Embed Size (px)
Citation preview

ULTRASONOGRAPHY OF THE NORMAL FELINE PANCREAS AND ASSOCIATED ANATOMIC LANDMARKS: A PROSPECTIVE STUDY OF
20 CATS
SHEILA M. ETUE, DVM, DOMINIQUE G . PENNINCK, DVM, DVSc, MARY ANNA LABATO, DVM, SUSAN PEARSON, BA, CVT, AMY TIDWELL, DVM
The sonographic appearance of the feline pancreas and associated anatomic landmarks including the pancreatic duct, duodenum, duodenal papilla, portal vein, and gastric lymph node were evaluated in 20 healthy, awake cats. The pancreas appeared nearly isoechoic to surrounding mesenteric tissues, iso- echoic to slightly hyperechoic to adjacent liver lobes, and hypoechoic to the spleen. The mean thickness measurements for the right pancreatic lobe, body, and left pancreatic lobe were 4.5 mm (range 2.8-5.9), 6.6 mm (range 4.7-94, and 5.4 mm (range 3.4-9.0), respectively. The pancreatic duct was consistently visualized in the left pancreatic lobe and had a mean thickness of 0.8 mm (range 0.5-1.3). It could be differentiated from the pancreatic vessel, by its central location, and the duct’s lack of Doppler flow signal. The duodenum was used as a landmark to identify the right lobe of the pancreas. The mean duodenal wall thickness measurement was 2.8 mm (range 2.1-3.8) in sagittal section, and 3.0 mm (range 2.2-4.4) in transverse section. The duodenal papilla was identified in 4 of 20 cats. It ranged in size from 2.9 to 5.5 mm in width, and had a maximum height of 4.0 mm in transverse section. The portal vein was used as a consistent anatomic landmark for identification of the left lobe and body of the pancreas. The mean diameter of the portal vein at the level where the pancreatic body joins the left pancreatic lobe was 4.3 mm (range 2.7-5.9) when viewed in sagittal section, and 4.5 mm (range 3.6-6.1) in transverse section. The gastric lymph node was identified cranial and ventromedial to the pyloroduodenal angle in 6 of 20 cats. It had an asymmetrical shape with a larger caudal pole in five of the six cats. The largest dimensions of the gastric lymph node were 10 mm in length, and 6 mm in width for the larger caudal pole, and 5.1 mm in width for the smaller cranial pole. Veterinary Radiology & Ultrasound, Vol. 42, No. 4, 2001, p p 330-336.
Key words: ultrasonography, pancreas, cat, feline.
Introduction
ISORDERS OF THE PANCREAS are considered uncommon D in the cat. However, there is growing evidence that pancreatitis occurs more frequently than once believed. ’*’ The ante-mortem diagnosis of feline pancreatic disease poses a significant challenge to the clinician because signs are often nonspecific, and blood chemistry and radiography are considered unreliable. -3 While computed axial tomog- raphy is the most useful imaging modality for pancreatic evaluation in humans, the expense, need for general anes-
From the Department of Clinical Sciences, Section of Radiology (Etue, Penninck, Pearson, Tidwell), and the Section of Medicine (Labato), Foster Hospital for Small Animals, Tufts University School of Veterinary Medi- cine, North Grafton, MA 01536.
Address correspondence and reprint requests to Dr. S.M. Etue, Depart- ment of Clinical Studies, Section of Radiology, Ontario Veterinary Col- lege, University of Guelph, Guelph, Ontario, Canada, NIG 2Wl .
This project was supported by a grant from the Quinby Taylor Education Foundation.
