Embed Size (px)
Citation preview

Turner Syndrome and the HeartCardiovascular Complications and Treatment Strategies
Claus Højbjerg GravholtMedical Department M (Endocrinology and Diabetes) and Medical Research Laboratories, Aarhus Kommunehospital,Aarhus University Hospital, Aarhus, Denmark
Contents Abstract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4011. History and Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4012. Congenital Malformations of the Heart and the Great Vessels . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4033. Hypertension and Ischemic Heart Disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4064. Aortic Dissection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4075. Growth Hormone Treatment and the Heart . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4076. Hormone Replacement Therapy and the Heart . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4087. Cardiovascular Management in Turner Syndrome . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 409
Abstract Turner syndrome is a condition usually associated with reduced final height, gonadal dysgenesis, and thusinsufficient circulating levels of female sex steroids, and infertility. A number of other signs and symptoms areseen more frequently with the syndrome. With respect to cardiac function, congenital malformations of the heartand the great vessels, hypertension and ischemic heart disease, and increased risk of aortic dissection are allconditions that the pediatrician or the physician caring for females with Turner syndrome should keep in mind.Many girls and adolescents with Turner syndrome receive growth hormone (GH) treatment, which has so farbeen an effective and well-tolerated therapy. Nevertheless, because of the experience from acromegaly, thephysician should monitor blood pressure and perform echocardiography, together with clinical examinationsby a cardiologist at regular intervals. During adulthood most women with Turner syndrome are faced withpremature menopause and the need for female hormone replacement therapy (HRT). During clinical evaluationof girls and women with Turner syndrome, these conditions and complications should be kept under surveillance.
Here the cardiovascular complications of Turner syndrome are reviewed. The risk of congenital heart defectssuch as bicuspid aortic valves, aortic coarctation, other valve abnormalities, and septal defect is increased.Likewise, the risk of aortic dissection at a young age is increased, as is the risk of hypertension, ischemic heartdisease, and stroke. GH therapy does not seem to adversely affect the heart, although longer-term follow-upstudies are needed. In short-term studies, HRT lowers blood pressure, while any effect on the risk of ischemicheart disease has not been evaluated. Treatment with GH and HRT are discussed in relation to the heart andgreat vessels. Presently, the pathophysiology of the congenital cardiovascular malformation in Turner syndromeis unexplained, although different theories exist. Recommendations for clinical practice are given, includinglife-long surveillance of cardiac function, aortic diameter and blood pressure.
REVIEW ARTICLE Am J Cardiovasc Drugs 2002; 2 (6): 401-4131175-3277/02/0006-0401/$25.00/0
© Adis International Limited. All rights reserved.
1. History and Introduction
Turner syndrome derives its name from the American physi-cian Henry H. Turner of Oklahoma City, Oklahoma.[1] In a reportin Endocrinology in 1938 he described seven patients with sev-eral characteristic features of the syndrome, such as infantilism,cubitus valgus and congenital webbing of the neck. Since the
initial report a number of abnormalities have been recognized inassociation with the syndrome. The cardinal stigmata are growthretardation with reduced final height, gonadal insufficiency andinfertility. Further congenital malformations and conditions aregiven in table I, with tentative frequencies, based on a number ofreferences.

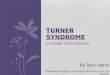
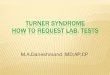
Turner syndrome is caused by an absent or structurally ab-normal X chromosome. The typical karyotype in Turner syn-drome is 45,X; i.e. one X chromosome is missing. Most womenwith Turner syndrome, however, are not carrying the ‘typical’karyotype of 45,X, but have several different variants all causingthe clinical signs of Turner syndrome. The most frequently oc-curring karyotypes are 45,X, karyotypes with an isochromosomeof X [i(Xq) or i(Xp)], the mosaic karyotype of 45,X/46,XX, andkaryotypes containing an entire Y chromosome or parts thereof.The 45,X karyotype was found in only 48% of all live-born fe-males with Turner syndrome during the period 1970–1995.[5] Theprevalence has never been firmly established, but a number ofcytogenetic studies have given estimates ranging from 25–210per 100 000 females,[7-10] and most seem to agree on a hypothet-ical proportion of about 50 per 100 000 girls in Caucasian popu-lations (figure 1). In the future, it is possible that the number ofgirls being born with Turner syndrome will decrease because ofincreased use of prenatal diagnostic measures (amniocentesis,chorionic villus sampling [CVS], ultrasonography, triple-blood-sample testing, etc.). However, treatment and prevention meas-ures are hampered by a considerable delay in diagnosis;[11] inDenmark the median age at diagnosis is 15 years when consider-ing all girls and women diagnosed between 1920 and 2000 (figure2). This means that many girls and women are treated rather latein life, and some are never diagnosed.
Turner syndrome is often complicated by congenital cardio-vascular malformations, hypertension, ischemic heart disease,
Table I. Abnormalities associated with Turner syndrome with tentativefrequencies[2-6]
Feature Frequency (%)
1. Retarded growth and reduced final height 95-100
2. Gonadal dysgenesis no pubertal development 85
infertility 98
chronic estrogen deficiency 95-98
androgen insufficiency ?
3. Endocrine disturbances glucose intolerance 15-50
type 2 diabetes mellitus 10
type 1 diabetes mellitus 2-3
thyroiditis 15
elevated hepatic enzymes 50-80
hypertension 30-50
android body composition ?
4. Physical abnormalitiesa) Eyes
epicanthus 20
nearsightedness 20
strabismus 15
ptosis 10
b) Ears
infection of middle ear 60
hearing defects 30
deformity of external ear 15
c) Mouth
micrognathia (small mandibular bone) 60
high arched palate 35
abnormal dental development ?
d) Neck
low posterior hairline 40
broad short-appearing neck 40
pterygium colli (webbed neck) 25
excess loose skin in the back of the neck of neonates
25
e) Thorax
broad chest (shield chest) with apparently wide-spaced nipples
30
inverted nipples 5
f) Skin, nails and hair
increased skin ridge count 30
lymphedema of hands and feet at birth (or later) 25
multiple pigmented nevi 25
nail hypoplasia 10
vitiligo 5
alopecia 5
g) Skeleton
bone age retardation 85
decreased bone mineral content 80
cubitus valgus 50
short fourth metacarpal 35
genu valgum 35
congenital hip (sub)luxation 20
scoliosis 10
Madelungs deformity 5
h) Heart
bicuspid aortic valves 13-34
coarctation of the aorta 4-14
aortic dilation/aneurysm 2 ?
other cardiac malformations 1-6
i) Kidneys
horseshoe kidney 10
abnormal positioning or duplication of renal pelvis, ureters or vessels
15
renal aplasia 3
5. Psychosocial problems emotional immaturation 40-85
specific learning problems 40
mental problems 25
6. Other failure to thrive during first year of life 50
402 Gravholt
© Adis International Limited. All rights reserved. Am J Cardiovasc Drugs 2002; 2 (6)

and aortic dilation with or without aortic aneurysm. These asso-ciated features are responsible for considerable morbidity, andpremature death in a number of patients.
Today, most girls and adolescents with Turner syndrome aretreated with growth hormone (GH) to increase final height[12] andestrogens to induce puberty, and after the advent of menarche,progestogens are added 10–12 days every month to simulate thecyclic events of the normal menstrual cycle.
Since GH and hormone replacement therapy (HRT) may ex-ert significant cardiovascular effects, complications relating tothe heart and effects on the heart of this treatment given to womenand girls with Turner syndrome are reviewed.
2. Congenital Malformations of the Heartand the Great Vessels
An association between Turner syndrome and congenitalcardiovascular malformations has been known from early on. Inthe early series focusing on heart defects, emphasis was primarilyon coarctation of the aorta;[13-15] pulmonary stenosis was also
noted (possibly due to ‘contamination’ of study groups by pa-tients likely to have Noonan syndrome),[15,16] as well as less se-vere congenital malformations of the heart,[4,17,18] especially withthe 45,X karyotype.[4,19-21] In addition, many case reports havedescribed specific, uncommon malformations linked to the syn-drome. Although the congenital malformations of the heart havebeen recognized for many years, a number of studies during re-cent years have meticulously documented these malformationsin relatively unselected populations, and approximate frequen-cies are available[4,18,22-24] (table II).
