Embed Size (px)
Citation preview
Turbinate Dysfunction
Shashidhar S. Reddy, MD, MPH
Faculty Advisor: Matthew Ryan, MD
The University of Texas Medical Branch
Department of Otolaryngology
Grand Rounds Presentation
March 12, 2003
Overview
Focus on Nasal Obstruction
Anatomy
Histology and Physiology
Evaluation of Nasal Obstruction
Turbinate Disorders
Medical Management
Surgical Management
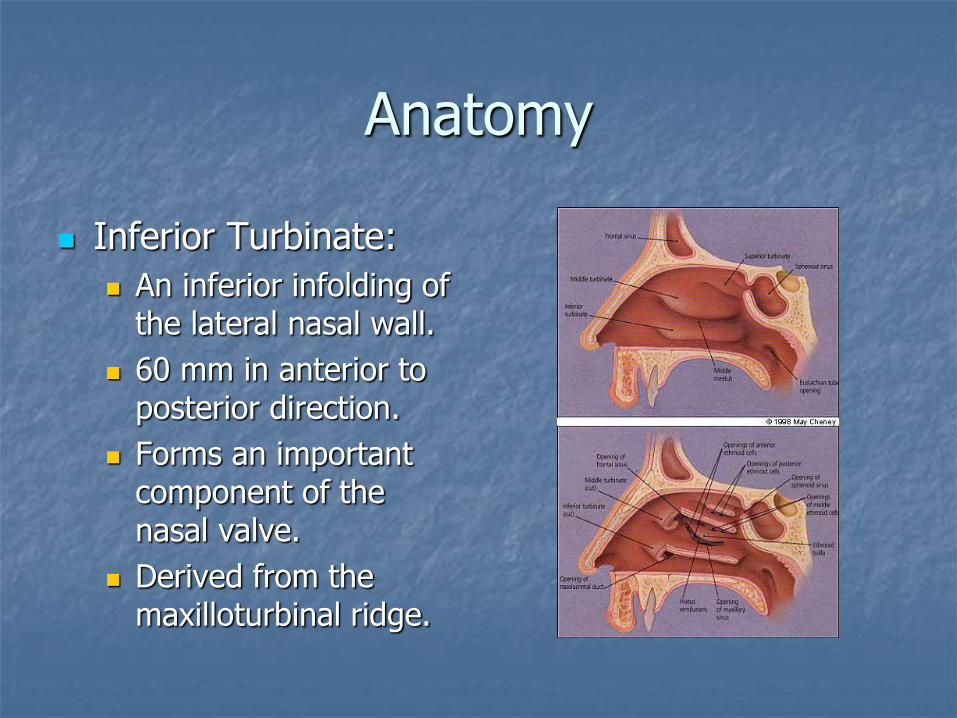
Anatomy
Inferior Turbinate:
An inferior infolding of the lateral nasal wall.
60 mm in anterior to posterior direction.
Forms an important component of the nasal valve.
Derived from the maxilloturbinal ridge.
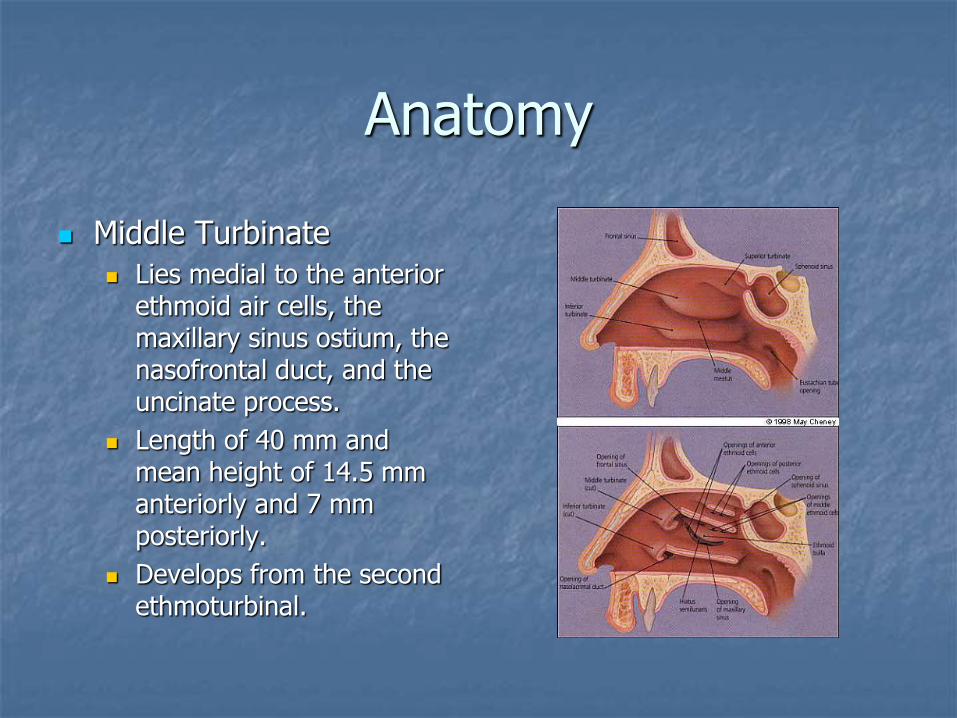
Anatomy
Middle Turbinate
Lies medial to the anterior ethmoid air cells, the maxillary sinus ostium, the nasofrontal duct, and the uncinate process.
Length of 40 mm and mean height of 14.5 mm anteriorly and 7 mm posteriorly.
Develops from the second ethmoturbinal.