Received August 9. 2000; accepted for publication November 27, 2000.
thesia, and limited availability make it less useful in veteri- nary medicine.”’ As a result, ultrasound is currently con- sidered the imaging modality of choice in the evaluation of pancreatic disease in animals.436 In a recent report of feline pancreatitis in four cats, one of the most significant obser- vations was the usefulness of ultrasound in detecting patho- logic changes.’ The ultrasonographic parameters used to evaluate canine pancreatitis have been Cur- rently, ultrasonographic evidence for pancreatitis in the dog consists of various changes, depending on the level of in- flammation, such as pancreatic enlargement, and changes in echogenicity. Decreased echogenicity in acute pancreatitis is thought to be a result of edema and inflammatory infil- trate.6 In contrast, increased echogenicity suggests fibrotic changes.6 Extrahepatic biliary obstruction, peritoneal effu- sion, duodenal hypomotility, and increased duodenal wall thickness have also been reported to be associated with pan~reati t is .~-~
To our knowledge, the normal ultrasonographic features of feline pancreatic anatomy have not been established. The
330

VOL. 42, No. 4 NORMAL FELINE PANCREAS ULTRASONOGRAPHY 33 1
purpose of our study was to establish the ultrasonographic characteristics of the feline pancreas by determining its nor- mal tissue echogenicity, structure, dimensions, and associ- ated anatomical landmarks. The reproducibility of pancre- atic measurements, and the effect of age, sex, body condi- tion, and weight were also assessed. Knowledge of these normal ultrasonographic features is essential for an accurate assessment of pathologic changes and can be used as a reference guide for the diagnostic workup of feline pancre- atic disease.
Materials and Methods
Ultrasonographic examinations were performed on 20 awake cats (1 1 neutered males and 9 neutered females) between 1 and 9 years of age with a body weight between 2.7 and 7.4 kg. All cats were healthy and free of alimentary tract disease on the basis of history, physical examination, and laboratory evaluation, including: a complete blood count (CBC), serum biochemical analysis with serum li- pase, fibrinogen level, urinalysis, feline leukemia and feline immunodeficiency virus testing, and toxoplasmosis titers (IgG and IgM). Each cat was assigned a body condition score from 1 to 9 based on published reference values for body fat indices.'" All procedures were approved by the Institutional Animal Care and Use Committee, Tufts Uni- versity, School of Veterinary Medicine.
Food was withheld for 12 hours prior to ultrasound ex- amination to limit the ultrasound wave propagation inter- ference with gas within the stomach and adjacent bowel. Water was available at all times. Ultrasound examinations were performed with the cats in dorsal recumbency. The hair was clipped from the ventral abdomen and acoustic, coupling gel was applied. All ultrasonic evaluations were performed using a real-time curvilinear array scanner with a transducer frequency of 8 to 5 MHz.* Real-time images were stored on videotape, and static images were recorded on single emulsion film using a multi-format camera.
Images of the pancreas were obtained in a manner similar to that previously described.6 Any difficulties in visualiza- tion of the pancreas were noted. The echogenicity of the pancreatic parenchyma was assessed relative to the sur- rounding mesentery, hepatic parenchyma and spleen. The echogenicity was defined as hypoechoic, isoechoic, or hy- perechoic.
Visualization of a pancreatic duct or vessel in the left and right pancreatic lobes was recorded and confirmed by color- flow Doppler analysis. The luminal diameter of the duct or vessel in sagittal section was recorded.
Thickness measurements in millimeters for the right lobe, body, and left lobe of the pancreas were made in both the
*ATL HDI 3000, Advanced Technology Laboratories, Inc., Bothell, WA 9804 I .
sagittal and transverse plane using electronic calipers. The right lobe was measured ventromedial to the right kidney and medial to the descending duodenum. Measurements of the body of the pancreas were obtained directly caudal to the pyloroduodenal angle whenever possible and medial to the proximal descending duodenum. The left lobe was mea- sured in the region caudal to the stomach, cranial to the left kidney, and medial to the spleen.
The diameter of the portal vein in the sagittal and trans- verse plane was recorded at the level of the pancreatic body. The mural thickness of the descending duodenum was mea- sured from the mucosal to the serosal surfaces. The dimen- sions of the duodenal papilla were recorded, when observed, in its largest left to right and dorsal to ventral axes. The cranial abdomen was scanned at the pyloroduodenal angle, craniomedial to the pylorus for the gastric lymph node. Its ultrasonographic appearance was recorded when it was ob- served, and its measurements were recorded in the sagittal plane.
