Embed Size (px)
Citation preview
Ulcerative colitis and Crohn’s diseaseAn overview of the diseases and their treatment
The informed patient
2nd edition 2005 (UK)
This publication is sponsored by the Falk Foundation e.V.The information herein represents the independent opinionof the author and does not necessarily reflect the opinionand recommendations of the Falk Foundation e.V.
Not all products discussed may have a licence or indicationin your country. Please consult your doctor regarding yourcountry’s specific prescribing information.
DR FALK PHARMA UK LTDBourne End Business ParkCores End RoadBourne EndBucks SL8 5AS, UK
For further information please contact
Leinenweberstr. 5Postfach 652979041 FreiburgGermany
FALK FOUNDATION e.V.
Publisher
© 2005 Falk Foundation e.V.All rights reserved.
The informed patient
J. Schölmerich, H. Herfarth,G. Rogler and A. Fürst
Ulcerative colitis and Crohn’s diseaseAn overview of the diseases and their treatment
Authors:Prof. Dr. J. SchölmerichPD Dr. H. HerfarthProf. Dr. Dr. phil. G. RoglerKlinik und Poliklinik für Innere Medizin IProf. Dr. A. FürstKlinik und Poliklinik für ChirurgieKlinikum der Universität RegensburgD-93042 RegensburgGermanyTel. xx 49 (9 41) 9 44-70 01
Associated authors of the 1st–15th editionsDr. P. Hoppe-Seyler, Helios-KlinikD-79379 MüllheimGermanyTel. xx 49 (76 31) 8 81
Prof. Dr. M. Lausen, Abt. AllgemeinchirurgieMathias-SpitalD-48431 RheineGermanyTel. xx 49 (59 71) 42 13 01
The informed patient
Contents
Foreword . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
The names: Ulcerative colitis – Crohn’s disease 7
The digestive tract . . . . . . . . . . . . . . . . . . . . . . . . 9
Symptoms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12The bowelOther organsUlcerative colitisCrohn’s disease
Methods of examination. . . . . . . . . . . . . . . . . . . . 17Physical examinationLaboratory testsUltrasoundEndoscopyGastroscopyColonoscopyProctoscopyRadiological examinationsMagnetic resonance imaging (MRI)Computed tomography (CT)Capsule endoscopyLeukocyte scintigraphyEndosonographyFollow-up studies
Causes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31Bowel diseaseAssociated conditionsComplications
3
Treatment. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35Ulcerative colitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35• Drugs• Side effects• Surgery• DietCrohn’s disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40• Drugs• Nutritional therapy• Surgery• Deficiency syndromesPsychotherapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45
Special problems . . . . . . . . . . . . . . . . . . . . . . . . . 46Course of the diseaseFistulaeOsteoporosisInflammatory bowel diseases in childhoodThe risk of cancerPsychic stressSelf help groupsDisability and careerRecreationSex and partnershipReproduction and genetic factorsPregnancy“Ostomy”: the artificial bowel outlet
What the patient should consider . . . . . . . . . . . . 56
Glossary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 58
Self help groups . . . . . . . . . . . . . . . . . . . . . . . . . . 61
4
The informed patient
Foreword
Every chronic disease represents a difficult challenge –for the patient, his family and for the physicians cooper-ating in his care. This is particularly true for diseases,the causes of which are only partially understood, andwhich are so rare that a typical family doctor may onlysee a few cases in his primary care practice. In Germany,the inflammatory bowel diseases (IBD) affect about onein every 250 to 500 persons. A person confronted withthe diagnosis “inflammatory bowel disease” usuallyreacts first with great uncertainty. Many troubling ques-tions come to mind: What does it really mean to have achronic disease? What course will it probably take?How will it affect my life? And, what effects is it likely tohave on my future? A survey of patients with IBD foundthat a majority felt that they did not possess sufficientinformation regarding their disease. While no brochurecan replace frank discussions with your physician, everyadditional source of information is useful. It may be ofparticular help in assisting the patient in converting hisuncertainties and anxiety into concrete questions thatcan then be discussed with his physician.
The present brochure is intended to be just such a sourceof information. We particularly hope to cover questionswhich, in our experience, are often posed by patients to their doctors. If, after reading this booklet, you findcertain questions unanswered, please let us know. Youropinions are important to us and will help us to improvethis brochure in future editions.
March 2003 J. Schölmerich, H. Herfarth,G. Rogler, A. Fürst
5

Seite 6 = Vakat
The informed patient
The names: Ulcerative colitis –Crohn’s disease
You or a member of your family has been confrontedwith the diagnosis “inflammatory bowel disease” or IBD.In most cases, this means either ulcerative colitis orCrohn’s disease. At first, these names seem strangeand you probably wonder what they can mean. Bothrefer to chronic inflammation of the mucosal lining of the intestine or bowel, though each has quite specificcharacteristics.
What do the names mean?
The use of different names is based on the fact that thedisease is often named according to the portion of thebowel it affects and which becomes inflamed. The charton page 11 shows the digestive tract and gives thenames of the various segments.
7
Dr. Burrill B. Crohn
The small bowel is normally 3–5 m in length, while thelarge bowel or colon is about 1.5 m long. We distin-guish between two main forms of IBD. The first is ulcer-ative colitis, an inflammation (“-itis”) affecting only thecolon and associated with the formation of ulcers. Insome cases, only the rectum is involved, and we speakof ulcerative proctitis (proctos = rectum). The secondmain type of IBD is Crohn’s disease. Named for its dis-coverer, the American gastroenterologist Burrill B.Crohn, it can affect any portion of the digestive tract,from the mouth to the anus. Depending on the exactsegments affected, we can speak of Crohn’s ileitis,ileocolitis, colitis or enteritis.
8
The informed patient
The digestive tract
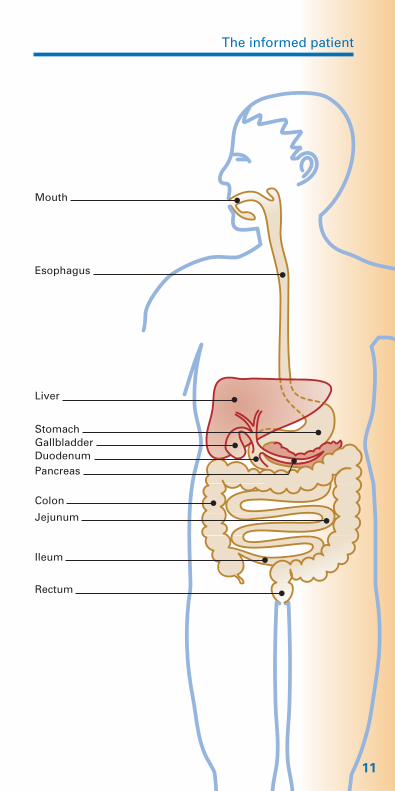
What you should know about the normal digestivetract
The digestive tract or canal begins in the mouth.Here, the food is chewed and mixed with saliva, lubri-cating and partially digesting it. Once swallowed, thefood passes into the esophagus, a muscular tube,whose walls move in wave-like patterns propelling thefood downward into the stomach. In the stomach, thefood is mixed with gastric juices, which consist of acid,mucus and various enzymes, which begin the break-down of proteins. In the duodenum, the food is furthermixed with secretions from the pancreas, which containother digestive enzymes, and with bile. Bile is producedin the liver and contains bile acids, which also help indigestion. These functions are rarely compromised inulcerative colitis, and, when they are, it is usually dueto an associated disorder of the biliary tract. They aresometimes be affected in Crohn’s disease.
The upper segment of the small bowel, also knownas the jejunum, is where fats, fat-soluble vitamins (A, D,E and K), protein breakdown products, sugars andsome trace elements are absorbed. Vitamin B12 and bileacids, however, are absorbed in the ileum, the lowerpart of the small bowel. This latter function is oftencompromised in patients with Crohn’s disease, thoughdisturbances of the upper small bowel are less frequent.The insufficient absorption and resulting loss of bileacids in the ileum, however, may adversely affect thedigestion and absorption of fats and fat-soluble vitaminsin the upper small bowel.
9
The colon’s main role is the absorption of water andminerals, which results in thickening and solidifying thestool. After advancing to the final segments of thecolon (the sigmoid colon and rectum), the stool isformed and held back by the action of the bowel outletor anus until a voluntary bowel movement occurs. Thesefunctions may be affected in both ulcerative colitis andCrohn’s disease. The result may be a tendency tounintended passage of gas or stool.
10
The human digestive tract �
The informed patient
11
Mouth
Esophagus
Liver
StomachGallbladderDuodenumPancreas
Colon
Jejunum
Ileum
Rectum
Symptoms
What are the symptoms of ulcerative colitis orCrohn’s disease?
Both ulcerative colitis and Crohn’s disease are charac-terized by an inflammation of the mucosal lining of thebowel. Thus, some symptoms are common to both dis-eases. There are, however, fundamental differences dueto the fact that the extent and location of the inflamedbowel segments differ between ulcerative colitis andCrohn’s disease.
Beside the general manifestations of disease, suchas fatigue, tiredness, loss of appetite and sometimesfever, the specific symptoms are related directly to the bowel.
These include irregular bowel movements containingmucus and/or blood and severe diarrhea; abdominalpain, sometimes focused on a certain spot, but oftenaffecting the entire abdomen, which can be crampy orpersistent. Many patients experience nausea and mayvomit. The inflammation may also result in loss of bloodthrough the bowel. This loss, which may take the formof so-called “occult”, or hidden, blood and be detectedonly with special tests, may lead to anemia. Wheneverthere is loss of blood, iron is also lost: in this case, thebone marrow lacks the iron necessary to form newblood cells. This is known as iron-deficiency anemia.
