Embed Size (px)
Citation preview
PERENCANAAN BEKERJADALAM KEMITRAAN DENGAN PEREMPUAN
DAN TIM MULTIDISIPLIN
TUGASMata Kuliah Manajemen Pelayanan Kebidanan
Dosen Pembimbing :
Dr. Emi Nurjasmi, M.Kes
Oleh :Kelompok IV
Rulfia Desi Elmispendriya Gusna
Indri Putri SariDian Febrida Sari
Laila RahmiEtika Mulia Sari
Irma Seriana
PROGRAM STUDI S2 KEBIDANANPASCASARJANA UNIVERSITAS ANDALAS PADANG
T.A 2012/ 2013
i
KATA PENGANTAR
Puji syukur penulis ucapkan kehadirat Allah SWT yang selalu melimpahkan rahmat
dan karunia-Nya serta nikmat kesehatan kepada penulis sehingga penulis dapat
menyelesaikan Tugas dengan judul “Perencanaan Bekerja dalam Kemitraan
dengan Perempuan dan Tim Multidisiplin” pada mata kuliah Manajemen Asuhan
Kebidanan Program Studi S2 Kebidanan Pascasarjana Universitas Andalas Padang
T.A 2013/ 2014 ini dapat diselesaikan. Shalawat beserta salam senantiasa tercurah
untuk Baginda Rasulullah SAW, sebagai simpul mata rantai agung seluruh
kebenaran, penyejuk dan penerang bagi umat manusia.
Penulis menyadari masih banyak kekurangan dalam penyusunan penugasan
ini, namun penulis berharap dengan kekurangan tersebut tidak mengurangi makna
dan tujuan dari penugasan ini.
Akhir kata hanya kepada-Nya lah kita semua kembali, semoga kita semua
mendapatkan karunia dan ridho dari-Nya sehingga menjadi cendikiawan yang
berguna, Amin.
Padang, Mai 2013
Penulis
i
DAFTAR ISI
KATA PENGANTAR............................................................................................ i
DAFTAR ISI ........................................................................................................ ii
BAB I PENDAHULUAN
BAB II PEMBAHASAN
A. Strategi Making Pregnancy Safer .................................................... 4
B. Bidan Sebagai Ujung TombakPelayanan Kesehatan Ibu dan Anak................................................. 6
C. Langkah Membangun Kemitraan .................................................... 12
BAB III PENUTUP
DAFTAR PUSTAKA
ii

BAB IPENDAHULUAN
Istilah bidan mencerminkan filsafat peduli; satu yang lebih khusus diarahkan
pada individu wanita dan kebutuhan reproduksi. Seorang bidan biasanya
menawarkan berbagai pilihan dan berusaha untuk menghilangkan atau
meminimalkan intervensi yang tidak perlu. Pelayanan/ praktik kebidanan didasarkan
pada philosophy kebidanan. Pada intinya, filsafat kebidanan menganggap bahwa
kelahiran yang aman, indah dan proses normal. Praktik kebidanan didasarkan pada
pemahaman bahwa kehamilan, persalinan dan kelahiran adalah pengalaman
mendalam yang membawa arti penting bagi seorang wanita, keluarga dan masyarakat
Praktik kebidanan menggabungkan seni dengan teoritis dan pengetahuan
berbasis penelitian untuk memungkinkan wanita dan bayi mencapai kesehatan yang
optimal. Pengetahuan berbasis penelitian untuk memungkinkan wanita dan bayi
mencapai kesehatan optimal dari prasangka, melalui kehamilan, persalinan, kelahiran
dan periode neonatal. Bidan menggunakan pengetahuan ilmiah ketika
mempromosikan, melindungi dan mendukung menyusui untuk memberikan yang
optimal kepada mereka dengan informasi dan bantuan yang diperlukan. Praktik
kebidanan menyediakan kesinambungan layanan antara bidan dan perempuan dari
prasangka, melalui kehamilan, persalinan, kelahiran, dan postpartum. Perawatan
kebidanan terjadi dalam kemitraan dengan perempuan dan keluarganya yang
didasarkan pada saling menghormati dan disediakan dalam cara yang holistik,
fleksibel, kreatif, memberdayakan dan mendukung. Perawatan kebidanan harus
tersedia sebagai pilihan untuk semua wanita, baik itu wanita tanpa komplikasi atau
dengan komplikasi kehamilan, terlepas dari lokasi geografis, status sosial ekonomi,
usia, latar belakang kebudayaan, orientasi gender dan agama. Mempromosikan
praktik kebidanan sebagai pengambilan keputusan bersama, tanggung jawab antara
wanita, keluarganya, dan penyedia layanan. Bidan menyediakan informasi yang
lengkap, akurat dan obyektif serta membantu wanita untuk mengambil keputusan.
Perawatan kebidanan dapat diatur, tetapi yang paling penting adalah memberdayakan
perempuan untuk menentukan pilihan dan mengambil keputusan.
1
BAB IIPEMBAHASAN
Istilah bidan mencerminkan filsafat peduli; satu yang lebih khusus diarahkan
pada individu wanita dan kebutuhan reproduksi. Seorang bidan biasanya
menawarkan berbagai pilihan dan berusaha untuk menghilangkan atau
meminimalkan intervensi yang tidak perlu. Pelayanan/ praktik kebidanan didasarkan
pada philosophy kebidanan. Pada intinya, filsafat kebidanan menganggap bahwa
kelahiran yang aman, indah dan proses normal. Praktik kebidanan didasarkan pada
pemahaman bahwa kehamilan, persalinan dan kelahiran adalah pengalaman
mendalam yang membawa arti penting bagi seorang wanita, keluarga dan
masyarakat. Kebidanan didasarkan pada keyakinan bahwa memiliki bayi adalah
proses kehidupan alam dan kesempatan bagi pertumbuhan yang cukup besar. Tujuan
dari perawatan kebidanan adalah untuk meningkatkan pengalaman hidup ini. Praktik
kebidanan didasarkan pada konsep kesehatan dan kesejahteraan. Melahirkan anak
dipandang sebagai proses fisiologis yang normal untuk sebagian besar perempuan,
dan pengalaman hidup utama bagi semua perempuan dan keluarga mereka.
Kebidanan didasarkan pada penghormatan terhadap perempuan dan keyakinan yang
kuat dalam nilai pekerjaan perempuan melahirkan dan membesarkan setiap generasi.
Bidan bekerja secara otonom dan bekerjasama dengan perawatan lain untuk
meningkatkan kesehatan dan kesejahteraan pada perempuan, bayi dan keluarga.
Praktik kebidanan menggabungkan seni dengan teoritis dan pengetahuan
berbasis penelitian untuk memungkinkan wanita dan bayi mencapai kesehatan yang
optimal. Pengetahuan berbasis penelitian untuk memungkinkan wanita dan bayi
mencapai kesehatan optimal dari prasangka, melalui kehamilan, persalinan, kelahiran
dan periode neonatal. Bidan menggunakan pengetahuan ilmiah ketika
mempromosikan, melindungi dan mendukung menyusui untuk memberikan yang
optimal kepada mereka dengan informasi dan bantuan yang diperlukan. Praktik
kebidanan menyediakan kesinambungan layanan antara bidan dan perempuan dari
prasangka, melalui kehamilan, persalinan, kelahiran, dan postpartum. Perawatan
kebidanan terjadi dalam kemitraan dengan perempuan dan keluarganya yang
didasarkan pada saling menghormati dan disediakan dalam cara yang holistik,
2
fleksibel, kreatif, memberdayakan dan mendukung. Perawatan kebidanan harus
tersedia sebagai pilihan untuk semua wanita, baik itu wanita tanpa komplikasi atau
dengan komplikasi kehamilan, terlepas dari lokasi geografis, status sosial ekonomi,
usia, latar belakang kebudayaan, orientasi gender dan agama. Mempromosikan
praktik kebidanan sebagai pengambilan keputusan bersama, tanggung jawab antara
wanita, keluarganya, dan penyedia layanan. Bidan menyediakan informasi yang
lengkap, akurat dan obyektif serta membantu wanita untuk mengambil keputusan.
Perawatan kebidanan dapat diatur, tetapi yang paling penting adalah memberdayakan
perempuan untuk menentukan pilihan dan mengambil keputusan. Bidan
menghormati hubungan mereka dengan wanita dan keluarganya, menjaga
kerahasiaan informasi yang diperoleh, dan hanya berbagi informasi terkait dengan
izin wanita atau berkaitan dengan hukum.
Pada prinsipnya asuhan yang diberikan oleh bidan kepada pasien harus
berdasarkan filosofi kebidanan. Beberapa keyakinan sebagai arahan bidan dalam
memberikan asuhan:
1. Kehamilan dan persalinan:
a. Merupakan proses alamiah/ fisiologis
b. Merupakan pengalaman yang sangat bermakna bagi perempuan, keluarga dan
masyarakat.
c. Akan membawa risiko bagi kehidupan ibu dan bayi bila terjadi kesalahan
dalam proses
2. Perempuan:
a. Pribadi yang memiliki hak, kebutuhan dan harapan.
b. Harus berpartisipasi aktif dalam pelayanan selama kehamilan, persalinan, dan
nifas.
c. Membuat pilihan dan keputusan tentang pelayanan.
d. Diperhatikan dan dihargai selama kehamilam, persalinan, dan nifas
e. Ibu dan keluarga adalah pusat asuhan kebidanan.