Anatomy
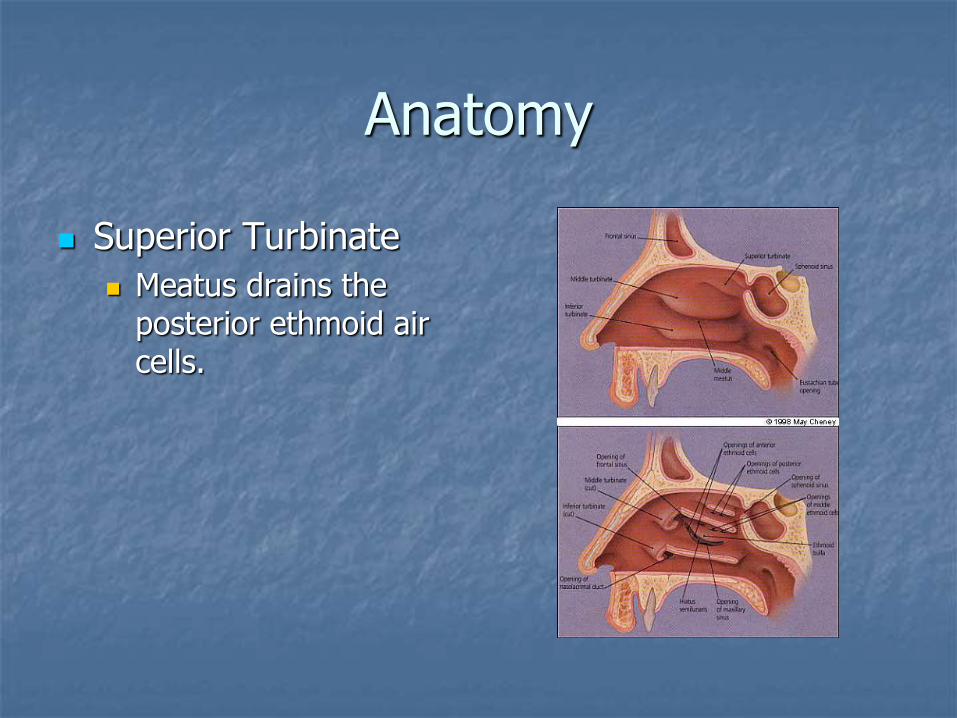
Superior Turbinate
Meatus drains the posterior ethmoid air cells.

Anatomy
Nasal Valve
External Nasal Valve
Boundaries include:
lower lateral cartilages
Soft tissue alae
Membranous septum
Sill of the nostril
Can be site of obstruction (e.g. s/p rhinoplasty)
Anatomy
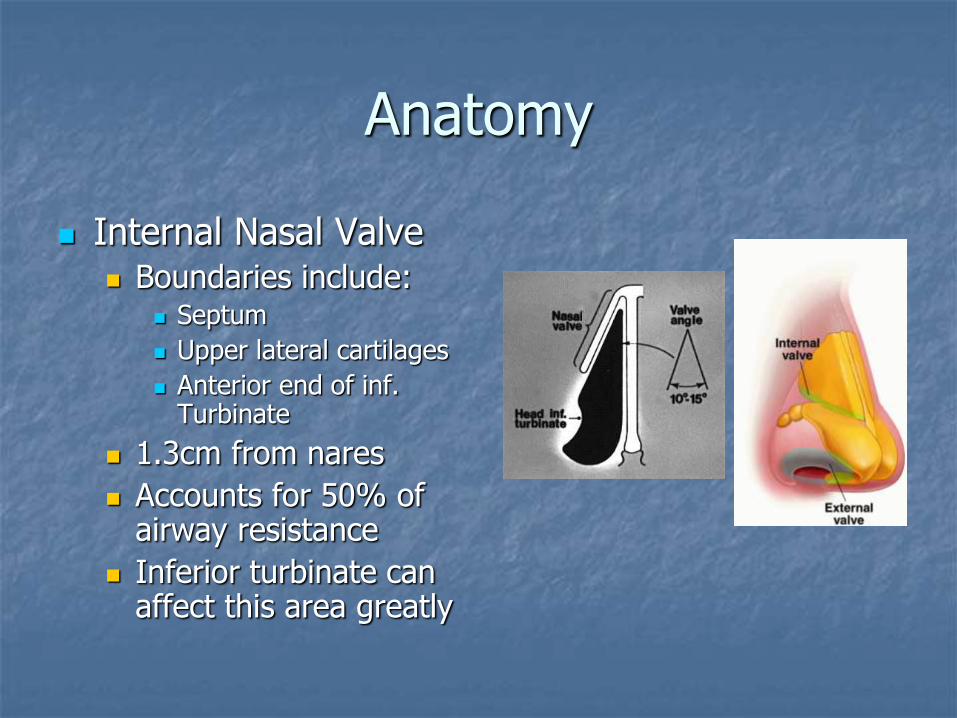
Internal Nasal Valve Boundaries include:
Septum
Upper lateral cartilages
Anterior end of inf. Turbinate
1.3cm from nares
Accounts for 50% of airway resistance
Inferior turbinate can affect this area greatly

Histology
Three layers of Turbinates
Medial thin mucosa
Bone
Lateral thick mucosa
From: Berger: Laryngoscope, Volume 111(12).December 2000.2100-2105
Histology
Mucosa
Pseudostratified columnar ciliated respiratory epithelium
Goblet cells produce salts, glycoproteins, polysaccharides, lysozymes.
Complex array of arteries, veins, and venous sinusoids.
Lamina Propria contains the above tissue.
Physiology
Functions of the Nose Related to Turbinates:
Airway
Filtration – most particles > 30m
Heating – to 31-37 degrees
Humidification – to 95%
Physiology
Chemical or microbial irritation leads to rapid inflammatory response.
Nasal cycle lasts 2-6 hrs, occurs in 20-80% of people.
Sympathetic nervous system increases vascular resistance
Parasympathetic nervous system (vidian nerve) relaxes capacitance vessels.
