Embed Size (px)
Citation preview

TUMORS OF THE SPINAL CORDI
1. In tramedullary Tumors
FRA~K PADBERG, M.D., and LOYAL DAVIS, M. D.
"' The results of lhe operative treatment of tumors of the spinal cord and membranes are as brilliant as any obtained in the entire realm of surgical therapy."
I N the period 1925 to 1951 , 143 patients were t reated for spinal cord tumors. Of
the total of 143, 25 were cases of int ramedullary tumor, 51 of subdural tumor ; in 67 of the cases the tumor occurred in the extradural space (Table I ).
Intramedullary Tumors are usually · gliomas although other types have been recorded (7). The cellular components of the spinal cord are essentially similar to those of the brain and the gliomas of the spinal cord correspond histologically with tumors arising from the substance of the brain. Nineteen of the 25 int ramedullary tumors were ependymomas. One patient had an astrocytoma and another had an oligodendroglioma. Five patients had "seeded" medulloblastoma metastases. In the brain the astrocytoma forms 16.6 per cent, the oligodendroglioma 2.5 per cent and the ependymoma 2 per cent of the gliomas, a completely contrary distribution.
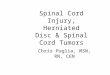
The ependymomas are composed essentially of adult cells, \rhich originate from the ependymal cells lining the cent ral canal of the spinal cord. Grossly these tumors are brownish-purple to grey in color ; usually soft, although occasionally, tKey are fleshy and tough. Microscopically, thi neoplastic tissue is formed into generously cellular and vascular sheets interspersed wi th varying amounts of fi brous stroma. Small groups of cells are characteristically arranged into rosettes radially arranged about blood \"essels (fig. 1).
The ages of the 19 patients varied from 21 to 57 years; 5 \\'ere females and 14 males. A graph of the distribut ion of the e ependymomas indicates that there
IFrom the D epartm ent of Surgery. Nort hwestern l:ni"ersity ~I edica l School. Received for p ubli ca tion , i\Iarch II , 1952.
Charles A. Elsberg
\\'as a definite predeliction for them to occupy the superior and inferior poles of the spinal cord. The histological background for their occurrence in the inferior pole of the spinal canal has been well described (5). The greater number of intracranial ependymomas are ident ified in the posterior fossa (2).
1'\\' 0 of the 19 patients had tumors which had invaded the high cervical spinal cord and the 4th Yent ricle. One patient had the init ial symptoms of a posterior fossa tumor 84 months before operation, \"hich " 'ere followed by signs of upper cervical spinal cord compression. Another patient had predominantly spinal cord signs for 26 months and on examination had a papilledema. These b \'o tumors "'ere \ridely removed at operation. Both patients ha\'e an ataxic gait but both are able to carryon their work as house,,·i,·es.
Six patients had an ependymoma in the cervical spinal canal. Initially, they had symptoms of sensory loss soon followed by a "'eakness in the upper extremities. The roentgen ray films of the cervical spine of these 6 patients "'ere normal. All of the patients had a subarachnoid space block. In each instance the spinal cord "'as enlarged and dilated tortous posterior spinal vessels were present. A dorsal myelotomy was performed \"hich exposed a cyst ic cavity lined with the tumor tissue. One patient had been operated upon 5 years previously and although an arachnoidi tis \\'as recognized at that time, there was no surface manifestation of a tumor. Three patients became paraplegic sometime before operation and remain unimproved. One of these patients \\'as followed for 2 years after operation " 'ithout signs of progression of the symptoms; another
204

PADBERG AND DAVIS- TUMOR OF ~PI~AL CORD 205
TABLE I
Type of Tumor Intramedullary
Ependymoma 19 Astrocytoma I Oliogodendroglioma . . 1 Medulloblastoma . ... . . .. . 4 Meningioma .. . ........... Keurofibroma . . .. . . . . ... . Hemangioma .. ..... . . . . ... .. Hemangioblastoma :\ eurolipoma ... .. . . . .. N" eurofi brosarcoma ..... . . . . . Meningeal Sarcoma . . . . . . . . . . Arachnoidal Cyst . ... .. . . .. .. Pheochromocytoma Carcinoma . . ... . .. . . .. . . . . . . Sarcoma Lymphosarcoma . . . . .. . .. . .. . Mult iple Myeloma .... Hodgkins Disease ... Giant Cell Tumor . . . . . . . . . . . Fibroma .... ..... .... Tuberculous Granuloma
25
Fig. 1. Photomicrograph of an intramedullw·y ependymona which shows the arrangement of cells with dark-stained nuclei in pseudo-rosette fonnation toith a fairly abundant connective tissue stroma. (H &: E x 212).
