Embed Size (px)
Citation preview

Placenta 28 (2007) 47e51
Twin AnemiaePolycythemia Sequence in Two MonochorionicTwin Pairs Without Oligo-Polyhydramnios Sequence
E. Lopriore MD a,*, J.M. Middeldorp MD b, D. Oepkes MD, PhD b, H.H. Kanhai MD, PhD b,F.J. Walther MD, PhD a, F.P.H.A. Vandenbussche MD, PhD b
a Division of Neonatology, Department of Pediatrics, Leiden University Medical Center, Leiden, The Netherlandsb Division of Fetal Medicine, Department of Obstetrics, Leiden University Medical Center, Leiden, The Netherlands
Accepted 18 January 2006
Abstract
Placental vascular anastomoses in monochorionic twins may lead to acute or chronic inter-twin transfusion. We report an uncommon form ofchronic inter-twin transfusion, referred to as twin anemiaepolycythemia sequence (TAPS), with severe anemia in one twin and polycythemia inthe other, without the characteristically associated twin oligo-polyhydramnios sequence (TOPS) seen in the classical twin-to-twin transfusionsyndrome (TTTS). The clinical course and placental characteristics of two pairs of monochorionic twins with TAPS born at, respectively, 33and 34 weeks’ gestation were reviewed. Serial fetal ultrasound examinations revealed no signs of TOPS. At birth, both donor twins were severelyanemic requiring blood transfusion and both recipients were polycythemic, one requiring partial volume exchange transfusions. Inter-twin dif-ference in reticulocyte counts was extremely high, suggesting a chronic form of inter-twin blood transfusion. Placental injection studies revealeda preponderance of very small (<1 mm) arterio-venous anastomoses in one direction. In conclusion, chronic inter-twin transfusion may lead toan uncommon form of inter-twin transfusion, named TAPS, not associated with TOPS, resulting in severe fetal or neonatal hematological com-plications. We hypothesize that TAPS is mediated through minuscule unidirectional anastomoses. TAPS can be diagnosed antenatally withDoppler studies and postnatally by hemoglobin and reticulocyte measurements.� 2006 Elsevier Ltd. All rights reserved.
Keywords: Chronic twin-to-twin transfusion syndrome; Oligo-polyhydramnios sequence; Anemia; Polycythemia; Vascular anastomoses
1. Introduction
Twin-to-twin transfusion syndrome (TTTS) is a heteroge-neous disease affecting monochorionic twin pregnancies andresults from hemodynamic imbalance due to placental vascu-lar anastomoses [1,2]. Various forms of TTTS have been de-scribed: acute perimortem TTTS, acute perinatal TTTS andchronic TTTS. Acute perimortem TTTS occurs after intrauter-ine fetal demise of a co-twin and is due to acute exsanguina-tion from the surviving twin into the low-pressure circulationof the demising co-twin. Acute perinatal TTTS may occur
* Corresponding author. E. Lopriore, MD, Division of Neonatology, Depart-
ment of Pediatrics, J6-S, Leiden University Medical Center, albinusdreef 2, PO
Box 9600, 2300 RC, Leiden, The Netherlands. Tel.: þ31-71-5262909; fax:
þ31-71-5248199.
E-mail address: [email protected] (E. Lopriore).
0143-4004/$ - see front matter � 2006 Elsevier Ltd. All rights reserved.
doi:10.1016/j.placenta.2006.01.010
during birth due to acute inter-twin shifts of blood resultingfrom blood pressure differences associated with uterine con-tractions or changes in fetal position. Both acute forms ofTTTS are mediated through superficial arterio-arterial andveno-venous anastomoses [3e5]. The most common form ofTTTS, referred to as chronic TTTS, occurs usually duringthe second trimester of pregnancy and affects 15% of mono-chorionic twin pregnancies. Chronic TTTS results fromchronic inter-twin transfusion of blood mediated through arte-rio-venous anastomoses [2]. Chronic TTTS itself is alsoa highly heterogeneous disease and may be staged using Quin-tero’s classification based on ultrasound criteria [6]. ChronicTTTS is diagnosed when antenatal sonographic evidence oftwin oligo-polyhydramnios sequence (TOPS) is found[1,2,7e10]. TOPS is defined by the deepest vertical pool of�2 cm and �8 cm in the donor’s and recipient’s amnioticsac, respectively [1,2,8,9].