Sensory receptors = temperature receptors
Evaluation of Patients
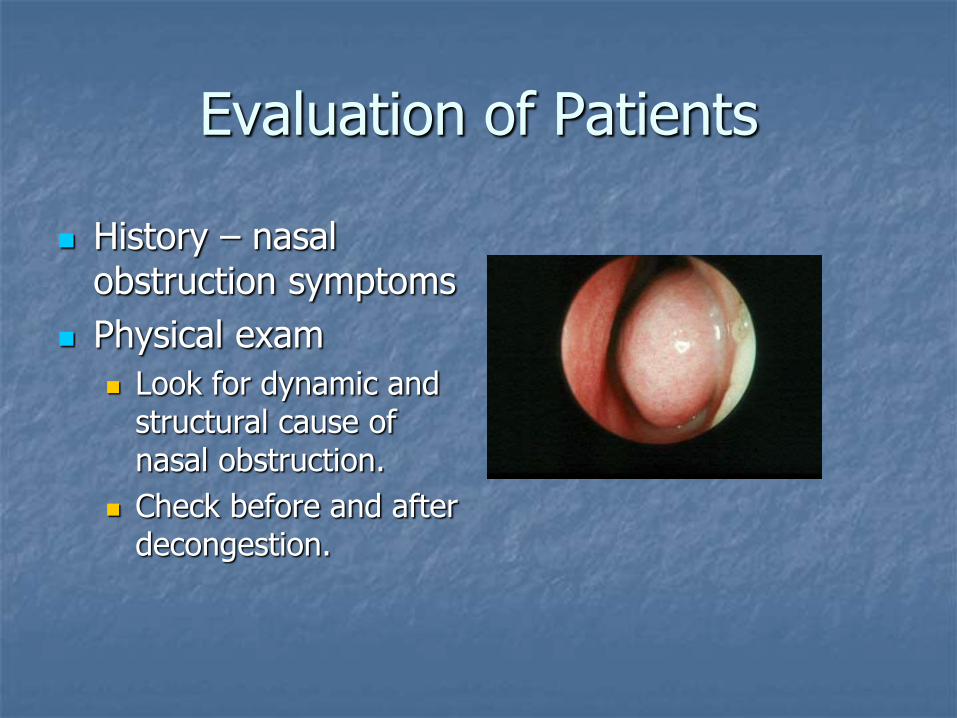
History – nasal obstruction symptoms
Physical exam
Look for dynamic and structural cause of nasal obstruction.
Check before and after decongestion.
Evaluation of Patients
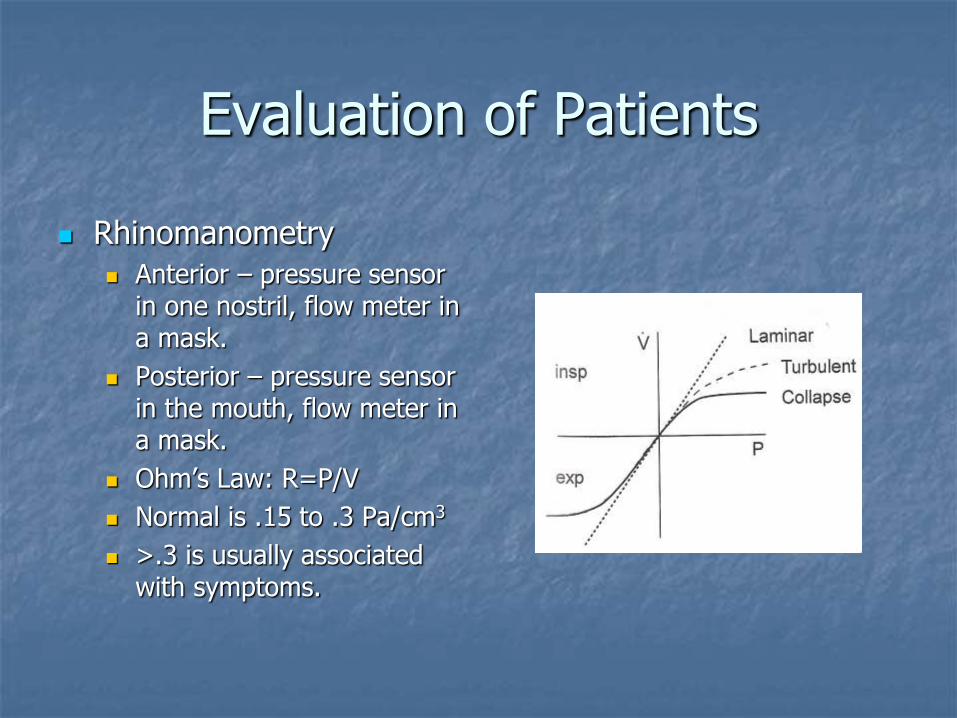
Rhinomanometry
Anterior – pressure sensor in one nostril, flow meter in a mask.
Posterior – pressure sensor in the mouth, flow meter in a mask.
Ohm’s Law: R=P/V
Normal is .15 to .3 Pa/cm3
>.3 is usually associated with symptoms.
Evaluating Patients
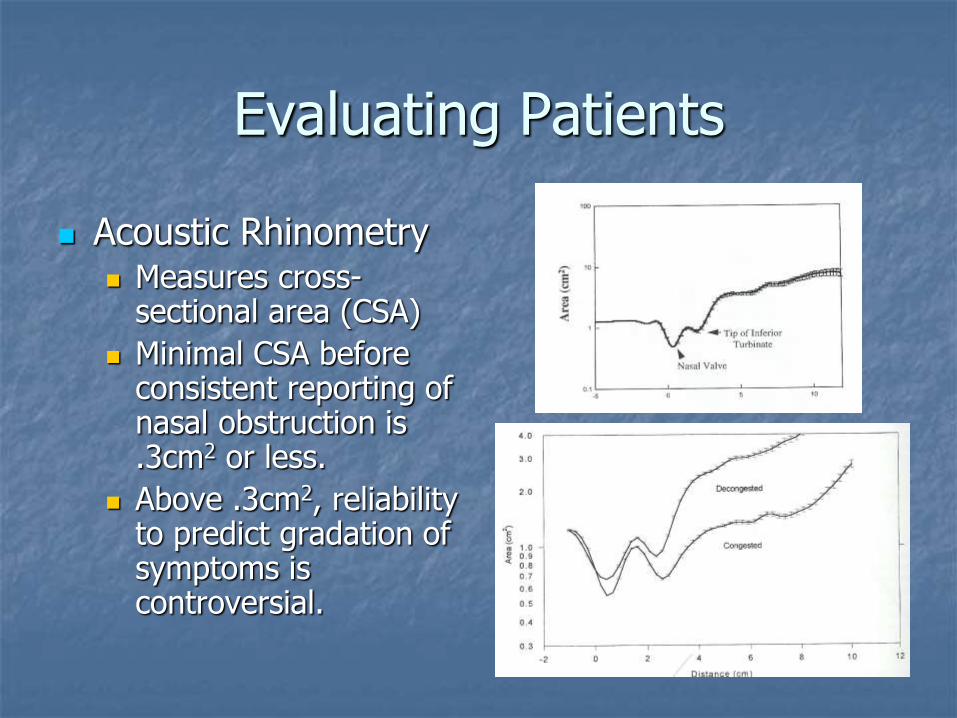
Acoustic Rhinometry Measures cross-
sectional area (CSA)
Minimal CSA before consistent reporting of nasal obstruction is .3cm2 or less.