Location Subdural Extradural Total
19 1 1 4
28 5 33 11 2 13 6 5 11 1 1 1 1 1 1 I 1 1 1 1 1
15 15 11 11 8 8 7 7 7 7 4 4 2 2 1 1
51 67 143
Fi g. 2. Photomicrograph of an intramedullary ependymomainmdingtheduramater. (H &: Er I25) .

206 QUARTERLY BULLETIN, N.U.M.S.
had no progression of symptoms for 11 years but then suddenly, \\'ithin a year, developed a complete loss of motor function in a previously weak upper extremity. One other patient could not be examined following discharge from the hospital. Three patients \\'ere not paraplegic at the time of operation and one patient died one year follo\\'ing operation \\'ith sign of a rapidly progressing lesion. Another patient \\"as relieved of his symptoms for 2 years and then over a period of 3 years had a progressive paralysis, deyeloped intracranial symptoms, and died. The other patient had complete relief from her symptoms and lI'as able to carryon her normal duties for 2 years. Her symptoms then recurred and she is noll' incapacitated.
Three patients had ependymomas in the thoracic spinal canal. 1'\\'0 of these had a spastic paraplegia and there was a ensory level at the time of surgery \\'hich
had developed oyer a period of 16 and 26 months. At operation, there was a fusiform enlargement of the thoracic spinal cord from which tumor tissue wa removed through a dorsal incision. Neither patient had improvement in the immediate postoperative period. A third patient had a 6-month history of weakness in one lower extremity follo\\'ed by pain in the sciatic distribution. Myelography \\"as peJformed and a herniated nucleus pulposus was removed. Postoperatively he \\"as incontinent, developed a spasticity in both 101l'er extremities and had a sensory 10 s. Three \\'eeks after the hemilaminectomy, he was operated upon again and a large ependymoma was partially removed. The patient was unimproved and has remained paraplegic for 2 years.
These patients with ependymomas in the spinal cord complained initially of a subjective sensory disturbance and/ or \\'eakness of the extremities. Pain was not a frequent early complaint. All had a relatively long duration of symptoms before operation and several lI'ere treated for other diseases before the diagno is \\"as suspected and neurological consultation sought. The predominating clinical feature was an alteration of sensation, which was frequently disassociated, and muscular weakness greater in the proximal
segments than in the more distal segments. The surgical treatment consisted of the midline dorsal myelotomy which extended into the mass of the tumor throughout its length and which allowed the tumor to extrude and be removed. Cystic cavities within the tumor were usually present. The most extensive removal of an ependymoma from the entire length of the spinal cord has been reported by Hon'ax and Henderson (3).
In general, these patients were rehabilitated fairly well immediately folio\\'ing operation but they had a markedly rapid progressive decline once a recurrence of symptoms had developed, as a brief recital of a case history will illustrate.
CASE REPORT
W.P . had first complained of a numbness and tingling sensation in the fingers of his left hand in 1932. This subjective ensation had slowly progressed and extended to the hand, arm, and elbo\\' . This was accompanied by a \\'eakness of the left hand. In the latter part of 1939, he had noted the beginni ng of a similar sensation in the fingers of the right hand and a vice-like sensation about the left side of the upper che. t.
Examination: April , 1940. There was no weakness or atrophy of the lower extremities. He had an atrophy of the muscles about the shoulder girdle, which was most severe on the left. Movements of the fingers of the left hand were clumsy and he had great difficul ty with coordinated movements of the left hand. When he coughed he could produce a severe radiating pain in both arms. The deep tendon reflexes in the upper extremities were depressed but equal. The patella I' tendon re flexes were equal and active. The cremasteric reflexes were brisk. Sensation for pin prick was normal in all four extremities but position sensation was disturbed in the fingers of the left hand . Spinal puncture demonstrated a complete subarachnoid space block but the spinal fluid was clear and colorles . The total protein of the spinal fluid was elevated to 300 mg. %. Roentgen-ray films of the cervical and thoracic spine were normal.