Congenital cardiovascular malformations occur more fre-quently in unselected populations of individuals with Turner syn-drome than in the background population. The malformationsnormally involve only the vessels of the left side of the heart andshow a very characteristic pattern when compared with that ofthe general population.[23,24] A recent Italian study found congen-ital cardiac malformations in 136 of 594 (22.9%) patients withTurner syndrome.[24] This figure corroborates previous findingsin unselected groups of patients, in whom congenital cardiac le-
Year
0
10
1920 1930 1940
20
30
40
50
60
70
80
Pre
vale
nce
of T
urne
r S
yndr
ome
per
100
000
liveb
orn
girls
1950 1960 1970 1980 1990 2000
Fig. 1. Recorded prevalence of Turner syndrome per 100 000 live-born girls by year of birth from 1910 to 2000 in Denmark. The broken line indicates the hypothetical prevalence
of 50 per 100 000 live-born girls (data from the Danish Cytogenetic Central Register).
Turner Syndrome and the Heart 403
© Adis International Limited. All rights reserved. Am J Cardiovasc Drugs 2002; 2 (6)

sions were found in 20–40% of.[4,23,25,26] Notably, a number ofpatients have more than one structural malformation. In a recentlarge study, it was shown that cardiac malformations were moreprevalent among the subgroup of patients with 45,X (39%) thanamong those with karyotypes that include an isochromosome(Xq) [11–12%] (mosaic or not).[23] In the large Italian study itwas also found that cardiac malformations were more prevalentamong patients with 45,X (30%) than among patients with Xmosaicism (24%) and X chromosome structural abnormalities(iXq, r[X], del[X], etc.) [11%].[24] The study group was suffi-ciently large to permit formal statistical evaluation of the risk ofcongenital malformations between these three major groups ofkaryotypes, with more malformations occurring among patientswith 45,X than among the group of patients with X chromosomestructural abnormalities (relative risk [RR] 2.7; 95% confidenceinterval [CI] 1.8–4.2), but with a comparable number of malfor-mations among patients with 45,X and X mosaicism (RR 1.2;95% CI 0.8–1.9).[24] Thus it seems that karyotypes involvingstructural abnormalities of the X chromosome confer some pro-tection towards cardiac malformations.
Likewise, in a registry study of all Danish patients withTurner syndrome, the 45,X karyotype was most frequently asso-ciated with congenital malformations, including cardiac malfor-mations.[5] In the same study, cardiovascular morbidity not re-lated to congenital malformations of the heart (such as acute
myocardial infarction, hypertension and arteriosclerosis) weremore frequently associated with karyotypes other than 45,X. Thesame pattern was seen for endocrine diseases, primarily hypothy-roidism and type 1 and 2 diabetes mellitus, indicating that themany different karyotypes involved in Turner syndrome maylead to different disease patterns, congenital as well as ac-quired.[5] It may be speculated that the increased morbidity dueespecially to endocrine disease is part of the explanation for theincreased morbidity due to cardiovascular diseases. Concerningother karyotypes (i.e. karyotypes with rings and markers or Ychromosomal material) known to result in clinical Turner syn-drome, current numbers are too small to allow formal statisticalcomparison with the 45,X karyotype.
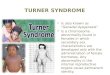
A bicuspid aortic valve is the most common finding and isseen in 13–34% of patients, with Turner syndrome comparedwith only 1–2% in the general population[27] (figure 3). Althoughsome individuals present with a systolic murmur or an ejectionclick on clinical examination, many (perhaps the majority) arenot identified clinically, but only echocardiographically.[22,23]
Bicuspid aortic valves are seen with most karyotypes, but pre-dominantly with the 45,X karyotype.[23,24]
Coarctation of the aorta is present in 4−14% of all patientswith Turner syndrome (figure 3), and predominates in patientswith the ‘classical’ karyotype of 45,X. Most patients with aorticcoarctation are diagnosed early, because of the relative severityof the condition. Coarctation occurs more than 350-fold morefrequently in patients with Turner syndrome than in the generalpopulation.[5] Today, patients with clinically significant coarcta-tion are operated on early, either with resection and end-to-endanastomosis, or subclavian flap operation, while some undergoprimary percutaneous balloon dilatation with or without stenting.Other malformations affecting the valves have also been re-ported, such as aortic valve stenosis, aortic valve regurgitation,mitral valve prolapse, mitral valve stenosis and cleft mitral valve.Furthermore, atrial septal defect, ventricular septal defect andpersistent ductus arteriosus are seen in 1–6% of patients.[4,23,24]
Surgery, or coronary catheterization if possible, should be under-taken wherever required. Clinical follow-up is necessary in mostor all patients. In any case, all patients with either bicuspid valves,septal defects or other valvular diseases should be informed ofthe risk of infectious endocarditis in relation to minor surgery,including dental work, and be issued with proper antibiotic pro-phylaxis when necessary. Rarely, hypoplastic left heart syndromehas also been described,[23,28] which leads to early death if un-treated.[23]
The incidence of any given malformation differs from studyto study (table II). These differences are probably not important,since it is clear that any figure given in the literature is grossly
Age at diagnosis (years)
120
100
80
60
40
20
0
Median = 15 yearsRange = 0−86 yearsn = 746
80706050403020100
Num
ber
Fig. 2. Delay in diagnosis of Turner syndrome. The x-axis illustrates the number of
patients with Turner syndrome at the chronological age of diagnosis. Bars illustrate
2.5-year periods. Data are from the Danish Cytogenetic Central Register from 1910–
2000. Data include all diagnosed females with a karyotype that can be associated with
Turner syndrome.
404 Gravholt
© Adis International Limited. All rights reserved. Am J Cardiovasc Drugs 2002; 2 (6)

elevated in comparison with the background population. Thus,any individual with Turner syndrome should always be seen bya cardiologist and at least have echocardiography performed. De-pending on the findings on echocardiography, some patientsshould also be examined by magnetic resonance imaging (MRI)scan, and rarely invasive examination, such as right- and/or left-sided cardiac catheterization, might be necessary.