12
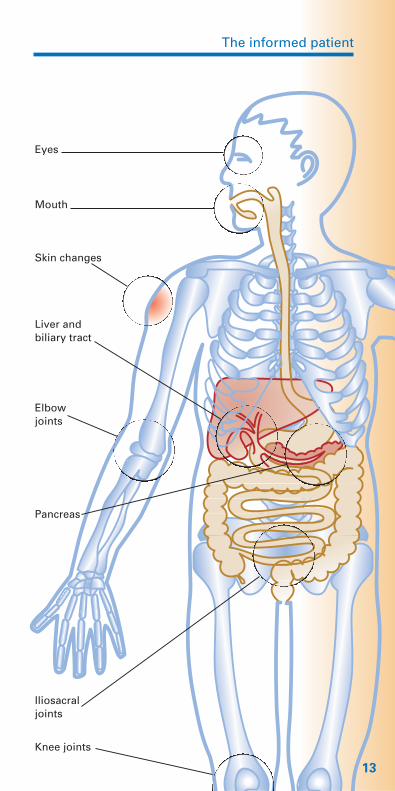
Involvement of other organs in inflammatory �bowel diseases (extraintestinal manifestations)
The informed patient
13
Eyes
Mouth
Skin changes
Liver and biliary tract
Elbowjoints
Pancreas
Iliosacral joints
Knee joints
In both ulcerative colitis and Crohn’s disease, symp-toms may occur not only in the bowel but also at dis-tant sites in the organism. Some patients experienceinflammation (arthritis) in the larger and smaller joints ofthe arms and legs, as well as in the joints of the spineand pelvis. As in other types of arthritis, this joint inflam-mation results in swelling, pain and restrictions in mo-tion. The skin in patients with IBD may also react in theform of painful purplish-red areas of thickening, mostcommonly occurring on the arms and legs (erythemanodosum).
Somewhat less frequent is inflammation affecting theeyes, particularly the iris and conjunctiva. In both,ulcerative colitis and Crohn’s disease, there may berather uncharacteristic associated inflammation of theliver. In very rare cases, the bile ducts can undergo in-flammation with extensive scar tissue formation result-ing in jaundice and digestive disturbances. Other rarecomplications include inflammation of the pericardium(the sac surrounding the heart) and pancreas, as well asvenous thromboses (blood clots).
Ulcerative colitis, which affects only the colon, is typi-cally characterized in its acute phase by diarrhea mixedwith mucus and/or blood. The severity of the diarrheadepends on the inflammatory activity and the extent ofthe inflammation. Diarrhea may be very severe in casesin which the entire colon is affected. If, however, onlythe final portions of the colon (the sigmoid or rectum)are affected, as in ulcerative proctitis, the stool may bemore solid but traces of blood can be detected.
Crohn’s disease may affect both the small bowel andcolon. In its initial phase, it may cause few or no symp-toms at all and, particularly in cases in which the colonis only partially affected or completely spared, there may
14
The informed patient
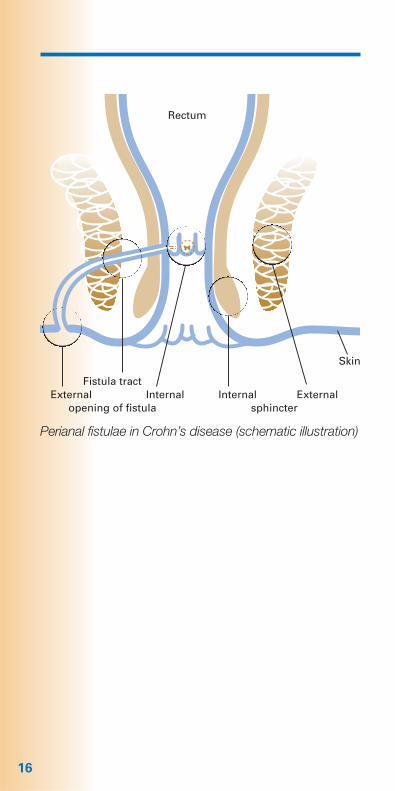
be no diarrhea. In many cases, there may be abdominalpain, which sometimes can be confused with appen-dicitis. Crohn’s disease is associated with nutritionaldeficiencies in its early stages, resulting in significantweight loss. In some patients, the disease manifestswith inflammation in the region of the anus, resultingin the formation of fistulae and abscesses. A fistula is atube-like tract lined with inflammatory cells. It mayconnect two hollow organs or open into the outer skinor the anal mucosal membrane (see illustration on page 16).
Weeping, purulent fistulae in the region of the anus, par-ticularly if they recur, should always suggest the needfor more extensive examination of the bowel. Whenevera patient reports the occurrence of several of the abovedescribed symptoms, the physician will consider thepossibility of IBD.
15
16
Rectum
Fistula tractExternal Internal Internal External
opening of fistula sphincter
Perianal fistulae in Crohn’s disease (schematic illustration)
Skin
The informed patient
Methods of examination
What will the physician do to determine the typeand extent of a patient’s disease?
He will inform you, the patient, that “diagnostic proce-dures” are now necessary, that you should undergocertain types of examinations.
As a first step, he will conduct a physical examinationof your entire body, particularly the abdomen and alsothe rectum. He will gather information by palpating theouter surface of the body, by listening with the stetho-scope and by tapping over hollow organs. This will helpdiscover whether the skin, mucous membranes, eyes orjoints show signs of disease. When examining the ab-domen, it may be possible to determine the exact siteof pain and the physician will be able to learn muchabout the condition of the liver and the activity of thebowel. In examining the anus, he will be able to recog-nize inflammation and, by gently examining the rectumwith his finger, possibly find traces of blood.
The physician will then obtain blood and urine samplesin order to perform certain laboratory tests, includingerythrocyte sedimentation rate (time required for settlingof suspended red blood cells), the number of white andred blood cells and platelets (the “blood count”), theprotein content of the blood (protein electrophoresisand C-reactive protein [CRP]) and other special labora-tory tests such as iron, electrolytes, vitamins (particularlyvitamin B12), folic acid and trace elements, such as zinc.Together, these tests help determine whether generalsigns of inflammation, absorption disorders (reduced
17
or inadequate uptake of nutrients from the bowel) orbleeding are present. The urine tests help evaluate thekidneys and urinary tract.
If the results of these tests confirm the suspicion of aninflammatory bowel disease, further examinations willbe necessary to determine the type of the individualpatient’s disease as well as its location and extent in the gastrointestinal tract.
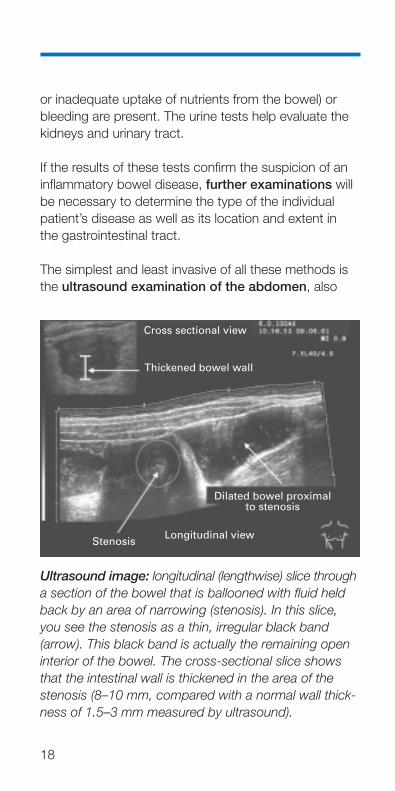
The simplest and least invasive of all these methods isthe ultrasound examination of the abdomen, also
18
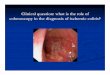
Ultrasound image: longitudinal (lengthwise) slice througha section of the bowel that is ballooned with fluid heldback by an area of narrowing (stenosis). In this slice,you see the stenosis as a thin, irregular black band (arrow). This black band is actually the remaining openinterior of the bowel. The cross-sectional slice showsthat the intestinal wall is thickened in the area of thestenosis (8–10 mm, compared with a normal wall thick-ness of 1.5–3 mm measured by ultrasound).
Dilated bowel proximal to stenosis
Cross sectional view
StenosisLongitudinal view
Thickened bowel wall
The informed patient
known as sonography. In most cases, ultrasoundsensitively uncovers changes in the abdomen, such as widening of the bowel and thickening of its wall,changes in the liver, gallbladder and kidney stones, ab-scesses and any condition hindering the outflow ofurine from the kidneys. Ultrasound is totally harmlessand can be safely repeated as often as necessary.Thus, any suspicious findings can be re-examined and monitored.
In determining the extent of the digestive tract affect-ed by any IBD, it is crucial to determine the exact site(s)of inflammation. A number of methods are available,including endoscopy, radiography and, in specialcases, scintigraphy.
Endoscopy uses an optical instrument to directly seethe inner surface of hollow organs. Entering through themouth, it is possible to examine the esophagus, stom-ach and duodenum. Entering through the anus, thephysician can check the rectum, the entire length of thecolon and usually the last few centimeters of the smallbowel, also known as the terminal ileum. The endoscopeis a flexible, tube-like instrument with a diameter of9–12 mm. These high-precision instruments contain anoptical system integrated into their tip connected to theouter end by a fiber-optic cable consisting of thousandsof fine glass fibers. This fiber-optic cable transmits lightinto the organ being examined and conveys the imageonto a television monitor. The endoscope has a sepa-rate channel through which a thin instrument can be in-troduced. This instrument, known as a biopsy forceps,can be used to obtain tissue samples for examination.
Endoscopy permits the examiner to look directly at themucous membrane of the digestive tract. Normal tissuecan usually be easily distinguished from inflamed areas.