48 E. Lopriore et al. / Placenta 28 (2007) 47e51
We report two cases of monochorionic twins with an un-usual form of chronic TTTS. Both cases had hematological ev-idence of severe chronic inter-twin transfusion but noantenatal sonographic signs of TOPS. Placental injection stud-ies revealed a preponderance of very small (<1 mm) arterio-venous anastomoses in one direction.
2. Case presentation
2.1. Case 1
A 35-year-old gravida 2 para 1 was referred at 27þ 1weeks’ gestation with a dichorionicetriamniotic triplet preg-nancy after in vitro fertilization. Weekly ultrasound examina-tion throughout pregnancy showed no signs of TTTS (lastultrasound examination was performed at 33þ 1 weeks’ ges-tation). Doppler measurement of the middle cerebral arterypeak systolic velocity (MCA-PSV) showed a mild increase(1.2 multiples of median) in one of the monochorionic fetuses(maximum velocity of 58 cm/s at 33þ 1 weeks’ gestation).Labor was induced and three girls were born vaginally at34þ 0 weeks’ gestation. The last two girls were the mono-chorionic twin pair. The second-born infant was pale andweighed 1725 g (between 9th and 25th percentiles for gesta-tional age). The third-born infant was plethoric and weighed1695 g (9th percentile for gestational age). Birth weight dis-cordance was 2%. Apgar scores were 8/9/10 and 7/8/8 forthe second-born and third-born infants, respectively. Hemoglo-bin values for twin 2 and twin 3 were 7.6 g/dL (<5th percen-tile for gestational age) and 21.7 g/dL (>95th percentile forgestational age) with reticulocyte counts of 21% (absolute re-ticulocyte count 399� 103/mm3) and 4% (absolute reticulocyte
count 181� 103/mm3), respectively. The anemic infant, whowas also the fetus with increased MCA-PSV, required a bloodtransfusion on day 1. No signs of acute hemorrhagic hypovo-lemic shock at birth (heart rate 140 bpm, blood pressure 44/35 mmHg) were present in the anemic infant. No evidenceof placental abruption was found and none of the infantswere hypoxic at birth. KleihauereBetke test was not done.The hematocrit value in the co-twin increased up to 69% onday 1, but the infant remained asymptomatic and did not re-quire a partial volume exchange transfusion. Cranial ultra-sound examination in both twins was normal and furtherneonatal course was uneventful.
Macroscopic placental examination showed a velamentousinsertion of the umbilical cord of twin 3 and an injection studywith colored dye revealed five very small (<1 mm) arterio-ve-nous anastomoses (<1 mm) from twin 2 to twin 3 (Figs. 1 and 2).
2.2. Case 2
A 31-year-old gravida 5 para 3 was referred to our center at16 weeks’ gestation with a twin pregnancy. The twin pregnancyhad been diagnosed as dichorionic in the referring hospitalbased on an ultrasound examination at 10 weeks’ gestation.The course of the pregnancy was uneventful and no signs sug-gestive of TTTS were found on monthly ultrasound examina-tion. MCA-PSV measurements were not done. One day afterthe last ultrasound examination at 33þ 3 weeks’ gestation,spontaneous rupture of membranes occurred, followed by thebirth of two boys. The first-born infant was pale and weighed1880 g (between 9th and 25th percentiles for gestational age).The second-born twin was extremely plethoric and weighed1980 g (between 25th and 50th percentiles for gestational
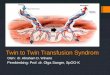
Fig. 1. Case 1. Triplet placenta after injection with colored dye. There is a monochorionic placenta (left-bottom side of the picture) and a fused dichorionic placenta
(top-right) (blue for arteries and orange or yellow for veins). The five anastomoses from donor to recipient are in the white square that is enlarged in Fig. 2 (For
interpretation of the references to colour in this figure legend, the reader is referred to the web version of this article.).

