Embed Size (px)
Citation preview
UK NEQAS Digital Morphology:approfondimento, esperienza e valutazione dello schema
Dott. Marco Rosetti
Settore Ematologia (U.O. Corelab) Laboratorio di Area Vasta Romagna (Pievesestina) e-mail: [email protected]

Prima del 2009
Dal 2009

Personale settore ematologia:3 Medici
4 Biologi
16 Operatori Tecnici
Attività giornaliera mediaemocromi 3200 (150 vetri)Biopsie Midollari 8HPLC dell’Hb (talassemie/emoglobinopatie) 30tipizzazioni oncoematologighe (citofluorimeria) 4
Coagulazione I e II livello (reperibilità H‐24) 2000+Ves, HbA1c, G6PDH, PK, BAL, tipizzazioni HIV, EPN

IMPLEMENTAZIONE VERIFICA
Corsi e congressi
Documentazione bibliograficaVerifica del dato e della sua
corretta interpretazione
STANDARDIZZAZIONE
Istruzioni Operative
Gruppi di lavoro
External QualityAssessment Scheme
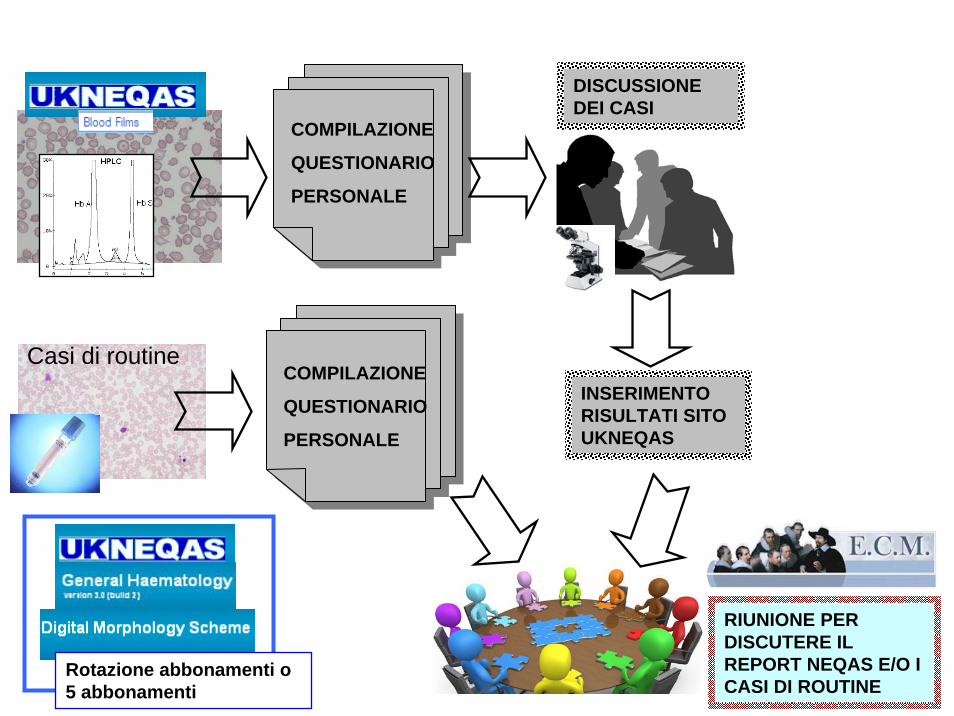
Casi di routine
COMPILAZIONE
QUESTIONARIO
PERSONALE
DISCUSSIONE DEI CASI
INSERIMENTO RISULTATI SITO UKNEQAS
RIUNIONE PER DISCUTERE IL REPORT NEQAS E/O I CASI DI ROUTINE
COMPILAZIONE
QUESTIONARIO
PERSONALE
2 abbonamentiRotazione abbonamenti o 5 abbonamenti