3. Fungsi profesi dan manfaatnya:
a. Mengupayakan kesehatan ibu dan bayinya.
b. Bidan mempunyai “power” untuk mempengaruhi/ memberikan asuhan
kebidanan.
3
c. Proses yang fisiologis harus dihargai, didukung dan dipertahankan, tapi bila
ada penyulit gunakan teknologi yang referal dan aktif agar bayi dan ibu sehat
4. Pemberdayaan dan pengambilan keputusan:
a. Perempuan harus diberdayakan dalam pengambilan keputusan melalui KIE
dan Konseling
b. Keputusan merupakan kesepakatan bersama antara bidan dengan ibu sebagai
penentu utama dalam proses pengambilan keputusan
5. Tentang asuhan :
a. Difokuskan pada aspek prevensi, promosi kesehatan dan kealamiahannya.
b. Menyediakan informasi yang obyektif, relevan guna memfasilitasi penentu
pilihannya.
c. Dilaksanakan secara kreatif, fleksible, mendukung, melayani, membimbing,
memonitoring, dan mendidik.
d. Dilakukan secara kontinyu, individual, dan tidak otoriter
e. Harus aman, memuaskan, menghormati, dan memberdayakan perempuan dan
keluarganya.
A. Strategi Making Pregnancy Safer
1. Peningkatan akses dan kualitas pelayanan kesehatan Ibu, Bayi Baru Lahir di
tingkat pelayanan dasar dan rujukan.
2. Membangun kemitraan yang efektif.
3. Mendorong pemberdayaan perempuan, keluarga, dan masyarakat.
4. Penguatan manajemen program KIA: sistem survailans, monitoring, dan
informasi KIA dan pembiayaan.
Ibu meninggal disebabkan karena tidak mempunyai akses ke pelayanan kesehatan
ibu berkualitas, terutama pelayanan kegawatdaruratan tepat waktu yang
dilatarbelakangi kejadian:
1. Terlambat mengenal tanda bahaya dan mengambil keputusan
2. Terlambat mencapai fasilitas kesehatan
3. Terlambat mendapatkan pelayanan di fasilitas kesehatan
4
Peningkatan Akses dan Kualitas Pelayanan Kesehatan Ibu, Bayi Baru Lahir
1. Keluarga Berencana
a. Penyediaan pelayanan KB gratis bagi Gakin
b. Penyediaan Alokon
c. Menurunkan kejadian Unmet Need dan 4 terlalu
2. Pelayanan Antenatal
a. Peningkatan kualitas: pemeriksaan laboratorium, konseling, imunisasi dan
gizi.
b. Integrasi dengan program terkait: IMS, HIV, Malaria, TB dan kecacingan.
c. Program perencanaan persalinan dan pencegahan komplikasi (P4K)
3. Pertolongan persalinan
a. Kemiteraan bidan – dukun
b. Persalinan dengan MAK III
c. Pertolongan persalinan di fasilitas kesehatan
4. Pelayanan masa nifas
a. Ibu
b. Neonatus
c. Dilakukan sedini mungkin
5. Penanganan Komplikasi
Penyediaan Puskesmas mampu PONED dan RS mampu PONEK yang berfungsi
menurunkan CFR
Pemberdayaan Perempuan, Keluarga dan Masyarakat
1. Pendidikan kesehatan reproduksi remaja di sekolah (formal dan non formal) dan
non sekolah.
2. Promosi tentang kesehatan reproduksi pada masyarakat termasuk pemerintah.
3. Peningkatan pengetahuan dan kesiapan tentang bahaya kehamilan, persalinan dan
nifas: Desa Siaga, GSI, pemanfaatan Buku KIA dan P4K
5
B. Bidan Sebagai Ujung Tombak Pelayanan Kesehatan Ibu dan Anak
Peningkatan Akses dan Kualitas Pelayanan Maternal dan Neonatal
1. Di masyarakat (Pelayanan esensial, deteksi kasus risti + PPGDON di Polindes/
Poskesdes).
2. Puskesmas (Pelayanan esensial, deteksi kasus risti + PONED (Tim PONED).
3. RS. Kabupaten/ Kota
4. (Pelayanan esensial, deteksi kasus risti + PONEK (Tim PONEK)
5. Pemantapan jaringan pelayanan obstetri dan neonatal di wilayah kabupaten/ kota.
6. Peningkatan Kemitraan (Lintas sektor dan program).
7. Jamkesmas
Prinsip Pelayanan Kebidanan di Desa
1. Pelayanan di komunitas desa sifatnya multi disiplin meliputi ilmu kesehatan
masyarakat, kedokteran, sosial, psikologi, komunikasi, ilmu kebidanan, dan lain-
lain yang mendukung peran bidan di komunitas.
2. Dalam memberikan pelayanan di desa bidan tetap berpedoman pada standar dan
etika profesi yang menjunjung tinggi harkat dan martabat manusia.
3. Dalam memberikan pelayanan bidan senantiasa memperhatikan dan memberi
penghargaan terhadap nilai-nilai yang berlaku di masyarakat, sepanjang tidak
merugikan dan tidak bertentangan dengan prinsip kesehatan.
Ukuran keberhasilan bidan dalam pelayanan di komunitas/ desa tidak hanya
penurunan AKI dan AKB, tapi juga bangkitnya gerakan masyarakat untuk mengatasi
masalah dan memenuhi kebutuhan kesehatan serta kualitas hidupnya.
Dapat disimpulkan bahwa:
1. Pada hakekatnya masyarakat mempunyai hak memperoleh pelayanan yang
berkualitas, sehingga Ibu Sehat Bayi sehat, selanjutnya juga Bangsa yang sehat.
2. Bidan sebagai pemberi jasa harus menjaga mutu pelayanan dan melayani sesuai
kebutuhan (mitra perempuan).
3. Bidan harus tetap meningkatkan kemampuan.
4. Bidan sebagai tenaga kesehatan pada lini terdepan (ujung tombak).
5. Bidan punya kebutuhan dan harapan (kesejahteraan, masa depan dan keamanan).
6. Pemerintah bertanggungjawab menyediakan yankes (Sarana prasana, SDM dll
(Sustainability dan Jamkesmas)
6
7. Pemerintah dan OP melakukan pengawasan dan pembinaan
Kesenjangan Kebijakan dan Implementasi Kebijakan Kesehatan Reproduksi
Penurunan Kematian Ibu di Indonesia Gerakan Sayang Ibu:
1. Indonesia ikut mendukung WSC (1990), yakni bersepakat untuk menurunkan
AKI menjadi separuh pada tahun 2000 (225 per 100.000 kelahiran) dan
meningkatkan layanan keluarga berencana bagi yang membutuhkan.
2. BKKBN melancarkan Kampanye Ibu Sehat Sejahtera (KISS), kemudian
diperbaharui menjadi Gerakan Keluarga Sehat Sejahtera (GKSS).
3. Perbaikan kualitas layanan antenatal untuk mengenali secara dini kehamilan
risiko tinggi – program bidan di desa.
4. Pada tahun 1996 dicanangkan Gerakan Sayang Ibu
Pokok Permasalahan
1. Rendahnya akses penduduk miskin pada layanan kesehatan yang berkualitas
sehingga status kesehatan mereka tertinggal dibandingkan dengan kelompok
masyarakat yang lebih mampu.
2. Motivasi rendah khususnya untuk penempatan di daerah terpencil dan miskin.
3. Kebijakan insentif yang lemah.
4. Dwi-fungsi memberikan insentif yang lebih kuat bagi petugas kesehatan untuk
bekerja di pusat-pusat pertumbuhan.
5. Program PTT dan berbagai insentif yang dikembangkan belum berhasil
mengatasi kesenjangan geografis.
6. Decentralisasi secara nyata semakin memperburuk skema insentif dan semakin
melemahkan sistem informasi kesehatan
Quality of Care
Bidan setelah mengenali kondisi gawatdarurat kebidanan perlu segera merujuk
ibu bersalin ke sistem rujukan yang handal. Namun, tidak jarang sistem rujukan yang
tersedia belum didukung kompetensi klinis dan kelengkapan peralatan medis yang
tersedia masih sub-standar. Peran bidan adalah mengenali kasus gawat darurat,
merujuk dan memfasilitasi proses rujukan.
7
Tantangan AKI di Indonesia
Masih rendahnya cakupan perawatan antenatal dan persalinan oleh nakes terlatih –
rendahnya posisi tawar perempuan. Penyebab utama AKI di Indonesia adalah
perdarahan dan infeksi, di balik angka ini tersembunyi abortus:
1. Ditaksir 2,3 juta abortus (tidak aman) terjadi setiap tahun di Indonesia.
2. 1 juta keguguran spontan.
3. 700.000 karena tidak menggunakan alkon – kehamilan tidak diinginkan.
4. 600.000 karena kegagalan KB.
