Embed Size (px)
Citation preview

1
USING TEAM AUDITS TO IMPROVE
IMAGE QUALITY:
Our Institution’s Experience
Lincoln L. Berland, MD
Deborah D. Flint, PE, BIE, MBA
Beth S. Winningham, BSRT, MBA
UAB Health System
900-bed Facility and Level 1 Trauma Center
Outpatient Center providing examinations and treatment
rooms for 660 physicians
219-bed facility acquired by UAB Health System in 2006

2
81 resident, fellow and faculty radiologists working in various
imaging subspecialties
Imaging Areas include:
Abdominal Imaging
Breast Imaging
Chest Imaging
Cardiopulmonary
Emergency Radiology
General Radiology
Interventional Radiology
Molecular Imaging and Therapeutics
Musculoskeletal Imaging
Neuroradiology
Pediatric Imaging
Physics & Engineering
VAMC
UAB Radiology
Background
• Radiologists believed that image quality was
sub-optimal too often
• Avoidable errors were being made
• Sub-optimal image quality could negatively
affect patient care
• Overall patient experience could be negatively
affected

3
Background
• In response, Image Quality Audit Teams were
formed
• Teams Consist of:
• Radiologists
• Technologists
• Radiology Educator
• Facilitator
Background
• This new image quality project was sponsored by:
• Radiology Vice Chair of Quality Improvement and Patient
Safety
• Radiology Vice Chair for Operations
• Administrative Director of Radiology, UAB Hospital

4
Exam Quality Audit Team Timeline
2009: CT Exam Quality Audit Team formed
(UAB Hospital and UED only)
2011: TKC and UAB Highlands CT added to CT Audit Team
2011: Diagnostic Radiograph Audit Team formed
(UAB Hospital and UED only)
2013: MRI Exam Quality Audit Team formed
(UAB Hospital, UED, TKC, and UAB Highlands)
2015: TKC Diagnostic, Highlands Diagnostic and Highlands
Orthopedic will be added to the Diagnostic Radiograph
Audit Team
• Each month team members review a set of exams randomly selected
by the team facilitator.
• Team members use a predetermined list of criteria based on the
factors that are most critical to optimal image quality. Each item is
scored with “yes” or “no.”
• Criteria include but are not limited to:
• Appropriate area scanned
• Appropriate field of view and centering
• Appropriate technical factors
• Are avoidable artifacts present
• Is the area of interest over scanned
• Appropriate contrast dose and documentation
• Appropriate contrast enhancement
• Are markers present and correct (no electronic markers used)
• Is the exam or protocol correct for the indication given on the order
Audit Process Overview

5
• Completed audits are returned to the facilitator to be summarized.
• Summarized audits are reviewed at the monthly team meetings.
• Feedback from the meetings is given back to radiology staff
through staff meetings, email, notice boards and one to one
meetings.
• The number of exams in each audit are based on a 95%
confidence interval
• The same basic protocol is used for all of the audit teams,
however, some variation in image selection and review is allowed
due to the differences in the imaging modalities being reviewed
Audit Process Overview-continued
• Each month the team reviews images selected from a
designated section.
• Auditing by section allows for more exams of each type to be
reviewed
• Physicians are able to attend the meetings related to their
specialty/section and provide feedback for improvement
• Sections for CT include:
• Neuro
• Body
• Chest
• Musculoskeletal
• Vascular Interventional
• Top opportunities for improvement are identified
• Yearly summaries are given for each section and for CT
overall
CT Exam Quality Audit

