Embed Size (px)
Citation preview
Journal of Medical Ultrasound (2013) 21, 21e28
Available online at www.sciencedirect.com
journal homepage: www.jmu-onl ine.com
ORIGINAL ARTICLE
Ultrasound Appearances of DermatofibrosarcomaProtuberans
Ryan K.L. Lee 1*, James F. Griffith 1, Alex W.H. Ng 1,Fernand Mac-Moune Lai 2
1Department of Imaging and Interventional Radiology, Prince of Wales Hospital, Chinese University of Hong Kong, and2Department of Anatomical and Cellular Pathology, Prince of Wales Hospital, Chinese University of Hong Kong, Hong Kong
Received 17 July, 2012; accepted 25 September, 2012
KEY WORDSdermatofibrosarcomaprotuberans,
DFSP,pathology,ultrasound
* Correspondence to: Ryan Ka Lok Leof Hong Kong, Hong Kong.
E-mail address: leekalok2909@yah
0929-6441 ª 2013, Elsevier Taiwan LLhttp://dx.doi.org/10.1016/j.jmu.2013
To analyze the ultrasound appearances of dermatofibrosarcoma protuberans (DFSP) and corre-late these with pathologic findings. Nine tumors in eight patients were analyzed (one patienthaving two separate DFSP tumors). All ultrasound images were assessed and correlated withthe histologic findings. Most (7/9, or 78%) tumors were located in the subcutaneous region.The shape of the tumor was round in 67% (6/9) and ovoid in 33% (3/9) of cases. The marginwas poorly defined in one (11%) and well-defined or circumscribed in eight (89%) tumors. Allthe tumors showed a mildly lobulated border and had a heterogeneously hypoechoic matrix,often with rounded, ovoid, or occasionally linear discrete hypoechoic areas. Very small echo-genic foci (<0.5 mm), usually without an accompanying comet tail artifact, were seen withinthe tumor matrix of all the cases. Posterior enhancement was also a feature of all the tumors.Most (67%) tumors showed moderate vascularity on color Doppler imaging. This vascularitytended to be more profound peripherally rather than centrally, and tended to be more orga-nized rather than chaotic in distribution. Based on its quite characteristic ultrasound appear-ances, one should be able to either diagnose, or at least suggest, the likelihood of a DFSPtumor. In such circumstances, either percutaneous biopsy or en-bloc resection with wide mar-gins is recommended.ª 2013, Elsevier Taiwan LLC and the Chinese Taipei Society of Ultrasound in Medicine.Open access under CC BY-NC-ND license.
e, Department of Imaging and Interventional Radiology, Prince of Wales Hospital, Chinese University
oo.com.hk (R.K.L. Lee).
C and the Chinese Taipei Society of Ultrasound in Medicine..01.009
Open access under CC BY-NC-ND license.

22 R.K.L. Lee et al.
Introduction
Dermatofibrosarcoma protuberans (DFSP) is a low-gradespindle cell sarcoma accounting for about 6% of all softtissue sarcomas. It is, however, the most common pri-mary sarcoma to occur in the subcutaneous tissues [1]. Itwas originally described as a distinct clinicopathologicentity in 1924 by Darier and Ferrand [2], with the ter-minology being coined by Hoffman 1 year later [3]. DFSPis a mesenchymal tumor nearly always arising from thedermis and usually associated with typical clinical ap-pearances [1].
Clinically, DFSP starts as a small nodule that will growinto a medium-sized erythematous or bluish lesion pro-truding from the skin [1]. This nodule may eventually ul-cerate [1]. Imaging is performed in those clinical situationswhere the typical clinical appearances are not present, orwhere the clinician is either unaware of the typical clinicalappearances or is unclear as to the depth of invasion.
The magnetic resonance imaging (MRI) and computedtomography (CT) appearances of DFSP have been describedas nonspecific [4,5]. The sonographic appearances of non-breast DFSP have been described in one case report and onecase series [6,7]. The ultrasound features of breast DFSPhave also been specifically reported [6,7]. Overall, theappearances of breast DFSP are similar to those of DFSPtumors occurring outside the breast [6,7].
This study was undertaken to document in greater detailthe ultrasound appearances of DFSP lesions in eight pa-tients, particularly with a view to identifying any charac-teristic ultrasound appearances that would enablepreoperative recognition of this tumor.
Materials and methods
The pathology database at our institution was retro-spectively accessed to identify tumors with a pathologicdiagnosis of DFSP presenting between May 1999 and Octo-ber 2010. A total of 52 patients with histologically con-firmed DFSP were retrieved, of whom 13 (23%) hadundergone ultrasound prior to excision. The ultrasoundimages of the DFSP were available for review in eight ofthese 13 patients. The mean patient age of these eightpatients was 49 � 10.3 (standard deviation) years, range30e60 years, with a slight female predominance (female:-male Z 5:3). All had undergone both grayscale and colorDoppler ultrasound with one of four musculoskeletal radi-ologists (with 5e15 years’ musculoskeletal ultrasoundexperience), using either high-resolution 12e17 MHz lineartransducers for superficial lesions or moderate resolution(5 MHz) linear transducers for deeper lesions (SonolineElegra, Siemens, Issaquah, WA, USA; iU22, Philips, Bothell,WA, USA).