15% aborsi dilakukan oleh kelompok usia <20 tahun (remaja) – tidak ada akses
pada alat kontrasepsi
Beberapa kajian tentang Bidan di desa menunjukkan bdi daerah terpencil Bidan di
Desa dituntut juga untuk melakukan asuhan perawatan anak, dan fungsi kuratif di
samping asuhan rawatan kehamilan/ persalinan. Selain itu utilisasi layanan kesehatan
masih rendah di desa, fungsi rujukan masih jauh dari optimal. Apakah masalahnya
terletak pada suplai atau demand? Sekalipun masyarakat miskin sudah dijamin
(askeskin, jamkesmas) untuk layanan kuratif, bagaimana dengan transportasi?
Catatan atas Kebijakan Kesehatan
1. Sektor swasta belum lagi diperhitungkan dalam perencanaan kesehatan, padahal
kontribusinya pada kespro sangat bermakna khususnya di perkotaan.
2. Merupakan kenyataan bahwa kebijakan publik masih belum menyentuh
persoalan publik yang semakin hari semakin merupakan ancaman: pengendalian
tembakau (Indonesia belum bersedia meratifikasi FCTC), pergeseran pola diit
yang semakin memburuk – junk food menjadi makanan trendy?, kebijakan
kesehatan masih fokus pada layanan kuratif (UKP?)
Indikator Sistem Informasi Manajemen Kesehatan Ibu dan Anak
Target global penurunan Angka Kematian Ibu (AKI) MDGs (Millenium
Development Goals sebesar tiga-perempatnya pada tahun 2015. Sementara target
penurunan Angka Kematian Bayi (AKB) dan Angka Kematian Balita (AKABA)
sebesar dua-pertiga. Berdasarkan kesepakat global tersebut Indonesia mempunyai
komitmen untuk menurunkan Angka Kematian Ibu menjadi 102/100.000 Kelahiran
Hidup (KH), Angka Kematian Bayi dari 68 menjadi 23/1.000 KH, dan Angka
8
Kematian Balita 97 menjadi 32/1.000 KH pada tahun 2015. Jika dilihat dari potensi
untuk menurunkan Angka kematian Ibu (AKI) masih on track walaupun diperlukan
sumber daya yang kompeten (Pedoman Pengawasan Wilayah Setempat Kesehatan
Ibu dan Anak, Depkes RI. 2009).
Terkait dengan tujuan dan target diatas, kemudian diterapkan berbagai
strategi untuk menurunkan AKI-AKABA, maupun AKB, sehingga tetap on the track
menuju target MDGs. Dan salah satu strategi ini, diantaranya dengan penerapan
system informasi manajemen kesehatan ibu dan anak, dengaan penerapan
pemantauan wilayan setempat (PWS) KIA.
Menurut Davis (1992), pada dasarnya, Sistem Informasi Manajemen
merupakan sistem manusia atau mesin yang terpadu guna menyajikan informasi
untuk mendukung fungsi operasional, manajemen dan pengambilan keputusan di
dalam suatu organisasi. Sementara menurut Jogiyanto (2009), sistem informasi
manajemen dapat digunakan untuk mendukung kegiatan-kegiatan yang ada di fungsi-
fungsi bisnis. Sistem informasi di fungsi-fungsi organisasi yang memanfaatkan basis
data (data base) ini untuk pelaporan-pelaporan manajemen ini disebut dengan sistem
informasi bisnis (business information systems).
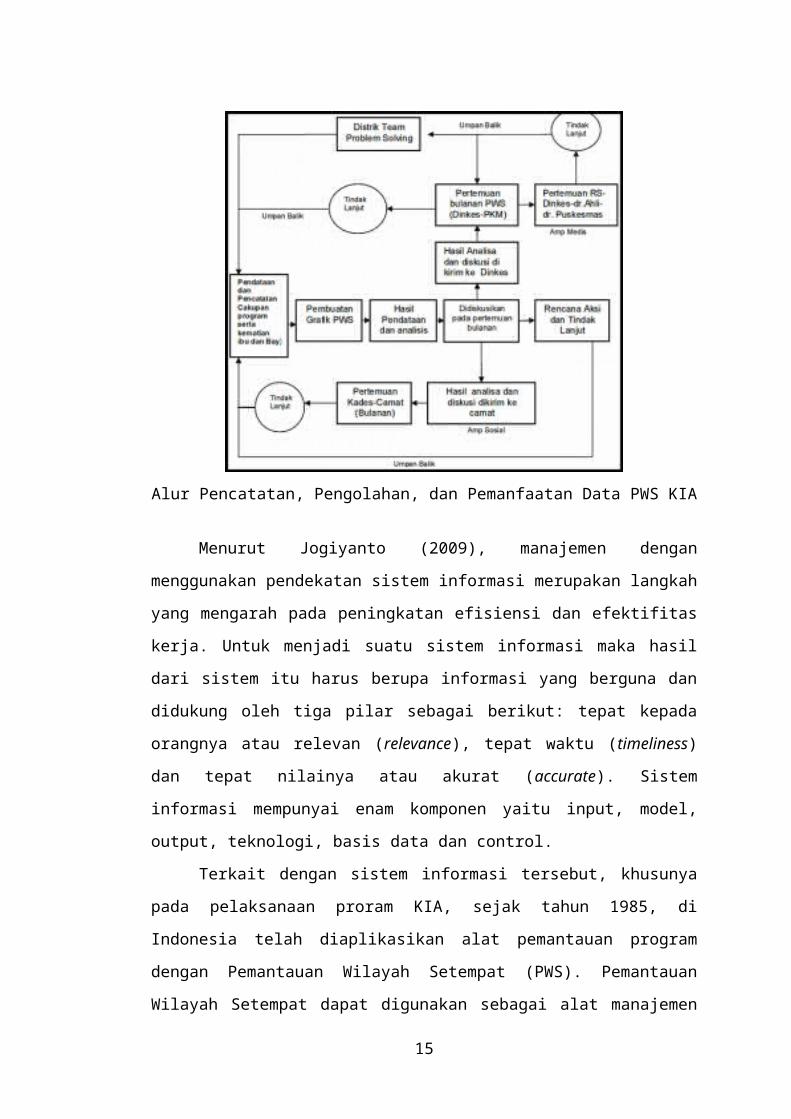
Alur Pencatatan, Pengolahan, dan Pemanfaatan Data PWS KIA
9
Menurut Jogiyanto (2009), manajemen dengan menggunakan pendekatan
sistem informasi merupakan langkah yang mengarah pada peningkatan efisiensi dan
efektifitas kerja. Untuk menjadi suatu sistem informasi maka hasil dari sistem itu
harus berupa informasi yang berguna dan didukung oleh tiga pilar sebagai berikut:
tepat kepada orangnya atau relevan (relevance), tepat waktu (timeliness) dan tepat
nilainya atau akurat (accurate). Sistem informasi mempunyai enam komponen yaitu
input, model, output, teknologi, basis data dan control.
Terkait dengan sistem informasi tersebut, khusunya pada pelaksanaan proram
KIA, sejak tahun 1985, di Indonesia telah diaplikasikan alat pemantauan program
dengan Pemantauan Wilayah Setempat (PWS). Pemantauan Wilayah Setempat dapat
digunakan sebagai alat manajemen untuk melakukan pemantauan program di suatu
wilayah kerja secara terus menerus, agar dapat dilakukan tindak lanjut yang cepat
dan tepat. Program PWS KIA dapat memantau program KIA yang meliputi
pelayanan ibu hamil, ibu bersalin, ibu nifas, ibu dengan komplikasi kebidanan,
keluarga berencana, bayi baru lahir, bayi baru lahir dengan komplikasi, bayi, dan
balita. Adapun kegiatan PWS KIA terdiri dari pengumpulan, pengolahan, analisis
dan interpretasi data serta penyebarluasan informasi ke penyelenggara program dan
pihak/ instansi terkait dan tindak lanjut.
Beberapa indikator pemantauan program KIA yang dipakai untuk PWS KIA
meliputi indikator yang dapat menggambarkan keadaan dalam program pokok KIA
sebagai, antara lain :
1. Akses pelayanan antenatal (K1)
Adalah cakupan ibu hamil yang pertama kali mendapat pelayanan antenatal oleh
tenaga kesehatan di suatu wilayah kerja pada kurun waktu tertentu. Indikator
akses ini digunakan untuk mengetahui jangkauan pelayanan antenatal serta
kemampuan program dalam menggerakkan masyarakat.
