Embed Size (px)
Citation preview

Turn down the heat!
Treating hot flashes
Amanda Place, PharmD, BCACPSt Vincent Joshua Max Simon
Primary Care CenterSeptember 2014

I HAVE NO ACTUAL OR POTENTIAL
CONFLICT OF INTEREST IN RELATION TO
THIS PROGRAM OR PRESENTATION.

ObjectivesDescribe both symptoms and possible
mechanisms of hot flashesDiscuss benefits and risks of estrogen-
containing products in the treatment of hot flashes
Identify the utility of and evidence supporting non-estrogen treatment alternatives
Define the role of complementary and alternative medicine therapies in the treatment of hot flashes

What is a hot flash?Sudden sensation of heat (face, neck
and chest)Skin flushing, sweatingMay be accompanied by anxiety,
irritationOften followed by chills
J Support Oncol 2006;4:315-320Ann N Y Acad Sci 1990;592:52-86

Prevalence70-80% of women will experience hot
flashesAverage duration: 2-5 years15-20% of women may have ongoing
hot flashesGreater severity in patients with
chemical or surgical menopause, or premature menopause (<40 yrs of age)
Am J Epidemiol 2000; 152:463Am J Public Health 2006; 96: 1226
Arch Intern Med. 2008;168(8):840-846

Pathophysiology Exact mechanism for vasomotor
flushing not yet identifiedSeveral proposed mechanisms
◦Decrease in hormones◦Changes in the hypothalamus◦Other factors implicated
Prostaglandins Endorphins Neurotransmitters
Acta Oncologica 2002;41:269-75 Ann Pharmacother1997;31:915-7
ONF 2002;29: 33-40 Ann Pharmacother2002;36:433-6

Contributing FactorsModifiable
◦ BMI◦ Smoking◦ Avoidance of
triggers◦ Exercise ◦ Depression/
anxiety
Difficult to modify◦ Cause of
menopause◦ Genetics◦ Socioeconomic
factors
Am J Epidemiol 2000; 152:463Am J Public Health 2006; 96: 1226

Assessment ToolsPatient history and recallHot flash diaryValidated tools:
◦Hot Flash Score◦Greene Climacteric Score◦Modified Kupperman Index◦Utian Quality of Life Scale
Menopause 2002; 9(6):402-410J Clin Oncol 2001; 19:4280-4290
Maturitas 2012 March;71(3):213-216

Treatment Options
Lifestyle modifications
Hormonal Therapies
SSRI/SNRIGabapentinClonidine
CAM modalities
Endocr Pract 2011;17 (suppl 6)Menopause 2012;19(3):257-271
Climacteric 2014;17:1-16

Lifestyle ModificationDecrease BMIDecrease caffeineModify or eliminate alcohol useIncrease exerciseImprove dietary habitsLayered clothingStress reduction/paced respirations
Menopause 2004;11:11Menopause 2012;20(2):179-184Menopause 2012;19(7):749-759

Estrogen Replacement (ET)Considered most effective agent
Endocr Pract 2011;17(Suppl 6)Menopause 2012;19(3):257-271
Climacteric 2014;17:1-16
Agent Initial dose
High dose
Conjugated equine estrogens (CEE)
0.3 mg 1.25 mg
17βEstradiol 0.5 mg 2 mg
Transdermal estradiol
0.025 mg 0.1 mg
Estradiol gel 0.5 mg 1.5 mg

ET Risks and BenefitsBenefits Risks
Vasomotor symptoms Coronary heart disease
Vaginal symptoms Stroke
Sexual function Venous thromboembolism
Urinary tract health Endometrial cancer
Osteoporosis Breast cancer
Quality of lifeEffect of ET on ovarian cancer, lung cancer, mood, dementia, and mortality remain mixed.
Endocr Pract 2011;17(Suppl 6)Menopause 2012;19(3):257-271
Climacteric 2014;17:1-16

ET ConsiderationsTransdermal = risk Duration of useAppropriate doseNeed for progestinChoice of progestinTaper vs. stopBioidentical ET
Menopause 2010;17:946-954Menopause 2006;13:370-376
Endocr Pract 2011;17(Suppl 6)Menopause 2012;19(3):257-271

Assessment questionAccording to data from the Women’s Health Initiative, which of the following is a benefit of using estrogen to treat hot flashes?1. Increase or maintenance of bone
mass2. Decrease in cardiovascular risk
because of increase in good cholesterol
3. Decrease in the risk of endometrial cancer
4. All of the above