6
Example of Audit Summary: CT
97.1%
98.4%
96.3%
95.0%
95.5%
96.0%
96.5%
97.0%
97.5%
98.0%
98.5%
99.0%
Oct-13 Mar-14 Aug-14
Audit scores represent the percentage of the audit without errors
FY14 CT Exam Audit Scores--Neuro
(includes UABH, UED, UAB Highlands, TKC and Acton Road)
Audit scores for each section are reported to the
team after the audits are reviewed in the monthly
meeting. The audit summary report for CT shows
the percentage of the audit without errors.
Pareto of Audit Summary Opportunities for Improvement: CT Neuro
27%
55%
82%
91%
100% 100% 100% 100% 100% 100%
0%
20%
40%
60%
80%
100%
120%
0
1
2
3
4
1. Entire area
scanned?
2.
FOV/centering
6.
Overscanned?
4. kVp 7. Doc
contrast dose
approp?
3. mAs 5. Rem obj
causing
artifacts?
8. Contrast
enhancement
approp?
9. ROI placed
approp?
10. Threshold
approp?
Opportunities for Improvement-Neuro FY 14
YTD Cumulative %
Opportunities for improvement
are identified and tracked
7
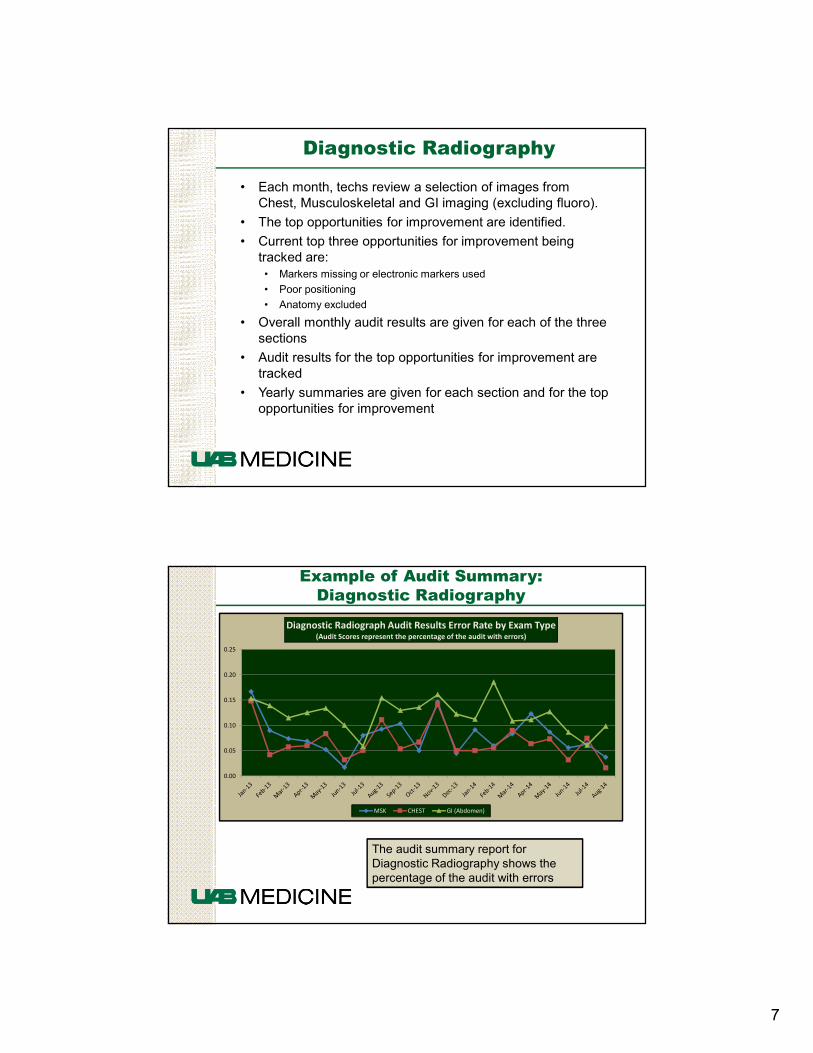
• Each month, techs review a selection of images from
Chest, Musculoskeletal and GI imaging (excluding fluoro).
• The top opportunities for improvement are identified.
• Current top three opportunities for improvement being
tracked are:
• Markers missing or electronic markers used
• Poor positioning
• Anatomy excluded
• Overall monthly audit results are given for each of the three
sections
• Audit results for the top opportunities for improvement are
tracked
• Yearly summaries are given for each section and for the top
opportunities for improvement
Diagnostic Radiography
Example of Audit Summary:
Diagnostic Radiography
0.00
0.05
0.10
0.15
0.20
0.25
Diagnostic Radiograph Audit Results Error Rate by Exam Type(Audit Scores represent the percentage of the audit with errors)
MSK CHEST GI (Abdomen)
The audit summary report for
Diagnostic Radiography shows the
percentage of the audit with errors