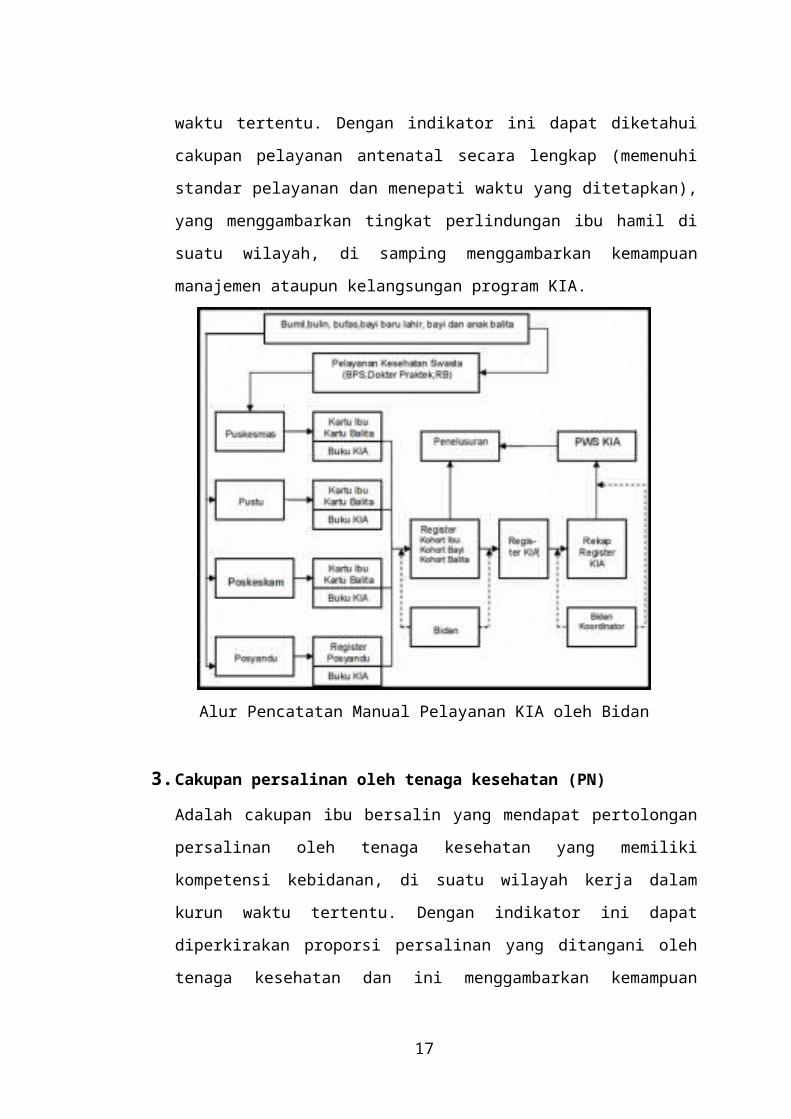
2. Cakupan pelayanan ibu hamil (K4)
Adalah cakupan ibu hamil yang telah memperoleh pelayanan antenatal sesuai
dengan standar, paling sedikit empat kali dengan distribusi waktu 1 kali pada
trimester satu, 1 kali pada trimester dua, dan 2 kali pada trimester tiga di suatu
wilayah kerja pada kurun waktu tertentu. Dengan indikator ini dapat diketahui
cakupan pelayanan antenatal secara lengkap (memenuhi standar pelayanan dan
menepati waktu yang ditetapkan), yang menggambarkan tingkat perlindungan ibu
10
hamil di suatu wilayah, di samping menggambarkan kemampuan manajemen
ataupun kelangsungan program KIA.
Alur Pencatatan Manual Pelayanan KIA oleh Bidan
3. Cakupan persalinan oleh tenaga kesehatan (PN)
Adalah cakupan ibu bersalin yang mendapat pertolongan persalinan oleh tenaga
kesehatan yang memiliki kompetensi kebidanan, di suatu wilayah kerja dalam
kurun waktu tertentu. Dengan indikator ini dapat diperkirakan proporsi
persalinan yang ditangani oleh tenaga kesehatan dan ini menggambarkan
kemampuan manajemen program KIA dalam pertolongan persalinan sesuai
standar.
4. Cakupan pelayanan nifas oleh tenaga kesehatan (KFIII)
Adalah cakupan pelayanan kepada ibu pada masa 6 jam sampai dengan 42 hari
pasca bersalin sesuai standar paling sedikit 3 kali dengan distribusi waktu 6 jam
sampai dengan 3 hari, 8 sampai dengan 14 hari dan 36 sampai dengan 42 hari
setelah bersalin di suatu wilayah kerja pada kurun waktu tertentu. Dengan
menggunakan indikator tersebut, dapat diketahui cakupan pelayanan nifas secara
lengkap (memenuhi standar pelayanan dan menepati waktu yang ditetapkan),
yang menggambarkan jangkauan dan kualitas pelayanan kesehatan ibu nifas,
11
disamping menggambarkan kemampuan manajemen ataupun kelangsungan
program KIA.
5. Cakupan pelayanan neonatus pertama (KN I)
Adalah cakupan neonatus yang mendapatkan pelayanan sesuai standar pada 6 –
48 jam setelah lahir di suatu wilayah kerja pada kurun waktu tertentu. Dengan
indikator ini dapat diketahui akses/jangkauan pelayanan kesehatan neonatal.
6. Cakupan pelayanan neonatus Lengkap (KN Lengkap).
Adalah cakupan neonatus yang mendapatkan pelayanan sesuai standar sedikitnya
tiga kali yaitu 1 kali pada 6 – 48 jam, 1 kali pada hari ke-3 sampai hari ke-7, dan
1 kali pada hari ke-8 sampai hari ke-28 setelah lahir disuatu wilayah kerja pada
kurun waktu tertentu. Dengan indikator ini dapat diketahui efektifitas dan
kualitas pelayanan kesehatan neonatal.
7. Deteksi faktor risiko dan komplikasi oleh Masyarakat
Adalah cakupan ibu hamil dengan faktor risiko atau komplikasi yang ditemukan
oleh kader atau dukun bayi atau masyarakat serta dirujuk ke tenaga kesehatan di
suatu wilayah kerja pada kurun waktu tertentu. Indikator ini menggambarkan
peran serta dan keterlibatan masyarakat dalam mendukung upaya peningkatan
kesehatan ibu hamil, bersalin dan nifas.
8. Cakupan Penanganan komplikasi Obstetri (PK)
Adalah cakupan Ibu dengan komplikasi kebidanan di suatu wilayah kerja pada
kurun waktu tertentu yang ditangani secara definitif sesuai dengan standar oleh
tenaga kesehatan kompeten pada tingkat pelayanan dasar dan rujukan.
Penanganan definitif adalah penanganan/pemberian tindakan terakhir untuk
menyelesaikan permasalahan setiap kasus komplikasi kebidanan. Indikator ini
mengukur kemampuan manajemen program KIA dalam menyelenggarakan
pelayanan kesehatan secara professional kepada ibu hamil bersalin dan nifas
dengan komplikasi.
C. Langkah Membangun Kemitraan
3 (tiga) Prinsip kemitraan, 7 (tujuh) Landasan dan 6 (enam) Langkah.
12
Langkah 1 adalah Penjajakan
Langkah ini untuk menjajaki para calon mitra yang akan diajak kerjasama untuk
suatu Tujuan Kemitraan Kesehatan.
Beberapa hal yang harus dilakukan adalah :
1. Mencari tahu organisasi apa saja yang akan kita ajak.
2. Mengetahui apa yang menjadi Tugas pokok dan fungsi (Tupoksi) dari masing-
masing organisasi tersebut, misal untuk kemitraan Posyandu :
a. Camat mempunyai Tupoksi sebagai koordinator dan penanggung jawab
pembangunan di Kecamatan (cocok kita ajak bermitra),
b. UPT Dinas Pendidikan tupoksinya sebagai penyelenggara pendidikan baik di
sekolah maupun luar sekolah (cocok kita ajak bermitra),
3. Setelah tahu tupoksinya dari masing-masing calon mitra maka kita kaji manfaat
apa yang akan kita tawarkan bagi calon mitra, agar yang bersangkutan mau
diajak bermitra.
Langkah ke-1 ini adalah untuk memenuhi Landasan 1 (Stucture) dan 2 (Capacity).
Langkah 2 adalah Penyamaan Persepsi
Disini kita mengundang para calon mitra untuk menawarkan kemitraan, dengan
menjelaskan secara rinci tentang :
1. Tujuan yang akan dicapai
2. Manfaat kemitraan (keuntungan bagi masyarakat dan masing- masing mitra)
3. Resiko yang mungkin akan dihadapi bersama.
Pada langkah ini dituntut kemampuan kita untuk berkomunikasi, lobi, dan menarik
perhatian calon mitra.
13
Langkah 3 adalah Pengaturan Peran
Pengaturan peran hanya di konsep kesehatan saja, secara tertulis (formal) adalah
tertulis. Peran/ Tugas masing- masing anggota mitra.
Ada 7 Peran untuk anggota mitra, yaitu :
1. Inisiator : memprakarsai kemitraan dalam rangka sosialisasi dan operasionalisasi
Indonesia Sehat.
2. Motor/dinamisator : sebagai penggerak kemitraan, melalui pertemuan, kegiatan
bersama dan sebagainya.
3. Fasilitator : memfasilitasi, memberi kemudahan sehingga kegiatan kemitraan
dapat berjalan lancer.
4. Anggota aktif : berperan sebagai anggota kemitraan aktif.
5. Peserta kreatif : Sebagai peserta kegiatan kemitraan yang kreatif.
6. Pemasok sumber daya : memberi masukan tehnis (Program kesehatan).
7. Dukungan sumber daya : memberi dukungan sumber daya sesuai keadaan,
masalah, dan potensi yang ada.
Langkah 4 adalah Komunikasi Intensif
Hal ini dilakukan untuk menjaga kesepakatan yang telah dicapai, dan untuk
mengetahui apa ada masalah yang dihadapi oleh masing- masing anggota mitra,
sehingga bisa pecahkan bersama.
Langkah 5 adalah Melaksanakan Kegiatan
Setelah Kesepakatan Kemitraan sudah disetujui oleh anggota Mitra, maka kita
menyusun rencana kerja kemitraan dan pelaksanaan kegiatan bersama dengan
14
anggota Mitra. Prinsip dari pelaksanaan kemitraan adalah seluruh anggota Mitra
yang telah diberi peran harus ikut serta dalam pelaksanaan.