49E. Lopriore et al. / Placenta 28 (2007) 47e51
age). Birth weight discordance was 5%. Apgar scores were 8/9/9 and 7/8/8 for the first-born and second-born infant, respec-tively. Hemoglobin values for twin 1 and twin 2 were 6.0 g/dL(<5th percentile for gestational age) and 26.3 g/dL (>95th per-centile for gestational age) with reticulocyte counts of 30%(absolute reticulocyte count 525� 103/mm3) and 3% (absolutereticulocyte count 192� 103/mm3), respectively. The anemicinfant had no signs of acute hemorrhagic hypovolemic shockat birth (heart rate 120 bpm; blood pressure 51/37 mmHg) butrequired a blood transfusion on day 1. No clinical or laboratoryevidence of placental abruption was found. KleihauereBetke
Fig. 2. Case 1. The sky-blue arrows indicate five very small (<1 mm) arterio-
venous anastomoses from twin 2 (donor) to twin 3 (recipient) (For interpreta-
tion of the references to colour in this figure legend, the reader is referred to
the web version of this article.).
test was not performed. The second-born twin required oxygenadministration and ventilatory support with CPAP due to cya-nosis and respiratory failure. Severe hypoglycemia was cor-rected by intravenous glucose infusions. The hematocritincreased up to 90% on day 1 and two partial volume exchangetransfusions were performed because of symptomatic polycy-themia-hyperviscosity syndrome. Cranial ultrasound showedpersistent bilateral periventricular echodensities in both twins.
At macroscopic examination, the placenta was monochor-ionicediamniotic. Colored-dye injection showed four verysmall (<1 mm) arterio-venous anastomoses from twin 1 totwin 2 and one very small (<1 mm) arterio-venous anastomo-sis from twin 2 to twin 1 (Figs. 3 and 4). Microscopic exam-ination showed that the dividing membrane was diamniotic.
3. Comment
In this study, we found evidence that monochorionic twinpregnancies without signs of TOPS can still be affected bychronic inter-twin transfusion resulting in severe fetal or neona-tal hematological complications. We have named this conditiontwin anemiaepolycythemia sequence (TAPS). Differential di-agnosis in monochorionic twins with highly discordant hemo-globin values at birth includes acute peripartum TTTS,chronic TTTS with TOPS and chronic TTTS with TAPS.
Other possible causes for isolated anemia or polycythemiashould also be ruled out. Chronic anemia in newborns may resultfrom partial placental abruption, infection or chronic feto-maternal hemorrhage. Unfortunately, KleihauereBetke test wasnot performed in our two cases, which is a limitation of ourstudy. However, the associated combination with polycythemia
Fig. 3. Case 2. Monochorionic placenta after injection with colored dye (blue or green for arteries and orange or yellow for veins). The five small arterio-venous
anastomoses are only visible after enlargement. The four anastomoses from donor to recipient are in the white square that is enlarged in Fig. 4 (the single anas-
tomosis from recipient to donor is not in the white square) (For interpretation of the references to colour in this figure legend, the reader is referred to the web
version of this article.).

50 E. Lopriore et al. / Placenta 28 (2007) 47e51
in the co-twin clearly suggests a form of feto-fetal transfusionrather than feto-maternal transfusion. Common causes for poly-cythemia should also be excluded, such as chronic hypoxia as-sociated with intrauterine growth retardation. Polycythemiadue to chronic in utero hypoxia results from increased erythro-poietin levels and reticulocytosis [11,12]. Reticulocyte countsin the polycythemic infants in our reported cases were normalfor gestational age, suggesting that polycythemia resultedfrom chronic inter-twin transfusion rather than from increasederythropoiesis secondary to chronic hypoxia.
A first possible diagnosis in both reported cases is that ofacute peripartum TTTS. However, the anemic infant in acuteperipartum TTTS has clinical signs of hemorrhagic hypovole-mic shock such as pallor, tachycardia and hypotension [2,3].Also, reticulocyte counts after acute blood loss are typicallynot increased due to lack of time for compensatory hematopoi-esis. Although it is difficult to completely rule out an acuteperipartum TTTS event in our cases, acute peripartum TTTSshould be disregarded for several reasons. First, no clinicalsigns of acute perinatal blood loss were found in the anemicinfants. Second, very high reticulocyte counts were measuredin both anemic infants, suggestive of chronic rather than acuteblood loss. Finally, acute peripartum TTTS is mediatedthrough (large) superficial anastomoses [3,4]. Placental injec-tion studies in both reported cases showed only minusculearterio-venous anastomoses without superficial anastomoses.Small-caliber anastomoses have a high vascular resistanceand theoretically do not allow large amounts of blood volumeto be transfused acutely from one twin to the other (accordingto Poisseuille’s law of fluid dynamics).