Operation: May 16, 1940. A laminectomy was performed which extended from C-4 to T-2. The blood vessels on the posterior surface of the spinal cord were enormously dilated and varicose. Directly beneath the 6th cervical lamina the spinal cord wa enlarged and soft over an area of 2Yz ems. The line of demarcation above and below this swollen segment was striking. Two cc. of dark yellow blood-tinged fluid was aspirated 'from the enlarged segment of the cord. The spinal cord was incised in the posterior median septum and a cavity which was lined with a purple colored tumor was found. This tumor was widely removed with moist cotton sponge dissection . The patient had a rapid re-

PADBERG AND DAVIS- TUMOR OF SPINAL CORD 207
covery following operation and was well rehabili tated to his work . He remained well until 1942 when he had a recurrence of his previous symptoms. He became blind and quadriplegic six months before his death in July, 1945.
Five patients were primarily treated early in the course of their symptoms for an ependymoma about the cauda equina, conus medullaris and / or the filum tenTIinale. These patients had the prominent first symptom of low back and unilateral or bilateral sciatic pain which was followed by a weakness and sensory loss in one or both lower extremities. Four patients had a subarachnoid space block with xanthochromic fluid and an increase in the spinal fluid total protein. Myelography was perfOlmed upon 3 patients to localize the tumor.
Two of these 5 patients had a swollen and enlarged spinal cord and conus. A dorsal myelotomy was perfoi'med and a dark purple, tough tumor was re·· moved in each instance. One patient was followed postoperatively for 12 months without signs of progression or improvement over his preoperative status. The other patient was unimproved for 18 months and then over a period of one month developed. intracranial symptoms and died. Both of these patients had postoperative roentgen-ray therapy. The other 3 patients had a tumor of the cauda equina with a soft, purple, mulberry-like mass among the caudal nerves. These tumors were large, contained within the dura mater, and were covered by a thick opaque arachnoid. These three tumors were, grossly, completely removed . After operation these patients did very well and have been followed for 12, 30 and 42 months. They were well rehabilitated and all 3 are at work. Two of the pat ients had some urinary difficulty for several months which subsided.
Two additional patients were t reated for a cauda equina ependymoma who had received primary treatment elsewhere early in the course of their symptoms. Both patients had a flaccid paraplegia and both had roentgen-ray t herapy following operation. One patient had a good recovery for 2 years, the other for 6 months, after which each had a rapid onset of paralysis.
One man had a large necrotic tumor
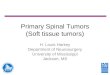
Fig. 3. Photomicrograph of an intramedullw'Y astrocytoma (H & E x 735).
mass under the lumbodorsal fascia, replacing the muscles, and invading the caudal nerves. The other patient had a large tumor, with a large cystic cavity. This tumor had invaded the dura mater and the caudal nerves (fig. 2). These tumors were widely removed. Neither of these 2 patients were improved neurologically postoperatively. One patient died 9 months after operation ; the other patient had a cordotomy 9 months after operation and could not be follo\\'ed after leaving the hospital.
The patients with ependymomas about the cauda equina and filum terminale had complained of a pain of a radicular character early in the course of their disease. At operation, these tumors extended, following the lines of least resistance, between the nerve roots of the cauda equina, upward over the lower port ion of the cord and downward into the sacral canal.
Another patient had a suboccipital craniectomy for an ependymoma of the fourth ventricle 4 years preceding the onset of spinal cord symptoms. He had

208 QUARTERLY BULLETIN, N.U.M.S.
r
I
f , tI f f It I ., I I II II ' f " "I ' " ITT,... .. It , If , , • , If' II , , , I , II , I II I I ; ' II I II \I I I I I 1 : I I I I II I I I II ; III 1 III I I f'l ' I Iii i d I I "I I I I . . I .
'I f I, I I . t I ~6 _ .1_ 71 __ ~ Ji~_1 -.91 1'0 ! 1.1 ' 1 2 I I i~ I _~ , i
Fig. 4. Gross appeamnce of an intramedullary oligodendroglioma.
received roentgen-ray irradiation immediately after the cranial operation. This was repeated 3 years later for a recurrence of his intracranial symptoms and relieved his symptoms. He then had a rapid onset of a spastic paraplegia ,,·ith a sensory loss below the 7th thoracic segment. He had a subarachnoid space block "'ith xanthochromic fluid. Several areas of fullness and fusiform enlargement of the thoracic spinal cord were seen at operation. He died one year later. The autopsy shO\\'ed an extensive tumor " 'hich involved the dura mater and all divisions of the spinal cord. Tumor implants were found throughout the spinal subarachnoid space and the tumor \\'as identified in the lateral vent ricles.