Two fellowship-trained musculoskeletal radiologists(with a musculoskeletal sonography experience of 5e15years) retrospectively reviewed, in consensus, the ultra-sound images of these DFSP tumors, noting the followingimaging features: the location (dermal, subcutaneous,intramuscular), shape (rounded, ovoid), margin (welldefined, ill defined), border (smooth, spiculated, lobu-lated), principal echogenicity (anechoic, hypoechoic,
isoechoic, or hyperechoic to subcutaneous fat), additionalechogenic areas (anechoic, hypoechoic, isoechoic, orhyperechoic to subcutaneous fat), central tiny echogenicfoci (absence or presence), posterior enhancement orshadowing, tumor rim (absence or presence), internal vas-cularity during color Doppler imaging (peripheral or cen-tral), and whether this vascularity was organized (i.e., withvessels dispersed at regular intervals) or chaotic (i.e. thevessels irregularly dispersed) [8]. The electronic medicalrecords were accessed to record the preimaging clinicaldiagnosis, biopsy findings, surgical findings, and clinicalrecurrence. The histology slides of both the biopsy andexcision specimens of the tumors under review wereretrieved and reassessed by a senior pathologist experi-enced in assessing soft tissue tumors.
Results
Imaging data
A total of nine tumors were analyzed (one patient hadtwo separate large tumors of the knee region). The pre-ultrasound clinical diagnoses were DFSP (2/9, 22%), softtissue sarcoma (5/9, 56%), hemangioma (1/9, 11%), andbreast carcinoma (1/9, 11%). Ultrasound was performedon all nine tumors. Additional MRI, CT, and positron-emission tomography CT (PET-CT) studies were performedin Case 1, Case 3, and Case 8, respectively, for presurgicalassessment.
Ultrasound appearances
For the nine tumors studied, the maximum dimensionranged from 1.8 to 11.0 cm, with a mean of 6.7 cm. Most[78% (7/9)] tumors were located in the subcutaneous tis-sues, with one located intermuscularly (between thetibialis anterior and extensor digitorum longus muscles) andone located just deep to the investing fascia of the upperleg. Most tumors were mainly round [67% (6/9)] in shaperather than ovoid [33% (3/9)]. One (11%) tumor showeda poorly defined margin, while the remainder [89% (8/9)]were well-marginated or circumscribed. All tumors showeda mildly lobulated border, while one tumor (11%) hada focal appendage-like elongation.
All the tumors had a heterogeneously hypoechoic ma-trix (compared to subcutaneous fat), often containinga rounded, ovoid, or occasionally linear more discretehypoechoic area or areas. Very small echogenic foci(<0.5 mm), usually without an accompanying comet tailartifact, were seen within the tumor matrix of all thecases. Posterior enhancement was also a feature seen inall the tumors.
Most [67% (6/9)] tumors showed moderate vascularityon color Doppler imaging. This vascularity tended to bemore profound peripherally than centrally, and tended tobe more organized rather than chaotic in distribution [8].Ultrasound-guided core biopsies using a 16 G Tru-Cutneedle and a coaxial system were performed on all tumors.These biopsies revealed features consistent with DFSP inall cases.
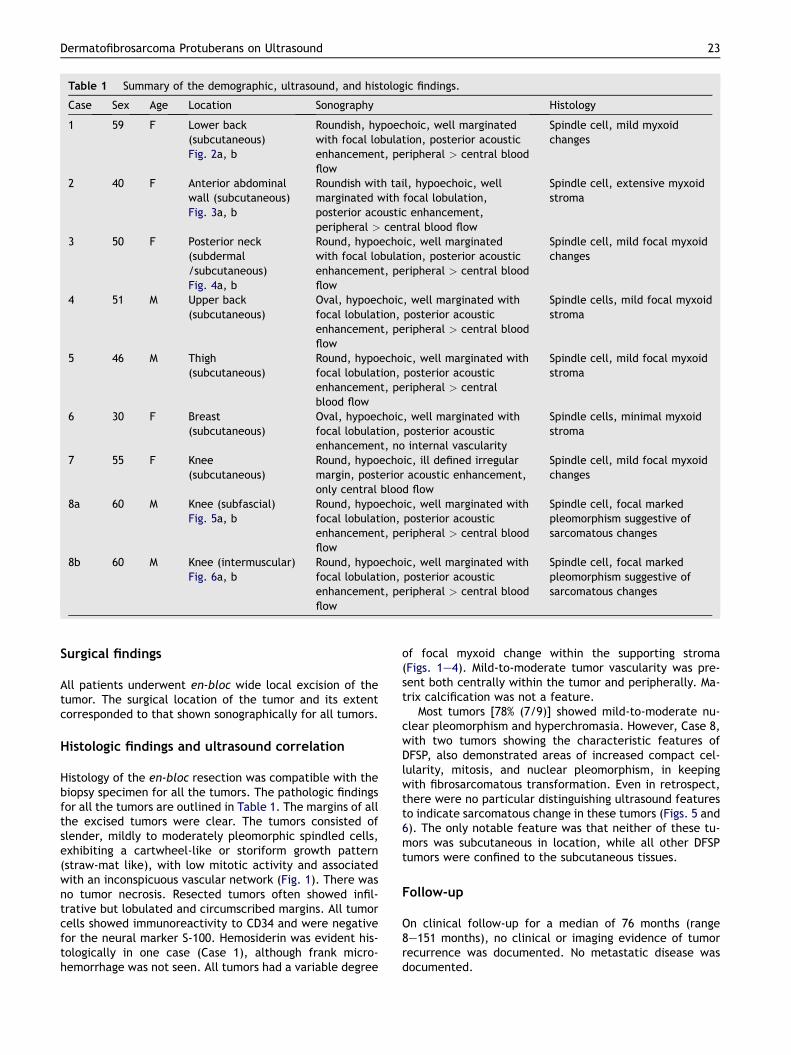
Table 1 Summary of the demographic, ultrasound, and histologic findings.