19
In addition, tissue samples can be taken from affectedareas and examined using microscopic methods, alsoknown as histological examination. This direct examina-tion under the microscope of samples of mucous mem-brane permits determination of whether inflammation ispresent, how severe it is, and what type of inflammationit is. Thus, it can establish the diagnosis of IBD and usu-ally (≥ 90%) can differentiate between ulcerative colitisand Crohn’s disease.
Endoscopic examination of the stomach is also knownas gastroscopy. For gastroscopy, the optical instru-ment is introduced through the mouth and advancedthrough the esophagus into the stomach and duode-num. This examination must be done in a fasting statein order that the food content of the stomach will notinterfere with inspection of the mucous membrane. Theexamination is painless; however, it is associated withunpleasant sensations of pressure in the neck during in-troduction of the instrument and in the upper abdomen.This discomfort can be significantly reduced by the ad-ministration of appropriate medication.
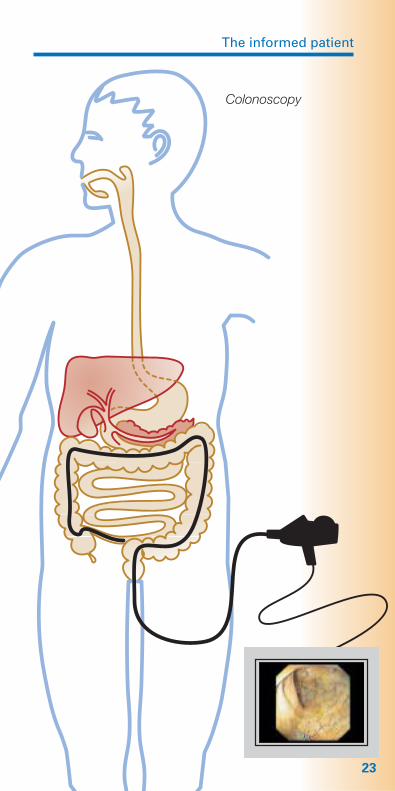
In colonoscopy, which involves endoscopic examina-tion of the bowel, the endoscope is introduced throughthe anus and advanced up the entire length of the colonto the entrance of the small bowel. Once the junctionbetween the small bowel and colon (the ileocecal valve)is passed, the terminal portion of the small bowel canalso be examined. Colonoscopy requires more intensivepreparation. Patients are not permitted to consume anysolid food for 24 hours prior to the examination. On theday before the examination, the patient may eat break-fast but for lunch, only clear broth is allowed. In theafternoon, the patient must also consume a suitable
20
The informed patient
21
Gastroscopy
irrigating solution (four liters) in order to cleanse thebowel. Various solutions are available with differenttastes. After this, only mineral water or tea is allowed.
Colonoscopy may be painful, particularly when there are inflammation-related adhesions in the abdomen.Patients may be given injections that help relax themand relieve pain, making the examination tolerable.
Proctoscopy is the simplest and least invasive endo-scopic method. It involves examination of the distalrectum and covers the last 5–10 cm above the anus.More convenient is sigmoidoscopy. After a small enemais given to cleanse the rectum, a short, flexible tube isinserted through the anus. It is also possible to obtainspecimens of tissue for biopsy using these methods. In patients with inflammation in the rectum, proctoscopyand sigmoidoscopy are the best methods for monitoringthe progress of the disease and treatment, since it canbe carried out without complicated preparations and iseasily repeated.
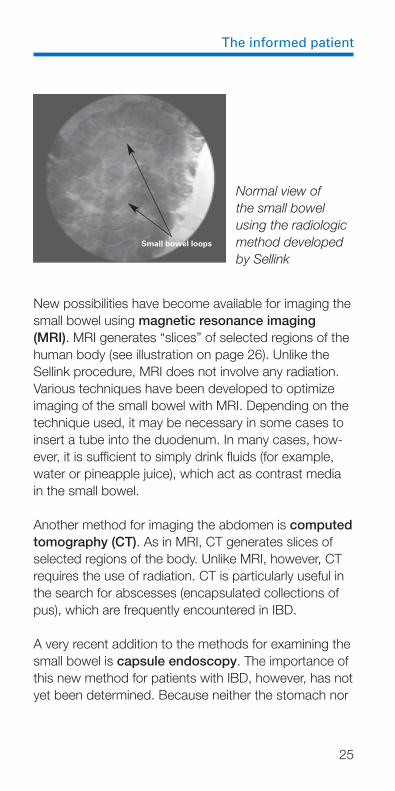
Radiological examinations represent another optionfor examining the digestive tract. One method makesuse of a solution (contrast medium) that is not penetrat-ed by x-rays to show the contours of the esophagus,stomach, small bowel or colon. In cases of IBD, exami-nation of the small bowel is particularly important. Insuch cases, the small bowel can be examined using aspecial method developed by and named for the radiol-ogist Sellink. In this method, a tube is passed throughthe stomach into the duodenum (see illustration onpage 25). This permits direct application of a dilutedcontrast medium in the small bowel. The segments ofthe small bowel between the duodenum and colon,which are not accessible to endoscopy, can be exam-ined using this method.
22
The informed patient
23
Colonoscopy
24
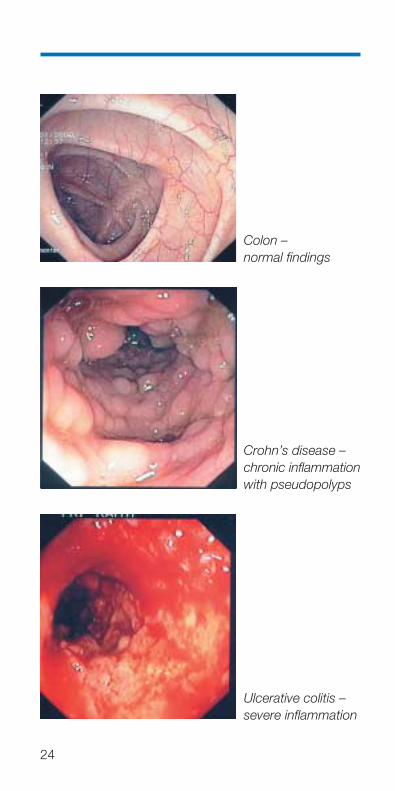
Colon – normal findings
Crohn’s disease –chronic inflammationwith pseudopolyps
Ulcerative colitis –severe inflammation
The informed patient
New possibilities have become available for imaging thesmall bowel using magnetic resonance imaging(MRI). MRI generates “slices” of selected regions of thehuman body (see illustration on page 26). Unlike theSellink procedure, MRI does not involve any radiation.Various techniques have been developed to optimizeimaging of the small bowel with MRI. Depending on thetechnique used, it may be necessary in some cases toinsert a tube into the duodenum. In many cases, how-ever, it is sufficient to simply drink fluids (for example,water or pineapple juice), which act as contrast mediain the small bowel.
Another method for imaging the abdomen is computedtomography (CT). As in MRI, CT generates slices ofselected regions of the body. Unlike MRI, however, CTrequires the use of radiation. CT is particularly useful inthe search for abscesses (encapsulated collections ofpus), which are frequently encountered in IBD.
A very recent addition to the methods for examining thesmall bowel is capsule endoscopy. The importance ofthis new method for patients with IBD, however, has notyet been determined. Because neither the stomach nor
25
Normal view of the small bowel using the radiologicmethod developedby Sellink
Small bowel loops
26
colon can be adequately studied with this method,however, it should not be considered an alternative foreither gastroscopy or colonoscopy.
Less frequently used is leukocyte scintigraphy. In thismethod, the white blood cells (leukocytes) are isolatedfrom a sample of the patient’s blood and marked with aradioactive substance. These marked leukocytes arethen returned to the patient’s blood stream. A specialrecording device is then used to document the localaccumulation of leukocytes in areas of inflammation inthe bowel or elsewhere in the body. This method doesnot require any special preparation for the patient and is not associated with any subjective stress. Because
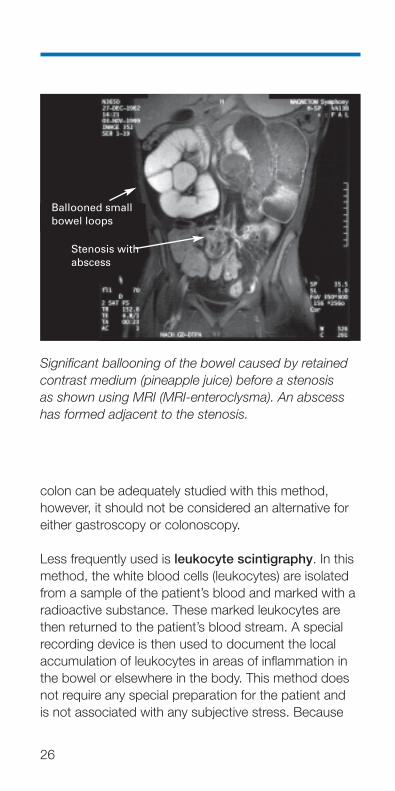
Ballooned smallbowel loops
Stenosis with abscess
Significant ballooning of the bowel caused by retainedcontrast medium (pineapple juice) before a stenosis as shown using MRI (MRI-enteroclysma). An abscesshas formed adjacent to the stenosis.
The informed patient
27
of the radiation exposure, however, and because themethod does not distinguish between the various typesof IBD but simply shows the extent of inflammation,leukocyte scintigraphy is used only in certain situations,such as stenosis (narrowing) of the bowel.
You may now be asking yourself whether all of theseexaminations must be performed. You can relax. Themore extensive array of methods is normally requiredonly to confirm the initial diagnosis of a disease and todetermine its extent and severity.