Above .3cm2, reliability to predict gradation of symptoms is controversial.
Evaluating Patients
Other tests:
Olfaction tests
Nasal smear
Tests of humidity and heating
Turbinate Disorders
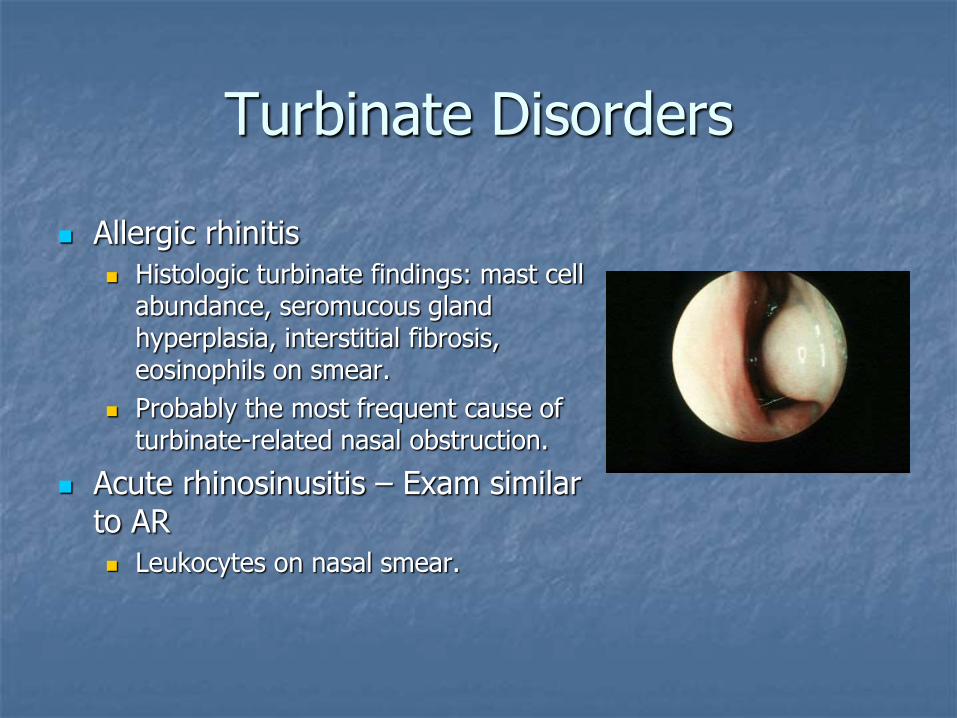
Allergic rhinitis
Histologic turbinate findings: mast cell abundance, seromucous gland hyperplasia, interstitial fibrosis, eosinophils on smear.
Probably the most frequent cause of turbinate-related nasal obstruction.
Acute rhinosinusitis – Exam similar to AR
Leukocytes on nasal smear.
Turbinate Disorders
Chronic Rhinosinusitis
Leads to longstanding changes in mucosa.
Fibrosis, polyposis.
Vasomotor Rhinitis
Nasal congestion, rhinorrhea only
Drug Induced Rhinitis
Turbinate Disorders
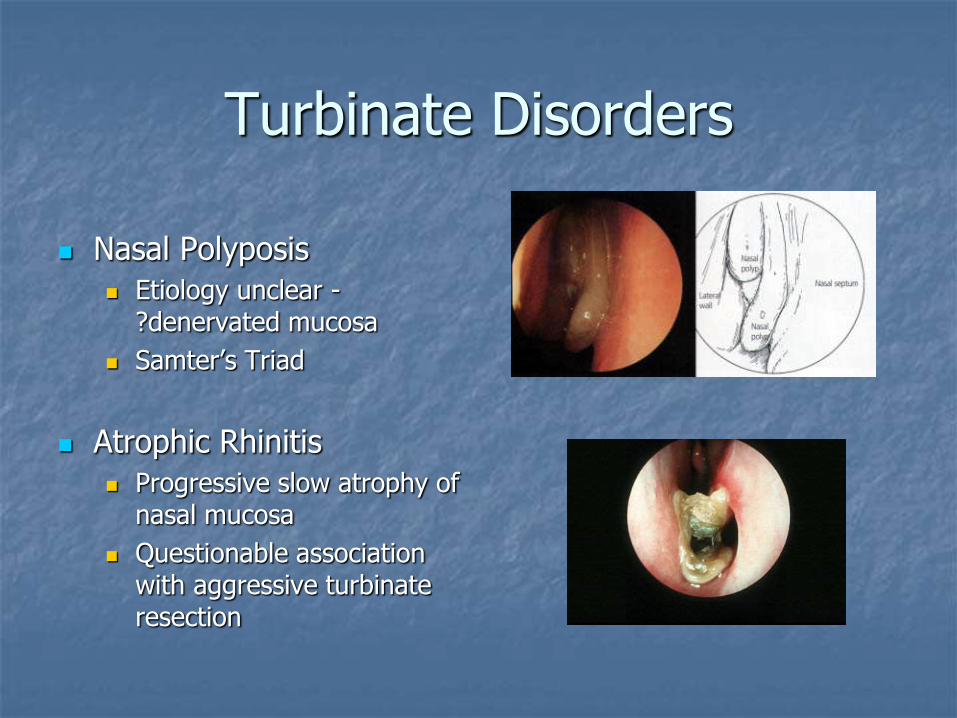
Nasal Polyposis
Etiology unclear - ?denervated mucosa
Samter’s Triad
Atrophic Rhinitis
Progressive slow atrophy of nasal mucosa
Questionable association with aggressive turbinate resection
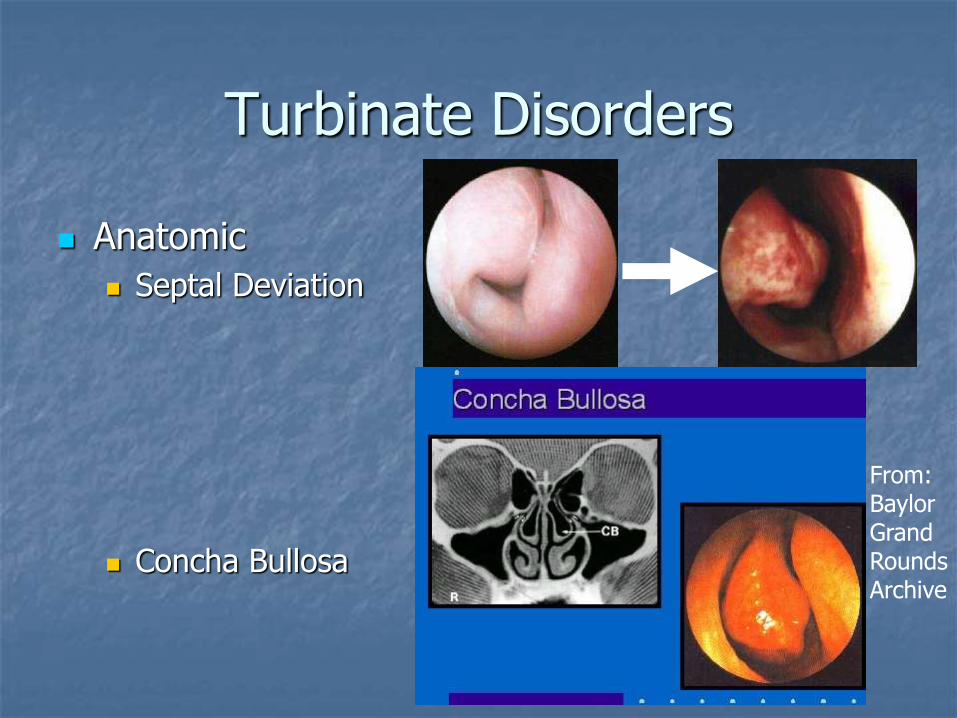
Turbinate Disorders
Anatomic
Septal Deviation
Concha Bullosa
From: Baylor Grand Rounds Archive
Turbinate Disorders
Anatomic
