make a key contribution every year to the Trust’s forward plans, which this year included both the Trust’s operational plan 2014-16 and the Strategic 5 year plan. They also participate in working groups which look at ways we can:
• make the experience of patients better, from enhancing communication to making it easier to get around our hospitals
• encourage better staff health and well being
• engage with our existing members in addition to promoting membership and Governor role
• act as a good corporate citizen, working on employment, education and cultural initiatives.
As a result of Governor attendance at the various meetings, hundreds of actions have been driven by Governors over the previous year. These have included actions to improve both our patient and staff experiences in addition to raising issues on behalf of our members. Governors are involved in a diverse range of projects - the Trust’s Internal Quality Reviews, Ward Accreditation Scheme, Quality Mark Assessments for “Elder-friendly Hospital Wards”, Staff Recognition Programme, Equality & Diversity Implementation Group, Complaints Review Panel, IT Strategy Board, Children’s Learning Disability Network, Workplace Shadowing Programme, Out-Patient Services Group and Patient Led Assessments of the Care Environment (PLACE). I want to emphasise that the Governors play a very active role in monitoring the performance of the Trust. We work in a very supportive and open way with the Board of Directors, and regularly review how the Trust is performing across a wide range of measures and targets. We are your eyes and ears, and take a robust and independent view of all the information we receive with Governors acting as the conduit between the Trust’s Board of Directors and members and the public by conveying membership/public interests and providing Board performance assurance.

28
If staff or public members do have questions or concerns, Governors would welcome the opportunity to discuss these with you and of course we are always keen to hear about positive experiences of the Trust's services. We look forward to speaking to you after this part of the meeting (Governors’ Question and Answer Session).

29
All our Governors are very hard-working and enthusiastic in representing you, their constituents. I’d like to thank those who are retiring this year for their very valuable contribution: Peter Clayton, Mariam Gaddah, Erica McInnis, Margaret Parkes, Lynne Richmond and Jenny Scott I’m delighted to be able to announce the results of our recent Governor elections, and would like to welcome all newly elected and nominated Governors in addition to re-elected Governors to our Council of Governors. I’m sure they will all do an excellent job in representing their constituents.
• Jayne Bessant – Public Governor (Manchester) • *Bashir Chaudhry MBE – Public Governor (Manchester) • *Patrick McGuinness – Public Governor (Manchester) • Sue Webster – Public Governor (Manchester) • *Dr Abebaw Yohannes – Public Governor (Manchester) • *Carole Shacklady – Public Governor (Greater Manchester) • *Geraldine Thompson – Staff Governor (Other Clinical) • *Prof Henry Kitchener – Nominated Governor (The University of
Manchester) • *Dr Stefan Meyer – Nominated Governor (The University of
Manchester) • *Cllr Paul Lally – Nominated Governor (Trafford Borough Council) • Cllr Rabnawaz Akbar – Nominated Governor (Manchester City
Council) • Angela Harrington – Nominated Governor (Manchester City Council) • *Graham Watkins – Nominated Governor (Volunteer Services)
*indicates newly elected or nominated Governors.

30
LOOKING AHEAD IN 2014/2015 – SIR MICHAEL DEEGAN, CHIEF EXECUTIVE Presentation Slides Speaker’s Narrative
The health and social care system is about to face unprecedented levels of demand as people are getting older and those with long term conditions are living longer. At the same time in real-terms, funding is projected to fall. The challenge is to bridge the gap between demand and resources. In recognition of this, the key stakeholders in the Manchester Health and Social Care System commissioned a study which showed that the current configuration of services is not sustainable. Income and cost pressures could drive a combined deficit of up to £58m in 2014/15 - a gap that could not be bridged by improving productivity alone. This echoed findings in other health economies, and as a result colleagues across the Greater Manchester health economy level are collaborating to address the potential gap. Four inter-dependent programmes of work have been established: -
• Integration – provision of seamless services, irrespective of which organisations delivers them, that prevent patients from being admitted to hospital unnecessarily (for Manchester this is called Living Longer, Living Better)
• Healthier Together – structuring care services in the best way • The Primary Care Strategy – further strengthening the role of primary
care.
Ongoing Quality, Innovation, Prevention and Productivity (QIPP) programmes in individual health economies

31
A major element of our longstanding strategy is developing and extending the specialised services we provide across our family of hospitals. This is aligned with two major initiatives happening across Greater Manchester. Living Longer Living Better is tasked with delivering integrated care, ensuring that hospital services, community services and social care are properly joined up to look after patients and their families. This is particularly important in view of our ageing population and the higher levels of support and care needed by older people to enable them to enjoy a good quality of life and remain in their own homes and communities. Healthier Together is a process led by the commissioners of healthcare services for Greater Manchester to create a more effective structure for providing these services, giving patients greater and more timely access to primary, secondary and specialist care. In the proposals, Central Manchester is one of three Trusts designated as ‘specialist’ and therefore providing a full range of hospital services. Local general hospitals will continue to deliver services such as emergency care, elective surgery and elderly care, and work alongside a specialist hospital. My Board colleagues and I have contributed to developing the proposals, and we fully support the principles behind them. The public consultation on the proposals has started and you can visit the Healthier Together stand here today to ask questions and share your views.

