Embed Size (px)
Citation preview
Typed With Clean Hands
Daniel M. Brailita M.D. Central Nebraska Infectious
Disease

O When do we isolateO How do we isolate O WHY do we isolate….


Objectives O 1. Name the types of isolations defined by the CDC for
acute care O 2. Explain the "mode of transmission" criteria in
determining isolation precautionsO 3. Review and discuss signage used to identify isolation
patientsO 4. Discuss alternative care settings and the use of
isolation practices (long term care/ rehab)O 5. Discuss isolation practices for emerging problematic
organisms O 6. Discuss C- Diff isolation practices.
History of Isolation Practices in U.S.
O 1877-some patients with infectious diseases are placed in separate facilities (infectious hospitals) from non-infected patients.
O 1910- “cubicle system” and “barrier nursing” allows treatment in regular hospitals
O 1950’s-1960’s- most of the infectious disease hospitals are closing
O 2012- Only one dedicated TB Hospital in U.S.
O 1970- CDC: “Isolation Techniques for Use in Hospitals to assist general hospitals with isolation precautions “. Manual for hospitals
O Introduced seven isolation categories: Strict Isolation, Respiratory Isolation, Protective Isolation, Enteric Precautions, Wound and Skin Precautions, Discharge Precautions, and Blood Precautions. ( revised 1975)

O 1983, “CDC Guideline for Isolation Precautions in Hospitals “
O Decision-making process to isolate the infection, but not the patient, and to reduce the costs associated with unnecessary isolation precautions. Gave liberty to use disease-specific or category-specific precautions as well as ownership by Infection Control Committees.
O Strict Isolation, Contact Isolation, Respiratory Isolation, Tuberculosis (acid fast) Isolation, Enteric Precautions, Drainage/Secretion Precautions, and Blood and Body Fluid Precautions ( including AIDS)
O Police Urged to Adopt Precautions on AIDSO Reuters
Published: August 03, 1987
O Police departments should require their officers to wear gloves and take a wide range of precautions for contact with those suspected of being infected with AIDS, the Justice Department's research agency said today.
O While acknowledging that studies show a low risk of infection from such contacts, the researchers recommended that police officers should wear gloves in searching people suspected of having AIDS or in handling evidence that may be contaminated with the virus of the deadly disease.
O ''When there is likely to be contact with blood, all cuts or open wounds should be covered with clean bandages and gloves worn,'' said the agency, the National Institute of Justice.
O 1985- introduction of Universal Precautions- largely due to AIDS epidemic
O 1987- Body Substance Isolation is used at UCSD. (MOIST BODY SITES)
O 1989- new OSHA guidelines re: bloodborne pathogens exposure
O 1990- TB precautions update (negative isolation)O Need for new guidelinesO 1996 Guideline for Isolation Precautions in
Hospitals (Garner JS & The Hospital Infection Control
Practices Advisory Committee )

Modus Operandi:
O 2007 Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Healthcare Settings ( Jane D. Siegel, MD; Emily Rhinehart, RN MPH CIC; Marguerite Jackson, PhD; Linda Chiarello, RN MS; the Healthcare Infection Control Practices Advisory Committee )
O http://www.cdc.gov/ncidod/dhqp/pdf/isolation2007.pdf
Infection Control Poll :O How long do you isolate somebody with
swine flu? O How many of you isolate all patients with
previous positive MRSA cultures? O How many of you require visitors to an
isolation room to follow the SAME precautions as healthcare workers ?
O How many of you believe in MRSA nasal screening at admission?
O How long do you isolate somebody with treated Cdiff ; “formed” soft stools?
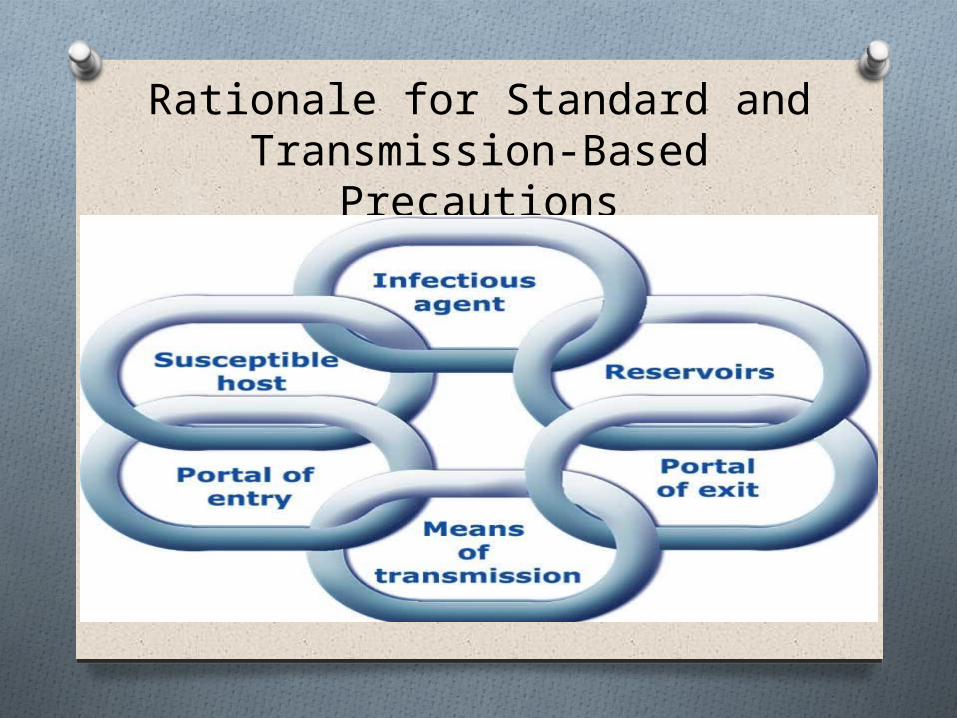
Rationale for Standard and Transmission-Based Precautions