The consistency of repeated measurements was assessed by linear correlation analysis. A minimum of 3 measure- ments were obtained whenever possible, for each anatomic area of interest, during each examination. Student's t test was performed to assess the influence of the fixed param- eters, age, sex, body weight, and condition score, on pan- creatic dimensions. A P-value of <0.05 was considered sig- nificant for all analyses. The descriptive statistics (mean, standard deviation, and range) were calculated directly from the individual measurements obtained at each ultrasono- graphic examination.
Results A schematic drawing of the pancreas in the cat is pro-
vided to demonstrate the position and shape of the pancreas within the abdominal cavity, as well as the principal ana- tomic landmarks used in this study (Fig. l). Figures 2, 3, and 4 illustrate the ultrasonographic appearance of the left lobe, right lobe, and body of the feline pancreas, respec- tively. The pancreatic echotexture was smooth and homo- geneous. It appeared nearly isoechoic to the surrounding mesenteric fat, isoechoic or slightly hyperechoic to the liver, and hypoechoic to the spleen. This finding is in agreement with previous reports.6.' '
The measured thickness of the right lobe, body and left lobe of the feline pancreas, pancreatic duct, duodenum, and portal vein are presented in Table 1. The reported pancreatic measurements were well correlated (linear correlation coef- ficient, r = 0.7 to 0.8), with no consistent bias evident. The pancreatic measurements were not significantly affected (P > 0.05) by differences in age, sex, body weight, or body condition. The body of the pancreas was not measured in cats 2 or 8. Cat #2 had not been fasted and the presence of food in the stomach hampered visibility of the adjacent pancreas. Cat #8 was too fractious to allow completion of

332 ETUE ET AL. 2001
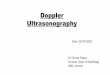
FIG. 2. Sagittal sonographic image of the normal left lobe of the feline pancreas. The margins of the uniformly echogenic pancreas are outlined by cursors. An ai-row points toward the pancreatic duct. S = stomach in the near field.
FIG. I . Schematic illustration of feline pancreas drawn from a cadaver specimen. The schematic represents a ventral view of the abdomen. Cranial is at the top of the illustration and caudal is at the bottom. GN = gastric lymph node, PV = portal vein, RK = right kidney, LK = left kidney, DD = descending duodenum, S = spleen.
the examination. A similar lack of patient cooperation pre- vented measurement of the right pancreatic lobe in cat #4. As a result, only 18 measurements of the pancreatic body, and 19 measurements of the right pancreatic lobe were ob- tained. It was not possible to obtain a minimum of 3 mea- surements for the right lobe, and pancreatic body, or for the duodenum. The left lobe of the pancreas was consistently easier to locate, and a minimum of 3 measurements of the left lobe was obtained for all 20 cats. The thickness mea- surements for the left pancreatic lobe were greater than the right lobe for every cat in the study. The thickness mea- surements for the pancreatic body were also consistently greater than either the right or left lobe. The pancreatic duct was identified by its anechoic, tubular appearance with sur- rounding, thin, hyperechoic wall, and its central location (Fig. 5). It was observed in all 20 cats in this study but could only be confirmed to be a nonvascular structure by the use of Doppler analysis (color and/or power angiography) in 17 of the 20 cats. In the 3 cats for which verification could not be established, respiratory or overall patient motion ham- pered confirmation. It was most consistently observed in the left pancreatic lobe, (14/17 cats). The pancreatic duct was
observed and verified in the right pancreatic lobe in only 2 cats (cats 5, 16). It was observed and verified in the body of the pancreas in 4 cats (cats 9, 12, 14, and 17). The pancre- atic duct could be followed to the duodenal papilla in 4 cats (Fig. 6A). The duodenal papilla, in transverse section ranged in size from 2.9 to 5.5 mm in width and 4.0 mm in maximum height (Fig. 6B).
The pancreatic duct appeared as a tubular, anechoic struc- ture with a well-defined, thin hyperechoic wall, coursing through the center of the pancreatic parenchyma. It had a narrow lumen with a mean diameter of 0.8 mm (Table 1). A vascular structure within the pancreatic parenchyma was identified in only one of the cats in our study (cat 11). Both the duct and vessel were clearly identified in the left pan- creatic lobe of this particular cat. The vessel was located ventral to the pancreatic duct, close to the ventral surface of the pancreas. While the appearance of the vessel was similar to the duct, it could be differentiated from the pancreatic duct by its eccentric position, and larger diameter of 2.1 mm, (more than twice the size of the pancreatic duct). Color-flow Doppler was helpful in confirming the flow within the vessel.