We haH treated one patient \\'ho had an intramedullary cervical and medullary astrocytoma (fig . 3). He had progressive symptoms for 1 year. These had started initially \\·ith numbness in the left hand. He had a " 'eakness and a hypesthesia of the left extremities and a profound loss of position sensation in the left hand and arm. These complaints "'ere accompanied by occipital headaches. Pneumoencephalography demonstrated enlarged lateral ventricles, the left larger than the righ t. Radioisotope localization demonstrated a concentration of the dye in the posterior fossa. A suboccipital craniectomy and
cervical laminectomy uncovered a tumor of the spinal cord and lo,,'er portion of the medulla. This \\'as on the left and extended across the mid-line. The fourth ventricle \\'as filled by the tumor mass which was partially removed. Following operation he was symptomatically improved. He has been able to go back to some of his duties but he has had no remarkable improvement in his motor strength. Roentgen-ray t herapy was given on 2 different occasions, at an interval of 8 months. He has survived for 15 months, is still living and has shown no signs of progression. The microscopic characteristics of these tumors are similar to the astrocytomas in t he brain.
One patient had an oligodendroglioma of the spinal cord. Russell and Bucy (6) revie"'ed the li terature finding 6 previously reported case histories of patients with an oligodendroglioma of the spinal cord. They added one case which they had treated surgically.
CASE REPORT
D.l(. ",as 27 years of age and had symptoms for 4 years. She had initia lly complained of a dull aching pain over the upper t horacic spinous processes. She also gave a history of a slapping gait wit h the left foot for 2 years. She had a minor fall on the buttocks and this was followed by numbness of the right toe. Several days following this fall, her gait became more unsteady and clumsy. She was unable to make her feet move

PADBERG AND DAVIS-TUMOR OF SPINAL CORD 209
as she in tended without watching them. She had noted a subjective sensory loss of slow progression in the lower extremities. She had been treated for multiple sclerosis with typhoid vaccine and histamine. In January 1945, she had progressive weakness and Glumsiness of both hands and several episodes of sphincteric disturbances.
Exam.ination: April, 1945. She had a slight spasticity of the left leg on passive movements. There was a weakness, without atrophy of the 10"'er extremities, most marked in the flexors of the ankles, legs and thighs; the left extremity was the more involved. She had weakness, ataxia and rlumsiness of both upper extremities. The small hand and deltoid muscles were weak, the left more so than the right . The biceps, triceps, radial and ulnar reflexes were absent. The achilles and patella r reflexes were brisk and more active on the left. A sustained clonus was elicited at the left patella. An exhaustible clonus was present at the right patella and left ankle. Bilateral Babinski signs were elicited. The abdominal reflexes were absent. An alteration of a ll modal i ties of sensation was found below the 7th cervical dermatome. An analgesia was present on the right side of the chest and the loss of pain sense was not so critical and more di ffi cul t to evaluate on the left. There was a loss of vibratory sensation in the feet and this was diminished as high as the 6th thoracic segment. Position and joint sensation were lost in the feet and ankles. A sweating test showed perspiration down to the 10th thoracic segment and in the lower sacral segments but not over the legs or the thighs. A
Fig. 6. Photomicrograph of (m intmcTanial medulloblastoma which has invaded the SlJinal cord (H &Ex125) .
complete subarachnoid space block was found on spinal puncture. The total protein of the spinal fluid was 272 mg. %. Roentgen-ray films of the cervical and dorsal spine were normal as was a graph of the interpeduncular spaces from C-2 to T-12.
Oplfration: April 12, 1945. A laminectomy was performed from C-4 to T-l. The bone of the 5th cervical lamina was thinned. Dilated veins were seen under the dura, before it was opened, on the posterior surface of the spi nal cord. The cord was tightly pressed against the dura except beneath the 4th cervical lamina. The cord was soft and bulging. An incision was made into the spinal cord in the posterior medium septum from the level of C-5 to T-l. A purple, firm, elastic yet soft tumor partially extruded through the entire length of the incision. This tumor Im s dissected free with traction sutures and moist cotton sponges. The lower extent of the tumor " 'as reached and the tumor successfully removed. (figs.4 and5). The upper extent of the tumor broke from the main mass and a portion of this part of the tumor remained. This portion of the tumor was not pursued since possible damage to the cord at the site of the origin of the phrenic nerve supply was to be a voided.