Assessment question
A 50 yo female would like to start estrogen therapy for hot flashes. She has no allergies and no significant medical or surgical history. Which would be a good initial choice for her?1. Estradiol 0.025 mg/24 hr transdermal patch
once weekly2. Estradiol 0.5 mg /norethindrone acetate 0.1
mg daily3. CEE 0.625 mg/medroxyprogesterone 2.5 mg
daily4. Estradiol cream 0.1 mg/gm: 2 gm
intravaginally once daily at bedtime

Bazedoxifene/CEE (Duavee)Tissue-selective estrogen complex
Safety data for up to 2 years
Indications Vasomotor symptoms, prevention of postmenopausal osteoporosis
Precautions/ warnings
Refer to CE
Dose CEE 0.45 mg and bazedoxifene 20 mg
Cost ≈$140 per month
Lexi-Comp, Inc. (Lexi-DrugsTM ). Lexi-Comp, Inc.; Version1.13.0 Accessed July 28th, 2014
Menopause 2009;16(6):1116-1124Menopause 2012;19(4):479-485

Clinical study limitationsSmall sample sizesOutcomes based on patient-reported
dataMany studies focus on patients with
breast cancer historyLarge placebo effect: 20-30%
reductions in hot flash score/frequency Limited duration of trials

Menopause 2008;15:655
Non-estrogen therapies

Progestational agents
• 20-80 mg dailyMegestrol acetate
• 400 mg depotMedroxy-
progesterone acetate
• 10 mg dailyNorethindrone acetate
N Engl J Med 1994;331(6);347J Clin Oncol 2008;26(10):1650
J Clin Oncol 2006;24(9):1409Ann Oncol 2002;13(6):883

Progestational agentsAdrenal
suppression
Clotting risk
Breast cancer risk
Bone loss
Weight gain

SSRIs/SNRIsMechanism: increases available
neurotransmittersDoses differ if only treating hot flashesSerotonin syndrome risksProduct selection:
◦ Drug interactions◦ Cost◦ Evidence◦ Co-morbid conditions

Paroxetine (Brisdelle®)Approved 2013
Cost ~$150/month
VMS frequency vs placebo
Trial #1 at 4 wks ↓ 1.2 /day
Trial #2 at 4 wks ↓ 1.3/day
Trial #1 at 12 wks
↓ 0.9/day
Trial #2 at 12 wks
↓ 1.7/day
Brisdelle PI, Noven Therapeutics, LLC, Miami, FL

Other antidepressantsDrug Daily
DoseOutcomes
Fluoxetine 20 mg ↓ monthly hot flash score
Sertraline 50-100 mg ↓ weekly frequency
Citalopram** 20-40 mg ↓ hot flash scores
Escitalopram 10-20 mg ↓ daily frequency
Venlafaxine 37.5-75 mg ER
↓ hot flash scores
Desvenlafaxine 100 mg ↓ daily frequency
Duloxetine 60 mg ↓ VMS** showed efficacy as an add-on to HRT as well
References provided at end of presentation

Antidepressant safety
T/F May inhibit platelet aggregation
T/F May be associated with bone loss/fracture risk
T/F Don’t need to be tapered when used for hot flashes
T/F May decrease the efficacy of antibiotics
T/F May decrease the efficacy of tamoxifen
T/F May increase risk of suicidality

Antidepressant pearlsWhich one must have a wash-out?
fluoxetineWhich ones should be cross-tapered?
paroxetine or venlafaxineWhich one to choose if a patient takes
clopidogrel?citalopram or venlafaxine
Which one causes the MOST hypertension?
venlafaxine

The gabasMechanism: GABA vs. NorepinephrineLower doses than used in neuropathic
painDrug interactions: CNS depressantsMonitoring: renal functionAdverse effects: drowsiness, dizziness,
rash, peripheral edema, weight gain

J Clin Oncol 2009; 27:2831-2837
Gabapentin dose range

Gabapentin ER interrupted
FDA declined approval in May 2013Trial VMS
change @ 4 weeks
VMS change @ 12 weeks
Breeze 1: 1200 mg
↓ 0.96/day ↓ 0.56/day**
Breeze 1: 1800 mg
↓ 1.51/day ↓ 1.53/day
Breeze 2: 1200 mg
↓ 1.61/day ↓ 1.56/day
Breeze 2: 1800 mg
↓ 1.51/day ↓ 1.12/day
Breeze 3: 1800 mg
↓ 1.69/day ↓ 1.14/day
** not statistically significant
www.clinicaltrials.gov accessed 2/13/14

PregabalinNot seeking FDA approval
Cost: pregabalin = gabapentin x 10
Daily dose Change in hot flash frequency
75 mg BID ↓ 1.7/day
150 mg BID ↓ 2.0/day
J Clin Oncol 28:641-647