Langkah 6 adalah Pemantauan dan Penilaian
Pemantauan dan penilaian sudah harus masuk dalam rencana kerja kemitraan,
sehingga dalam pelaksanaannya sudah ada kesepakatan tentang : Indikator
penilaian
15
Health Promotion Services For Lifestyle Development Within A UK Hospital – Patients' Experiences And Views
Charlotte L Haynes Correspondence: Charlotte L Haynes [email protected] AffiliationsClinical Effectiveness Unit, Stockport NHS Foundation Trust, Cheshire, UK BMC Public Health 2008, 8:284 doi:10.1186/1471-2458-8-284© 2008 Haynes; licensee BioMed Central Ltd.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
BackgroundUK public health policy requires hospitals to have in place health promotion services which enable patients to improve their health through adopting healthy behaviours, i.e. health education. This study investigated hospitalised patients' experiences of health education for smoking, alcohol use, diet, physical activity, and weight, and their views concerning the appropriateness of hospitals as a setting for the delivery of health education services.
MethodsRecently discharged adult hospital patients (n = 322) were sent a questionnaire asking about their smoking, alcohol use, diet, physical activity, and weight. For each of these risk factors, participants were asked whether they agreed with screening for the risk factor, whether they received health education, whether it was "helpful", and if they wanted to change their behaviour. Participants were also asked a set of general questions concerning health education within hospitals.
Results190 patients responded (59%). Over 80% agreed with screening for all risk factors. 80% of smokers, 52% consuming alcohol above recommended limits, 86% of obese, 66% consuming less than five fruit and vegetables a day, and 61% of physically inactive participants wanted to change their respective behaviour. However only a third reported receiving health education. While over 60% of patients wanted health education around discharge, the majority of those receiving health education did so at admission. The majority agreed that "hospital is a good place for patients to receive" health education (87%) and that "the hospital should provide patients with details of community organisations that provide" health education (83%). Only a minority (31%) reported a preference for health education from their GP instead of hospital.
16
ConclusionWhile the delivery of health education to patients within hospital was poor, hospitals are viewed by patients as an appropriate, and in some cases preferred setting for the screening of risk factors and delivery of health education.
Background
There is increasing pressure on hospitals to deliver health promotion services for
healthy lifestyles to patients [1-4]. The Ottawa charter for health promotion, 1986
provides a broad definition of health promotion as "the process of enabling people to
increase control over, and to improve, their health" [5]. This can only be achieved
through coordinated action from governmental and nongovernmental organisations,
the health, social and economic sectors, voluntary organization, local authorities,
industry, the media and communities to achieve "healthy public policy" [5] which
creates environments supportive of health, (such as safe walking and cycling routes),
supporting people in developing personal skills (by providing information on healthy
lifestyles and disease management, enhancing health literacy and life skills),
reorienting health services so that they focus on preventing disease/encouraging
health in addition to curing existing conditions [5] and strengthening community
action by involving communities in socio-political activities that impact on their own
health [5,6]. The principles and practice of health promotion specifically within
hospitals has been further developed in The Budapest Declaration on Health
promoting Hospitals, 1991 [7] and The Vienna Recommendations on Health
Promoting Hospitals, 1999 [8]. These recommendations are embodied in the
guidelines developed by the World Health Organisation Health Promoting Hospitals
(WHO HPH) project/network [3,4]. One of the core aims of the WHO HPH network
is to facilitate change within the quality management of hospitals, with health
promotion a core quality dimension [9]. To this end the WHO HPH network has
recently developed a strategic and quality framework for health promoting hospitals
[4]. This highlights areas which all health promoting hospitals should have as part of
their quality development strategy that would benefit key stakeholders: patients, staff
and communities (see table 1 for the development strategy aimed at patients). The
first three strategies (PAT 1 to PAT 3) should be delivered by all health promoting
hospitals as they aim to further develop the health promoting quality of the hospital
services and setting, whereas strategies PAT 4 through to PAT 6 are viewed as
additional health promotion strategies which hospitals can offer.
17
Key to the concept of health promotion is "empowerment" of individuals,
social groups and communities: "a process through which people gain greater
control over decisions and actions affecting their health" [10]. Health promotion
interventions within healthcare can empower people through "self-reproduction":
supporting patients to take responsibility for self-care physically, mentally and
socially; through "co-production": collaboration of the patient in their therapy;
empowering health promotion services for illness management (usually part of
integrated care and beyond the hospital boundaries); and empowering health
promotion services for lifestyle development: people are empowered to live healthy
lives by preventing risk (e.g. not smoking or excessive alcohol intake) or enhancing
lifestyles (e.g. becoming more physically active). This latter aspect of empowerment
relates to the concept of "health education" which can be defined as "an activity that
seeks to inform the individual on the nature and causes of health/illness and that
individual's personal level of risk associated with their lifestyle-related behaviour....
[it] seeks to motivate the individual to accept a process of behavioural-change
through directly influencing their value, belief and attitude systems, where it is
deemed that the individual is particularly at risk or has already been affected by
illness/disease or disability" (p. 313 [6]).
It is the provision of health promotion services for lifestyle development
(health education) to patients within hospitals which is of interest in this study (Table
1, strategy PAT 5). Specifically, the strategy for health promoting lifestyle
development aims at "improving the outcome of hospital interventions by
empowering patients to build up specific health literacy (knowledge, skills and
preferences) for developing and maintaining health promoting life styles" ([4] p.30).
The strategies should be viewed as a coherent programme of development as they are
inextricably linked with one another. For example, for the health education strategy
(PAT 5) to work optimally, patients who are empowered to self care and co-produce
will be more able to take responsibility for developing and maintaining healthy
lifestyles post-discharge (PAT 1 and 2). The hospital also has to be an appropriate
environment for providing health education (e.g. suitable rooms; PAT 3); and
empowerment to self manage diseases/impairments will often be associated with
particular lifestyles (PAT 4).
18
In addition to the WHO HPH network strategies, public health policy in the
UK now highlights the importance of providing personalised support (understanding
patients' cultural and social background, etc) to patients to enable them to lead a
"healthy" life (not smoking, sensible alcohol use, etc) [1]. While UK hospitals have
always had elements of health promotion within routine care, the explicit demand
that hospitals provide health promotion services to patients for lifestyle development,
in particular focusing on smoking, alcohol misuse, obesity, diet, and exercise, is
relatively new [11].
An audit of health promotion activities within 9 English hospitals revealed
that while the majority of hospitalised patients were screened for smoking (94.1%)
and alcohol use (83.1%), few were screened for diet (23.0%), physical activity
(2.6%) or obesity (11.7%). The provision of health education was poor: an average
of 22.5% of patients received health education for smoking cessation, 36.0% for
alcohol misuse and very few for diet, physical activity or weight management
(numbers of patients identified as requiring health education for the latter three risk
factors was so low that reporting the average figures would be misleading) [12].
While the above findings present a bleak picture of health education services
within hospitals, there is evidence that medical records show low levels of accuracy
for the recording of such activities [13,14]. Direct observation is viewed as the "gold
standard" for measuring practice; however it is not practical for exploring the
provision of health education provision to hospitalised patients as these services may
be delivered at any/many points during an admission. Previous research within
primary care settings indicates that patients' recall of health education is more
accurate than medical records [14]. It therefore appears that relying on patient recall
may be the most pragmatic approach to measuring health education delivered on
potentially multiple occasions and by multiple healthcare professionals.
There is evidence that approximately 50% of the English public support the
NHS "taking a lead role in preventing illness and improving health" [15], and that the
majority of adult hospitalised patients think hospitals should take a role in health
education [16]. However, with the exception of a study by McBride, 2004, views
regarding the appropriateness of hospitals as a setting for the delivery of health
promotion services, including health education, have received little investigation
[16].
19
This study aimed to provide an insight into the provision of health education
for smoking, alcohol misuse, obesity, diet, and exercise within a UK hospital
following UK public health policy changes highlighted above and the WHO HPH
strategy for health promoting lifestyle development for patients; and to address the
paucity of research on patients' views of the appropriateness/acceptability of the
hospital as a setting for the delivery of health promotion services for lifestyle
development.
Methods
Rationale
A search of the literature at the time of developing this study indicated that there was
no one survey tool that adequately met the study research questions: What lifestyle
development (health education) services do patients want from a hospital setting? Is
the hospital a suitable setting for the delivery of health education services? And how
are patients' views related to their lifestyles? A self-administered questionnaire was
deemed the most appropriate tool for investigating the research questions as it could
be distributed to a relatively large number of patients and allowed for anonymity,
hence increasing the likelihood of honest opinions about views and experiences of
health education within the hospital [17].
Questionnaire
The following tools were adapted to assess the prevalence of smoking, alcohol
misuse, obesity, physical inactivity and unhealthy diet (risk factors): Stockport
Health and Lifestyle Survey [18], the "Five Shot Screening Tool": a validated test for
detecting hazardous and harmful alcohol use [19], and a validated two-item dietary
questionnaire [20]. As no questionnaires existed which addressed patients' attitudes
to health education in hospitals a semi-structured interview was developed, based on
face validity, by the researcher and steering group (patient representatives, hospital
management, nursing, clinician and academic representatives). This was undertaken
to the point of data saturation: 10 hospital patients differing in age, gender and
ethnicity.