The choice of method depends on individual factors,particularly the patient’s current physical condition.Endoscopy and radiological methods can be used tocomplement each other. Usually, endoscopy is used toexamine the more easily accessible segments of thedigestive tract, since radiation exposure is avoided andit is normally possible to obtain tissue samples (biopsy)from suspicious areas for microscopic evaluation. Inorder to properly evaluate the small bowel, as well as incases in which the presence of fistulae or severe nar-rowing (stenosis) in the colon are suspected, it will notbe possible to avoid radiologic examinations. The exactanalysis of fistulae and/or abscesses can often be doneusing a special ultrasound examination of the rectum(endosonography) or with MRI.
In endosonography, an ultrasound transducer head isintroduced through the rectum as in proctoscopy or sig-moidoscopy. This permits ultrasound examination ofunderlying tissue and determination of possible fistulaformation.
28
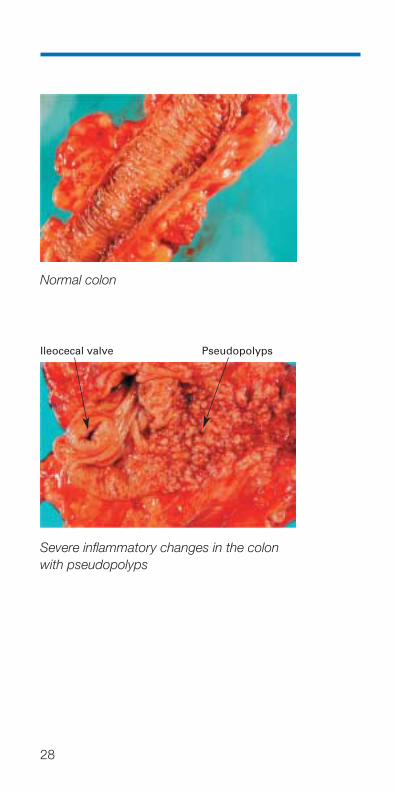
Normal colon
Severe inflammatory changes in the colonwith pseudopolyps
Ileocecal valve Pseudopolyps
The informed patient
How does the physician monitor the course ofinflammatory bowel diseases?
It is important for you, the patient, to understand that,while both ulcerative colitis and Crohn’s disease arechronic diseases of the bowel that can become andremain inactive, careful medical attention is crucial formonitoring and control of your disease. This means reg-ular visits to the physician: at least twice a year is rec-ommended, even when you are free of symptoms. If,however, drugs are required to control your disease,follow-up examinations should be done at least everythree months. Beside a physical examination includingpalpation of the abdomen and examination of thebowel, patients undergo blood tests that help identifysigns of inflammation or of nutritional deficiencies. Atleast once a year, the physician will order an ultrasoundexamination of the abdomen. If there is no evidence ofinflammation, the more complex examination methodscan usually be avoided.
During an acute disease episode or flare-up, patientsdo not necessarily have to re-undergo the entire batteryof tests. In those cases in which symptoms are signifi-cantly different than in earlier disease phases, however,it may be helpful to re-assess the extent of the disease,since changes may occur, possibly necessitating amodification in treatment strategy. In ulcerative colitis,this is particularly important in cases in which the initialextent of the disease did not involve the entire colon. InCrohn’s disease, significant changes in symptomsusually necessitates re-examining both the small boweland colon in order to exclude the presence of fistulae,stenoses or other complications. If, however, there areno changes and the disease remains inactive, these in-vasive methods are not necessary. Patients who havesuffered from ulcerative colitis for a long period of time
29

(more than 10 years), however, should undergo regularcolonoscopy (once a year is recommended) in order toexclude the development of malignant tumors in thebowel. This is particularly important in extensive colitis.
30
The informed patient
Causes
What causes inflammatory bowel diseases?
Despite numerous studies, the actual cause of the in-flammatory bowel diseases remains elusive. It is likely,however, that these chronically recurring episodes ofinflammation in the human bowel are related to a com-plex interaction between various environmental factorsand a hereditary predisposition for these diseases. In recent years, research has identified various sites(chromosomes) within the human genome that may beassociated with these diseases. In 2001, scientists dis-covered that changes in the NOD2/CARD15 gene areassociated with a significantly increased risk of develop-ing Crohn’s disease. Such changes appear to be atleast partially responsible in about 20% of all Crohn’spatients for the occurrence of this disease. On the otherhand, it is clear that this hereditary predisposition alonecannot lead to the outbreak of disease: this requires thepresence of further, as yet unidentified factors. Changesin the NOD2/CARD15 gene are found in about 4% ofindividuals, who do not develop this disease. This meansthat genetic predisposition requires the action of other,still unknown factors in order for an affected individualto actually develop the disease. These factors may in-clude viruses or bacteria, changes in nutritional behavioror the consumption of certain preservatives or otherfood additives, as well as disturbances of the body’sown immune defense system. To date, no definitive evi-dence has been found to prove a connection betweenthese factors and the development of inflammatorybowel disease. It is, however, very probable that envi-ronmental factors play a role. Crohn’s disease, for ex-ample, is much more common in Western industrialnations than in other regions of the world. On the other
31
32
hand, it is very unlikely that IBD is due to an underlyinginfectious disease – hence, infecting other persons withthe disease is not possible.
The role of psychological factors remains controversial.While psychic stress may, under certain circumstances,provoke an acute flare-up of an existing disease, it isnot the underlying cause of inflammatory bowel disease.
We also do not know the exact reason why many pa-tients with IBD also suffer from inflammatory changesin other organs, such as the joints, skin or eyes. Oneexplanation is an overreaction on the part of the body’simmune defenses to either invading microbes or eventhe body’s own tissues. This, however, has not yet beenproven.
On the other hand, the causes of many other compli-cations of these bowel diseases are known. For exam-ple, the reduced absorption of vitamins and some traceelements (minerals) in patients with IBD is responsiblefor symptoms such as night blindness, deafness, changesin taste sensation, vulnerability to infection, hair loss,infertility (in men), growth retardation (in children) andcertain skin changes frequently seen in these patients.Anemia may be caused by iron deficiency, by loss of
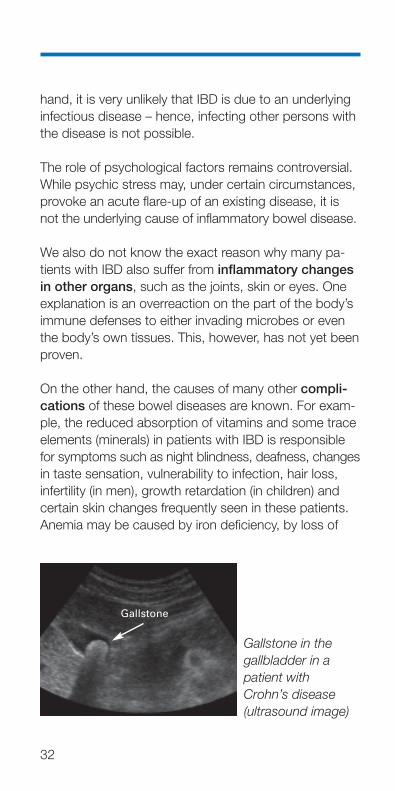
Gallstone in the gallbladder in a patient with Crohn’s disease (ultrasound image)
Gallstone
The informed patient
33
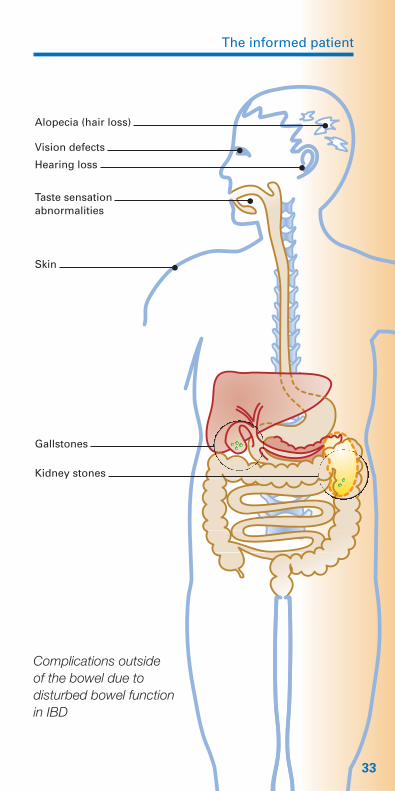
Complications outside of the bowel due to disturbed bowel function in IBD
Alopecia (hair loss)
Vision defects
Hearing loss
Taste sensation abnormalities
Skin
Gallstones
Kidney stones
blood from the bowel or by vitamin B12 malabsorption.A reduced uptake of bile acids in the small bowel andan increased absorption of bilirubin in the colon is re-sponsible for the increased risk of gallbladder stones,while kidney stones may result from the increased lossof water.
In both main types of IBD, serious complications suchas acute ballooning of the bowel (“toxic megacolon”) orperforation, the formation of a hole in the wall of thebowel, may occur in a few patients. Peritonitis, the in-flammation of the membranous lining of the abdomen,and intestinal obstruction or paralysis (ileus) may result.These are life-threatening conditions requiring immedi-ate hospital admission and often emergency surgery.Extensive intestinal hemorrhage occurs most often inpatients with ulcerative colitis. Stenoses caused by in-flammation or scar tissue formation and fistulae be-tween the bowel loops and other organs are direct con-sequences of Crohn’s disease.