Paradoxical middle turbinate curvature in 10-29%
Synechiae, polypoid changes

Medical Management
Allergic Rhinitis – Nasal steroids with oral and/or topical antihistamines, systemic decongestants.
Drug induced rhinitis – cessation of topical medicine and switch to steroids.
Nasal Polyposis – systemic steroids, topical steroids.
Rhinosinusitis: Antibiotics
Surgical Management
Total inferior Turbinectomy
Benefits:
Most effective in terms of LONG TERM improvement of airway
Ophir et al followed 186 patients for 10 years and showed that 82% showed subjective improvement, 95% had widely patent airways
Surgical Management
Total Inferior Turbinectomy
Disadvantages –
Postoperative hemorrhage rate of 5-8%
Nasal crusting, sometimes lasting for months, up to 15% at one year, in a study by Mabry et al (40pts. followed for one year)
Synechiae 6-12% of the time
Atrophic rhinitis? Classic study by Moore shows rate of 66% in group of 18 pts at 3-5 years. Six ENTs in Australia reported none in 17,000 cases. (Fry et al 1992)
Surgical Management
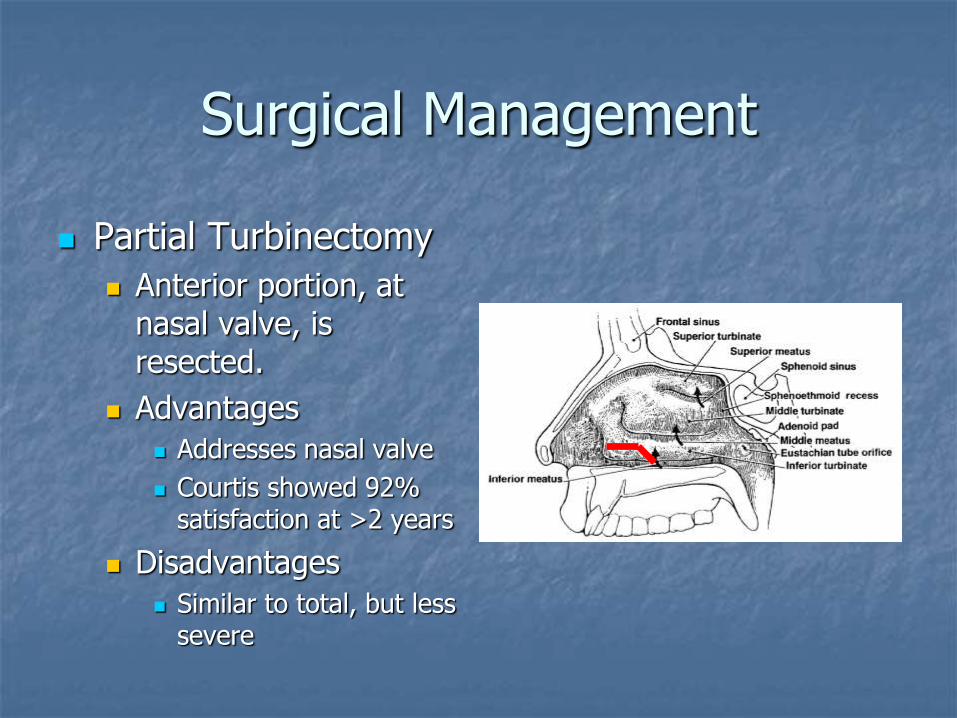
Partial Turbinectomy
Anterior portion, at nasal valve, is resected.