20
Following content analysis of the interviews and adaptation of the aforementioned
existing tools, the questionnaire was designed. The steering group and hospital
patients provided comments on the coherence and legibility of the questionnaire to
ensure that it adhered to the principles of good survey design [17]. The questionnaire
was finalised following a pilot phase in which 19 recently discharged patients
completed the questionnaire.
For the purposes of the study, the term health promotion rather than "health
education" was used throughout the questionnaire as the former term was deemed
more familiar to the public and there were concerns that "education" would be
interpreted as reflecting a "teacher-pupil" relationship rather than a collaborative
relationship where the patient plays an active role in their lifestyle development.
"Health promotion" was defined as any action taken by a member of staff at the
hospital to enable the patient to take control over aspects of their lifestyle that may
have a negative effect on their health. Actions included verbal and written advice,
medications and referral to specialists/services that aim to change unhealthy
behaviours into healthy behaviours (e.g. quitting smoking). While patients were
being asked their views on "health promotion", given that the definition provided
more accurately reflects "health education", the latter term will be used throughout
the paper.
The questionnaire followed the same format for each risk factor (smoking,
alcohol, diet, exercise, and weight). Patients were asked whether they agreed that "all
adult patients should be asked about their risk factor" (screening agreement).
Responses were on a five point likert scale ranging from "strongly agree" to
"strongly disagree". Patients were then asked whether anyone at the hospital asked
them about the risk factor (screening). For example "During your hospital admission
were you asked about the amount of alcohol you drink?" Participants could answer
"yes" or "no". Measurements of height and weight were not asked about as this does
not necessarily indicate that body mass index (BMI) was calculated. Information was
then gathered on whether the patient has a risk factor (risk factor prevalence). They
were then asked whether they wanted to change their "risky" behaviour (change).
The options were "yes" or "no".
21
Information on the type of health education delivered within the hospital was
gathered. This could range from leaflets, verbal advice, referral to a
specialist/service. Participants were asked to circle the correct option(s) and there
was a free text option for describing any additional health education delivered.
Patients were asked who delivered the health education and to rate the "helpfulness"
of the health education on a likert scale from 1 ("not at all helpful") to 5 ("very
helpful"). Patients were also asked a set of general questions relating to the
appropriateness of health education within hospitals.
Participants
Participants for this study were selected on the basis that they were from the adult (≥
17 years old) hospitalised and day-case patient populations of one Acute Trust. A
routine was established in which all patients discharged alive between January and
March 2006 were identified within one week of their discharge from twelve wards
representing surgery and medicine. Patients who were terminally ill were excluded
from this study as it was deemed inappropriate to deliver health education to these
patients.
A total of 322 people were identified and sent a questionnaire within a
maximum of one month of their discharge. To optimise return-rate patients were sent
a pre-letter, pre-paid return addressed envelopes along with the questionnaire, and
two reminders sent 1 week and 2 weeks following the questionnaire.
Analyses
An Excel workbook was developed for recording all data. Analyses were performed
using StatsDirect Version 2.4.5 and SPSS 15.0. Patients who returned the
questionnaire are described as "responders" and those who did not return the
questionnaire "non-responders". Differences in age between responders and non-
responders were assessed by one-way ANOVA with gender as a factor. Mann-
Whitney U tests were employed to assess differences in length of stay (LoS) and
Index of Multiple Deprivation (IMD) scores [21] as data were distributed non-
parametrically. IMD scores provide an indicator of deprivation based on income,
employment status, self-reported health and disability, educational level, housing,
living environment and crime based on geographical area (the small area level).
22
The higher the score, the greater the level of deprivation. Proportion
differences for screening of smoking and alcohol use, smoking behaviour and
alcohol misuse were calculated for responders versus non-responders based on
findings in patients' case notes.All reported significance values are two-tailed. In
order to describe the responses to all questions, these were subject to descriptive
statistics: proportions, proportions ± 95% confidence interval (CI) and tests for
proportion differences where appropriate. SCREENING AGREEMENT questions
were also subject to the Friedman test to examine whether responses were similar
across the four risk factors (smoking, diet, alcohol and exercise).
This study received Local Research Ethics approval.
Results
Demographics
One hundred and three females and eighty-seven males returned the questionnaire
(59% response rate). The mean age and median length of stay for responders and
non-responders are reported in table 2. There was a trend towards male non-
responders being younger than female non-responders and all responders. There were
no significant differences in the median length of stay or socio-economic status
(IMD score) between the groups, nor in the proportion of responders and non-
responders who were (according to their medical case notes) screened for smoking
and alcohol, or identified as misusing alcohol (see table 3). There were however
significantly more smokers (according to case note information) amongst non-
responders compared to responders.
Questionnaire findings
Screening
The majority of responders reported that they were asked by a member of the
hospital staff whether they smoked (156/183; 95% CI = 0.79 to 0.90) and they were
asked about their alcohol use (115/188; 95% CI = 0.54 to 0.68). However only about
a quarter were asked about their usual diet (46/184; 95% CI = 0.19 to 0.32) and
physical activity (42/175; 95% CI = 0.18 to 0.31).
23
Risk factor prevalence and health education delivered
Additional file 1 reports the proportion of responders identified by the questionnaire
as having a risk factor, and of those with a risk factor, the proportion receiving any
type of health education, plus details of the form health education took for each risk
factor. Of the 20.5% respondents identified as smokers, 44.4% reported receiving
some type of health education. The proportion of patients identified as misusing
alcohol according to self-reported weekly consumption compared to the Five shot
tool is not significant (proportion difference = -0.019, 95% CI = -0.11 to 0.08 P =
0.70). Between 21% and 29% of these patients received health education for alcohol
misuse. While the majority of respondents consumed less than five portions of fruit
and vegetables a day and were physical inactive, only 11.9% and 15.4% received
health education for diet and physical activity respectively.
Nearly half of respondents were either obese or overweight, but very few
received any form of health education concerning weight loss. In total sixty-three
patients reported receiving health education for at least one risk factor during their
hospital episode (i.e. 33.2% of respondents). Forty-four received health education for
one risk factor only, eleven for two risk factors, six for three risk factors and two
received health education for four risk factors.
Figure 1 reports the "helpfulness" ratings for the health education delivered.
51.7% of patients reported that the health education they received was helpful (score
of 4 or 5), 27.6% appear undecided (score of 3) and 20.7% viewed the health
education services as unhelpful (score of 1 or 2).
Ratings of "helpfulness" for health promotion delivered. A score of 1 indicated
that the health promotion was "not at all helpful" and a score of 5: "very helpful".
White fill: Exercise, Horizontal lines fill: Diet, Diagonal lines fill: Alcohol, Grey
dots fill: Smoking.
Change
Figure 2 shows the percentage of participants who reported that they would like
advice concerning how to change a risk factor (only for those with evidence of the
risk factor). The majority of smokers wanted to quit smoking. Based on self-reported
alcohol consumed in the past week, 16/31 identified as harmful/hazardous drinkers
reported that they wanted to reduce their alcohol intake.
24
On the basis of the Five shot tool 25/48 participants categorised as potentially
misusing alcohol said they wanted to reduce their alcohol intake.Of those who
consumed alcohol within recommended weekly limits (100) only 9 wanted to reduce
their alcohol intake; and only 2/140 participants categorised as having no alcohol
problem according to the Five shot tool wanted to reduce their alcohol intake.
Figure 2. Percentage of responders who wanted to change a risk factor. Figures
are based on identified need. Grey fill: Yes, White fill: No.
While approximately half of all respondents wanted to reduce their weight,
when desire to lose weight was related to BMI, 86% of obese individuals (BMI >30
Kg/m2; see figure 2), 78% of overweight individuals (BMI 26–30 Kg/m2), 28% of
those with a normal BMI (18.5–25 Kg/m2) and none of the underweight participants
(BMI <18.5 Kg/m2) wanted to lose weight.
Significantly more people who consumed less than five portions of fruit and
vegetables a day wanted dietary advice during their hospital admission compared to
those who consumed five portions a day (67% and 36% respectively, chi-square test
using continuity correction, P = 0.0012).
There was no difference in the proportion of patients who wanted to increase
exercise when assessed according to whether patients engaged in the recommended
30 minutes of moderate physical activity five times a week or not (55.1% and 61.3%
respectively, chi-square test using continuity correction, P = 0.397).
Appropriateness of health education within hospitals
Screening agreement
Inspection of figure 3 reveals that the majority of participants "strongly
agreed"/"agreed" with all adult hospital patients being asked about their smoking,
alcohol use, diet and exercise. The overall Friedman test statistic was significant (F =
31.94, P < 0.0001). Patients agreed significantly more with screening for smoking
compared to screening for all other risk factors (P < 0.0001 for smoking compared to
each remaining risk factor) and with screening for alcohol compared to exercise (P <
0.02).
25
Timing of health education
Of those participants who received health education, 52/63 reported when it
was delivered. The majority reported that health education was delivered at only one
time-point, with only three patients reporting health education at two time points.
While the majority of patients who received health education within the hospital
reported that it was delivered on admission (22/52), most reported that they would
like health education delivered just prior to discharge or at discharge (see figure 4).