Gabas’ safetyT/F These should not be used in pts with NYHA class 3 HF
T/F These drugs should be dose adjusted for hepatic function
T/F Since these agents are hepatically metabolized, they have many drug interactions
T/F Dizziness/somnolence may go away over time

Gabas’ pearlsPossible to direct switch
Gabapentin dosing regimen may differ from pain dosing:◦600-900 mg hs vs. 300 mg TID
Gabapentin Pregabalin0-900 mg per day 150 mg per day901-1500 mg per day 225 mg per day1501-2100 mg per day 300 mg per day
Pain Med. 2010; 11(3): 456-465

ClonidineMechanism: decreases available
neurotransmittersDose range: 0.1 to 0.2 mg per day-
oral or transdermal Drug interactions: antihypertensives,
SNRIsAdverse effects: drowsiness, dizziness,
fatigue, dry mouth, orthostatic hypotension, dermatologic reactions with transdermal form
Obst Gynecol 1982;60:583-586J Clin Oncol 1994;12:1155-158

Comparator Trials(Gabapentin = estrogen) >placeboVenlafaxine preferred vs gabapentinGabapentin = gabapentin + SSRI/SNRIMPA = megestrolFluoxetine = citalopram = placeboMPA > venlafaxineVenlafaxine > clonidine(Estradiol ≈ venlafaxine) > placebo
JAMA Intern Med 2014;174(7):1058-1066 Obstet Gynecol 2006;108:41-48J Clin Oncol 2010;28:147-5152 J Clin Oncol 2007;25:308-312Ann Oncol 2002;13:883-888 Menopause 2005;12(1):18-26
J Clin Oncol 2006:24:1409 Ann Oncol 2007;18:689-693

Assessment question
Which of the following drug classes have NOT shown efficacy in the treatment of hot flashes:1. Estrogens2. Dihydropyridine calcium
channel blockers3. α-2-δ ligands4. Serotonin/norepinephrine
reuptake inhibitors

Assessment questionA 47 yo female with a strong family of breast cancer would like to start drug treatment for hot flashes. She takes tamoxifen 20 mg and a multivitamin daily. Blood pressure at most recent visit was 114/74 mm Hg. What would you recommend?1. Paroxetine 7.5 mg daily2. Estradiol 0.5 mg/norethindrone acetate 0.1 mg
daily3. Clonidine 0.1 mg/24 hr transdermal patch
weekly4. Gabapentin 300 mg in the morning and 600 mg
before bedtime

CAM Hormonal agentsAlfalfaBlack CohoshChasteberryDHEADong QuaiFlaxseedHops
KudzuLicoricePanax GinsengRed cloverSoyWild Yam

CAM Hormonal agentsAlfalfaBlack CohoshChasteberryDHEADong QuaiFlaxseedHops
KudzuLicoricePanax GinsengRed cloverSoyWild Yam

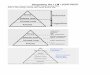
CAM Treatments for Hot FlashesLikely safe Possibly safe
Effective
Likely effective
Possibly effective
FlaxseedSoy foods
Black CohoshSoy extracts
Insufficient evidence
ChasteberryGinkgoVitamin E
AlfalfaDHEA (short term)HopsKudzuLicoriceValerian
Possibly ineffective
Evening Primrose oil
Dong Quai (short term)Red CloverWild YamPanax GinsengAdapted from Natural Medicines
ComprehensiveDatabase-Accessed 5/17/2010

CAM Hormonal agentsGeneral cautions:
◦Unknown or questionable estrogenic activity
◦Standardization of products/preparations
◦Consistent quality of products◦Lack of high quality evidence

AcupunctureDifficult to determine a true
“placebo” groupDiffering disciplines of
acupuncturePt expectationsLack of understanding about
physiologic effects of acupuncture
Menopause 2010;17(2):228-230Menopause 2009;16:1065-1073

ConclusionsChoice of agent should be made
with patient-specific variables as a guide.
Patient expectations may impact efficacy.
Different agents or combinations may need to be tried to achieve desired benefit.

Turn down the heat!
Treating hot flashes
Amanda Place, PharmD, BCACPSt Vincent Joshua Max Simon
Primary Care CenterSeptember 2014

Slide 17 References Obst Gynecol 1982;60:583-586
J Clin Oncol 1994;12:155-158
J Clin Oncol 2002;20:1578-1583
Lancet 2000;356:2059-2063
J Clin Oncol 2010;28:3278-3283
JAMA 2001;305(3):267-274
J Clin Oncol 2009;27:2831-2837
Drugs 2011;71(3):287-304
Pharmacotherapy 2009;29(11):1357-1374