Embed Size (px)
DESCRIPTION
Uganda’s new approach to improve testing, retention & care of HIV-exposed infants. Kiyaga Charles Ministry of Health Uganda 23 July 2010 [email protected]. Background. - PowerPoint PPT Presentation
Citation preview

Uganda’s new approach to improve testing, retention & care of HIV-exposed infantsKiyaga CharlesMinistry of Health Uganda23 July [email protected]
1

2
Background• The national EID program in Uganda has rapidly scaled up since its start in
2007, providing services at 550 sites and testing over 50,000 infants by the end of 2009.
• Despite rapid scale-up, comprehensive review of EID services in 2009 showed that infants were being lost throughout the EID process:
Infant Retention Cascade at 3 Regional Referral HospitalsSept 2007 – Feb 2009
39% of positive infants never received results
35% of positive infants receiving results were never enrolled into care 42% of positive
infants in care & treatment were lost

In response to identified challenges, MOH developed a package of 6 complementary “strengthening” interventions
3
1. Establish EID ‘Care Point’ within either MCH or ART clinic where all exposed infant care/follow-up is centralized
2.Integrate routine care into EID process & establish regular visit schedule
3. Strengthen & standardize counseling for caregivers of exposed infants
4. Improve tracking tools to centralize data & follow infants longitudinally
5. Establish referral system for DBS testing and follow-up at EID care point
6. Establish referral system for care/treatment at the ART clinic

EID “strengthening” interventions were piloted by MOH at 21 sites in 8 districts
4
Facility Level No. of sitesRRHs 3
Hospitals 7H/C IVs 9HC IIIs 2
To increase the number of HIV-exposed infants accessing PCR testing
To increased the percentage of tested infants receiving results AND eithera) Completing the infant testing algorithm (if negative), orb) Accessing care and treatment at the ART clinic (if positive)
To improve the quality of care provided to HIV-exposed infants by shifting EID services from the lab to a clinic-based program with sufficient staff & basic resources
The objectives of the strengthening pilot were;
Since the pilot, EID Strengthening interventions have been scaled up by IPs to 64 sites across 25 districts
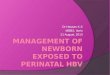
5• 4-day training including 3-5 facilities (30 trainees)
• Mix of didactic modules and practical exercises
Initial Training Workshop for Health
Workers
• Continuous mentorship visits are vital to ensure program is functioning effectively
• 4 mentorship visits per year
Mentorship Visits
•Program includes many new data tools, job aids, posters, and brochures
Provision of data tools and job aids
•Medical equipment essential for integration of care into EID
Provision of medical equipment
•At minimum, each site receives phone and airtime to regularly follow up all lost infants
Follow-up for lost infants
1
2
3
4
5
EID strengthening rollout package has 5 key components (Method)
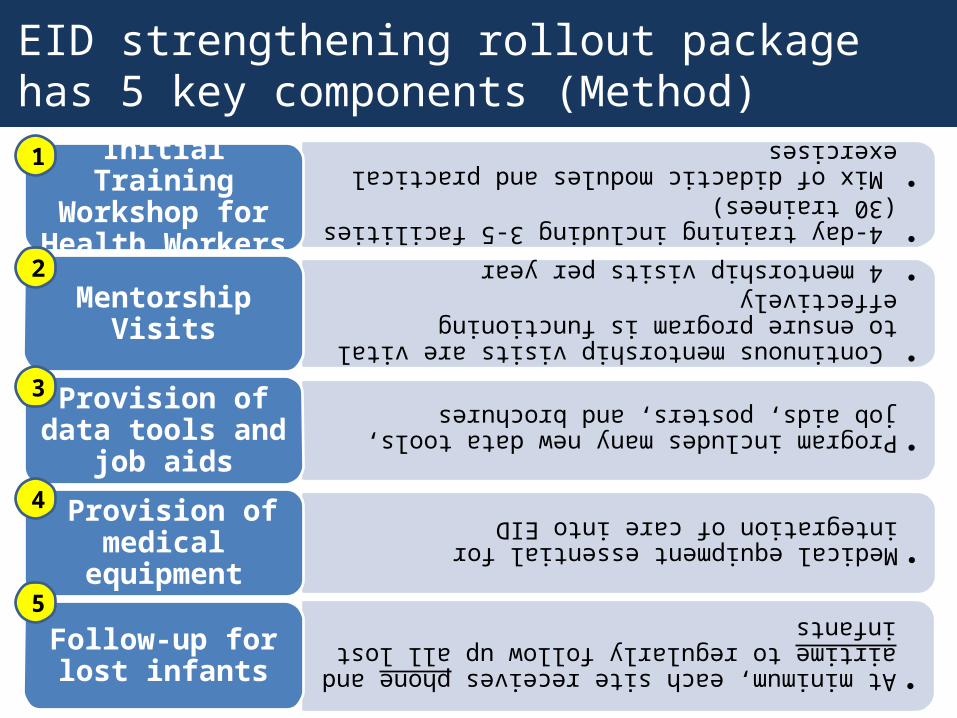
This pilot was assessed in 4 health facilities as a mini-assessment. It has demonstrated that, identification and testing of exposed infants can be extended to earlier stages in the EID process…
6
Exposed infants now being identified and referred before & at birth— likely that many wouldn’t have accessed health system again
All departments are actively referring— can be attributed to increased focus on EID and sensitization of HCWs throughout the facility
NOT actively referring before pilot