Advantages
Addresses nasal valve
Courtis showed 92% satisfaction at >2 years
Disadvantages
Similar to total, but less severe
Surgical Management
Submucous Resection
Advantages
Decreased risk of hemorrhage
Preserves mucociliary clearance and air conditioning
Disadvantages
Technical difficulty
Tendency to relapse – 25% in a 1988 study by Mabry et al
Surgical Management
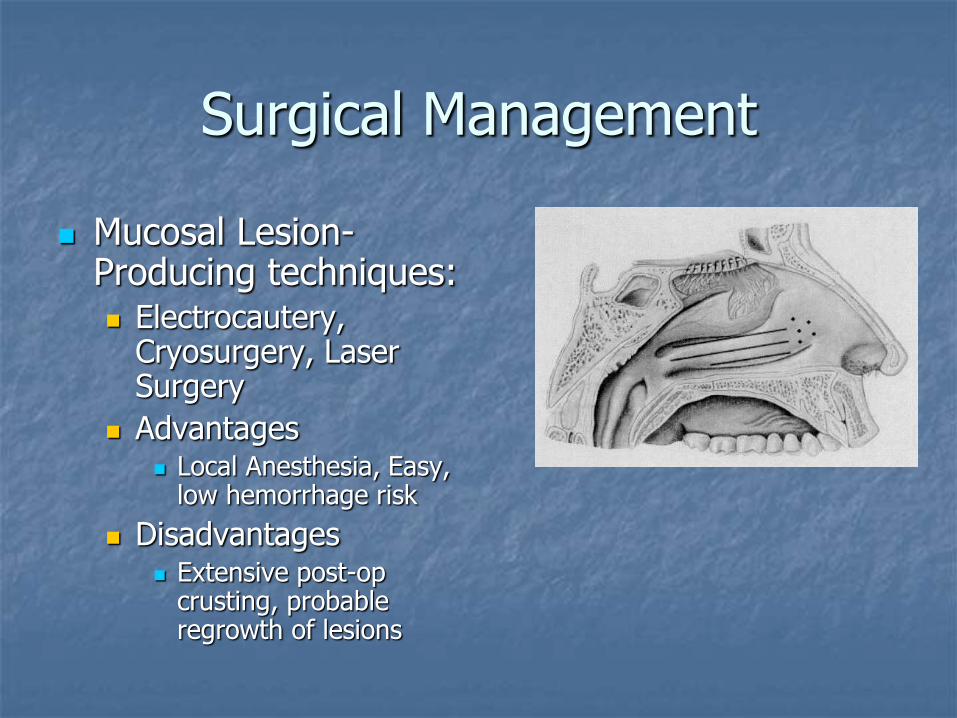
Mucosal Lesion-Producing techniques: Electrocautery,
Cryosurgery, Laser Surgery
Advantages Local Anesthesia, Easy,
low hemorrhage risk
Disadvantages Extensive post-op
crusting, probable regrowth of lesions
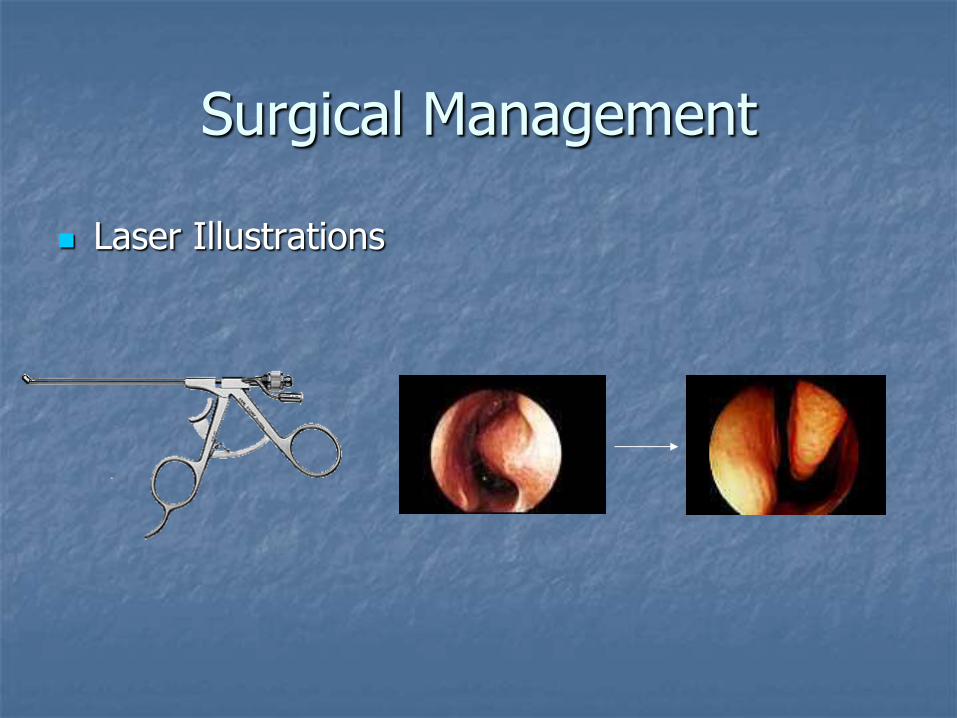
Surgical Management
Laser Illustrations
Surgical Management
Submucous Lesions Radiofrequency –
unipolar or bipolar Study by by Back et al
on twenty patients showed improvement in nasal cross-sectional area by acoustic rhinometry at one year
KTP, Argon, and CO2 have all been shown to be effective.