A second possible diagnosis, that of the common form ofchronic TTTS can be disregarded due to absence of the typicalsigns of TOPS. We suggest therefore that atypical forms ofchronic TTTS without TOPS, but associated with anemia inone twin and polycythemia in the other, be referred to asTAPS. TAPS differs significantly in terms of diagnosis and
Fig. 4. Case 2. The sky-blue arrows indicate four small arterio-venous anasto-
moses from twin 1 (donor) to twin 2 (recipient) (For interpretation of the ref-
erences to colour in this figure legend, the reader is referred to the web version
of this article.).
management from the typical form of chronic TTTS with thecharacteristic signs of TOPS. Therefore, a clear distinction be-tween TAPS and TOPS is clinically more useful and reflectsmore accurately the heterogeneity of TTTS. TAPS may occurspontaneously (natural form) as reported in this study, but mayalso develop after laser surgery (iatrogenic form). Recent reportssuggest that the iatrogenic form of TAPS may occur in up to 13%of cases after laser surgery [13,14]. Interestingly, in iatrogenicTAPS, it is usually the former recipient who becomes anemic,whereas the former donor becomes polycythemic [13,14].
Most authors consider the presence of TOPS to be the ma-jor diagnostic criterion for chronic TTTS [1,2,8,9]. Marked fe-tal growth discordances and inter-fetal hemoglobin differencesmay also be present, but these features are not considered keyelements in the diagnosis of chronic TTTS [1,7,9]. Dopplerstudies are a standard requirement to determine Quintero stag-ing once chronic TTTS is diagnosed [1,8] and are also helpfulin the diagnosis of fetal anemia after single intrauterine fetaldeath (acute perimortem TTTS) [15]. Routine Doppler studiesare also recommended after laser surgery to rule out fetal ane-mia [13,14].
We suggest that Doppler studies and MCA-PSV measure-ments also be performed during each follow-up visit in all un-complicated monochorionic twin pregnancies, even in theabsence of TOPS. Signs of fetal anemia in a monochorionictwin should then alert the perinatologist of the possibility ofTAPS. Fetal anemia may affect cerebral oxygenation and re-sults in hypoxic-ischemic cerebral injury, whereas polycythe-mia has been suggested to cause cerebral injury in TTTS byvascular sludging [16]. Hypothetically, TAPS may also be re-sponsible for some cases of unexplained fetal demise in mono-chorionic pregnancies without signs of chronic TTTS.
Whether TAPS is associated with increased mortality ormorbidity is not known. If so, invasive procedures such as fe-toscopic laser surgery, intrauterine blood transfusion or a com-bination of both, may improve outcome. At present, however,we think that invasive procedures are not indicated because therisk of procedure-related complications may outweigh the riskof mortality or morbidity.
There are several hypotheses on the origin of inter-twin am-niotic discordances in the common form of chronic TTTS withTOPS [2]. It is, however, not yet clear why there are no inter-twin amniotic fluid discordances in TAPS. One of the commondenominators between the two reported cases is the preponder-ance of very small (<1 mm) arterio-venous anastomoses inone direction. Vascular resistance in small-caliber vessels ishigher than in larger vessels and reduces the volume of fluidpassage (Poisseuille’s law). We hypothesize that if onlya few very small placental vascular anastomoses are present,inter-twin blood transfusion occurs very slowly and allowsmore time for hemodynamic compensatory mechanisms totake place. Activation or inactivation of the renineangiotensinsystem may then induce the hypovolemic donor and the hyper-volemic recipient to remain euvolemic, which in turn explainsthe absence of TOPS. However, compensatory hematopoiesismay not be sufficient to prevent severe anemia in the donor,despite the extremely high reticulocyte count. Another

51E. Lopriore et al. / Placenta 28 (2007) 47e51
possible explanation is that the reported infants were born be-fore TOPS had time to develop. Inter-twin hemoglobin discor-dance and amniotic fluid discordance vary with the state ofprogression of chronic TTTS [7]. It is conceivable that sometwins with chronic TTTS may first develop TAPS and thenTOPS. As placental blood vessels enlarge throughout preg-nancy, these vessels may eventually become just large enoughto produce TAPS at a certain point in gestation, but not beforethis time. Regardless of the various hypotheses, our under-standing of TAPS is clearly still incomplete.