PCR testing volumes have increased by over 40% since implementation of the EID strengthening pilot
7
Number of DBS Tests4 Health Centers (Aggregate)
Sep 2009 – April 2010
Trainings
Avg Monthly Testing Volumes Pre- and Post-Training
4 health centers
Pre-Training Post-Training

Exposed infants are now being tested at a much younger age
8
Average Age at 1st PCR Test (months) Pre- and Post-Implementation
2 Health Centers
n = 31 n = 35 n = 134 n = 139

Provision of Cotrimoxazole has increased every month since implementation, and infants are clinically assessed at every visit
9
% of exposed infants initiated on CTX Post-Implementation
4 Health Centers
Care assessments now done at every visit:
Clinical assessment Growth monitoring (weight, height) Head circumference Developmental milestones
Regular and increasing levels of cotrim provision at pilot sites can be attributed to:
Creation of “EID care point” & improved clinic flow with centralization of care
HCWs trained and sensitized on the use/ important of CTX for exposed infants
HCWs required to document CTX provision on Register and Clinical Chart
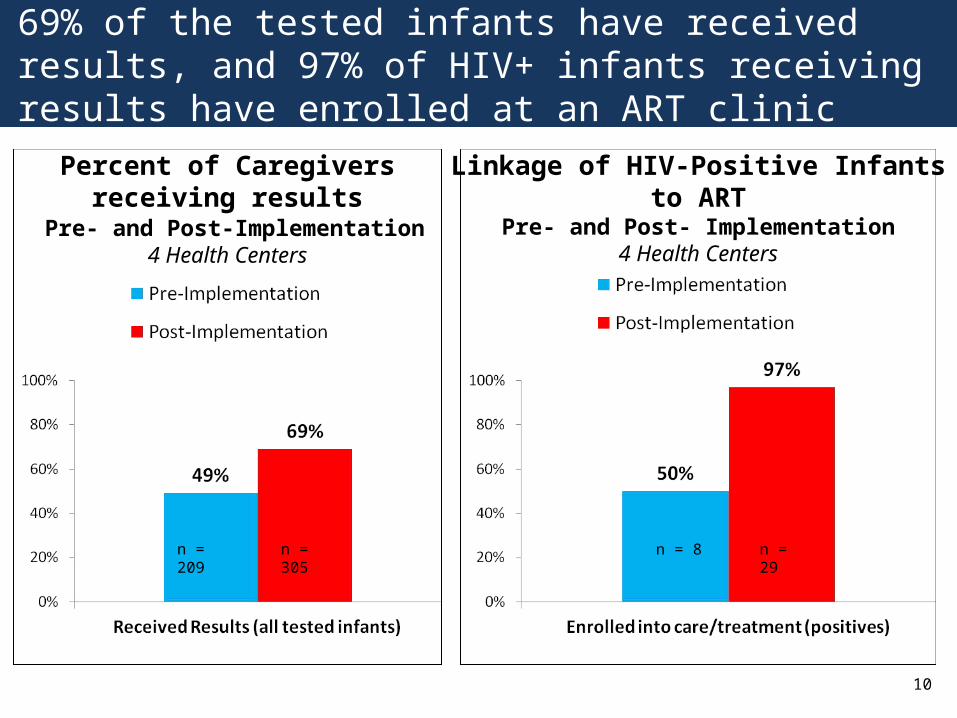
69% of the tested infants have received results, and 97% of HIV+ infants receiving results have enrolled at an ART clinic
10
Linkage of HIV-Positive Infants to ARTPre- and Post- Implementation
4 Health Centers
Percent of Caregivers receiving results Pre- and Post-Implementation
4 Health Centers