32
Our key challenge for 2014/15 (and beyond), especially within this extremely difficult economic climate, is maintaining and further improving the quality of care we provide while becoming more efficient.

33
We have set out an ambitious programme in our Annual Plan covering quality, service, research, human resources and finance. Priorities include: -
• Providing the best possible care to our patients and their families: Key clinical priorities for our organisation during the next 12 months will place renewed emphasis on delivering safe, harm-free care focusing on evidence based pathways, supervision and clinical leadership. Last year we set out three key clinical priorities as Mortality, Harm Free Care and Dementia Care. We worked with staff, patients, our Governors and the wider public to identify these as our priorities, reflecting both national and local issues of importance. They remain priorities for 2014/15, and we have added sepsis to the list.
• Developing existing services and investing in new ones: For example, transforming urgent and emergency care for the local populations and beyond with a particular emphasis on frail elderly and developing our community and integrated care services (Reduced A&E attendances; Reduced non-elective admissions; Reduced Length of Stay; Reduced readmissions for frail older people and adults with dementia, adults with long term conditions and adults at the end of life. This will also include developments to our hospital campus estate are supporting many of these priorities. For example, we are preparing a business case for expanding the facilities at MRI for adult emergency care, to meet growing demand. Developing, maintaining and consistently deploying nursing and midwifery establishments, which are informed by evidence based acuity and dependency tools and professional guidance.

34
• Supporting and developing our staff:
• Implementing the Human Resources and Occupational Development strategies, focusing on: developing leadership capability; accountability and recognition; values and behaviours (including Equality & Diversity and health and well-being); education and training, in particular for medical staff Examples include an Equality & Diversity objective included in the objectives/appraisal for every member of staff; 3% improvement on retention figures compared to 2013/14 level; 225 most senior leaders completed senior leadership development over next 3 years; 5% improvement compared to 2013/14 staff survey results for self-rated health, perceived managerial interest in personal health and well-being, work-related stress and perceived pressure to come to work
• Managing our finances and resources well: Achieving financial stability and generating funds to re-invest in our services
• Boosting our research activity and involving more patients. The opening of the new Citylabs innovation centre in the old Eye Hospital building will be a major boost for our research teams.

35
The Board of Directors has a very clear future vision for our Trust. I have every confidence that we have the right leadership, people, skills and resources to make this vision a reality. We are absolutely committed to working together to care for you and your families, delivering treatment and care that everyone can be proud of over the coming months and years.

36
YOUR QUESTIONS TO THE BOARD OF DIRECTORS – PETER MOUNT, CHAIRMAN Presentation Slides Speaker’s Narrative
Peter Mount, Chairman closed the formal presentation part of the meeting with the invitation being given to members to ask questions.

37
General Questions/Closing Remarks The Board of Directors gave their introductions and invited members to forward any questions. The following questions/issues were raised: -
• Issue was raised that the Trust’s Annual Report (2013/14) did not contain disability information.
In response, whilst no specific section of the Trust’s Annual Report (2013/14) is solely headed under the term “disability information”, the report does contain an Equality, Diversity and Human Rights Section which includes disability information in addition to the work that has been progressed in relation to patient services and our workforce. Of note, the Trust has established a Disabled Staff Network Group in order to provide a forum at which disabled staff members can raise any issues. Further plans are being progressed over the coming year to continue to make improvements which will be facilitated by the new Associate Director of Equality, Diversity and Inclusion. Andrew Peel, Public Governor (Manchester), highlighted that as a person who has suffered from disabilities from birth, he has been very proactive in his Governor role in raising disability awareness and issues to the Board of Directors which have been positively received. Of note, issues raised in relation to patient accessibility and parking have been both taken on board and acted upon with the relocation of disabled parking spaces having been implemented as a result of Andrew’s direct involvement. Assurance was given that Andrew will continue to be proactive in raising disability awareness and issues on behalf of patients and members with the need for more frequent dialogue and transparency being cited in the future. The invitation was given to attendees to forward any ideas/suggestions or issues in relation to disability to Andrew – [email protected]
• Concerns were raised in relation to the transition of patients with disabilities from children’s services to adults services.
In response, the Trust has invested significantly in relation to the transition process between Children’s and Adults Services in order to make improvements in addition to attempting to make the process as seamless as possible. Of note, the Trust has recently appointed a Deputy Director of Nursing for Communication, Safeguarding and Learning Disabilities who is progressing further plans to ensure that our patient experiences are enhanced further which for many patients with disabilities is often throughout the duration of their lifetime. The invitation was given to attendees to forward any further ideas and suggestions in order to make improvements to Marie Forshaw, Deputy Director of Nursing for Communication, Safeguarding and Learning Disabilities ([email protected])