Course: This patient made an excellent recovery . One month following operation she was able to walk. Eleven months later she was at work as a secretary. She had no gross evidence of muscular weakness but she did complain of urgency on urination. Fifty-four months after operation she remains well.

210 QUARTERLY BULLETI N, N.U.M.S.
Fig. 7. Gross appearance oj spinal curd and cauda equina which shows implants oj medulloblastoma.
Four patients have beeri treated for "dropped" metastases from a medulloblastoma in the int racranial posterior fossa. These patients \\·ere in the 25 to 30 year age group. The time interval from the attack on t he primary tumor to the development of spinal cord symptoms varied from 6 to 15 months. All 4 patients developed a paraplegia from 1 week to 5 months following the onset of the symptoms of spinal cord compression .
Spinal roentgen-ray therapy, alone, was given to one patient with some relief of his symptoms. The 3 other patients were operated upon and roentgen-ray therapy was given post-operatively.
Pathologically these spinal tumors were fi at, verrucose, grey-red masses which were vascular and attached to the cord by vessels. They greatly compressed and replaced the spinal cord (fig . 6). Two patients had numerous firmly attached vascular tumor masses about the roots
of the caudaequina (fig. 7). Thesepatients had little or no improvement after operation and / or roentgen-ray therapy.
SUMMARY
Nineteen patients with ependymomas, 1 Patient with an astrocytoma, 1 patient with an oligodendroglioma of the spinal cord and 4 patients who had medulloblastoma metastases have been among the group of intramedullary spinal cord tumors.
The ependymoma was the most frequently encountered intramedullary spinal cord tumor and in this group of patients the tumors were more commonly located at the superior and inferior poles of the spinal canal.
The one patient in this series with an oligodendroglioma had an excellent postoperative recovery, is well rehabilitated to her regular work and remains well 54 months following her operation.
In patients with medulloblastoma metastases the onset of the symptoms of spinal cord compression, once started, was rapid varying from 1 week to 5 months. These patients had little or no improvement after operation and / or roentgenray therapy.
Despite their varied pathological classification, these tumors are gliomatous in origin. Often, they are fairly well circumscribed, although not definitely encapsulated, and are associated with a cystic cavity. This facilitates attack on the tumor by allowing aspiration of the cyst , dorsal myelotomy into the tumor throughout its extent, extrusion, dissection and removal of the tumor. However, it is practically impossible to remove completely a gliomatous tumor of the spinal cord without damaging previously uninvolved fiber tracts.
The predominating clinical feature of an intramedullary tumor is an alteration of sensation, which is frequently disassociated, and greater muscular weakness in the proximal segments than in the more distal segments.
R E FER ENCES
1. Davis, L., Martin, J ., Padberg, F . and Anderson, R. K.: A Study of 182 Patients with Verified Astrocytoma, Astroblastoma and

PADBERG AND DAVIS-TUMOR OF SPINAL CORD 211
Oligodendroglioma of the Brain, J. Neurosurg., 7:299-312, 1950.
2. Davis, L., Martin, .J. and Ruge, D.: Ab~·aha.m Levinson Anniversary Volume, StudIes III
Pediatrics and Medical History, New York Froeben Press, Inc., 1949.
3. HOl'I'ax, G. and Henderson, D. G.: Encapsulated Intramedullary Tumors Involving the whole Spinal Cord from Medulla to Conus: Complete Enucleation with Recovery, Surg., Gynec. & Obst., 68:814-819, 1939.
4. Kernohan, J. W. and Fletcher-Kernohan ,
E. M.: Ependymomas, A. Research :\erv. & Ment. Dis., Proc., 16:182-209, H)37.
5. Kernohan M. W., Woltman , H. W. and Adson A: W.: Gliomas Arising from the Regio~ of the Cauda Equina, Clinical, Surgical and Histologic Con iderations, Arch.
. Neurol. & Psychiat., 29:287-305, 1933. 6. Russell J. R. and Bucy, P . C.: Oligodendro
glioma 'of the Spinal Cord, J. l\euroslll'g., 6:433-437, 1949.
7. Taniguchi , T. and Mufson, J. A.: Intradural Lipoma of the Spinal Cord, J. :\eurosurg., 7:584-586, 1950.