Admission was the third most popular time for receiving health education, and just
after admission the least popular. A number of patients (10.9%) also reported that
they did not want any form of health education during their hospital admission.
When patients want health promotion and when they were delivered
health promotion within the hospital. White fill: When patients wanted to receive
health education, Grey fill: When patients received health education.
Hospital setting
The majority of participants agreed that hospital was a "good place" to
receive health education and that "the hospital should provide patients with details of
community organisations that provide" health education (see Table 4). The largest
proportion of respondents were undecided about whether they would prefer to get
health education from their GP rather than hospital staff.
Just over half of the responders would like the hospital to let their GP know
about their risk factors and the health education they received while in hospital.
While 23.8% did not want their GP to know about their risk factors, only 15.7% did
not want the hospital to inform their GP of the health education they had received.
Out of the 31 disagreeing with letting their GP know about their risk factors, 2 were
smokers, 2 reported consuming alcohol above recommended limits (and 7 had
positive five shot scores). Of the 10 strongly disagreeing, 3 were smokers and 2
misused alcohol (self-reported units and five shot tool). Exactly the same people who
misused alcohol "disagreed"/"strongly disagreed" with their GP being told about the
health education they received, but only 1 smoker (strongly) disagreed with their GP
being told about the health education received.
26
Discussion
The results of this survey indicate that hospital patients view hospitals as an
appropriate place for the delivery of health education for all risk factors. While there
was clear support for screening all adult hospital patients for risk factors, reported
screening was not ideal for any of the risk factors, in particular for diet and physical
activity. There was also considerable demand for health education, but little
provision.
While it appears that the hospital may not be meeting UK public health
requirements or international standards for health education within hospitals [1-4],
some may question whether patients' recall was accurate. Patients' memory may be
affected by the emotional state they were in when information was imparted,
potentially resulting in attentional narrowing or state-dependent learning [22,23].
Memory may also be affected by the perceived importance of information (diagnosis
is viewed as very important and treatment less so), and age-related cognitive
impairments [23]. The communication style of healthcare professionals delivering
health promotion services also affects recall, with patients more likely to remember
medical information if healthcare professionals provide simple to follow, specific
written instructions (rather than general/verbal instructions) [23]. Medical
information is least likely to be recalled, and therefore acted upon, if it is delivered
verbally compared to written/pictorial presentation or a combination of written and
verbal presentation, yet the most frequent form health education took was verbal
advice.
The questionnaire showed good criterion validity as risk factor prevalence in
this sample was similar to national and local profiles for the age group: 22% of the
local population are smokers and 22% are estimated to be obese [24]. In England,
87% of the population does not consume five portions of fruit and vegetables a day,
63% of men and 76% of women are physically inactive [25]; and approximately 20%
of adult in-patients are expected to be hazardous or harmful drinkers [26]. The
percentage of smokers wanting to quit is also similar to previous reports that more
than 70% of smokers wish to quit [27]. There is however little data on the proportion
of people with other risk factors who want to change their behaviour. The
information on the percentage of patients wishing to reduce the amount of alcohol
they drink, reduce their weight, and improve their diet and level of physical activity
27
can be used by hospitals as the basis for developing realistic standards for the
number of patients delivered health education once a risk factor has been identified.
The findings indicate that hospitals should initially aim to deliver health education to
a minimum of 70% of smokers and obese individuals and 50% of people misusing
alcohol, consuming an unhealthy diet and physically inactive.
The timing of health education is also important to patients. While the
majority felt that the time around discharge was the most appropriate period for
health education, those receiving health education reported that it was usually
delivered on admission. This may be because admission is the usual time for
screening of risk factors. However, it is likely that this is not necessarily the optimum
time for health education as patients may be in an unreceptive state due to their
condition and their primary concern may be the immediate improvement in health
(Haynes, 2004 unpublished).
As the purpose of health promotion is to enable people to change a behaviour,
it is important to assess whether the different potential forms of health education
have achieved this. This was evaluated by asking patients how "helpful" the health
education services they received were. While more patients viewed the services as
"helpful" than "unhelpful", given that so few patients received any form of health
education, it is not possible to draw definitive conclusions concerning the
"helpfulness" of the different services. It is recommended that this question remains
as it could provide valuable information about health education services when they
are delivered to a larger number of patients.
Given that primary care is the traditional setting for the delivery of health
education it was surprising that approximately a quarter of respondents expressed
disagreement with the statement "I would prefer health promotion [education] from
my GP rather than hospital staff". While this infers that they would prefer health
education from a hospital, further research is required to verify this finding (e.g.
changing the statement to "I would prefer to get health education from hospital staff
instead of my GP"); and to explore the reasons for this preference. For example, are
hospital staff viewed as more approachable than GPs? Is there a perception of greater
anonymity within a hospital, circumventing embarrassment? Although 1 in 10
respondents expressed that they never wanted health education while hospitalised, it
28
is encouraging that only 3% disagreed with the statement that "hospital is a good
place for patients to receive health promotion [education]".
Disagreement with the statements "I would like the hospital to let my GP
know about my smoking, diet, exercise, and alcohol intake/the health promotion
[education] I received from hospital staff" indicates that there is an objection to the
sharing of information between hospitals and GPs. However, the use of the word
"like" may be the reason, and further research is required to clarify whether there is
an actual objection. If there is a true objection to communication between hospitals
and GPs, it may be difficult to justify automatically informing a patient's GP of their
patient's risk factors and health education delivered, and hospitals may need to ensure
that they have patient consent for sharing this type of information. However an
argument can be made for the transfer of information as being in the public interest
and part of continuing care, and therefore not subject to the need for informed patient
consent [28]. With the drive towards greater collaboration/communication between
services, and the creation of electronic patient records available to all health care
providers, these findings are of concern. Reasons for such an objection also require
clarification. There was no evidence that disagreement with the sharing of
information was related to the presence of risk factors.
Study Limitations
There were some limitations to this study. The sample included patients from
only one hospital and results may therefore not be generalisable to other hospital
populations. The trend towards fewer young men responding to the questionnaire
indicates that the views of this group were not expressed. Young men are less likely
than other populations to respond to questionnaires [29]; and it may be that other
methods such as focus groups are more appropriate for investigating this group's
preferences for health promotion services for lifestyle development. The views of
this population need to be explored as young men consume more alcohol and less
fruit and vegetables than older adults, and are more likely to be smokers [25]; hence
they are at risk of developing chronic diseases. The finding that smokers were less
likely to respond to the questionnaire may have repercussions on the findings
concerning the receptivity of patients to health education. Previous research has
indicated that smokers are less likely to believe that "the way people live affects their
29
health" [16], suggesting they may be less responsive to health education, and that
hospitals may face additional challenges in successfully delivering health education
to smokers.
While there was a reasonable response rate to the questionnaire, the poor
provision of health education meant that statistical analysis of some questionnaire
items was limited by small sample sizes. Improvements in the provision of health
education within hospitals and/or larger sample sizes would improve the situation.
Some questionnaire items require minor changes in wording to allow for definitive
conclusions concerning patients' views on sharing information between healthcare
sectors and preferences for hospitals over GPs for health education delivery.
Conclusion
The findings of this study should encourage hospitals to improve their health
promotion services. Hospital healthcare professionals should be made aware that
approximately a quarter of patients may in fact prefer health education from a
hospital setting rather than their GP, that there is a demand for health education, and
agreement with screening of all risk factors. This information may allay concerns
that some risk factors are too sensitive to address, and challenge the view that lack of
receptivity from patients is an obstacle to delivering health education [30,31]. Health
education is however not for everyone, with approximately 1 in 10 patients choosing
not to receive health education for risk factors while hospitalised, and staff need to
ensure that they respect this desire. The (apparently substantial) challenge now
facing UK hospitals, is how will they meet their patients' demand for health
education? Guidance on how to embed health promotion services within hospitals
has been provided by the WHO HPH [3,4]. While there is some controversy
concerning the "success" of this project/network [32-35], there are examples of
successful health promotion projects within hospitals and some reports of hospitals
becoming health promotion settings [36-38], lessons from which, UK hospitals
would be wise to learn from.
Competing interests
The author declares that they have no competing interests.
30
Authors' contributions
CH was involved in the conception and design of the project. CH collected, analysed
and interpreted the data. CH wrote the entire article.
Acknowledgements
Thanks to the "Health Promotion in Hospitals Steering Group" and Dr Gary Cook,
Stockport NHS Foundation Trust for their contribution to this project. This project
was funded by Stockport NHS Foundation Trust Research & Development Funds.
References
1. Department of Health: Choosing Health. Making Healthy Choices Easier. 2004.
2. Department of Health: Essence of Care. Benchmarks for Promoting Health. [http:/ / www.dh.gov.uk/ en/ Publicationsandstatistics/ Publications/ PublicationsPolicyAndGuidance/ DH_075613] webcite 2006.
3. World Health Organisation Europe: Standards for Health Promotion in Hospitals. [http://www.euro.who.int/document/e82490.pdf] webcite 2004.
4. World Health Organisation: Putting HPH Policy into Action. Working paper of the WHO Collaborating Centre on Health Promotion in Hospitals and Health Care. [http://www.hph-hc.cc/Downloads/HPH-Publications/wp-strategies-final.pdf] webcite 2006.