O Source of infection: 1. Human reservoir- infected patients - asymptomatic
patients, colonized, incubating, endogenous flora
- healthcare personnel
- visitors2. Environment

O Susceptible hosts1. Altered immunity2. Normal immunity3. Chronic diseases4. Medical, surgical, oncology
procedures, disruption of skin, GI, GU, lung, mucosal barriers, foreign bodies
5. Microbiota alterations6. Age groups

Modes of Transmissiono Contact Transmission: - Direct ( ex. blood to blood)- Indirect ( ex. Thermometers)
o Droplet Transmission: - Transmission via droplet nuclei or particles
suspended in air, various diameter range, <5 to > 30 micrometer, travelling short distance to susceptible mucosal surface.
o Airborne Transmission: - Transmission via airborne nuclei or smaller
respiratory particles remaining infectious over longer distances and time, when inhaled.

QuizO What is the droplet particle
infectious range?

HICPAC Precautions to Prevent Transmission of
Infectious Agents : O STANDARD PRECAUTIONSO TRANSMISSION-BASED
PRECAUTIONS: 1. Contact Precautions2. Droplet precautions3. Airborne Precautions

STANDARD PRECAUTIONS
O A group of infection control precautions that are applicable to all patients
O Assume that any body excretions or secretions, contact with body fluids or nonintact skin and mucosa can transmit infection
O Combines previous Universal Precautions and Body Substance isolation
O Now includes Respiratory Hygiene/Cough Etiquette, use of masks for catheter insertion, safe injection practices
O Includes hand hygiene, anticipate need to use of gloves, gown, mask, eye protection, safe injection practices.
TRANSMISSION-BASED PRECAUTIONS
O Used in addition to StandardO More than one modality may be
neededO The indication re: new pathogens may
change over time
O Example: H1N1 pandemicO Newer MDRO’s ( Acinetobacter,
ESBL’s)

Infection Control Poll#2:
O What type of isolation did you use when H1N1 pandemic started?
O Why? O What do you use now? O How do you isolate Acinetobacter
Baumanii?O How about ESBL? O Why?

What Isolation Signs do You Use?



Long-Term Care Facilities
O Residents of nursing homes, homes for the elderly, institutionalized individuals with developmental and psychiatric disorders are a high-risk category for infection and colonization
O Since residents interact freely with each other, controlling transmission of infection is difficult
O Isolating residents has major implications for their life
O Psychosocial risks need to be balanced against infection risks
O There is growing evidence that a huge number of hospital infections stem from the “community”, especially long term care facilities.
O More decision power over SNU’s, LTAC’s than nursing homes/ assisted living. Use your best judgment!
Randomized Evaluation of Decolonization vs. Universal Clearance to Eliminate
Methicillin-Resistant Staphylococcus aureus in ICUs (REDUCE MRSA Trial)
SUSAN S. HUANG, MD, MPH, FIDSA
O Presented at ID week 2012O Three-arm infection prevention strategy in
ICU’s ( 43 hospitals)O Arm 1: Screening and isolation: nasal
screening+ isolation if positiveO Arm 2: Targeted decolonization: screen and
if positive, isolate, decolonize with mupirocin nasal and chlorhexidine baths
O Arm 3: Universal Decolonization: no screening, add mupirocin and chlorhexidine baths to all patients