The cause of congenital heart defects in Turner syndromeremains unknown. Various investigators have presented differentviews on the subject depending on whether they see congenitalmalformation of the heart in Turner syndrome as a true malfor-mation, linked to the expression of a specific gene or cluster ofgenes, possibly being X-linked (a gene or genes escaping X in-activation), or the result of disruption of normal embryonic de-velopmental events, and thus not caused by the karyotype itself.Since patients with 45,X karyotype are predominantly affectedby congenital cardiovascular malformations, as well as bylymphedema (and thus webbed neck), deficient development oflymphatics has been proposed as a causative factor. In utero,developing lymph channels distend secondary to failed emptyingof jugular lymph sacs into central veins. It is suggested that thesedistended lymph channels encroach on the heart and great ves-sels, in this way mechanically inducing congenital heart de-fects.[20,21,29] The development of coarctation of the aorta may bedue to a combination of maldevelopment of lymphatics and de-
creased left-sided blood flow in utero (through the aorta), leadingto increased flow through the pulmonary artery and the ductusarteriosus, which may induce development of a shelf or flange,leading to later coarctation.[20] Recent intriguing observationsshow that cardiac hypoplasia, along with lung hypoplasia, iswidespread among Turner syndrome fetuses recognized becauseof massive hydrops or large nuchal hygromas.[30] The authorsexamined 117 Turner syndrome fetuses (32% definitely verifiedby karyotyping, the rest due to typical stigmata), ad found morethan 90% of the fetuses to have heart weights below the 2.5 cen-tile, and suggested that myocardial hypoplasia is a primary defectin Turner syndrome leading cardiac pump inadequacy impedingvenous return and thereby elevating venous pressure, and that theresulting venous hypertension could lead to diminished lym-phatic outflow, and, eventually to hydrops formation. The phe-notype would thus result in intra-uterine death or, if only mini-mally restricted heart growth was seen, the fetus could survive tobirth.[30] The study leaves several questions unanswered: is car-diac and lung hypoplasia present in live-born Turner syndrome;is the hypoplasia linked to other congenital malformations of theheart; is the hypoplasia actually leading to lymphedema, or is itvice-versa, etc. Other researchers have speculated whether oneor more genes on the missing X chromosome are causative. It issupposed that such a gene (or genes) would be one of the manygenes on the X chromosome known to normally escape X inac-
Table II. Incidence of congenital malformations in patients with Turner syndrome. Data have been compiled from five trials with apparent unbiased inclusionof patients and presented as number of patients affected/total number examined (%)
Congenital malformation Incidence in clinical trials
Miller et al.[22]
(n = 35)aDawson-Falk et al.[18]
(n = 40)bGotzsche et al.[4]
(n = 179)aSybert[25]
(n = 244)aMazzanti & Cacciari[24]
(n = 594)c
Aortic coarctation 5/40 (12.5) 18/179 (10) 34/244 (14) 41/594 (6.9)
Dilated ascending aorta 2/35 (6) 5/40 (12.5) 17/594 (2.9)
Hypoplastic aortic arch 1/40 (2.5)
Bicuspid aortic valve 12/35 (34) 7/40 (17.5) 25/179 (14) 33/244 (14) 74/594 (12.5)
Mitral valve prolapse or regurgitation 2/35 (6) 2/40 (5) 1/179 (0.6) 6/244 (2) 53/594 (8.9)
Interrupted inferior vena cava with azygoscontinuation
1/40 (2.5)
Cardiac dextroposition 1/40 (2.5) 1/179 (0.6)
Aortic valve disease (stenosis and/orincompetence)
19/179 (11) 14/244 (6) 19/594 (3.2)
Partial anomalous pulmonary venous drainage 1/179 (0.6) 1/244 (0.5) 17/594 (2.9)
Ventricular septal defect 3/594 (0.5)
Atrioventricular septal defect 12/244 (5) 1/594 (0.2)
Pulmonary valve abnormality (stenosis,regurgitation)
2/179 (1)
Persistent ductus arteriosus 2/179 (1) 1/244 (0.5)
a Patients were examined only with clinical examination and echocardiography.
b Patients were examined by magnetic resonance imaging scan and echocardiography.
c Patients were examined with clinical examination, ECG, chest x-ray and transthoracic echocardiography.
Turner Syndrome and the Heart 405
© Adis International Limited. All rights reserved. Am J Cardiovasc Drugs 2002; 2 (6)

tivation,[31] a situation leading to haploinsufficiency of the gene(or genes) and the gene product.
The recently reported cloning of the SHOX gene (short sta-ture homeobox-containing gene or PHOG [pseudoautosomalhomeobox-containing osteogenic gene]) from the pseudoautoso-mal region (PAR1) on the X and Y chromosome,[32,33] responsi-ble for part of the reduced growth seen in Turner syndrome andin the Leri-Weil syndrome, and perhaps especially the dispropor-tionate growth, has spurred enthusiasm, and work is in progressto identify genes responsible for other parts of the Turner pheno-type. A gene on chromosome 16 responsible for the lymphedemain the lymphedema-distichiasis syndrome has been described.[34]
Very recent work has suggested that at least one lymphogenicgene is present on the short arm of the X chromosome (Xp) distalto Xp11 between the genes of Duchenne muscular dystrophy andmonoamine oxidase A.[35] The concept of chromosomal imbal-ance, and thus disturbed pairing during mitosis, has also beenimplicated.[35]
3. Hypertension and Ischemic Heart Disease
Thirty percent of girls with Turner syndrome have mild hy-pertension on 24-hour ambulatory blood pressure monitoring,and as many as 50% have an abnormal diurnal blood pressureprofile.[36] Hypertension is also prominent in women with Turnersyndrome, who have significantly elevated blood pressure com-
pared with an age-matched control group,[37] and as many as 50%have clinical hypertension.[6,37] The nocturnal fall in diastolicblood pressure is blunted in many compared with controls, andan increase is seen with HRT, as well as in systolic night/dayratio. The significance of this is unknown. It seems that womenwith Turner syndrome are ‘non-dippers’, i.e. have a diminishedreduction of blood pressure during the night.[37] A blunted noc-turnal fall in blood pressure in hypertensive women has beenshown to predict future major cardiovascular events.[38] Inwomen with essential hypertension, non-dippers have an in-creased left ventricular mass which is considered to be an inde-pendent marker of cardiovascular morbidity and mortality.[39,40]
In Turner syndrome, compared with controls, 24-hour, day, andnight heart rate is significantly elevated,[37] which could be sug-gestive of the presence of parasympathetic neuropathy. At pres-ent there are no longitudinal studies of blood pressure and hyper-tension in patients with Turner syndrome. There is a definite needfor such studies. Furthermore, it is essential to establish the effectof treatment and to determine which drugs to choose as first- andsecond-line treatment.
Previously, the incidence of ischemic heart disease was notfound to be increased in patients with Turner syndrome, despitereports of increased plasma levels of cholesterol,[41] increasedblood pressure, and congenital cardiac malformations. Recently,in the Turner syndrome population in Denmark (n = 594), how-ever, ischemic heart disease (acute myocardial infarction and ar-teriosclerosis) was found more frequently in an epidemiologicalregister study of morbidity.[5] The RR of disease was increasedto 2.1 (95% CI 1.2–3.4), while hypertension occurred with an RRof 2.9 (95% CI 1.2–6.0), and cerebrovascular diseases of 2.7(95% CI 1.04–5.3). In a clinical study, we could not detect anydifference in measures of lipid status between a group of un-treated women with Turner syndrome before treatment and a con-trol group.[42]
Compensated hypothyroidism is associated with coronaryartery disease and elevated plasma levels of low-density lipopro-tein-cholesterol and apolipoprotein B.[43,44] This may help ex-plain part of the increased risk of cardiovascular disease in Turnersyndrome,[5] since hypothyroidism and thyroid antibody forma-tion are common in Turner syndrome, especially in a subgroupwith an isochromosome of the long arm of the X chromosome[i(Xq)].[45-57] In a recent cross-sectional study of 145 women withTurner syndrome, 14% had hypothyroidism; in a subgroup ofwomen with an isochromosome (iXq), an impressive 37.5% hadhypothyroidism, emphasizing the grossly elevated risk of thecondition linked to this karyotype.[58]
Aorticdissection
Aorticcoarctation
Fig. 3. Typical congenital malformations seen in Turner syndrome, i.e. coarctation of
the aorta and bicuspid aortic valves. The figure also illustrates the occurrence of aortic
dilation and dissection. It is noteworthy that the presence of congenital malformations
and/or systemic hypertension is not a prerequisite for the development of dilation and
dissection of the aorta.
406 Gravholt
© Adis International Limited. All rights reserved. Am J Cardiovasc Drugs 2002; 2 (6)

4. Aortic Dissection
The association of aortic dissection and Turner syndrome hasbeen acknowledged for many years.[23] More than 60 case reportsof aortic dilation or dissection, some of which were fatal, havebeen described.[26,59-85] In most cases, risk factors were present.In the general population, risk factors for aortic dissection includethe following: systemic hypertension, which is present in up to90% of cases;[86,87] Marfan and Ehlers-Danloss syndrome, wheremutations in the fibrillin and the collagen type III gene are pres-ent, respectively, (which are also conditions with increased riskof dilation, aneurysm and rupture); congenital bicuspid or uni-commissural aortic valves (especially for type I and II dissec-tions);[27,86] and coarctation of the aorta.[86,87] In addition, preg-nancy, trauma and iatrogenic trauma (cannulation or incisiontrauma during cardiopulmonary bypass procedures) are risk fac-tors.[86,87] Other, rarer, risk factors include temporal arteritis, con-nective tissue disease, cystic medial necrosis of the aorta, syphi-litic aortitis, and fibromuscular dysplasia.[87] Usually, but notalways, these risk factors (other than Turner syndrome) areknown to be present in the reported cases of aortic dissection inTurner syndrome.[26,68]
At the same time, the prevalence and the nature of cardio-vascular malformations have been described in several studies(see section 2).[4,18,23,24,88] Aortic root dilation, which is a riskfactor for later rupture, is often seen and seems to be associatedwith elevated systolic blood pressure.[6] Undoubtedly, Turnersyndrome should be included in this list of risk factors for aorticdissection. At present, no abnormalities of the aortic wall havebeen identified in Turner syndrome. Cystic medial necrosis, sim-ilar to the changes found in Marfan syndrome, has been describedin some (for review see Lin et al.[26]), but not in all cases. Nobiochemical or genetic abnormalities have been described inTurner syndrome thus far.