5. World Health Organisation: Ottawa Charter for Health Promotion. [http://www.euro.who.int/AboutWHO/Policy/20010827_2] webcite 1986.
6. Whitehead D: Health promotion and health education: advancing the concepts. Journal of Advanced Nursing 2004, 47(3):311-320. PubMed Abstract | Publisher Full Text
7. Health promoting Hospitals Network: The Budapest Declaration on Health promoting Hospitals. Budapest: Health promoting Hospitals Network; 1991.
8. WHO – Europe: The Vienna Recommendations on Health Promoting Hospitals. Vienna: WHO; 1999.
9. [http://www.euro.who.int/healthpromohosp] webcite10. WHO: Health Promotion Glossary. section II 1998, 6. 11. Healthcare Commission: Criteria for assessing core standards. Information
for acute services. 2005.12. Haynes C, Cook G: Greater Manchester Health Promotion in Hospitals Audit
report 2007. [http://www.burypct.nhs.uk/538.html] webcite 2007.13. Stange KC, Zyzanski SJ, Smith TF, Kelly R, Langa DM, Flocke SA, Jaen CR:
How Valid Are Medical Records and Patient Questionnaires for Physician Profiling and Health Services Research? A Comparison With Direct Observation of Patient Visits.
14. Medical Care 1998, 36:851-867. PubMed Abstract | Publisher Full Text 15. Wilson A, McDonald P: Comaprison of patient questionnaire, medical
record, and audio tape in assessment of health promotion in general practice consultations.
31
16. British Medical Journal 1994, 309:1483-1485. PubMed Abstract | Publisher Full Text
17. King's Fund: Public attitudes to public health policy. King's Fund publications, London; 2004.
18. McBride A: Health promotion in the acute hospital setting: the receptivity of adult in-patients. Patient Education and Counselling 2004, 54:73-78. Publisher Full Text
19. Mitchell M, Jolley J: Research Design Explained. Third edition. Harcourt Brace College Publishers;
20. Stockport PCT: Stockport Health and Lifestyle Survey. 2005.21. Seppä K, Lepistö J, Sillanaukee P: Five-shot questionnaire on heavy drinking.
Alcoholism: Clinical and Experimental Research 1998, 22:1788-1791. Publisher Full Text
22. Cappuccio FP, Rink E, Perkins-Porras L, Mc Kay C, Hilton S, Steptoe A: Estimation of fruit and vegetable intake using a two-item dietary questionnaire: a potential tool for primary health care workers. Nutr Metab Cardiovasc Dis 2003, 13:12-19. PubMed Abstract | Publisher Full Text
23. Office of the Deputy prime Minister: The English indices of Deprivation. [http://www.communities.gov.uk/documents/communities/pdf/131209.pdf] webcite 2004.
24. Ley P: Memory for Medical Information. Br J Soc Clin Psychol 1979, 18(2):245-255. PubMed Abstract
25. Kessels RPC: Patients' memory for medical information. Journal of the Royal Society of Medicine 2003, 96:219-222. PubMed Abstract | Publisher Full Text | PubMed Central Full Text
26. North West Public Health Observatory: Health Inequalities. [http://www.nwpho.org.uk/information] webcite 2005
27. Allender S, Peto V, Scarborough P, Boxer A, Rayner M: Coronary heart disease Statistics, 2006 edition. [http://www.heartstats.org/datapage.asp?id=5712] webcite British Heart Foundation Health Promotion Research Group Department of Public Health, University of Oxford; 2006.
28. Canning UP, Kennell-Webb SA, Marshall EJ, Wessely SC, Peters TJ: Substance misuse in acute general medical admissions. QJM 1999, 92(6):319-326. PubMed Abstract | Publisher Full Text
29. West R: Smoking: prevalence, mortality and cessation in Great Britain. [http://www.robertwest.asp-host.co.uk/RJWestNet/smokingcessationgb.pdf] webcite 2005.
30. Haynes CL, Cook GA, Jones MA: Legal and ethical considerations in processing patient-identifiable data without patient consent – lessons learnt from developing a disease register. Journal of Medical Ethics 2007, 33:302-307. PubMed Abstract | Publisher Full Text
31. Cunradi CB, Moore R, Killoran M, Ames G: Survey Nonresponse Bias Among Young Adults: The Role of Alcohol, Tobacco, and Drugs. Substance Use & Misuse 2005, 40:171-185. PubMed Abstract | Publisher Full Text
32. Steptoe A, Doherty S, Kendrick T, Rink E, Hilton S: Attitudes to cardiovascular health promotion among GPs and practice nurses. Family Practice 1999, 16:158-163. PubMed Abstract | Publisher Full Text
32
33. Hudon E, Beaulieu MD, Roberge D: Integration of the recommendations of the Canadian Task Force on Preventive Health Care. Family Practice 2004, 12:11-17. Publisher Full Text
34. Anjoulat I, Le Faou A-L, Sandrin-Berthon B, Martin F, Deccache A: Implementing health promotion in health care settings: conceptual coherence and policy support. Patient Education and Counselling 2001, 45:245-254. Publisher Full Text
35. Whitehead D: The European Health Promoting Hospitals (HPH) project: how far on? Health Promotion International 2004, 19(2):259-267. PubMed Abstract | Publisher Full Text
36. Groene O: Evaluating the progress of the Health Promoting Hospitals Initiative: A WHO perspective. Health Promotion International 2005, 20(2):205-207. PubMed Abstract | Publisher Full Text
37. Pelikan JM: Health Promoting Hospitals – Assessing developments in the network. Italian Journal of Public Health 2007, 4(4):261-270.
38. Tountas Y, Pavi E, Tsamandouraki K, Arkadopoulos N, Triantafyllou D: Evaluation of the participation of Aretaieion Hospital, Greece in the WHO Pilot Project of Health Promoting Hospitals. Health Promotion International 2004, 19(4):453-462. PubMed Abstract | Publisher Full Text
39. Polluste K, Alop J, Groene O, Harm T, Merisalu E, Suurorg L: Health-promoting hospitals in Estonia: what are they doing differently? Health Promotion International 2007, 22(4):327-336. PubMed Abstract | Publisher Full Text
40. Johnson A, Baum F: Health promoting hospitals: a typology of different organizational approaches to health promotion. Health Promotion International 2001, 16(3):281-287. PubMed Abstract | Publisher Full Tex
33
BAB IIIKESIMPULAN
Ukuran keberhasilan bidan dalam pelayanan di komunitas/ desa tidak hanya
penurunan AKI dan AKB, tapi juga bangkitnya gerakan masyarakat untuk mengatasi
masalah dan memenuhi kebutuhan kesehatan serta kualitas hidupnya.
1. Pada hakekatnya masyarakat mempunyai hak memperoleh pelayanan yang
berkualitas, sehingga Ibu Sehat Bayi sehat, selanjutnya juga Bangsa yang sehat.
2. Bidan sebagai pemberi jasa harus menjaga mutu pelayanan dan melayani sesuai
kebutuhan (mitra perempuan).
3. Bidan harus tetap meningkatkan kemampuan.
4. Bidan sebagai tenaga kesehatan pada lini terdepan (ujung tombak).
5. Bidan punya kebutuhan dan harapan (kesejahteraan, masa depan dan keamanan).
6. Pemerintah bertanggungjawab menyediakan yankes (Sarana prasana, SDM dll
(Sustainability dan Jamkesmas).
7. Pemerintah dan OP melakukan pengawasan dan pembinaan.
Target global penurunan Angka Kematian Ibu (AKI) MDGs (Millenium
Development Goals sebesar tiga-perempatnya pada tahun 2015. Sementara target
penurunan Angka Kematian Bayi (AKB) dan Angka Kematian Balita (AKABA)
sebesar dua-pertiga. Berdasarkan kesepakat global tersebut Indonesia mempunyai
komitmen untuk menurunkan Angka Kematian Ibu menjadi 102/100.000 Kelahiran
Hidup (KH), Angka Kematian Bayi dari 68 menjadi 23/1.000 KH, dan Angka
Kematian Balita 97 menjadi 32/1.000 KH pada tahun 2015. Jika dilihat dari potensi
untuk menurunkan Angka kematian Ibu (AKI) masih on track walaupun diperlukan
sumber daya yang kompeten (Pedoman Pengawasan Wilayah Setempat Kesehatan
Ibu dan Anak, Depkes RI. 2009).
34
DAFTAR PUSTAKA
Kemenkes RI, 2010, Pedoman Bidan Koordinator. Jakarta: Bina Husada, Kemenkes RI
Kementrian Pendidikan Nasional, 2010, Membangun Jejaring Kerja Kemitraan, Jakarta: Direktorat Jenderal Pendidikan Nonformal dan Informal.
UNFPA. 2006, Kebijakan dan Strategi Nasional Kesehatan Reproduski di Indonesia, Jakarta: UNFPA.
Kemenkes RI. 2011, Pedoman Pemantauan Wilayah Setempat Kesehatan Ibu dan Anak, Jakarta: Bina Husada.
Haynes, Charlotte L, 2008, Health promotion services for lifestyle development within a UK hospital – Patients' experiences and views. United Kingdom: BMC Public Health.
35





