n = 8 n = 29 n = 209 n = 305
11
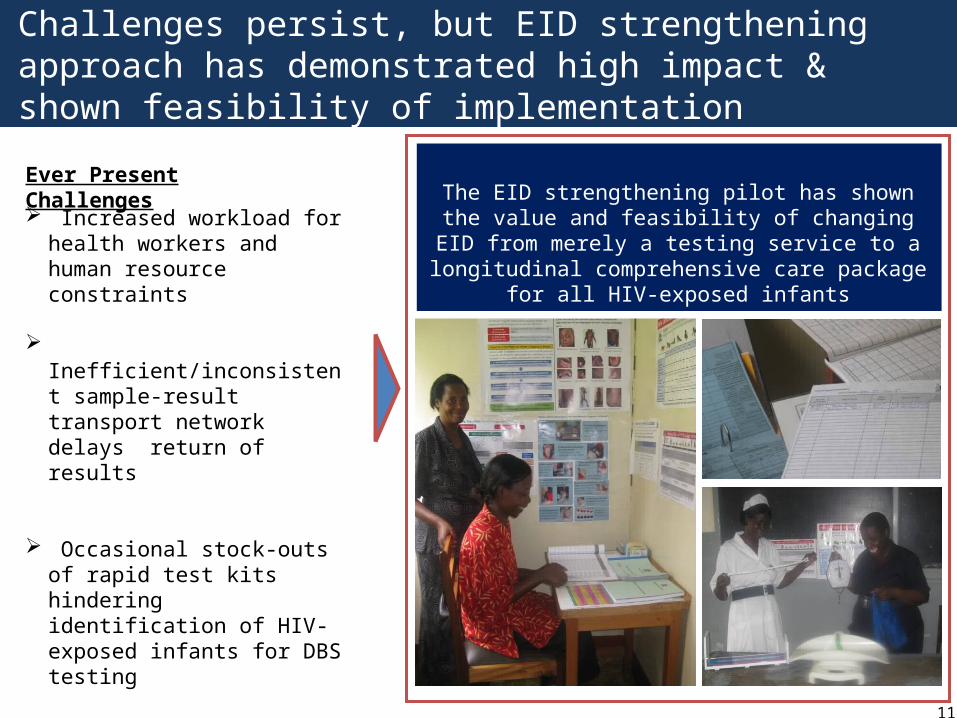
Ever Present Challenges
Increased workload for health workers and human resource constraints
Inefficient/inconsistent sample-result transport network delays return of results
Occasional stock-outs of rapid test kits hindering identification of HIV-exposed infants for DBS testing
Increased cost of Strengthening Program compared to previous implementation model
The EID strengthening pilot has shown the value and feasibility of changing EID from merely a testing
service to a longitudinal comprehensive care package for all HIV-exposed infants
Challenges persist, but EID strengthening approach has demonstrated high impact & shown feasibility of implementation

Acknowledgements
12
The Ministry of Health would like to thank two key partners for their support in making this pilot a resounding success:
2) Joint Clinical Research Centre has been an indispensible partner. JCRC analyzes and tests almost all DBS samples in Uganda, which makes provision of EID services possible.
1) The Clinton Health Access Initiative (CHAI) has supported the Ministry in the development of the strengthening approach, and provides all the supplies and reagents for EID. The Ministry is extremely grateful for the technical and logistical support by CHAI.
Co-authors: Vijay Narayan, Ian McConnell,Peter Elyanu, Cordelia Katureebe, Adeodata Kekitiinwa, Sangeeta Tripathi and Zainab Akol
13
Questions?