Pregnancy is a rare event in patients with Turner syn-drome.[89,90] Owing to an increasing number of egg donation pro-grams, more patients can be expected to go through pregnancy inthe future.[91] Because of the pregnancy-associated changes inblood pressure, cardiac work load, etc., the risk of aortic dissec-tion is likely to be increased. Uneventful cases of pregnancy havebeen reported;[89,92,93] however, fatal and nonfatal cases due toaortic dissection have also been described.[94-97]
Prospective studies are needed to establish the exact risk ofaortic dissection, to identify patients at an elevated risk, and, ifpossible, to introduce procedures and/or medicine to lower therisk, both during pregnancy and during normal life.
5. Growth Hormone Treatment and the Heart
Short stature is a key feature of Turner syndrome. Growthretardation can be identified prenatally[98-100] and growth remainssubnormal not only during the first years of life[99,100] butthroughout childhood. The normal pubertal growth spurt is ab-sent in Turner syndrome,[101] even in the 15% of girls with spon-taneous puberty.[102] The rationale for starting GH treatment isnot a lack of GH secretion, but rather reduced final height. Al-though the results of different studies are equivocal and the spon-taneous and stimulated GH secretion has been found by some tobe diminished,[103,104] others have found normal GH secre-tion.[105-107] Treatment with GH has generally been found to bewell tolerated in most patients. However, in Turner syndromesupraphysiological (or pharmacological) GH doses are used, re-sulting in circulating insulin-like growth factor (IGF)-1 valuesoften in the acromegalic range, in comparison with conditionssuch as hypopituitarism (including the GH axis), chronic kidneyfailure, and other conditions. The reason for high-dose GH treat-ment is to overcome the apparent GH or IGF resistance presentin Turner syndrome,[108] and thus increase height appropri-ately.[12]
Safety of treatment clearly remains important. This has to beseen in the light of the increased cardiovascular morbidity andmortality in acromegaly,[109] a pathological condition with chron-ically elevated GH and IGF-I levels, where cardiac function isimproved with restoration of normal GH values.[110] Differentaspects of the safety of GH administration have been studied.Studies have shown that insulin resistance is induced by GH treat-ment in Turner syndrome[12,111,112] and reversed when GH treat-ment is stopped.[12] The induction of insulin resistance is of con-siderable concern, since the prevalence of type 2 diabetesmellitus is increased in Turner syndrome,[5] and a prolonged pe-riod of hyperinsulinemia could potentially lead to overt diabetesmellitus. So far, no long-term (more than 5 years) studies haveaddressed the issue of late effects of GH-induced hyperinsuline-mia. Total and regional body composition is altered in Turnersyndrome, with more body fat and less muscle mass,[113] and ismodified during GH treatment, with a reduction in truncal fat andan increase in muscle mass, presumably favorable changes nor-mally associated with a reduction in cardiovascular risk. How-ever, it is doubtful whether these changes persist after cessationof GH treatment.
Few studies have addressed the effect of GH treatment onthe heart. This is of special interest because of the increasedoccurrence of cardiovascular malformations, aortic dilation andcoronary heart disease later in life in Turner syn-drome.[4,5,18,23,26,37,114] In a recent study very high doses of GHwere used in a subgroup of patients for, on average, 7 years.[12]
Turner Syndrome and the Heart 407
© Adis International Limited. All rights reserved. Am J Cardiovasc Drugs 2002; 2 (6)

No signs of left ventricular hypertrophy or evidence of worseningof hypertension were found in these girls. However, two girlswith pre-existing left-sided obstruction (congenital abnormalaortic and mitral valve, respectively) developed significant valvestenosis, and thus possibly left ventricular hypertrophy, and wereexcluded from further statistical analysis. This could suggest thatpre-existing valve abnormalities might be a risk factor for devel-oping left ventricular hypertrophy. At inclusion, many girls withTurner syndrome had relatively increased systolic and diastolicblood pressure in comparison with normal reference values, butat the end of the study there was a slight decrease in the age-adjusted diastolic blood pressure. In a recent cross-sectionalstudy of girls with Turner syndrome receiving either no treatment(mostly young girls), GH or GH in combination with estradioland a progestogen, 17% had elevated blood pressure in compar-ison with age-matched reference data.[115] Furthermore, by 24-hour blood pressure evaluation, it was shown that 57% of allgirls had a blunted nocturnal fall in blood pressure (‘non-dip-pers’).[31,116] This is a situation often encountered in hypertensionand diabetes mellitus, and thought to be indicative of autonomousneuropathy, and in adult women with hypertension (withoutTurner syndrome) it is considered an independent risk factor forlater development of cardiovascular events.[31] It remains to beseen if there are any long-term effects of GH treatment on thecardiovascular system. It is recommended that long-term follow-up is continued in previous and ongoing GH treatment trials forincreasing final height.
6. Hormone Replacement Therapy and the Heart
The chronic estrogen deficiency known to affect many adultwomen with Turner syndrome is likely to be associated with car-diovascular morbidity. It is generally assumed that treatment withestrogens not only confers cardioprotection through a loweringof harmful circulating lipids, but also through direct antioxidanteffects,[117] a change in the vascular reactivity[118] and its inter-action with vascular smooth muscle.[119,120] Part of the increasedcardiovascular morbidity and mortality in Turner syndromecould therefore be explained by non-use of estrogens.
At present, no long-term studies have assessed the effect ofHRT on the heart and on the increased mortality seen in Turnersyndrome. It might be speculated that HRT would have positiveeffects on aortic ‘stiffness’ in the long term,[121] but any directeffect on the aortic wall has not been described. Far from allpatients receive HRT during adulthood, and many adolescentsare introduced to estrogens rather late, in order to achieve thehighest final height. Recently, there has been speculation that thestandard HRT dose given to women with Turner syndrome
(estradiol 2mg or equivalent) is too low. This speculation hasbeen based on the fact that when trying to establish a ripe endo-metrium for egg donation, patients need estradiol 4mg, or more,for a prolonged period.[90]
Hypertension is frequent among patients with Turner syn-drome (see section 3), and treatment with female HRT causes asmall but significant reduction in the 24-hour diastolic pressureand the diastolic day pressure and a near significant fall in sys-tolic day pressure.[37] In postmenopausal women with hyperten-sion, treatment with estrogen, with or without gestagen, has beenshown to decrease 24-hour ambulatory blood pressure in short-term studies.[122] Although lipid abnormalities have been foundin a few, but not in most studies (see section 3), changes havebeen found during HRT in one study, with a significant, albeitsmall, fall in high-density lipoprotein-cholesterol, while otherlipid variables were unchanged;[42,123] another study found lipidsto be unaffected by HRT.[121] There are no long-term studies ofthe effect of HRT on cardiovascular morbidity and mortality inTurner syndrome. In healthy, postmenopausal women (aged 50–75years) without prior cardiovascular disease the results from therecent Women’s Health Initiative randomized trial show thatHRT should not be initiated for primary intervention of cardio-vascular disease.[124] In addition to an increased risk of cardio-vascular disease in the treated group, the results showed increasesin the risk of breast cancer, stroke, and pulmonary embolism, anda decreased risk of fractured and colorectal cancer amongst ac-tively treated women.[124] In postmenopausal women with a pre-vious cardiovascular event (secondary intervention), HRT hasproved to have no effect on cardiovascular mortality and morbid-ity.[125] In postmenopausal women with a previous stroke, has
Sur
viva
l
Median survival: Turner syndrome 70 years Background population 78 years
Age (years)
0 20 40 60 80
Fig. 4. Kaplan-Meier survival plot of females with Turner syndrome versus the back-
ground population.[125]
408 Gravholt
© Adis International Limited. All rights reserved. Am J Cardiovasc Drugs 2002; 2 (6)

HRT has been unsuccessful, albeit not deleterious, as secondaryintervention.[126]
Previous research has documented that adult women withTurner syndrome are characterized by several features: glucoseintolerance, deficient insulin secretion, thyroid and hepatic ab-normalities, android body composition, decreased physical fit-ness and elevated blood pressure, with a specific increase in thenight/day ratio. Thus, several features of the metabolic syndrome(syndrome X)[127] are present in Turner syndrome, and a compar-ison with the hormonal and metabolic profile of relatives of pa-tients with type 2 diabetes mellitus is warranted. It should also bepointed out that women with Turner syndrome have a decreasedlife expectancy (figure 4), especially those with the 45,X karyo-type (figure 5).[128-130] The RR of death has been found to be high(4.16; 95% CI 3.22–5.39), especially from causes such as aorticdissection, ischemic heart disease, congenital malformations ofthe heart, epilepsy and pneumonia,[130] while the rate of malig-nancy has been found to be low in three studies.[5,128,130] Diabetes
mellitus has in many cases been found to be an accompanyingcause of death.[128] Thus, increased mortality may be due to anumber of reasons: congenital malformations leading to prema-ture death (e.g. coarctation of the aorta); osteoporosis, becauseof lack of replacement therapy; hormonal or metabolic disease,especially type 2 diabetes mellitus; ischemic heart disease;chronic estrogen deficiency, due to insufficient HRT.