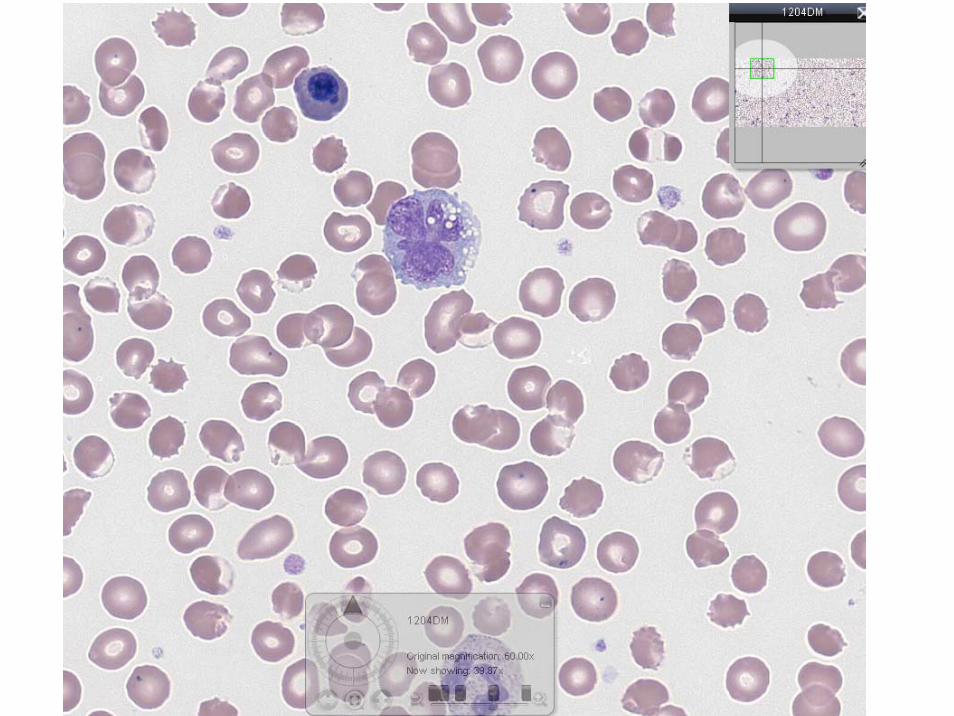





OverviewA film prepared from the blood of a 60 year old man recently commenced on treatment for a significant medical condition. The reason for treatment was not given to you but, on looking at the film, you might consider whether the underlying medical problem had a haematological cause. The patient has a raised white cell count with a reduced platelet count and is mildly anaemic. On looking at the image on low power we can see a variety of abnormal morphological features, particularly for red cells and white cells. The appearances raise the question of whether the features present support a single clinical condition, or whether these features indicate a more complex combination of causes. What can we deduce by looking at the film more closely? PlateletsThe image confirms that although platelets are present, the count is reduced and there is no evidence of clumping. We are not told which technology was used to assess the platelet count, so it is important to consider whether the presence of red cell fragments or large platelets might impact on the platelet count if an impedance counting method was employed. The platelet morphology is relatively normal with some variation in size (P1). Erythrocytes.There are various features to the red cell morphology that require attention. We were not told the MCV or RDW but when compared to a small lymphocyte there are few normal sized erythrocytes present (R1). The most prominent abnormal cells are the frequent small dense erythrocytes that have irregular shape and lack central pallor (R2, R3). These are often termed Irregularly Contracted Cells (ICC). These are not spherocytes – generally speaking spherocytes are recognised as regular round cells that lack central pallor and have a uniform density of haemoglobin – while there may be some irregularity of spherocytes it is always worth specifically asking yourself: Are the dense cells that I see spherocytic or irregularly contracted? In this case, I am sure that you will agree that the level of irregularity of both membrane shape and haemoglobin content means that these cells are ICCs (R4). It is important not to report these as spherocytes as this could lead the clinical team to consider an autoimmune condition, which would be incorrect. The erythrocytes in this image have small areas of membrane that contain no haemoglobin, resembling a surface blister – these are often called ‘blister’ cells which is an easily remembered and evocative term (R5, R6). There are some cells in which the haemoglobin is condensed at one pole of the cell – ‘hemi-ghosts’ (R7) , and note also those red cells that contain no haemoglobin and so appear as a membrane only: these are the ‘ghost cells’ (R8 R8a). Polychromasia is a feature (R9, R10) and occasional nucleated red blood cells are also present (R11) as the bone marrow responds to the red cell destruction. However, some of the newly formed red cells also show features of membrane abnormality (R12, R12a). Along side the blister and ghost cells, there are spiculated red cells (R13, R14), basophilic stippling (R15), and Howell-Jolly inclusion bodies (R16). These features are probably associated with hyposplenism – this need not imply that splenectomy has occurred, as functional hyposplenism may accompany massive red cell destruction.White cellsThe total white cell count is raised, a finding that may be associated with marrow reaction in the face of acute red cell destruction, but does require further consideration. A reactive marrow usually is characterised by neutrophilia with reactive features such as a left shift or the presence of toxic granulation. This is not entirely the case, the neutrophil count is raised and some do show vacuoles in the cytoplasm (W1), there are also apoptotic nuclei which may reflect neutrophil damage or an aged sample (W2). However, the majority of neutrophils appear morphologically to be relatively normal (W3). There is an occasional myelocyte (W1) and eosinophils are present (W4) all of which supports an element of reactive response. There is, however, an additional and substantial population of large, abnormal mononuclear cells with dark basophilic cytoplasm lacking in granules (W5). It is important to consider the morphological appearance of these cells to ascertain if they are reactive, and if so why, or if there is another clinical cause for these cells. The mononuclear cells vary in size between medium to large, they are irregular in shape compared to a normal lymphocyte (W0), but all show abnormal morphology with a lobulated or convoluted nucleus (W6, W7, W8 ,W9), with occasional nucleoli, together with a small population of smear cells (W10). Notably there is a folded arrangement to the nucleus in some cells, which creates a flower like appearance (W11, W12); this is a significant feature. The question must be asked: are these cells simply a part of the reactive process, or are they neoplastic? Summing upThere is a lot to consider in this image and many participants might rightly feel that this is one for immediate referral to the clinical lead. There are important features of morphological abnormality in both the red cell and white cell populations. The reduced platelet count also has to be considered. The question you must consider is whether the abnormal morphology of the erythrocytes and leukocytes are due to separate causes or whether they are related, and if so what is the nature of the relationship?We hope you have found this case interesting. It is a particularly difficult and rare case and we are grateful for the participating laboratory who submitted it to UK NEQAS(H). The final diagnosis will be revealed when the case closes.


The reported diagnosis of ATLL has a high potential for tumor lysis syndrome. A preventive supportive care is recommended before treatement. We hypothesize that in this contest Rasburicase could be the drug used and the causative of oxidative damage

In conclusione…
Ottima simulazione delle reali problematiche clinico-laboratoristiche
Facile utilizzo e adattabilità alle diverse realtà laboratoristiche
Aiuta la standardizzazione inter-laboratori ed intra-laboratorio
Permette ai partecipanti di condividere casi di interesse con altri partecipanti
Unisce efficacemente un valore educazionale alla verifica esterna di qualità

Dott Romolo Dorizzi (responsabile U.O. Corelab)
Dott. Poletti Giovanni (responsabile sett. Ematologia)
Dott. Baldrati Luca Dott.ssa Clementoni Alice
Dott.ssa Molino Domenica Dott. Monti Franco
Dott.ssa Zucchini Alessandra
Grazie per l’attenzione!