34
The informed patient
Treatment
As the name “chronic inflammatory bowel diseases”implies, both ulcerative colitis and Crohn’s disease arechronic disorders. This means that the patient will con-tinue to have them for the rest of his or her life. The pro-gression of the disease, however, can differ significantlyfrom patient to patient. While some individuals experi-ence very mild disease with infrequent flare-ups, otherswill suffer from much more severe disease with frequenthospitalizations. It is, unfortunately, impossible to predictat the outset the comparative severity of an individualpatient’s future clinical course. Large studies, however,have shown that more than half of all patients with ul-cerative colitis or Crohn’s disease do not require evenone course of treatment with cortisone preparations.
What treatment methods are available?
Treatment options fall into four main groups and includedrugs, surgery, diet and supportive measures. One veryimportant supportive measure is for the patient affectedwith Crohn’s disease to quit smoking. Compared tosmokers, patients who quit smoking have a 60% lowerchance of experience disease recurrence within a two-year period.
Treatment of ulcerative colitis
The primary goal of treatment is to improve patients’symptoms (diarrhea, pain, blood loss) and, once this issuccessful, to prevent recurrence.
The usual first step is the use of drugs. The choice oftherapy depends on the severity of patients’ symptoms.
35
36
In cases with mild to moderately severe inflammation,5-aminosalicylic acid is often prescribed. In patients inwhom the joints are also affected, sulfasalazine can be tried. This drug, discovered in 1942 by the Swedishphysician Nanna Svartz, was the standard treatment forulcerative colitis prior to the introduction of 5-aminosali-cylic acid.
5-aminosalicylic acid, also known as mesalazine, is aspecially manufactured agent designed to be releasedin the lower third of the small bowel and in the uppertwo-thirds of the colon. In those cases in which ulcera-tive colitis affects only the rectum or left side of thecolon (up to 80% of patients), the disease may respondto suppositories, enemas or rectal foams that containeither 5-aminosalicylic acid or cortisone preparations.Enemas containing the locally acting cortisone deriva-tive budesonide are also effective and are associatedwith a significantly lower occurrence of side effects inthe body. In severe cases, the administration of corti-sone preparations either as pills or injections is usuallyeffective.
Dr. Nanna Svartz
The informed patient
If cortisone in the form of tablets or enemas does notlead to an improvement in a patient’s symptoms, thephysician may recommend medications that reduce thebody’s immune reactions. These drugs are frequentlyeffective because, as we noted above, chronic inflam-matory bowel diseases represent a disorder in whichthe body’s immune system has been misdirectedagainst its own tissues.
If this type of treatment is selected, the first drugs triedare usually azathioprine or 6-mercaptopurine. Theirmaximum effect, however, becomes apparent only after10–12 weeks of therapy. Unfortunately, not all patientsrespond to these drugs and about 10 in 100 patientsexperience significant side effects, including acute he-patitis, acute pancreatitis or a disorder of blood cell for-mation. Hence, patients must undergo regular (weekly,then biweekly) laboratory tests of liver and pancreaticfunction and complete blood counts. If these testsremain normal for three months, the test frequency canbe reduced to every 2–3 months.
If azathioprine or 6-mercaptopurine successfully preventdisease recurrence, they should be taken for at leastfour years. Within this time period, patients must prac-tice a secure form of contraception.
If an ulcerative colitis flare is very severe and cortisonetherapy does not result in any improvement, patientsshould be hospitalized. In such cases, cyclosporine canbe administered intravenously for 24 hours. Cyclosporinewas originally developed for use in patients with kidneytransplants to suppress the body’s rejection of thetransplanted organ.
If cyclosporine proves ineffective, the last option is thesurgical removal of the colon (colectomy).
37
Patients in whom therapy results in resolution of inflam-mation are usually started on 5-aminosalicylic acid inorder to maintain their status of disease remission.
The choice between the various preparations and themethod of administration depends on the extent andactivity of the disease. This fact explains the importanceof a complete examination before treatment and incases in which the pattern of symptoms has changed.
In determining the best treatment strategy, the physicianwill take into consideration the severity of the flare-upand the extent of inflammation. In any case, the drugsmust be taken long-term, that is, even after symptomshave resolved. Long-term administration of 5-aminosali-cylic acid preparations has been shown to effectivelyprevent a new flare-up of the disease. As with all med-ications, undesired side effects may occur. These in-clude headache, stomach complaints, nausea, anemiaand hair loss. These side effects, however, are rare and resolve once administration of the drug has beenstopped. The detailed description of these side effectson the package insert should not cause you to stoptaking the drug out of fear. Instead, you should alwaysconsult your physician who will use appropriate methodsto determine whether, in your case, the administrationof the drug should be stopped or the dosage changed.Complications are more frequently due to patients’discontinuing their medication without consulting theirphysician than to side effects of the drug themselves.This is also true for patients who are, for the moment,free of complaints.
Recent studies have shown that disease recurrence inulcerative colitis can be effectively blocked by the ad-ministration of so-called probiotics. Probiotics influencethe bowel’s bacterial flora and include such agents as
38
The informed patient
Escherichia coli Nissle and various lactobacilli. Theyappear to be as effective as 5-aminosalicylic acid. Thismethod is particularly attractive in patients who do nottolerate 5-aminosalicylic acid. The efficacy of thismethod, however, has not been substantiated in thetreatment of Crohn’s disease or of the acute diseasephase of ulcerative colitis.
Because of the success associated with drug treat-ment, surgery is rarely necessary. Life-threatening com-plications (see page 34), severe complaints persistingdespite adequate drug treatment and serious drug-in-duced side effects are indications for surgery.
The surgical removal of the entire colon cures ulcera-tive colitis. In many cases, it may be possible to removethe colon without the need for a permanent “ostomy” orartificial bowel outlet in the abdominal wall. This usuallyinvolves surgical creation of a “pouch” out of loops ofsmall bowel that acts as a reservoir and substitute forthe rectum (see page 41). In most cases, this results inalmost normal stool consistency and a bowel move-ment frequency of about five to eight times per day.
Patients with ulcerative colitis do not require a specialdiet. It is advisable, however, to avoid foods such ascabbage, onions or high-fat items that may cause com-plaints even in healthy persons. In our experience, it isusually best for each patient to test his or her own indi-vidual tolerance to different foods. Nutritional deficien-cies occur very rarely in patients with ulcerative colitis.These may manifest themselves as edema (swelling dueto accumulation of water in various tissues caused byprotein deficiency) or anemia (due to blood loss or irondeficiency) occurring most often in instances of pro-longed disease flare-ups. They respond to substitutionof the appropriate substances.
39
Disease manifestations outside of the bowel (joints,skin, eyes) can also be successfully treated with med-ication, usually with preparations containing cortisone.Surgical or dietary measures are usually less effective.Changes occurring in the biliary tract are often treatedwith ursodeoxycholic acid (UDCA), a bile acid. UDCAdoes not “cure” these conditions but may significantlyslow their progression. Every case of abnormal “liverenzymes” requires careful study and appropriate treat-ment.
The treatment of Crohn’s disease
The treatment of Crohn’s disease is based on the sameprinciples as that of ulcerative colitis. Because of themore divergent pattern of disease, symptoms and com-plications, however, it is more challenging to establishthe optimum treatment for each individual patient.
Acute flare-ups are usually treated with cortisone prepa-rations. Recently, preparations containing budesonidehave been introduced for the treatment of Crohn’s dis-ease. Their efficacy is similar to that of cortisone and its derivatives. Because their effects are limited to thebowel and the overwhelming proportion of the drug isde-activated in the liver prior to reaching the general cir-culation, these agents are associated with a significantlylower rate of side effects. Crohn’s disease can also betackled with dietary measures. Patients can convert
40
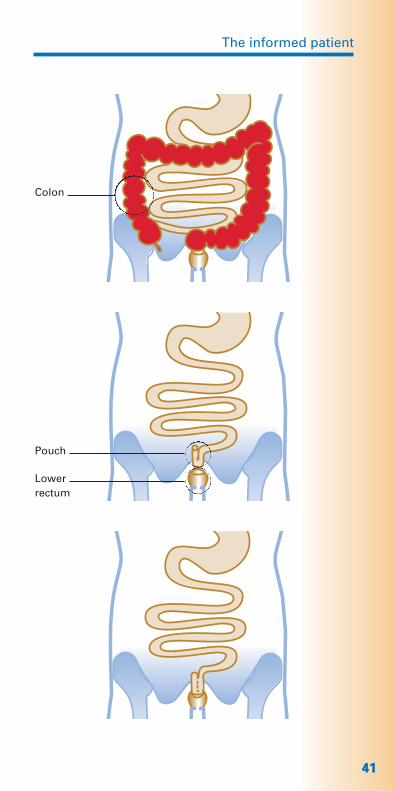
In the pouch operation, the whole colon is removed �with the exception of a small section of the lower rectum. A pouch is then created out of a part of
the small bowel (terminal ileum) and sutured to the remaining portion of the rectum.
The informed patient
4141
Colon
Pouch
Lower rectum
their dietary intake to the so-called “astronaut diet”,consisting of substances wholly digested and absorbedin the upper gastrointestinal tract. Nourishment can alsobe administered through infusions of nutrient solutionsdirectly into the blood stream. Dietary measures areusually associated with lower chances of success. Incases in which the inflammation is restricted to thesmall bowel, cortisone preparations are normally usedfirst. If patients do not respond to either of these drugs,intestinal antibiotics (metronidazole) or drugs that sup-press the immune system (for example, azathioprine)may be added. All of these drugs may be associatedwith side effects, such as itching sensations in the armsand legs, hair loss, anemia, increased risk of colds andthe like. Should these or other side effects occur, it isimportant to consult your physician, who will advise youon the proper course of action. In any case, you shouldnot stop taking your medication or change its dosewithout asking your doctor. In most cases, these drugssuccessfully treat acute flare-ups of Crohn’s disease.The same is true for manifestations of the diseaseoccurring outside of the digestive tract. The use of 5-aminosalicylic acid preparations has been shown toreduce the recurrence of the disease after surgery,though this effect is unfortunately less pronouncedfollowing successful treatment with cortisone. Newertreatment methods, such as inhibition of tumornecrosis factor (TNF), a messenger substance in thebody, should only be tried if the above described drugshave proven unsuccessful.