The portal vein was measured at the junction of the left pancreatic lobe and the pancreatic body. The relationship to the pancreatic body and left lobe is shown in Fig. 4. The mean diameter, including range and standard deviation is listed in Table 1 .
The gastric lymph node was observed in 6 of 20 cats. All 6 cats were approximately one year of age. The gastric lymph node was located craniomedial to the pylorus. In 5 of

VOL. 42, No. 4 NORMAL FELINE PANCREAS ULTRASONOGRAPHY 333
FIG. 3. (A) Sagittal sonographic image of the normal right lobe of the feline pancreas. The margins of the pancreas are outlined by cursors. The ventrolateral position of the descending duodenum, wen in the near field, is helpful in localizing this lobe. Arrow points to the pancreatic duct. DUOD = descending duodenum. (B) Transverse sonographic image of the normal right lobe of the feline pancreas. The pancreatic parenchyma, out- lined by cursors, is poorly distinguished from the surrounding mesenteric fat. The duodenum, outlined by arrows, is a useful anatomic landmark. The layered wall of the duodenum is clearly seen.
the 6 cats it had an asymmetric shape with a larger caudal pole than cranial pole (Fig. 7). In the 6th cat, it had a rounded appearance with no visible poles. The gastric lymph node in all 6 cats had a hyperechoic central region surrounded by a more hypoechoic outer region. Its largest dimensions were 6 mm (ventral to dorsal plane) for the larger caudal pole, 5.1 mm (ventral to dorsal plane) for the smaller cranial pole, and 10 mm (left to right axis) for its greatest overall length.
FIG. 4. Sagittal sonographic image of the normal body of the feline pancreas at the level of the pyloroduodenal angle. The margins of the pancreas are outlined by arrows. The portal vein (PV) is seen in cross- section. ST = stomach, B = body of the pancreas, LL = left lobe of pancreas.
Discussion
Ultrasonographic evaluation of the feline pancreas can be technically challenging. Systematic scanning technique and knowledge of surrounding anatomic structures are impor- tant to accurate evaluation. Even with higher frequency transducers, the margins of the pancreas are not well delin- eated from surrounding structures." This may, in part, be attributed to the similar intrinsic echogenicity of the pan- creas and surrounding fat. Attenuation of the sound beam is also increased in obese individuals making examination of young, thin individuals e a ~ i e r . ~ The interference by intralu- minal gas within the stomach and duodenum can hamper evaluation. A fluid-filled duodenum may change shape with differential pressure and the presence of peristaltic activity may hamper clear visualization of the right pancreatic lobe. Therefore, the quality of the examination can be improved with fasting. Poor patient cooperation and excessive breath motion also are significant factors contributing to the qual-
TABLE I . Measurements of the Normal Feline Pancreas and Associated Anatomical Landmarks
Anatomical Structure
Right lobe Body Left lobe Duct (S) Portal vein (T) Portal vein (S) Duo (T) Duo (S)
No. of Cats
19 18 20 17 19 19 14 17
Range (mm)
Minimum
2.8 4.7 3.4 0.5 3.6 2.7 2.2 2.1
Maximum
5.9 9.5 9.0 I .3 6.1 5.9 4.4 3.8
Mean (mni) S.D.
4.5 0.87 6.6 1.32 5.4 1.46 0.8 0.25 4.5 0.61 4.3 0.86 3.0 0.69 2.8 0.55
S.D. = standard deviation, mm = millimeter5, T = transverse section, S = sagittal section.

334 ETUE ET AL. 2001
FIG. 5. Power Doppler sonogram. The absence of flow in the pancreatic duct in the cat is apparent. The pancreatic duct is seen as a tubular anechoic structure with a thin, hyperechoic wall, coursing through the center of the pancreatic parenchyma. An arrow is directed toward the duct. The margins of the left lobe of the pancreas are outlined by cursors.
ity of the ultrasonographic examination. During examina- tion of the diseased pancreas, the use of sedation, or anal- gesics may be useful to improve tolerance of the procedure and reduce patient motion.