Surgical Management
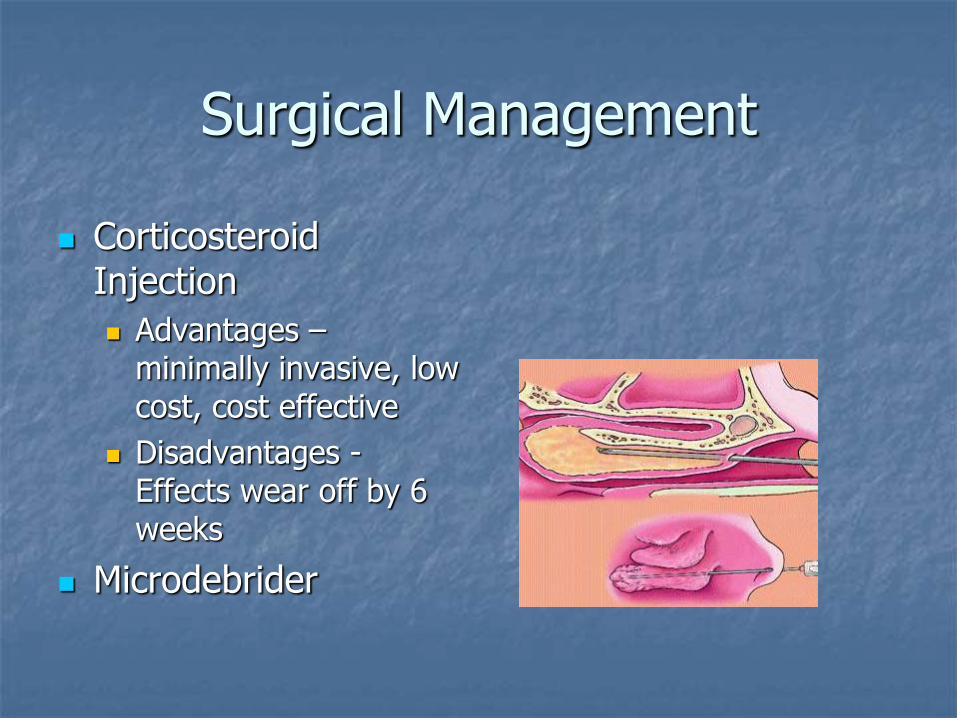
Corticosteroid Injection
Advantages – minimally invasive, low cost, cost effective
Disadvantages - Effects wear off by 6 weeks
Microdebrider
Surgical Management
Vidian Neurectomy Ligate vidian nerve, thus cutting
parasympathetic supply.
Transantral, Transseptal, Transpalatal.
Good immediate relief (Fernandes et al) reports 88% of 139 patients reported improvement in rhinorrhea.
Can have high complication rate including bleeding
Surgical Management
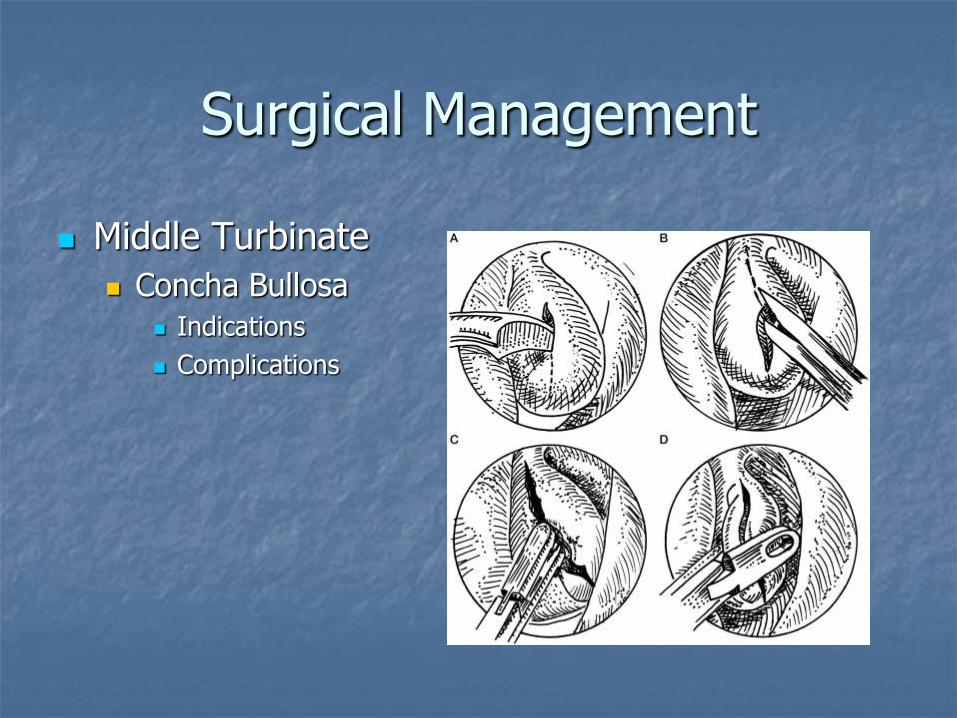
Middle Turbinate
Concha Bullosa
Indications
Complications
Surgical Management
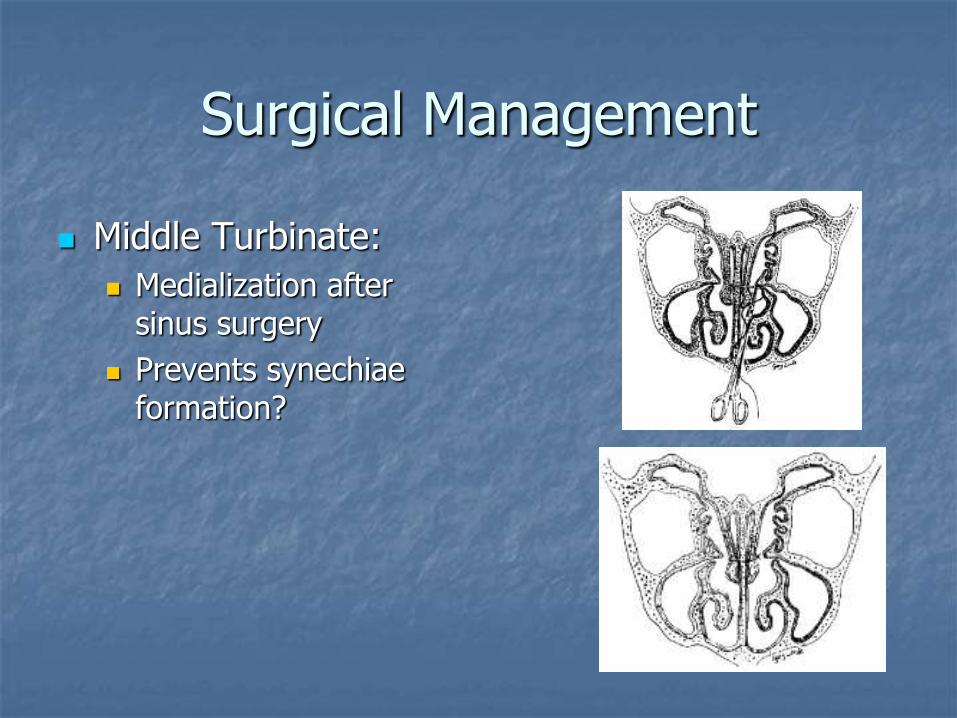
Middle Turbinate:
Medialization after sinus surgery
Prevents synechiae formation?