At present, there is a lack of longitudinal, observational andinterventional studies in adults with Turner syndrome. It is notknown how long-term HRT affects cardiovascular morbidity andmortality. Likewise, the question of when to stop HRT, if ever,is unresolved.
7. Cardiovascular Managementin Turner Syndrome
In the clinical practice careful monitoring of glucose meta-bolism, weight, thyroid function, bones, hepatic function andblood pressure should be performed in patients with Turner syn-drome. A cardiovascular risk profile should be determined at di-agnosis, and the patient should be informed about risks and ben-efits from GH and HRT. Patients should be seen by a cardiologistand have echocardiography performed, together with clinical ex-amination (table III). When pubertal induction is taking place, itmay be prudent to perform a new cardiovascular assessment, andlikewise in adulthood.[131] If any congenital cardiac malforma-tion is present, this should be dealt with appropriately (see section2), relevant examinations and tests performed, and the patientshould be followed up at regular intervals. Endocarditis prophy-laxis should be given in case of bicuspid aortic valves, and in caseof any surgical procedures having to be performed. The potentialconsequences of GH treatment on the heart and great vesselsshould be discussed, as well as consequences of HRT, and per-haps especially the consequences of not taking HRT. Based onthe available literature, HRT is highly recommended duringadulthood. The unsolved problem of who will eventually developdilation of the aorta, and thus be at great risk of later aortic dis-
Median survival: 45,X 66 years Other karyotypes 72 years p < 0.02
0 20 40 60 80 100
Sur
viva
l
Age (years)
Fig. 5. Kaplan-Meier survival plot of females with Turner syndrome with the 45,X
karyotype versus females with Turner syndrome with any other karyotype.[125]
Table III. Cardiovascular management of patients with Turner syndrome
Echocardiography at diagnosis should be performed in all patients
If congenital cardiac malformations are diagnosed, these should be dealt with appropriately, including: surgery, if deemed clinically necessary; regularclinical examinations (echocardiography, MRI scan, blood tests, BP, etc.); prophylaxis for infectious endocarditis (visits at the dentist, minor surgery, etc.)
The potential consequences of growth hormone treatment should be evaluated
The benefits and drawbacks of HRT should be discussed with the patient at a relevant age; at present, HRT is recommended
Evaluation of the aorta, with emphasis on aortic dilation, and the subsequent risk of aortic dissection
Cardiac monitoring prior to assisted reproductive therapy or spontaneous pregnancy, and during pregnancy
Risk of ischemic heart disease
BP at every visit at the physician
BP = blood pressure; HRT = hormone replacement therapy; MRI = magnetic resonance imaging.
Turner Syndrome and the Heart 409
© Adis International Limited. All rights reserved. Am J Cardiovasc Drugs 2002; 2 (6)

section, leaves the patient and her physician in a situation whererepeat echocardiography, at present, is the only solution. Cur-rently, it is not known how frequently echocardiography (and/orMRI) should be performed.
In adulthood, a new cardiovascular risk assessment shouldbe performed, and at every visit blood pressure should be moni-tored. It is recommended that special precautionary steps be takenbefore and during pregnancy, whether spontaneous or assisted,with cardiac monitoring (heart auscultation, blood pressure,echocardiography and/or MRI [only on vital indication duringpregnancy]) at regular intervals. Since general physicians onlyinfrequently encounter patients with Turner syndrome, it is rec-ommended that the care and treatment of Turner syndrome iscentralized in outpatient clinics devoted to the care of these girlsand women.
Acknowledgements
Claus Højbjerg Gravholt is supported by a research fellowship by theUniversity of Aarhus, by a grant from the Danish Diabetes Association, andthe Danish Health Research Council, grant number 9600822 (Aarhus Univer-sity – Novo Nordisk Center for Research in Growth and Regeneration).
Lone Svendsen, Karen Mathiasen, Joan Hansen, Lone Korsgaard, IbenChristensen, Kirsten Nyborg, Inga Bisgaard, and Merete Møller are thankedfor expert technical help. Line Gether and Solveig Skærlund are thanked forexpert secretarial help.
References1. Turner HH. A syndrome of infantilism, congenital webbed neck, and cubitus
valgus. Endocrinology 1938; 23: 566-74
2. Lippe B. Turner syndrome. Endocrinol Metab Clin North Am 1991; 20: 121-52
3. Sylven L, Hagenfeldt K, Brondum NK, et al. Middle-aged women with Turner’s
syndrome: medical status, hormonal treatment and social life. Acta Endocrinol
1991; 125: 359-65
4. Gotzsche CO, Krag-Olsen B, Nielsen J, et al. Prevalence of cardiovascular mal-
formations and association with karyotypes in Turner’s syndrome. Arch Dis
Child 1994; 71: 433-6
5. Gravholt CH, Juul S, Naeraa RW, et al. Morbidity in Turner syndrome. J Clin
Epidemiol 1998; 51: 147-58
6. Elsheikh M, Casadei B, Conway GS, et al. Hypertension is a major risk factor for
aortic root dilatation in women with Turner’s syndrome. Clin Endocrinol (Oxf)
2001; 54: 69-73
7. Jacobs PA, Melville M, Ratcliffe S, et al. A cytogenetic survey of 11 680 newborn
infants. Ann Hum Genet 1974; 37: 359-76
8. Hook EB, Warburton D. The distribution of chromosomal genotypes associated
with Turner’s syndrome: livebirth prevalence rates and evidence for dimin-
ished fetal mortality and severity in genotypes associated with structural X
abnormalities or mosaicism. Hum Genet 1983; 64: 24-7
9. Nielsen J, Wohlert M. Chromosome abnormalities found among 34,910 newborn
children: results from a 13-year incidence study in Arhus, Denmark. Hum
Genet 1991; 87: 81-3
10. Imaizumi K, Kuroki Y. Prevalence of Turner syndrome in Japan. Int Symposium
on Turner Syndrome: 1992; Japan, 3-6
11. Savendahl L, Davenport ML. Delayed diagnoses of Turner’s syndrome: proposed
guidelines for change. J Pediatr 2000; 137: 455-9
12. Sas TC, Muinck Keizer-Schrama SM, Stijnen T, et al. Normalization of height in
girls with Turner syndrome after long-term growth hormone treatment: results
of a randomized dose-response trial. J Clin Endocrinol Metab 1999; 84: 4607-12
13. Haddad HM, Wilkins L. Congenital anomalies associated with gonadal aplasia:
review of 55 cases. Pediatrics 1959; 23: 885-902
14. Lemli L, Smith DW. The XO syndrome: a study of the differentiated phenotype
in 25 patients. J Pediatr 1963; 63: 577-88
15. Nora JJ, Torres FG, Sinha AK, et al. Characteristic cardiovascular anomalies of
XO Turner syndrome, XX and XY phenotype and XO-XX Turner mosaic. Am
J Cardiol 1970; 25: 639-41
16. Rainier-Pope CR, Cummingham RD, Nadas AS, et al. Cardiovascular malforma-
tions in Turner’s syndrome. Pediatrics 1964; 19: 919-25
17. Mutinelli MR, Nizzoli G, Chiumello G, et al. Echocardiographic diagnosis of
congenital bicuspid aortic valves in gonadal dysgenesis. G Ital Cardiol 1986;