If these methods prove unsuccessful, or if complicationssuch as intestinal obstruction or repeated stenoses occur,surgery may provide long-term relief. When surgery isrecommended, emphasis is placed on techniques thatpreserve as much bowel as possible. Short areas ofnarrowing (stenoses or strictures) can be relieved using
42
The informed patient
43
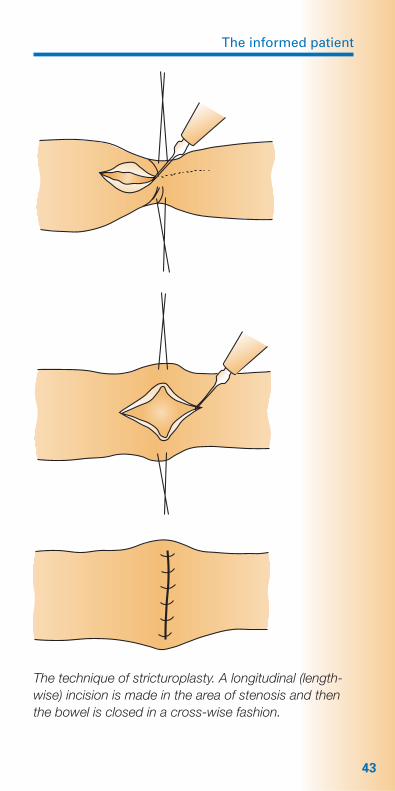
The technique of stricturoplasty. A longitudinal (length-wise) incision is made in the area of stenosis and thenthe bowel is closed in a cross-wise fashion.
a technique called stricturoplasty (see figure on page43). This involves placing a longitudinal (lengthwise)incision into the area of stenosis and then closing thebowel in a cross-wise fashion. This relieves the narrow-ing and normal passage of stool is again possible. Themain advantage of this method is that no bowel mustbe sacrificed. Stricturoplasty can be performed on sev-eral segments of stenosed bowel during a single opera-tion. Surgery must also be considered for the treatmentof fistulae. Abscesses are usually treated today by meansof a drainage placed through the skin under ultrasoundor computed tomographic guidance. Surgery, however,is usually required after the acute symptoms have sub-sided to treat the underlying cause, which may be afistula or stenosis of the bowel. Following successfulsurgery, it is advisable to undergo regular follow-up con-ducted by experienced internists and surgeons workingtogether. This permits early recognition and treatment ofany complications that may arise.
Unlike ulcerative colitis, Crohn’s disease is associat-ed with a number of different nutritional deficiencies,including vitamins, trace elements, minerals and protein.This requires appropriate substitution (vitamins, calcium,iron, potassium, zinc). Your doctor will use regular bloodtests to identify the exact nutrients that require substitu-tion. One very common deficiency is that of vitamin B12,where absorption from the bowel is often reduced inCrohn’s disease. In order to prevent a deficiency ofvitamin B12 and the resulting anemia, the life-long ad-ministration of the vitamin by injection every threemonths may often be necessary.
44
The informed patient
As in ulcerative colitis, patients with Crohn’s diseasemust determine for themselves which foods they toler-ate and which foods cause them problems. A balanceddiet providing the necessary nutrients, vitamins andminerals should be the goal.
To date, no special diet or nutritional form has beenproven to either accelerate treatment or prevent recur-rence.
Psychotherapy
Different researchers have expressed different opinionson the need for and expected success of psychothera-peutic treatment. On the one hand, it is certain thatinflammatory bowel diseases cannot be cured by psy-chotherapy. Whether such therapy can help prevent aflare-up in patients with psychic stress is not known. It is probable, however, that a behavioral therapy thathelps patients better cope with the problems of theirdisease and of daily life could be useful. In any case,such a treatment should only be conducted in coopera-tion with your physician.
45
Special problems
What kinds of special problems may occur?
Now that we have discussed the issues of the develop-ment, diagnosis, treatment and follow-up in cases of in-flammatory bowel disease, we will turn to a few specialproblems that must be confronted by patients living withthese diseases.
Course of the disease
Probably the most important question you will wish todiscuss with your physician deals with the future courseof your disease: how will it progress and what problemswill confront you in the future? When discussing yourprognosis (that is, the probable future course of yourdisease), your physician will explain that, in individualcases of inflammatory bowel disease, reliable predic-tions are often possible only after fairly extensive periodsof observation. We know today that patients’ life ex-pectancies are not reduced in either ulcerative colitis orCrohn’s disease, provided they are correctly diagnosedand appropriately treated. Ulcerative colitis and Crohn’sdisease are chronic diseases that will affect your life foryears to come. Both diseases tend toward an episodicpattern of activity, alternating between symptom-freeand active disease states. Early diagnosis and appropri-ate treatment can usually suppress the inflammatory ac-tivity and lead to re-establishment of an inactive diseasephase. Complications are more likely in patients in whomthe inflammation has become chronic and has led to pro-gressing changes in the bowel. The most effective wayof reducing the risk of complications is regular follow-up by your physician who can recognize inflammatory
46
The informed patient
flare-ups early and institute appropriate treatment.Flare-ups and associated complications can severelyreduce your quality of life and overall happiness. Thus,minor side effects of special drug therapy can be toler-ated with this larger goal in mind.
Fistulae
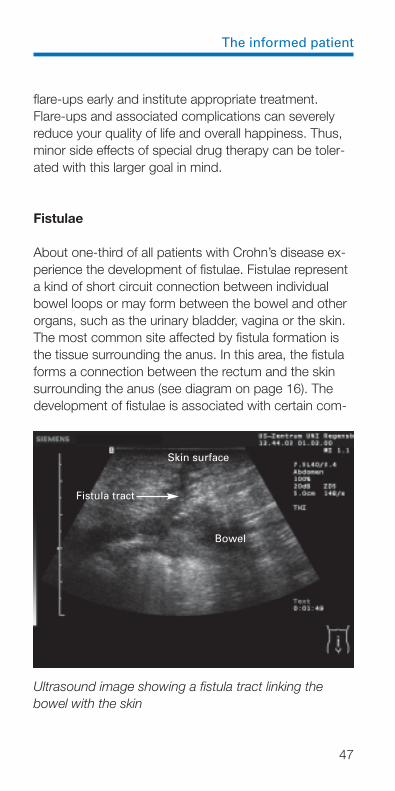
About one-third of all patients with Crohn’s disease ex-perience the development of fistulae. Fistulae representa kind of short circuit connection between individualbowel loops or may form between the bowel and otherorgans, such as the urinary bladder, vagina or the skin.The most common site affected by fistula formation isthe tissue surrounding the anus. In this area, the fistulaforms a connection between the rectum and the skinsurrounding the anus (see diagram on page 16). Thedevelopment of fistulae is associated with certain com-
47
Skin surface
Fistula tract
Bowel
Ultrasound image showing a fistula tract linking thebowel with the skin
plications, including the formation of abscesses (encap-sulated collections of pus). When the formation of fistu-lae is suspected, the physician will perform certain diag-nostic procedures. Depending on location, these includeradiologic examinations such as CT or MRI, proctoscopyand/or endosonography. The therapy of fistulae dependson their location and associated complications. Becauseof the associated inflammatory reaction, treatment maybegin with the administration of antibiotics. In certaincases, however, it may be necessary to surgically re-move the fistula or the bowel segment from which thefistula originates. This is often recommended in cases of fistulae that form between two bowel loops or whencomplicated by extensive abscess formation. In thelonger term, most patients will ultimately require eithersurgical or immunosuppressive (e.g. azathioprine) thera-py to definitively close the fistulae. A new treatmentmethod involves the suppression of the messengersubstance, tumor necrosis factor (TNF). This, however,usually results in only temporary closure of the fistulaand the method should be reserved for patients who donot respond adequately to the above-described medicalor surgical treatments. To date, however, no totally sat-isfactory method for treating fistulae has been devised.However, in most patients treatment is successful.
Osteoporosis
Over half of all patients with inflammatory bowel diseasessuffer from reduced bone mineral content. While suchbone loss can be mild or severe, both forms respond todrug treatment. Patients’ bone density should be mea-sured especially in cases of long-term administration ofcortisone preparations. Bone density is measured usingradiologic methods that expose the patient to relativelylow doses of radiation. Therapy in mild forms of bone
48
The informed patient
49
loss consists of the administration of vitamin D and cal-cium. More severe bone loss may require the use ofother drugs (bisphosphonates). These drugs directly in-hibit bone destruction but are associated with a higherrate of side effects than vitamin D and calcium.
Inflammatory bowel diseases during childhood
It would appear that the frequency of Crohn’s diseasein children is increasing. Thus, children and adolescentsshould be just as carefully examined and treated asadults. An additional problem in these young patients isthe fact that both the chronic bowel inflammation and,in some cases, the necessary drugs may result in dis-turbances of physical development. In such cases, aswell as in patients who do not respond to drug treat-ment, surgery must be considered. This will at leasttemporarily remove the site of inflammation.
Children by nature are more greatly affected than areadults by psychic stress. They also suffer more pro-foundly under the effects of chronic diseases and there-fore should be seen by a child psychiatrist as early aspossible after first diagnosis. More so than with adults, it is advisable that the treatment of inflammatory boweldiseases in children should be conducted in cooperationbetween the child’s family doctor and a clinical center.