8
Pareto of Audit SummaryOpportunities for Improvement: Diagnostic Radiography
44%
78%
89%
100% 100% 100% 100% 100% 100% 100% 100% 100% 100%
0%
20%
40%
60%
80%
100%
120%
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
August 14 Diagnostic Radiograph Audit
MSK Chest GI (Abdomen) Cumulative %
Opportunities for improvement
are identified and tracked
Example of Audit Summary:
Diagnostic Radiography
0.0%
2.5%
5.0%
7.5%
10.0%
Pe
rce
nt
of
Au
dit
ed
Exa
ms
wit
h N
o M
ark
er
err
or
typ
e
Diagnostic Radiograph Audit
Type of Error: No Markers
MSK CHEST GI
The opportunities for improvement that are
most often seen are tracked for each exam
type. Note: Electronic markers are not
permitted and are considered “No Markers.”

9
• Each month the team reviews images from a particular
section.
• Sections for the MRI audit includes:
• Neuro
• Body
• Breast
• Musculoskeletal
• Top opportunities for improvement are identified
• Current top opportunities for improvement include:
• Patient motion
• Artifacts present
• Yearly summaries are given for each section and for MRI
overall
MRI
Example of Audit Summary: MRI
92.9% 93.8%96.2%
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
120.0%
Dec-13 Apr-14 Aug-14
(Audit scores represent the percentage of the audit without errors)
MRI Exam Quality Audit Scores -Body FY 14
Audit scores for each section are reported to
the team after the audits are reviewed in the
monthly meeting. The audit summary report for
MRI shows the percentage of the audit without
errors.

10
Pareto of Audit Summary Opportunities for Improvement: Body MRI
25%
50%
72%
86%92% 94% 97% 100% 100% 100% 100% 100% 100% 100%
0%
20%
40%
60%
80%
100%
120%
0
1
2
3
4
5
6
7
8
9
10
MRI Exam Quality Audit: Body Opportunities for Improvement
Sep-14 Cumulative %
Opportunities for improvement are
identified and tracked.
Results: CT
6.3% decrease in errors from the baseline to Present
This report represents the percentage
of the audit without errors.
90.3%
94.4%
92.8%
94.8%
96.3%
88.0%
90.0%
92.0%
94.0%
96.0%
98.0%
100.0%
**FY 10 FY 11 *FY12 FY 13 FY 14
**Baseline
CT Exam Audit Scores--All Sections
(includes UABH, UED, UAB Highlands, TKC. Acton Road)
*TKC and UAB Highlands added to the audit

11
Results: Diagnostic Radiography
Decrease in errors from baseline
MSK: 9.0%
Chest: 12.9%
GI (Abdomen): 4.8%
87%
83%
91%
96%
85% 85%
95%
98%
85%85%
89%
90%
75.0%
80.0%
85.0%
90.0%
95.0%
100.0%
Jan-12 Jan-13 Jan-14 YTD 14
Diagnostic Radiograph Audit Scores
MSK CHEST GI (Abdomen)
This report represents the percentage
of the audit without errors.
Results: MRI
0.2% decrease in errors from the baseline
94.5% 95.1%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
FY 13 FY 14
MRI Exam Quality Audit Scores- All Sections
This report represents the percentage
of the audit without errors.

12
• All areas have seen a decrease in preventable errors
• Opportunities for improvement are more easily identified
and tracked
• Improvement plans are determined jointly by the
technologists performing the exams and the radiologists
reading them
• Communication between the technologists and
radiologists is more open both in and outside of the
teams
Conclusions
• Staff members are more engaged in quality improvement
because they are active participants in the process
• Team members are publicly recognized for excellent work
identified during the audits
• Staff with outstanding recognitions are identified as
potential mentors for new staff members
• Best practices in exam performance and quality management are
taught to new staff from the beginning of employment
Conclusions-continued

13
UAB School of Medicine Department of Radiology
http://www.uab.edu/medicine/radiology/
Sources