Surgical Management
Resection of the normal middle turbinate?
Havas, et al. show clear benefit in reducing synechiae requiring revision at osteomeatal complex after partial resection of middle turbinate (15% without resection vs. 7.1% with) in a randomized trial of >1000 patients.
Conclusion
Anatomy
Histology/Physiology
Evaluation of Nasal Obstruction
Turbinate Disorders
Medical Management
Surgical Management
Controversial
Bibliography: McCaffrey, Thomas V., “Nasal Function and Evaluation,” Byron J. Bailey’s Head and Neck Surgery – Otolaryngology, Third Edition, pgs 261-271. Lippincott Williams and Wilkins Philadelphia, 2001.
Lindemann, Jorg, MD “Impact of Unilateral Sinus Surgery with Resection of the Turbinates by Means of Midfacial Degloving on Nasal Air Conditioning,” Laryngoscope, 112(11), pgs. 2062-2066.
Jafek, Bruce W. et al “ Nasal Obstruction,” Head and Neck Surgery – Otolaryngology, Third Edition, pgs 293-308. Lippincott Williams and Wilkins Philadelphia, 2001.
Dowley, A.C. et al “The effect of inferior turbinate hypertrophy on nasal spray distribution to the middle meatus,” Clinical Otolaryngology 26(6) pgs 488-490.
Ophir, D. et al, ”Total inferior turbinectomy for nasal airway obstruction,” Archives of Otolaryngology 111:93, 1985. Courtiss, E.H. et al “Resection of obstructing inferior turbinates: a 6 year follow-up,” Plastic Reconstructive Surgery
72: 913, 1983. Jackson, Lance E et al “Controversies in the Management of Inferior Turbinate Hypertrophy: A Comprehensive
Review,” Lippincott Williams and Wilkins, Plastic and Reconstructive Surgery 103(1) pgs 300-312. Leunig, Andread, MD et al “Ho: YAG Laser Treatment of Hyperplastic Inferior Nasal Turbinates,” Laryngoscope
109(10) pgs 1690-1695. Havas, TE; Lowinger, DSG, “Comparison of functional endonasal sinus surgery with and without partial middle
turbinate resection,” Annals of Otolgoy, Rhinology, Laryngology, 109:634-640 pp 113-119. 10. Fisher, E.W. “Acoustic Rhinometry Reproducibility and Reliablity,” Clinical Otolaryngology, 22(4) pp 307-317.
Hanif, J et al, “The nasal cycle in health and disease.” Clinical Otolaryngology and Allied Sciences, 25(6) pp 461-467. Mygin, N. “Nasal Polyposis, Eosinophil dominated inflammation, and Allergy,” Thorax 55(supplement 2) pp s79-s83.
Berger, Gilead et al, “Histopathology of the inferior turbinate with compensatory hypertrophy in patients with deviated nasal septum,” Laryngoscope 111(12) pp 2100-2105.
Saunders, M.W. et al, “Parameters of nasal airway anatomy on magnetic resonance imaging correlate poorly with subjective symptoms of nasal patency” Clinical Otolaryngology & Allied Sciences 24(5) pp 431-434.Howard, et al “Understanding the Nasal Airway: Principles and Practice,” Plastic and Reconstructive Surgery, 109(3) pp 1128-
1146.Thornton, Robert S., “Middle Turbinate Stabilization Technique in Endoscopic Sinus Surgery” Arch Otolaryngol Head Neck Surg.1996;122:869-872Dogru, Harun. Tuz, Mustafa. Uygur, Kemal. Cetin, Meltem, “A New Turbinoplasty
Technique for the Management of Concha Bullosa: Our Short-Term Outcomes,” Laryngoscope. 111(1):172-174, January 2001.Back et al, “Sumucosal Bipolar Radiofrequency thermal ablation of inferior turbinates: A long-term
follow-up with subjective and objective assessment,” Laryngoscope 112(10) pp 1806-1812.






![Peroperative Findings Middle Turbinate in 50 Chronic ... · lays over the bulla ethmoidalis and in most cases over the hiatus semilunaris and the uncinate pro-cess [1]. This turbinate](https://img.pdfslide.net/doc/110x75/5c92553309d3f244438d38a6/peroperative-findings-middle-turbinate-in-50-chronic-lays-over-the-bulla.jpg)




