The risk of cancer
The well-informed patient understands that the dangerof cancer is associated with any chronic inflammationthat persists for a long period of time. What does thismean, however, for patients with ulcerative colitis orCrohn’s disease?
Studies have shown that there is an increased risk ofcancer in patients with ulcerative colitis in whom theentire colon is affected and in whom the disease startsearly and has persisted for more than 10 years. For thisreason, all patients who have suffered from ulcerativecolitis for longer than 10 years should undergo endo-scopic examination of the colon at least every twoyears. This is the only way to detect the early signs ofmalignant degeneration, such as mucous membranedysplasia. If discovered in time, this abnormal tissue can be removed surgically, thus preventing the develop-ment of cancer. The risk of cancer is significantly lowerin Crohn’s disease. However, when only the colon isaffected, colonoscopy should be performed every twoyears in patients whose disease has persisted morethan 10 years.
Psychic stress
The realization that you have been diagnosed with achronic disease and will be confronted with it and itsassociated problems for many years to come naturallyaffects your personal sense of intactness and psychicconstitution in a very profound way. What can you do inorder to better cope with these problems?
Rule number one: You must confront your disease,then come to terms with it and accept it. You have theadvantage of recognizing your disease, an advantagenot shared by many other people. Coping with such adisease has its purpose and can be a source of enhancedself-confirmation and worth.
Rule number two: You must not let your illness controlyou. Those who lose courage suffer the most from theirdisease. You must actively confront your disease and
50
The informed patient
live a normal life – despite and even because of yourdisease. All means of actively confronting your diseaseare open to you. First and foremost, of course, are ra-tional medical treatment and drugs. However, otheralternatives – again, after consultation with your doctorto prevent undesired consequences – are preferable tolosing heart and doing nothing. Disease attacks the in-dividual as a whole. All therapeutic measures musttherefore also treat the person as a whole.
Self help groups
You are not alone in your disease. Coping with a chron-ic or other long-lasting illness can be made much easierby talking about it and its problems with others sufferingfrom the same disease. Self help groups and associa-tions have been formed in many towns and countries.The appendix offers more information on such groups inyour country.
Disability and career
You are unable to work during the active phase of yourdisease. This is equally true for inflammatory bowel dis-eases as for any other disease and applies to every pro-fession or line of work. Because of the typical chronic,episodic course of the disease, you must be prepared,whatever your work, for short, disease-related periodsof disability. However, job re-training or giving up acareer are only necessary in a few individual cases.Under certain circumstances, such as after major ab-dominal surgery, the presence of fistulae or in patientswhose disease has not responded adequately to med-ical treatment, heavy physical work is not advisable.
51
Such patients, however, can normally perform otherjobs involving only light physical activity or that can beperformed in seated position.
Adolescents, in whom there has been an increasedoccurrence of inflammatory bowel diseases in recentyears, should particularly be encouraged to completetheir vocational or professional training.
Recreation
Similar considerations apply to recreation as apply towork and career. All options remain open to you despiteyour disease. Only in phases of severe inflammationshould certain restrictions be placed on your physicalactivity. With the exception of high-performance sports,physical activity in any form is fully recommended. Thisis true even in patients undergoing long-term drug treat-ment. In fact, particularly in patients receiving cortisonepreparations, regular exercise of the muscles, joints andbones is highly recommended and may help reduce orprevent some of the side effects of these drugs.
It is also normally possible to take vacations in foreigncountries. The required vaccinations, however, shouldbe given only after consultation with the physician treat-ing your IBD, though, as a rule, there is no reason not toget them. One special factor is the long-term treatmentof Crohn’s disease with the antibiotic, metronidazole.Patients receiving this drug should protect themselvesfrom direct sunlight and avoid alcohol.
52
The informed patient
Sex and partnership
Here, too, no specific restrictions are required. Sexualactivity will naturally be reduced during an acute diseaseflare-up. In females, the body’s natural mechanism forconserving its energies and resources may result in in-terruption of menstruation.
The formation of fistulae in patients with Crohn’s diseasemay, in certain cases, affect the internal and externalgenital organs, resulting in a mechanical restriction ofsexual activity. Such fistulae require intensive medicalattention and drug therapy. Thus, prompt consultationof a physician is advisable.
Reproduction and genetic factors
In our discussion of the causes of inflammatory boweldiseases, we noted that genetic predisposition probablyplays a role in both ulcerative colitis and Crohn’s dis-ease. Should this be considered a reason not to havechildren?
The probability of inheriting a predisposition to inflam-matory bowel disease is low. Thus, the risk that childrenof persons with IBD will develop either ulcerative colitisor Crohn’s disease is therefore not considered to bevery high. This small risk should not deter personsaffected by IBD from having children.
53
Pregnancy
This section is closely related to the last. Is it advisablefor women with IBD to become pregnant and shouldthese women attempt to carry pregnancies to term anddeliver normally?
In answering these questions, it is important to state atthe outset that pregnancy has not been shown to ad-versely affect the clinical course of either ulcerative coli-tis or Crohn’s disease in any way. Thus, the decision toconceive can be supported in patients who desirechildren. It is, of course, important to plan the pregnan-cy, so that it does not occur during a period of morepronounced disease activity. During pregnancy, patientsshould be carefully monitored in cooperation betweenan internist and gynecologist. Should an acute diseaseflare-up occur during pregnancy, treatment with corti-sone and 5-aminosalicylic acid preparations is possible.Careful administration of these drugs will control inflam-matory activity without producing side effects in theembryo. Patients undergoing long-term treatment withazathioprine, however, should use contraception. Thetwo most effective methods of birth control, the pill andthe intrauterine device (IUD), are both somewhat contro-versial in patients with IBD. The best form of contracep-tion must be individually decided, if possible, by an in-ternist and gynecologist working together.
“Ostomy”: the artificial bowel outlet
Newly developed surgical techniques make it possiblein many cases of ulcerative colitis to remove the entirecolon without permanent creation of an artificial boweloutlet, or “ostomy” (see illustration on page 41). In fact,a permanent ostomy is required only in very rare cases.
54
The informed patient
The creation of a temporary ostomy in patients with ul-cerative colitis and Crohn’s disease may, however, actu-ally have a beneficial effect on the disease. The ostomyis usually closed after four to six months. Modern osto-my appliances make it possible to live a practically nor-mal life, including sports and sexual activity, despite theartificial bowel outlet. Early retirement due to a perma-nent ostomy is necessary only in the rarest of cases.
If, however, your disease and its treatment do requirethe placement of an artificial bowel outlet, you shouldcontact and listen to the experiences of others whohave been in your condition. Ostomy patients haveformed self help groups in many cities and countries.Once again, we refer you to the appendix for a list ofgroups and contact information.
55
What should you keep in mind, as apatient with inflammatory boweldisease?
1 Maintain regular medical follow-up even in phaseswhen your illness is in remission. Patients with com-plications should seek rapid referral to a gastroen-terological center in which internists and surgeonswill cooperate in your care.
2 Inform yourself about possible dietary measures andconsult a reputable dietician.
3 Never forget: the more you control your disease theless your disease will control you.
4 If your physician prescribes a long-term drug therapyregimen, you must comply with it as closely as pos-sible. Medications should be discontinued or theirdose changed only after consulting with the respon-sible physician. Ask your doctor about possible sideeffects and about how to recognize them.
5 Learn to recognize the signs of increased diseaseactivity. In ulcerative colitis, these include changesin the stool up to and including bloody diarrhea, ab-dominal pain and general signs such as tirednessand fatigue. In Crohn’s disease these include ab-dominal pain, weight loss, changes in stool (diarrheaor constipation) and general deterioration in physicalperformance. In both diseases, there may be symp-toms outside the bowel, including pain in the joints,inflammation of the eyes, changes in the skin andmucous membranes, back pain and renal colics.You should inform your doctor immediately if thesesigns are recognized. These symptoms may not
56
The informed patient
always be due to IBD, however. Often, they may bedue to dietary mistakes (for example, diarrhea fol-lowing consumption of raw fruit) or bowel infections,which may occur as well in patients with IBD.
6 Inform yourself about your disease and about yourindividual case. It may also be helpful to keep a diaryor journal. In any long-term disease, it is probablethat a number of physicians, independent of eachother, will be involved in your care. Collect informa-tion on the examinations you have undergone aswell as surgical reports. Important are the namesand addresses of the physicians and hospitals whoexamined you or performed operations or other pro-cedures, as well as the date and measures under-taken. You yourself should know how extensive yourinflammation is and what treatment methods havealready been tried. Also note any side effects or in-tolerance to medications.
57
Glossary
Abscess Encapsulated collection of pus oc-curring in areas of inflammation dueto bacteria
Anemia An abnormality of the blood caused by a deficiency of hemoglobin or in the number of red blood cells(erythrocytes)
Colon The large bowel
Duodenum First segment of the small bowel
Dysplasia Abnormal development of tissue. Dysplasia may occur in differentdegrees of severity and may be considered a precursor of cancer of the bowel
Erythema Violet-red thickening of the nodosum skin, usually on the arms or legs
Fistula Abnormal, “short circuit” connectionbetween two bowel segments,between the bowel and the bladderor vagina, or between the bowel andthe skin occurring as a result of inflammation
IBD Inflammatory bowel disease
Ileocecal valve Valve-like structure forming the junction between the lower segmentof the small bowel (ileum) and thecolon
Ileum Final segment of the small bowel
Ileus Obstruction of the bowel caused bynarrowing (stenosis) or paralysis
58
The informed patient
Immuno- Therapy aimed at inhibiting the body’s suppression immune system
-itis Suffix denoting inflammation. For ex-ample, “colitis” means inflammation of the colon.