O Universal decolonization did better than the other two strategies:37% reduction in MRSA isolates and 44% reduction is all BSI’s
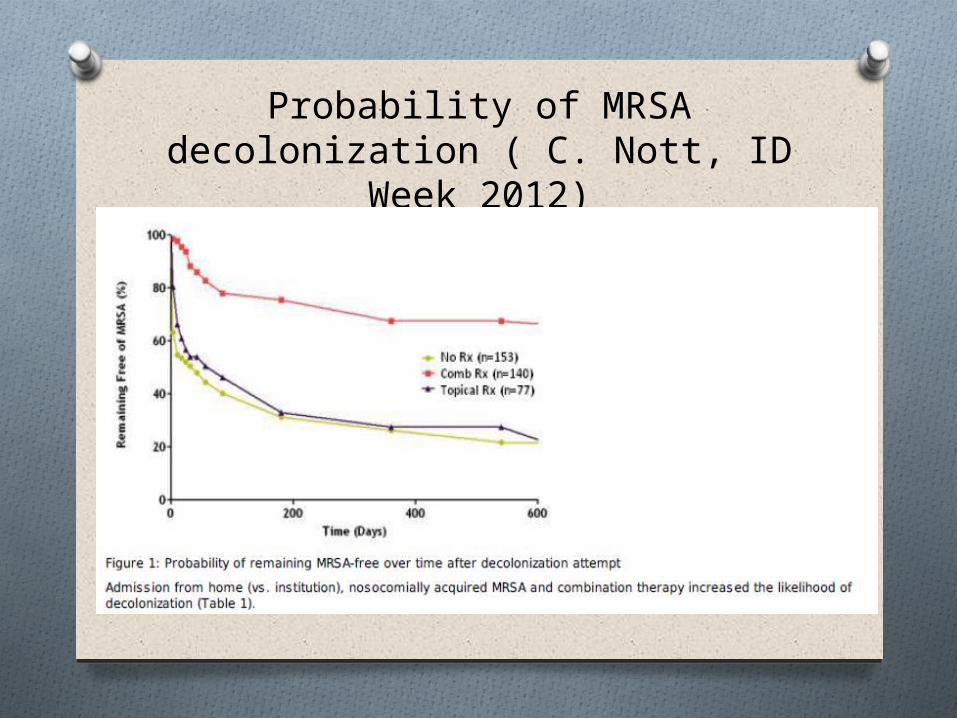
Probability of MRSA decolonization ( C. Nott, ID Week 2012)

Clostridium Difficile: New Data
O The Use of Portable Pulsed Xenon Ultraviolet Light (PPX-UV) after
Terminal Cleaning Associated with a Significant Decline in the Hospital-associated Clostridium difficile Infection (HA-CDI) rate, Colectomy and Death in a Community Hospital
JOANNE LEVIN, MD, LINDA RILEY, RN, MED, CIC, CHRISTINE PARRISH, MSN, RN, CIC and DANIEL ENGLISH, MHCIMA; Cooley
Dickinson Hospital, Northampton, MA
Previous studies were done only in big, university-type Hospitals ( MD Anderson is the most recent example) and all look promising.

O Methods:O Programs in place at baseline(prior and during implementation of PPX-
UV)O Chorine-based agents for terminal cleaning C diff roomsO Contact precautions for the duration of the hospital stay for patients with C
diffO HCW use of soap and water for hand hygiene in C diff roomsO Enhanced education of environemental service (ES) workersO Implementation of competency evaluations for ES workersO Efficient communication system for notification of discharges to ES
In 2011 (Intervention year):O 2 PPX-UV devices added to usual terminal cleaning toolsO PPX-UV used for three 7-minute exposuresO (once in bathroom, twice in main room).O Goal of using PPX-UV in every discharge roomO Also used in the operating suite, emergency department and other areas as
availableO Surveillance for HA-CDI per routineO No other new infection prevention interventions instituted during this time

Too good to be true? O HA-CDI rates per 10,000 patient days
(pd) were reduced from 9.5/ 10,000 pd for 2010 to 4.5/10,000 pd in 2011. (53%decline, p=0.0142)
O The number of colectomies and deaths attributable to HA-CDI dropped from 6 colectomies and 3 deaths in 2010 to 0 colectomies and 1 death in 2011
Clostridium Difficile Comes From the
CommunityO Antibiotic stewardship needs to be
community-centered, not only hospital-centered
O In Europe, the greatest reduction in MDRO’s was seen after implementation of restrictive antibiotic use policies ( as many countries had over-the-counter status for antibiotics)
O Big progress toward reducing the number of BSI’s but still to improve on Cdiff.

O Thank you