16: 496-8
18. Dawson-Falk KL, Wright AM, Bakker B, et al. Cardiovascular evaluation in
Turner syndrome: utility of MR imaging. Australas Radiol 1992; 36: 204-9
19. Berdahl LD, Wenstrom KD, Hanson JW. Web neck anomaly and its association
with congenital heart disease. Am J Med Genet 1995; 56: 304-7
20. Lacro RV, Jones KL, Benirschke K. Coarctation of the aorta in Turner syndrome:
a pathologic study of fetuses with nuchal cystic hygromas, hydrops fetalis, and
female genitalia. Pediatrics 1988; 81: 445-51
21. Clark EB. Neck web and congenital heart defects: a pathogenic association in 45
X-O Turner syndrome? Teratology 1984; 29: 355-61
22. Miller MJ, Geffner ME, Lippe BM, et al. Echocardiography reveals a high inci-
dence of bicuspid aortic valve in Turner syndrome. J Pediatr 1983; 102: 47-50
23. Sybert VP. Cardiovascular malformations and complications in Turner syndrome.
Pediatrics 1998; 101 (1): E11
24. Mazzanti L, Cacciari E. Congenital heart disease in patients with Turner’s syn-
drome. Italian Study Group for Turner Syndrome (ISGTS). J Pediatr 1998; 133:
688-92
25. Mazzanti L, Prandstraller D, Tassinari D, et al. Heart disease in Turner’s syn-
drome. Helv Paediatr Acta 1988; 43: 25-31
26. Lin AE, Lippe B, Rosenfeld RG. Further delineation of aortic dilation, dissection,
and rupture in patients with turner syndrome. Pediatrics 1998; 102 (1): e12
27. Larson EW, Edwards WD. Risk factors for aortic dissection: a necropsy study of
161 cases. Am J Cardiol 1984; 53: 849-55
28. Natowicz M, Chatten J, Clancy R, et al. Genetic disorders and major extracardiac
anomalies associated with the hypoplastic left heart syndrome. Pediatrics 1988;
82: 698-706
29. Greenlee R, Hoyme H, Witte M, et al. Developmental disorders of the lymphatic
system. Lymphology 1993; 26: 156-68
30. Barr Jr M, Oman-Ganes L. Turner syndrome morphology and morphometrics:
cardiac hypoplasia as a cause of midgestation death. Teratology 2002; 66:
65-72
31. Carrel L, Cottle AA, Goglin KC, et al. A first-generation X-inactivation profile
of the human X chromosome. Proc Natl Acad Sci U S A 1999; 96: 14440-4
32. Rao E, Weiss B, Fukami M, et al. Pseudoautosomal deletions encompassing a
novel homeobox gene cause growth failure in idiopathic short stature and
Turner syndrome. Nat Genet 1997; 16: 54-63
33. Ellison JW, Wardak Z, Young MF, et al. PHOG, a candidate gene for involvement
in the short stature of Turner syndrome. Hum Mol Genet 1997; 6: 1341-7
410 Gravholt
© Adis International Limited. All rights reserved. Am J Cardiovasc Drugs 2002; 2 (6)

34. Fang J, Dagenais SL, Erickson RP, et al. Mutations in FOXC2 (MFH-1), a forkhead
family transcription factor, are responsible for the hereditary lymphedema-dis-
tichiasis syndrome. Am J Hum Genet 2000; 67: 1382-8
35. Ogata T, Muroya K, Matsuo N, et al. Turner syndrome and Xp deletions: clinical
and molecular studies in 47 patients. J Clin Endocrinol Metab 2001; 86: 5498-508
36. Nathwani NC, Unwin R, Brook CG, et al. Blood pressure and Turner syndrome.
Clin Endocrinol (Oxf) 2000; 52: 363-70
37. Gravholt CH, Naeraa RW, Nyholm B, et al. Glucose metabolism, lipid metabolism,
and cardiovascular risk factors in adult Turner syndrome: the impact of sex
hormone replacement. Diabetes Care 1998; 21: 1062-70
38. Verdecchia P, Schillaci G, Gatteschi C, et al. Blunted nocturnal fall in blood pres-
sure in hypertensive women with future cardiovascular morbid events. Circula-
tion 1993; 88: 986-92
39. Verdecchia P, Schillaci G, Boldrini F, et al. Sex, cardiac hypertrophy and diurnal
blood pressure variations in essential hypertension. J Hypertens 1992; 10: 683-92
40. Verdecchia P, Schillaci G, Guerrieri M, et al. Circadian blood pressure changes
and left ventricular hypertrophy in essential hypertension. Circulation 1990; 81:
528-36
41. Ross JL, Feuillan P, Long LM, et al. Lipid abnormalities in Turner syndrome. J
Pediatr 1995; 126: 242-5
42. Gravholt CH, Klausen IC, Weeke J, et al. Lp(a) and lipids in adult Turner’s syn-
drome: impact of treatment with 17beta-estradiol and norethisterone. Athero-
sclerosis 2000; 150: 201-8
43. Dean JW, Fowler PB. Exaggerated responsiveness to thyrotrophin releasing hor-
mone: a risk factor in women with coronary artery disease. BMJ 1985; 290:
1555-61
44. Arem R, Patsch W. Lipoprotein and apolipoprotein levels in subclinical hypothy-
roidism: effect of levothyroxine therapy. Arch Intern Med 1990; 150: 2097-100
45. Ivarsson SA, Ericsson UB, Nilsson KO, et al. Thyroid autoantibodies, Turner’s
syndrome and growth hormone therapy. Acta Paediatr 1995; 84: 63-5
46. Van Campenhout J, Antaki A, Rasio E. Diabetes mellitus and thyroid autoimmunity
in gonadal dysgenesis. Fertil Steril 1973; 24: 1-9
47. Williams ED, Engel E, Forbes AP. Thyroiditis and al dysgenesis. N Engl J Med
1964; 270: 805-10
48. Pai GS, Leach DC, Weiss L, et al. Thyroid abnormalities in 20 children with Turner
syndrome. J Pediatr 1977; 91: 267-9
49. Bright GM, Blizzard RM, Kaiser DL, et al. Organ-specific autoantibodies in chil-
dren with common endocrine diseases. J Pediatr 1982; 100: 8-14
50. Germain EL, Plotnick LP. Age-related anti-thyroid antibodies and thyroid abnor-
malities in Turner syndrome. Acta Paediatr Scand 1986; 75: 750-5
51. Fleming S, Cowell C, Bailey J, et al. Hashimoto’s disease in Turner’s syndrome.
Clin Invest Med 1988; 11: 243-6
52. Gruneiro PL, Iorcansky S, Coco R, et al. High incidence of thyroid disturbances in
49 children with Turner syndrome. J Pediatr 1987; 111: 258-61
53. Radetti G, Mazzanti L, Paganini C, et al. Frequency, clinical and laboratory features
of thyroiditis in girls with Turner’s syndrome. The Italian Study Group for
Turner’s Syndrome. Acta Paediatr 1995; 84: 909-12
54. Marner B, Bille G, Christy M, et al. Islet cell cytoplasmic antibodies (ICA) in
diabetes and disorders of glucose tolerance. Diabet Med 1991; 8: 812-6
55. Emans SJ, Grace E, Hoffer FA, et al. Estrogen deficiency in adolescents and young
adults: impact on bone mineral content and effects of estrogen replacement
therapy. Obstet Gynecol 1990; 76: 585-92
56. Larizza D, Martinetti Bianchi M, et al. Autoimmunity, HLA, Gm and Km poly-
morphisms in Turner’s syndrome. Autoimmunity 1989; 4: 69-78
57. Chiovato L, Larizza D, Bendinelli G, et al. Autoimmune hypothyroidism and hy-
perthyroidism in patients with Turner’s syndrome. Eur J Endocrinol 1996; 134:
568-75
58. Elsheikh M, Wass JA, Conway GS. Autoimmune thyroid syndrome in women with
Turner’s syndrome-the association with karyotype. Clin Endocrinol (Oxf) 2001;
55: 223-6
59. Jeresaty RM, Basu SK, Franco J. Dissecting aneurysm of the aorta in Turner’s
syndrome. JAMA 1972; 222: 574-6
60. Strader III WJ, Wachtel HL, Lundberg Jr GD. Hypertension and aortic rupture in
gonadal dysgenesis. J Pediatr 1971; 79: 473-5
61. Youker JE, Roe BB. Aneurysm of the aortic sinuses and ascending aorta in Turner’s
syndrome. Am J Cardiol 1969; 23: 89-93
62. Cecchi F, Samoun M, Santoro G, et al. Chronic dissecting aortic aneurysm and
Turner’s syndrome: apropos of a case. Arch Mal Coeur Vaiss 1992; 85: 1043-6
63. Kusaba E, Imada T, Iwakuma A, et al. Aortic aneurysm complicated with coarcta-
tion of the aorta and Turner syndrome. Kyobu Geka 1995; 48: 1115-7
64. Ota Y, Tsunemoto M, Shimada M, et al. Aortic dissection associated with Turner’s
syndrome. Kyobu Geka 1992; 45: 411-4
65. Oohara K, Yamazaki T, Sakaguchi K, et al. Acute aortic dissection, aortic insuffi-
ciency, and a single coronary artery in a patient with Turner’s syndrome. J
Cardiovasc Surg (Torino) 1995; 36: 273-5
66. Imamura M, Aoki H, Eya K, et al. Balloon angioplasty before Wheat’s operation
in a patient with Turner’s syndrome. Cardiovasc Surg 1995; 3: 70-2
67. Lie JT. Aortic dissection in Turner’s syndrome. Am Heart J 1982; 103: 1077-80
68. Price WH, Wilson J. Dissection of the aorta in Turner’s syndrome. J Med Genet
1983; 20: 61-3
69. Slater DN, Grundman MJ, Mitchell L. Turner’s syndrome associated with bicuspid
aortic stenosis and dissecting aortic aneurysm. Postgrad Med J 1982; 58: 436-8
70. Kostich ND, Opitz JM. Ullrich-Turner syndrome associated with cystic medial
necrosis of the aorta and great vessels. Am J Med 1965; 38: 943-9
71. Edwards WD, Leaf DS, Edwards JE. Dissecting aortic aneurysm associated with
congenital bicuspid aortic valve. Circulation 1978; 57: 1022-5
72. Asch AJ. Turner’s syndrome occurring with Horner’s syndrome: seen with coarc-
tation of the aorta and aortic aneurysm. Am J Dis Child 1979; 133: 827-30
73. Ravelo HR, Stephenson LW, Friedman S, et al. Coarctation resection in children
with Turner’s syndrome: a note of caution. J Thorac Cardiovasc Surg 1980; 80:
427-30
74. Kido G, Miyagi A, Shibuya T, et al. Turner’s syndrome with pituitary hyperplasia:
a case report. No Shinkei Geka 1994; 22: 333-8
75. Rubin K. Aortic dissection and rupture in Turner syndrome [letter]. J Pediatr 1993;
122: 670
76. Ohuchi H, Kawazoe K, Kosakai Y, et al. One-staged repair for coarctation of the
aorta and annuloaortic ectasia with severe aortic regurgitation in a patient with
Turner syndrome. Nippon Kyobu Geka Gakkai Zasshi 1992; 40: 2247-51
77. Pollak H, Veit F, Enenkel W. Presumed "successful" fibrinolysis in unrecognized
acute aortic dissection. Dtsch Med Wochenschr 1992; 117: 368-71
78. Martin MM, Beekman RH, Rocchini AP, et al. Aortic aneurysms after subclavian
angioplasty repair of coarctation of the aorta. Am J Cardiol 1988; 61: 951-3
79. Bartlema KA, Hogervorst M, Akkersdijk GJ, et al. Isolated abdominal aortic dis-
section in a patient with Turner’s syndrome [letter]. Surgery 1995; 117: 116-7
80. Apostolopoulos T, Kyriakidis M, Toutouzas P. Endarteritis of the aortic arch in
Turner’s syndrome with cystic degeneration of the aorta. Int J Cardiol 1992; 35:
417-9
Turner Syndrome and the Heart 411
© Adis International Limited. All rights reserved. Am J Cardiovasc Drugs 2002; 2 (6)

81. Allemann J, Muller G, Legat M. Rare variant of a Turner-Ullrich syndrome.
Schweiz Med Wochenschr 1982; 112: 1249-55
82. Buheitel G, Singer H, Hofbeck M. Aortic aneurysms in Ullrich-Turner syndrome.
Klin Padiatr 1996; 208: 42-5
83. Akimoto N, Shimizu T, Ishikawa M, et al. The surgical treatment of aortic dissec-
tion in a patient with Turner’s syndrome: report of a case. Surg Today 1994;
24: 929-32
84. Meunier JP, Jazayeri S, David M. Acute type A aortic dissection in an adult patient
with Turner’s syndrome. Heart 2001; 86 (5): 546
85. Anabtawi IN, Ellison RG, Yeh TJ, et al. Dissecting aneurysm of aorta associated
with Turner’s syndrome. J Thorac Cardiovasc Surg 1964; 47: 750-4
86. Roberts WC. Aortic dissection: anatomy, consequences, and causes. Am Heart J
1981; 101: 195-214
87. Spittell PC, Spittell Jr JA, Joyce JW, et al. Clinical features and differential diag-
nosis of aortic dissection: experience with 236 cases (1980 through 1990).
Mayo Clin Proc 1993; 68: 642-51
88. Prandstraller D, Mazzanti L, Picchio FM, et al. Turner’s syndrome: cardiologic
profile according to the different chromosomal patterns and long-term clinical
follow-up of 136 nonpreselected patients. Pediatr Cardiol 1999; 20: 108-12
89. Nielsen J, Sillesen I, Hansen KB. Fertility in women with Turner’s syndrome: case
report and review of literature. Br J Obstet Gynaecol 1979; 86: 833-5
90. Hovatta O. Pregnancies in women with Turner’s syndrome. Ann Med 1999; 31:
106-10
91. Foudila T, Soderstrom AV, Hovatta O. Turner’s syndrome and pregnancies after
oocyte donation. Hum Reprod 1999; 14: 532-5
92. Swapp GH, Johnston AW, Watt JL, et al. A fertile woman with non-mosaic Turn-
er’s syndrome: case report and review of the literature. Br J Obstet Gynaecol
1989; 96: 876-80
93. Kaneko N, Kawagoe S, Hiroi M. Turner’s syndrome: review of the literature with
reference to a successful pregnancy outcome. Gynecol Obstet Invest 1990; 29:
81-7
94. Birdsall M, Kennedy S. The risk of aortic dissection in women with Turner syn-
drome [letter]. Hum Reprod 1996; 11: 1587
95. Nagel TC, Tesch LG. ART and high risk patients [letter]. Fertil Steril 1997; 68:
748-9
96. Beauchesne LM, Connolly HM, Ammash NM, et al. Coarctation of the aorta:
outcome of pregnancy. J Am Coll Cardiol 2001; 38: 1728-33
97. Weytjens C, Bove T, Van Der NP. Aortic dissection and Turner’s syndrome. J
Cardiovasc Surg (Torino) 2000; 41: 295-7
98. Ranke MB, Pfluger H, Rosendahl W, et al. Turner syndrome: spontaneous growth
in 150 cases and review of the literature. Eur J Pediatr 1983; 141: 81-8
99. Karlberg J, Albertsson WK, Nilsson KO, et al. Growth in infancy and childhood
in girls with Turner’s syndrome. Acta Paediatr Scand 1991; 80: 1158-65
100. Davenport ML, Punyasavatsut N, Gunther D, et al. Turner syndrome: a pattern of
early growth failure. Acta Paediatr Suppl 1999; 88: 118-21
101. Lyon AJ, Preece MA, Grant DB. Growth curve for girls with Turner syndrome.
Arch Dis Child 1985; 60: 932-5
102. Pasquino AM, Passeri F, Pucarelli I, et al. Spontaneous pubertal development in
Turner’s syndrome. Italian Study Group for Turner’s Syndrome. J Clin En-
docrinol Metab 1997; 82: 1810-3
103. Massarano AA, Brook CG, Hindmarsh PC, et al. Growth hormone secretion in
Turner’s syndrome and influence of oxandrolone and ethinyl oestradiol. Arch
Dis Child 1989; 64: 587-92
104. Reiter JC, Craen M, Van Vliet G. Decreased growth hormone response to growth
hormone-releasing hormone in Turner’s syndrome: relation to body weight and
adiposity. Acta Endocrinol 1991; 125: 38-42
105. Ranke MB, Blum WF, Haug F, et al. Growth hormone, somatomedin levels and
growth regulation in Turner’s syndrome. Acta Endocrinol 1987; 116: 305-13
106. Saenger P, Schwartz E, Wiedemann E, et al. The interaction of growth hormone,
somatomedin and oestrogen in patients with Turner’s syndrome. Acta Endo-
crinol 1976; 81: 9-18
107. Wit JM, Massarano AA, Kamp GA, et al. Growth hormone secretion in patients
with Turner’s syndrome as determined by time series analysis. Acta Endocrinol
1992; 127: 7-12
108. Hochberg Z, Aviram M, Rubin D, et al. Decreased sensitivity to insulin-like
growth factor I in Turner’s syndrome: a study of monocytes and T lymphocytes.
Eur J Clin Invest 1997; 27: 543-7
109. Swearingen B, Barker FG, Katznelson L, et al. Long-term mortality after trans-
sphenoidal surgery and adjunctive therapy for acromegaly. J Clin Endocrinol
Metab 1998; 83: 3419-26
110. Colao A, Cuocolo A, Marzullo P, et al. Is the acromegalic cardiomyopathy revers-
ible? Effect of 5-year normalization of growth hormone and insulin-like growth
factor I levels on cardiac performance. J Clin Endocrinol Metab 2001; 86:
1551-7
111. Caprio S, Boulware SD, Press M, et al. Effect of growth hormone treatment on
hyperinsulinemia associated with Turner syndrome. J Pediatr 1992; 120: 238-43
112. Saenger P, Attie KM, DiMartino Nardi J, et al. Carbohydrate metabolism in chil-
dren receiving growth hormone for 5 years: chronic renal insufficiency com-
pared with growth hormone deficiency, Turner syndrome, and idiopathic short
stature. Genentech Collaborative Group. Pediatr Nephrol 1996; 10: 261-3
113. Gravholt CH, Naeraa RW. Reference values for body proportions and body com-
position in adult women with Turner’s syndrome. Am J Med Genet 1997; 72:
403-8
114. Bordeleau L, Cwinn A, Turek M, et al. Aortic dissection and Turner’s syndrome:
case report and review of the literature. J Emerg Med 1998; 16: 593-6
115. Sas TC, Cromme-Dijkhuis AH, de Muinck K, et al. The effects of long-term
growth hormone treatment on cardiac left ventricular dimensions and blood
pressure in girls with Turner’s syndrome. J Pediatr 1999; 135: 470-6
116. Nathwani NC, Unwin R, Brook CG, et al. The influence of renal and cardiovas-
cular abnormalities on blood pressure in Turner syndrome. Clin Endocrinol
(Oxf) 2000; 52: 371-7
117. Sack MN, Rader DJ, Cannon RO. Oestrogen and inhibition of oxidation of low-
density lipoproteins in postmenopausal women. Lancet 1994; 343: 269-70
118. Gilligan DM, Quyyumi AA, Cannon RO. Effects of physiological levels of estro-
gen on coronary vasomotor function in postmenopausal women. Circulation
1994; 89: 2545-51
119. Losordo DW, Kearney M, Kim EA, et al. Variable expression of the estrogen
receptor in normal and atherosclerotic coronary arteries of premenopausal
women. Circulation 1994; 89: 1501-10
120. Selzman CH, Gaynor JS, Turner AS, et al. Ovarian ablation alone promotes aortic
intimal hyperplasia and accumulation of fibroblast growth factor. Circulation
1998; 98: 2049-54
121. Elsheikh M, Bird R, Casadei B, et al. The effect of hormone replacement therapy
on cardiovascular hemodynamics in women with Turner’s syndrome. J Clin
Endocrinol Metab 2000; 85: 614-8
412 Gravholt
© Adis International Limited. All rights reserved. Am J Cardiovasc Drugs 2002; 2 (6)

122. Seely EW, Walsh BW, Gerhard MD, et al. Estradiol with or without progesterone
and ambulatory blood pressure in postmenopausal women. Hypertension 1999;
33: 1190-4
123. Gravholt CH, Naerra RW, Fisher S, et al. Body composition and physical fitness
are major determinants of the growth hormone_IGF axis aberrations in adult
Turner syndrome, with important modulations by treatment with 17-Beta-Estra-
diol. J Clin Endocrinol Metab 1997; 82: 2570-7
124. Risks and benefits of estrogen plus progestin in healthy postmenopausal women:
principal results from the Women’s Health Initiative randomized controlled
trial. JAMA 2002; 288: 321-33
125. Hulley S, Grady D, Bush T, et al. Randomized trial of estrogen plus progestin for
secondary prevention of coronary heart disease in postmenopausal women.
Heart and Estrogen/progestin Replacement Study (HERS) Research Group.
JAMA 1998; 280: 605-13
126. Viscoli CM, Brass LM, Kernan WN, et al. A clinical trial of estrogen-replacement
therapy after ischemic stroke. N Engl J Med 2001; 345: 1243-9
127. Reaven GM. Banting lecture 1988. Role of insulin resistance in human disease.
Diabetes 1988; 37: 1595-607
128. Naeraa RW, Gravholt CH, Hansen J, et al. Mortality in Turner syndrome. In:
Albertsson-Wikland K, Ranke MB, editors. Turner syndrome in a life span
perspective: research and clinical aspects. Amsterdam: Elsevier, 1995: 323
129. Price WH, Clayton JF, Collyer S, et al. Mortality ratios, life expectancy, and causes
of death in patients with Turner’s syndrome. J Epidemiol Community Health
1986; 40: 97-102
130. Swerdlow AJ, Hermon C, Jacobs PA, et al. Mortality and cancer incidence in
persons with numerical sex chromosome abnormalities: a cohort study. Ann
Hum Genet 2001; 65: 177-88
131. Saenger P, Wikland KA, Conway GS, et al. Recommendations for the diagnosis
and management of Turner syndrome. J Clin Endocrinol Metab 2001; 86: 3061-9
Correspondence and offprints: Dr Claus Højbjerg Gravholt, Medical Depart-ment M (Endocrinology and Diabetes), Aarhus Kommunehospital, DK-8000Aarhus C, Denmark. E-mail: [email protected]
Turner Syndrome and the Heart 413
© Adis International Limited. All rights reserved. Am J Cardiovasc Drugs 2002; 2 (6)