38
• Clarification was sought as to whether the Trust is progressing plans to provide nursing staff with electronic IT hand-held devices e.g. iPads.
In response, the Trust has produced an Information and Technology (IT) Strategy which includes the provision of access to WIFI across the Trust (required to enable the functionality of electronic IT hand-held devices). Of note, the Trust’s nursing bed management system has been computerised, however there is still a significant way to go before being in a position to provide electronic IT hand-held devices, across the Trust. Attention was drawn to the Trust’s ambition to develop and establish a new Electronic Patient Record by the year 2018 with the Trust making significant investment each year (£5M) in order to fulfil this ambition and progress its IT Strategy. The establishment of the Electronic Patient Record will enable the Trust to move away from its current practices of paper recordkeeping.
• Clarification was sought in relation to the Healthier Together Consultation and specifically the finding that hospitals are not performing to the required standards (outlined in the consultation information).
In response, the NHS is experiencing a combination of factors namely challenges around adequate levels of resources combined with increasing demands on services and the health needs of patients now being more complex. As outlined in the consultation documentation, over 500 quality and safety standards have been produced by Senior Doctors and Nurses with no hospital in Greater Manchester currently delivering all these standards. The Healthier Together Consultation process has been established to review hospital healthcare provisions across Greater Manchester and sets out proposals in order for patients to be provided access to the highest standards of care wherever they live, whatever time of day or night, or whether it is a weekday or the weekend. The best results for patients are seen when hospital care is delivered by experienced Doctors and Nurses working together however currently, access to a Consultant (Senior Doctor) 24 hours a day, 7 days a week is not possible due to shortages in workforce numbers. As set out in the consultation proposals, by combining medical teams from separate hospitals into single services it is hoped will enable this standard to be met. However, this means providing care to patients at two types of hospitals namely a local General Hospital and a Specialist Hospital. Both types of hospitals will work together and will be staffed by a single team of medical staff so that patients can access a Consultant 24 hours a day, 7 days a week. Attention was drawn that Sir Bruce Keogh, NHS England’s National Medical Director has asked NHS organisations to submit plans as to how they are going to deliver this standard (7 day services) by 2016.

39
Cllr Paul Lally, new Nominated Governor (Trafford Borough Council) informed attendees that whilst the formal Healthier Together Consultation process completes on 30th September 2014, comments/feedback will be accepted up until 24th October 2014. Attendees were sign-posted to the interactive stand available at the meeting entitled “Shaping Future Health Services Together” at which representatives from the Healthier Together Team were available to discuss the programme/consultation in addition to attendees being able to complete the consultation document on-line. Of note, the Trust has progressed plans to both improve our patient experiences in addition to driving more cost effective ways of working with the savings found being reinvested back into our patient services. One of the programmes that the Trust has put in place is its Enhanced Recovery Programme which is a model of care that actively works with patients to improve their recovery time and outcomes following surgery. The evidence found following the implementation of this programme is that patients are benefitting from better outcomes and improved experiences, in addition to delivering more cost-effective ways of working.
• Consideration was requested to be given to sourcing an alternative venue for future Annual Members’ Meetings. In response, the number of members and the public attending this meeting was felt to be one of the highest to date, and consideration would be given to sourcing an alternative venue for next year’s meeting.
• Concerns were raised in relation to the Council’s requirement to segregate domestic waste and the negative effect that this can cause people living with disabilities (physical inability to undertake this process).
In response, the Trust is currently working with partner organisations (including the Manchester City Council) as part of the Living Better, Living Longer Programme which is a programme of work, in Manchester, to improve the way health and wellbeing services work together to provide high quality care in people’s home, communities and neighbourhoods. As part of this programme of work, public events are being held in order to provide a forum at which members of the public can find out more about the Living Longer, Living Better programme and forward any ideas/suggestions and issues.
• Clarification was sought as to the progress made in relation to Stem Cell Research. In response, it was stated that a lot of activity is being progressed in this area of research with the close introduction of new stem cell treatments for children being cited. It is anticipated that these new possible treatments may help people with cartileges/knees and heart conditions.

40
• Thanks and appreciation were forwarded to the Trust for the care and treatment recently received by both an attendee and her son which resulted in a “wonderful experience” which was provided by “wonderful people”.
Thanks and appreciation were forwarded to members for attending the formal presentations of the Annual Members’ Meeting and for raising a variety of questions/issues. The invitation was given to members to view the information stands which have been based around the meeting theme of “Working Together to Care for You”. Encouragement was given to attendees to participate in the interactive demonstrations provided by Trust colleagues and partner organisations provided throughout the Nowgen Centre.





