Jejunum Middle segment of the small bowel
Osteoporosis Loss of bone tissue or changes in theoverall form of the bone resulting inreduced mechanical strength and atendency to fracture
Perforation Formation of a hole in the wall of ahollow organ, such as the bowel
Peritonitis Inflammation of the membrane liningthe inner surface of the abdomen
Pouch Reservoir for stool that is surgicallycreated from a bowel loop
Recurrence Renewed manifestation of diseasesymptoms, such as an acute flare-upin IBD
Stenosis Narrowing of the bowel often causedby inflammation. Over time, long-lasting inflammation can result inscar-tissue formation that makes thenarrowing permanent.
Stricture Another name for stenosis. Strictures,however, represent narrowing of thebowel that has become permanentdue to scar-tissue formation.
Stricturoplasty Surgical procedure to release stric-tures in the bowel without excision(removal) of the entire segment ofnarrowed, stenotic bowel
59
Subileus Incomplete form of intestinal obstruc-tion or ileus
Toxic Complication occurring mostly in megacolon patients with ulcerative colitis and
involving an acute dilation (ballooning)of the colon
Tumor-Necrosis- Messenger substance in the humanFactor (TNF) body that plays an important role in
inflammatory processes
Ulcer Hole or defect in the mucous mem-brane lining of an internal organ
60
The informed patient
Self help groups
Ulcerative colitis/Crohn’s disease
AustraliaAustralian Crohn’s and Colitis Association Inc. (ACCA)National OfficeP.O. Box 201Moorolbark, VIC., 3138Tel.: xx (61) 397/269008Fax: xx (61) 397/269914E-mail: [email protected]: http://www.acca.net.au
AustriaÖsterreichische Morbus Crohn/Colitis ulcerosa Vereinigung – ÖMCCV –Obere Augartenstr. 26–28A-1020 ViennaTel./Fax: xx (43) 1-3330633E-mail: [email protected]: http://www.oemccv.or.at/crohn-colitis
BelgiumCrohn en Colitis ulcerosa Vereniging vzw (CCV)Groeneweg 151B-3001 HeverleeTel.: xx (32) 16207312Fax: xx (32) 16208732E-mail: [email protected]: http://www.ccv-vzw.be
61

Association Crohn-RCUHSecrétariat administratif17, rue de la Forêt de SoignesB-1410 WaterlooTel./Fax: xx (32) 23541285E-mail: [email protected]: http://www.mici.be
CanadaCrohn’s and Colitis Foundation of Canada (CCFC)National Office60 St. Clair Avenue EastSuite 600Toronto, ON, Canada, M4T 1N5Tel.: 001 (416) 920.5035Fax: 001 (416) 929.0364E-mail: [email protected]: http://www.ccfc.ca
Czech RepublicCrocodile CzJirovcova 24CZ-37004 BudweisTel./Fax: xx (420) 38635364 9E-mail: [email protected]: http://www.volny.cz/ccd
DenmarkColitis-Crohn-Foreningen (CCF)Birkegade 11DK-2200 Copenhagen NTel.: xx (45) 35354882Fax: xx (45) 35354782E-mail: [email protected]: http://www.ccf.dk
62

The informed patient
European Federation of Crohn’s and Ulcerative Colitis Associations – EFCCA –Mr. Tor Erik Jørgensen, secretaryParallellen 13 AN-1430 AsNorwayTel.: xx (47) 64941671Fax: xx (47) 22937213E-mail: [email protected]: http://www.efcca.org
FinlandCrohn ja Colitis RY (CCAFIN)Kuninkaankatu 24 ASF-33210 TampereTel.: xx (358) 32662600Fax: xx (358) 32662660E-mail: [email protected]: http://www.crohnjacolitis.fi
FranceAssociation François Aupetit (AFA)Hôpital Rothschild33, Boulevard de PicpusF-75571 Paris-Cedex 12Tel.: xx (33) 140199919Fax: xx (33) 140193436Internet: http://www.afa.asso.fr
GermanyDeutsche Morbus Crohn/Colitis ulcerosa Vereinigung – DCCV – e.V.Paracelsusstr. 15D-51375 LeverkusenTel.: xx (49) 214 /87608-0Fax: xx (49) 214 /87608-88E-mail: [email protected]: http://www.dccv.de
63
HungaryMagyarországi Crohn-ColitesesBetegek Egyesülete (MCCBE)Igmándi utca 22. Fzst. 1H-1112 BudapestTel.: xx (361) 3228098Fax: xx (361) 3229287E-mail: [email protected]: http://www.extra.hu/mccbe
IrelandIrish Society for Colitis and Crohn’s Disease (ISCC)Carmichael CentreNorth Brunswick StreetDublin 7Tel.: xx (353) 18721416Fax: xx (353) 18735737E-mail: [email protected]: http://www.iscc.ie
ItalyFederazione Nazionale delle Associazioni per le Malattie Infiammatorie Croniche dell’lntestino (AMICI)Via Adolfo Wildt,19/4I-20131 MilanTel.: xx (39) 22893673Fax: xx (39) 226822670E-mail: [email protected]: http://www.amicilom.org
64

The informed patient
LuxembourgAssociation Luxembourgeoise de la Maladie de Crohn (ALMC)P.O. Box 648L-2016 LuxembourgTel.: xx (352) 47509828Fax: xx (352) 47982020E-mail: [email protected]: http://www.afa.asso.fr/luxembourg
The NetherlandsCrohn en Colitis Ulcerosa Vereniging Nederland (CCUVN)Wilhelminastraat 45aNL-3621 VG BreukelenTel.: xx (31) 346261001Fax: xx (31) 346264974E-mail: [email protected]: http://www.crohn-colitis.nl
NorwayLandesforeningen mot Fordøyelsessykdommer (LMF)c/o FFO, SmågruppesekretariatetPostboks 4568, NydalenN-0404 OsloTel.: xx (47) 88005021Fax: xx (47) 88005031E-mail: [email protected]
PortugalAssociação Portuguesa da Doença Inflamatória do Intestino (APDI)Rua Santa Catarina no. 922, 4° esq.P-4000-446 PortoTel./Fax: xx (351) 222086350E-mail: [email protected]: http://www.apdi.org.pt
65

SlovakiaSlowak Crohn Club (SCC)c/o Ing. Tomáš Gertler/COSMEXNevädzova 8, P. O. Box 60SK-827 99 BratislavaTel.: xx (421) 243427448Fax: xx (421) 243338020E-mail: [email protected]: http://www.cosmex.sk
South AfricaSouth African Crohn’s & Colitis AssociationP.O. Box 2638ZA-8000 Cape Town Tel./Fax: xx (27) 21214677E-mail: [email protected]: http://www.ccsg.org.za
SpainAsociación de Enfermos de Crohn y Colitis ulcerosa de España (ACCU)c/Hileras 4, 4º, 6 y 7E-28013 MadridTel.: xx (34) 915475505Tel./Fax: xx (34) 915426326E-mail: [email protected]: http://www.accu.esp.com
SwedenRiksförbundet för Mag- och Tarmsjuka (RMT)P.O. Box 20054S-10460 StockholmTel.: xx (46) 86424200Fax: xx (46) 86421100E-mail: [email protected]: http://www.magotarm.se
66
The informed patient
SwitzerlandSchweizerische Morbus Crohn/Colitis ulcerosa-Vereinigung (SMCCV)PostfachCH-5001 AarauTel./Fax: xx (41) 628248707E-mail: [email protected]: http://www.smccv.ch
UKNational Association for Colitis and Crohn’s Disease (NACC)4 Beaumont House, Sutton RoadSt. Albans, Herts AL1 5HHTel.: xx (44) 1727844296Fax: xx (44) 1727862550E-mail: [email protected]
[email protected]: http://www.nacc.org.uk
USACrohn’s and Colitis Foundation of America, Inc. (CCFA)386 Park Avenue South, 17th FloorNew York, NY 10016-8804Tel.: 001 (800) 932-2423
001 (212) 685-3440Fax: 001 (212)779-4098E-mail: [email protected]: http://www.ccfa.org
67
Self help groups for patients with ileostomy
AustriaÖsterreichische ILCOObere Augartenstr. 26–28A-1020 ViennaTel.: xx (43) 1-3323863E-mail: [email protected]: http://www.ilco.at
GermanyDeutsche ILCO e.V.Landshuter Str. 30, D-85356 FreisingPostfach 1265, D-85312 FreisingTel.: xx (49) 8161/934301/934302Fax: xx (49) 8161/934304E-mail: [email protected]: http://www.ilco.de
Switzerlandilco-Schweizc/o Peter SchneebergerBuchenweg 35CH-3054 SchüpfenTel.: xx (41) 318792468
UKIleostomy and Internal Pouch Support GroupPeverill House1–5 Mill RoadBallyclareCo. AntrimBT39 9DRTel.: xx (44) 2893344043, 08000184724Fax: xx (44) 2893324606E-mail: [email protected]: http://www.the-ia.org.uk
68
Further information for patientswith inflammatory bowel disease:
– Nutrition in inflammatory bowel diseases55 pages (S84UK)
– Accompanying Diseases inCrohn’s Disease40 pages (S85UK)
– Corticosteroid therapy in inflammatory bowel diseases28 pages (Bu80UK)
– Crohn’s Disease, Ulcerative Colitis and Pregnancy51 pages (S82UK)
These brochures can be ordered free of chargefrom Falk Foundation e.V. or the local Falk partner.
The informed patient
Leinenweberstr. 5Postfach 652979041 FreiburgGermany
FALK FOUNDATION e.V.

S80U
K2-
12/2
005/
2.00
0 K
on
k
Leinenweberstr. 5Postfach 652979041 FreiburgGermany
FALK FOUNDATION e.V.
FOUNDATION e.V.