In conclusion, perinatologists involved in the care of mono-chorionic twins should maintain a high index of suspicion, asantenatal ultrasound examination without Doppler studiesdoes not rule out a chronic form of inter-twin transfusion.TAPS can occur in the absence of the characteristic inter-twin discordance in amniotic fluid volumes. TAPS should bediagnosed when large inter-twin discordance in fetal or neona-tal hemoglobin levels and reticulocyte counts is found, in theabsence of TOPS. Placental injection studies may then reveala preponderance of very small arterio-venous anastomoses inone direction.
References
[1] Huber A, Hecher K. How can we diagnose and manage twinetwin trans-
fusion syndrome? Best Pract Res Clin Obstet Gynaecol 2004;18:543e56.
[2] Lopriore E, Vandenbussche FP, Tiersma ES, de Beaufort AJ, de
Leeuw JP. Twin-to-twin transfusion syndrome: new perspectives.
J Pediatr 1995;127:675e80.
[3] Lopriore E, Sueters M, Middeldorp JM, Vandenbussche FP, Walther FJ.
Haemoglobin differences at birth in monochorionic twins without chronic
twin-to-twin transfusion syndrome. Prenat Diagn 2005;25:844e50.
[4] Danskin FH, Neilson JP. Twin-to-twin transfusion syndrome: what are
appropriate diagnostic criteria? Am J Obstet Gynecol 1989;161:365e9.
[5] Duncan KR, Denbow ML, Fisk NM. The aetiology and management of
twinetwin transfusion syndrome. Prenat Diagn 1997;17:1227e36.
[6] Quintero RA, Morales WJ, Allen MH, Bornick PW, Johnson PK,
Kruger M. Staging of twinetwin transfusion syndrome. J Perinatol
1999;19:550e5.
[7] Denbow M, Fogliani R, Kyle P, Letsky E, Nicolini U, Fisk N. Haemato-
logical indices at fetal blood sampling in monochorionic pregnancies
complicated by feto-fetal transfusion syndrome. Prenat Diagn
1998;18:941e6.
[8] Wee LY, Fisk NM. The twinetwin transfusion syndrome. Semin Neona-
tol 2002;7:187e202.
[9] Jain V, Fisk NM. The twinetwin transfusion syndrome. Clin Obstet
Gynecol 2004;47:181e202.
[10] Lewi L, Van Schoubroeck D, Gratacos E, Witters I, Timmerman D,
Deprest J. Monochorionic diamniotic twins: complications and manage-
ment options. Curr Opin Obstet Gynecol 2003;15:177e94.
[11] Meberg A, Jakobsen E, Halvorsen K. Humoral regulation of erythropoi-
esis and thrombopoiesis in appropriate and small for gestational age
infants. Acta Paediatr Scand 1982;71:769e73.
[12] Snijders RJ, Abbas A, Melby O, Ireland RM, Nicolaides KH. Fetal
plasma erythropoietin concentration in severe growth retardation. Am J
Obstet Gynecol 1993;168:615e9.
[13] Robyr R, Lewi L, Salomon LJ, Yamamoto M, Bernard JP, Deprest J,
et al. Recurrence of twinetwin transfusion syndrome (TTTS) and feto-
fetal hemorrhage: two complications of laser treatment with distinct ul-
trasound features [Abstract]. Ultrasound Obstet Gynecol 2005;26:433e4.
[14] Yamamoto M, Ville Y. Twin-to-twin transfusion syndrome: management
options and outcomes. Clin Obstet Gynecol 2005;48:973e80.
[15] Senat MV, Loizeau S, Couderc S, Bernard JP, Ville Y. The value of mid-
dle cerebral artery peak systolic velocity in the diagnosis of fetal anemia
after intrauterine death of one monochorionic twin. Am J Obstet Gynecol
2003;189:1320e4.
[16] Lopriore E, Wezel-Meijler G, Middeldrop JM, Sueters M, Vandenbus-
sche FP, Walther FJ. Incidence, orgin and character of cerbral injury in
twin-to-twin transfusion syndrome treated with fetoscopic laser surgery.
Am J Obster Gynecol 2006;194.