Detailed descriptions of scanning techniques have been published for the canine6,7 and feline6 pancreas. H ~ ~ ~ ~ ~ ~ , no detailed anatomic description is avaiIable for the cat.
FIG. 6. (A) Sagittal sonographic image of the duodenal papilla. Color Doppler was used to confirm the absence of flow signal in the pancreatic duct. D = duodenum, DP = duodenal papilla, PV = portal vein. (B) Transverse sonographic image of the duodenal papilla (between cursors),
3.7 nlm in left to right awis. Feline pancreatic anatomy can be compared to the canine pancreas. Like the dog, the cat pancreas is divided into three anatomic regions, which include the right lobe, left lobe, and body (Fig. 1). The right pancreatic lobe lies dorsome- dial to the descending duodenum and is united with the left lobe at the pancreatic body.12 In contrast to the dog, the distal third of the feline right lobe curves cranially giving it a hook-like appearan~e. '~ The left lobe originates at the pancreatic body, and extends across the abdomen dorsocau- dal to the stomach and dorsocranial to the transverse co- lon.6312 The distal extremity of the left lobe, in the region of the left kidney has a curved appearance, however to a lesser extent than the right. In comparison to the dog, the py- loroduodenal angle14 and the pancreatic body are more cen- trally located. Also in the cat, the angle formed by the left and right lobes with the pancreatic body is smaller. This finding may be partially attributed to the more acute inci- sura angularis of the feline s t0ma~h . l~
In our study, the left pancreatic lobe was consistently more easily visualized than the right, while in the dog, the left pancreatic lobe is less consistently identified.I6 The rea- son for this difference remains unclear, however it may be
partially attributed to the thinner size of the right pancreatic lobe in the cat compared to the left. The larger size deter- mined for the pancreatic body compared to the right and left lobes in this study may have been overestimated by overlap of the pancreatic parenchyma where the two lobes unite (Fig. 8). Nevertheless, the measurements were highly re- peatable.
The pancreatic duct(s) arise embryonically from either the dorsal or ventral bud-like duodenal primordia. Large, interlobular ducts run longitudinally in the middle of the pancreas, forming a common duct at about the angle of the gland, terminating in the duodenum. They may arise em- bryonically from either the dorsal or ventral, bud-like duodenal primordia. In the cat, usually only one duct, the main pancreatic duct exists. It arises from the ventral pri- mordium and usually opens with the bile duct on the major duodenal papilla. The major duodenal papilla is located on the dorsal internal wall of the duodenum approximately 3 cm distal to the py10rus.'~ In approximately 20% of cats a second duct, the accessory duct, exists. It arises from the

VOL. 42, No. 4 NORMAL FELINE PANCREAS ULTRASONOGRAPHY 335
FIG. 7. Normal sonographic appearance of the gastric lymph node (be- tween cursors), located craniomedial to the pyloroduodenal angle. Note the asymmetric shape seen in 5 of 6 cats; the caudal pole is larger than the cranial pole. The outer margins are hypoechoic in comparison to the hy- perechoic center. Dimensions (cursors) are 10 mm for left to right axis and 4.6 mm for ventral to dorsal axis. D = duodenum, L = liver.
dorsal primordium and opens into the minor duodenal pa- pilla approximately 2 cm caudoventral to the major duode- nal papilla.'23'7318 The pancreatic duct was most often ob- served in the left pancreatic lobe and proved to be a useful landmark for identifying pancreatic tissue. In addition, by always assuming a central location of the duct within the pancreatic parenchyma, a more accurate determination of the pancreatic margins could be made, avoiding over or under estimation of pancreatic size by tangential beam angle.
Blood supply to the pancreas is primarily from branches of the celiac artery, which include: 1) the splenic artery supplying the distal segment of the left lobe; 2) the gas- troduodenal artery to the body of the pancreas, and its ter-
FIG. 8. Right lobe, left lobe, and body of the feline pancreas in a cadaver specimen outlined by arrows. Note the folded appearance of the body of the pancreas where the two lobes unite. The tip of a 22 gauge needle is directed toward the portal vein (portal v.) which crosses the body of the pancreas dorsally on its way to the hepatic hilus. Lt = left lobe, Rt = right lobe, D = descending duodenum.
minal branch; and 3 ) the pancreaticoduodenal artery and its branches which course through the parenchyma of the gland. The caudal pancreaticoduodenal branch of the cranial mesenteric artery supplies the remainder of the pan- creas.12.18.19 Various anastomoses are formed between these vessels within the substance of the gland. Drainage occurs through several portal tributaries, which include the cranial and caudal pancreaticoduodenal veins to the splenic and cranial mesenteric veins, r e s p e c t i ~ e l y . ' ~ ~ ' ~ ~ ~ ~ In the dog, the pancreaticoduodenal artery and vein have been described ultrasonographically coursing along a longitudinal path through the parenchyma of the right pancreatic lobe.6393' ' , I 6
In our study, a pancreatic vessel was identified in only one cat. It was located in the left lobe of the pancreas close to the ventral surface of the pancreas. The sonographic appearance of the pancreatic duct or vessel is similar; however, the duct is more frequently visualized in the cat, the duct's size is smaller than the vessel, and the duct's position is more central within the pancreatic parenchyma. Doppler analysis, however, remains the best method of differentiating these structures.
In our experience, the identification of the pancreas was often assisted by recognition of its neighboring structures. For example, localization of the duodenum was useful in identification of the right lobe because of the close anatomi- cal association of these structures. Identification of vascular landmarks such as the portal vein and splenic vein also proved very useful in localizing the feline pancreas. The portal vein lies just dorsal to the left lobe and body of the pancreas and can be followed to the hepatic hilus. While scanning in the sagittal plane, the portal vein is easily iden- tified as a longitudinal vessel running parallel to, and im- mediately dorsal to the left pancreatic lobe. At the junction of the left pancreatic lobe with the pancreatic body, how- ever, the orientation of the portal vein changes from longi- tudinal to transverse while still scanning in the sagittal plane. The pancreatic body can be localized more precisely, by observing the transverse or cross-sectional orientation of the portal vein during sagittal scanning of the pancreatic body (Fig. 4). In some cats, visualization of a large splenic vein curving around the tip of the left pancreatic lobe can also serve as a very useful vascular landmark in identifica- tion of the pancreas (Fig. 9). The triangular window formed by the caudal edge of the stomach, the cranial aspect of the left kidney, and medially delineated by the spleen6 is useful in locating the splenic vein and the tip of the left lobe of the pancreas which courses ventral to it. The single, large splenic vein is formed by the convergence of the many splenic vein branches from the mesenteric border of the spleen.6 It follows the curvature of the stomach and can be traced to the portal vein.
A gastric lymph node was inconsistently observed in the cats of this study and has been reported to be present in- consistently in the dog and the cat.'2317,20 The number of

336 ETUE ET AL. 200 1
FIG. 9. Sagittal sonographic image of the left lobe of the pancreas and the splenic vein. The splenic vein (sp. vein) is a useful vascular landmark as it is located dorsal to the left lobe of the pancreas in the cat. Cursors outline the margins of the pancreas. ST = stomach.
gastric lymph nodes reported in the cat, ranges from 0 to 4.l2,l7 The gastric lymph node(s), when present, are located in the lesser omentum, close to the lesser curvature of the stomach. I 2 , l 7 They receive afferent lymphatic drainage from the stomach, liver, esophagus, diaphragm, and perito- neum. A single gastric lymph node was observed in 6 cats
during localization of the pancreatic body. By angling the transducer caudal to, and slightly lateral to the gastric lymph node, the pancreatic body could be visualized at the level where the portal vein crosses it.
At the outset of this study, the mural thickness measure- ments for the feline duodenum had not yet been established. Ultrasonographic changes reported in canine pancreati-
include increased duodenal wall thickness. It was important, therefore, to establish the normal duodenal mural thickness in the cat. The mean duodenal wall thickness of 2.8 mm in sagittal section and 3.0 mm in transverse section is slightly larger then the measurements reported in a recent study of 14, healthy, awake cats.I4
In conclusion, prior knowledge of the normal pancreatic dimension, echogenicity and relationship to adjacent ana- tomical structures is essential for an accurate evaluation of pancreatic disease. This study provides reference values for pancreatic thickness in the healthy cat, as well as the di- mensions of the pancreatic duct, duodenal wall, duodenal papilla, portal vein, and gastric lymph node. It is hoped that these data will be of value to clinicians investigating dis- eases of the feline pancreas.
tis6,9, I6
REFERENCES
I . Steiner JM, Williams DA. Feline exocrine pancreatic disorders: in- sufficiency, neoplasia, and uncommon conditions. Compend Contin Educ for the Pract Vet 1997;19:836-849.
2. Simpson KW, Shiroma JT, Biller DS, et al. Ante mortem diagnosis of pancreatitis in four cats. J Small Animal Practice 1994;3.5:93-99.
3. Williams K, Shiroma JT. Biller DS. Exocrine pancreatic disease. In: Ettinger. Textbook of Veterinary Internal Medicine, 4th ed. Saunders 199.5: 1372-1392.
4. Saunders HM, Pugh CR, Rhodes WH. Expanding applications of abdominal ultrasonography. J Am Anim Hosp Assoc 1992;28:369-374.
5. Miles K, Lattimer JC, Krause GF, Knapp DW, Sayles CE. The use of intraperitoneal fluid as a simple technique for enhancing sonographic visualization of the canine pancreas. Journal of Vet Radiol and Ultrasound 1988;29:258-263.
6. Saunders HM. Ultrasonography of the pancreas. In: Problems in Veterinary Medicine, I99 1;3:583-603.
7. Nyland TG, Mulvany MH, Stombeck DR. Ultrasonic features of experimentally induced, acute pancreatitis in dogs. Vet Radiol and Ultra- sound I983;24:260-266.
8. Murtaugh RH, Herring DS, Jacobs RM, DeHoff WD. Pancreatic ultrasonography in dogs with experimentally induced acute pancreatitis. Vet Radiol and Ultrasound 198.5;26:27-32.
9. Lamb CR, Simpson KW. Ultrasonographic findings in cholecysto- kinin-induced pancreatitis in dogs. Vet Radiol and Ultrasound, 1995;36: 139- 14.5.
10. Laflamme D. Development of a Body Condition Score System for Cats: A Clinical Tool. Feline Practice l997;25: 13-18,
11. Homco LD. Pancreas. In: Green RW. Small Animal Ultrasound. Philadelphia: Lippencott-Raven, 1996: 177-1 96.
12. Hudson LC, Hamilton WP. Atlas of feline anatomy for veterinar- ians, 1" ed. Philadelphia: WB Saunders, 1993:287.
13. Barone R. Anatomie Comparee des mammiferes domestique. Tome 3, splanchnologie 1" ed. Paris: Vigot. 1997.
14. Newell SM, Graham JP, Roberts GD. Ginn PE, Harrison JM. So- nography of the normal feline gastrointestinal tract. Vet Radiol and Ultra- sound 1999;40:4M3.
1.5. O'Brien TR. Pancreas. In: Radiographic diagnosis of abdominal disorders in the dog and cat. Philadelphia: WB Saunders, 1978:460-468.
16. Lamb CR. Recent developments in diagnostic imaging of the gas- trointestinal tract of the dog and cat-progress in gastroenterology. Vet Clin North Am (Small Anim Pract) 1999:307-342.
17. Crouch JE. Text-atlas of cat anatomy. Philadelphia: Lea and Fe- biger, 1969:339.
18. Grandage J. The pancreas. In: Slatter DH. Textbook of Small Ani- mal Surgery. Philadelphia: WB Saunders, 1985:828-853.
19. Nickel R, Schummer A, Seiferle E, Sack WO. The viscera of the domestic mammals. New York: Verlag Paul Parey, 1973:401.
20. Rogers KS, Ldndis M, Barton C. Canine and feline lymph nodes. part 1. anatomy and function. Compend Contin Educ for the Pract Vet 1993;15:397-409.