Case Sex Age Location Sonography Histology
1 59 F Lower back(subcutaneous)Fig. 2a, b
Roundish, hypoechoic, well marginatedwith focal lobulation, posterior acousticenhancement, peripheral > central bloodflow
Spindle cell, mild myxoidchanges
2 40 F Anterior abdominalwall (subcutaneous)Fig. 3a, b
Roundish with tail, hypoechoic, wellmarginated with focal lobulation,posterior acoustic enhancement,peripheral > central blood flow
Spindle cell, extensive myxoidstroma
3 50 F Posterior neck(subdermal/subcutaneous)Fig. 4a, b
Round, hypoechoic, well marginatedwith focal lobulation, posterior acousticenhancement, peripheral > central bloodflow
Spindle cell, mild focal myxoidchanges
4 51 M Upper back(subcutaneous)
Oval, hypoechoic, well marginated withfocal lobulation, posterior acousticenhancement, peripheral > central bloodflow
Spindle cells, mild focal myxoidstroma
5 46 M Thigh(subcutaneous)
Round, hypoechoic, well marginated withfocal lobulation, posterior acousticenhancement, peripheral > centralblood flow
Spindle cell, mild focal myxoidstroma
6 30 F Breast(subcutaneous)
Oval, hypoechoic, well marginated withfocal lobulation, posterior acousticenhancement, no internal vascularity
Spindle cells, minimal myxoidstroma
7 55 F Knee(subcutaneous)
Round, hypoechoic, ill defined irregularmargin, posterior acoustic enhancement,only central blood flow
Spindle cell, mild focal myxoidchanges
8a 60 M Knee (subfascial)Fig. 5a, b
Round, hypoechoic, well marginated withfocal lobulation, posterior acousticenhancement, peripheral > central bloodflow
Spindle cell, focal markedpleomorphism suggestive ofsarcomatous changes
8b 60 M Knee (intermuscular)Fig. 6a, b
Round, hypoechoic, well marginated withfocal lobulation, posterior acousticenhancement, peripheral > central bloodflow
Spindle cell, focal markedpleomorphism suggestive ofsarcomatous changes
Dermatofibrosarcoma Protuberans on Ultrasound 23
Surgical findings
All patients underwent en-bloc wide local excision of thetumor. The surgical location of the tumor and its extentcorresponded to that shown sonographically for all tumors.
Histologic findings and ultrasound correlation
Histology of the en-bloc resection was compatible with thebiopsy specimen for all the tumors. The pathologic findingsfor all the tumors are outlined in Table 1. The margins of allthe excised tumors were clear. The tumors consisted ofslender, mildly to moderately pleomorphic spindled cells,exhibiting a cartwheel-like or storiform growth pattern(straw-mat like), with low mitotic activity and associatedwith an inconspicuous vascular network (Fig. 1). There wasno tumor necrosis. Resected tumors often showed infil-trative but lobulated and circumscribed margins. All tumorcells showed immunoreactivity to CD34 and were negativefor the neural marker S-100. Hemosiderin was evident his-tologically in one case (Case 1), although frank micro-hemorrhage was not seen. All tumors had a variable degree
of focal myxoid change within the supporting stroma(Figs. 1e4). Mild-to-moderate tumor vascularity was pre-sent both centrally within the tumor and peripherally. Ma-trix calcification was not a feature.
Most tumors [78% (7/9)] showed mild-to-moderate nu-clear pleomorphism and hyperchromasia. However, Case 8,with two tumors showing the characteristic features ofDFSP, also demonstrated areas of increased compact cel-lularity, mitosis, and nuclear pleomorphism, in keepingwith fibrosarcomatous transformation. Even in retrospect,there were no particular distinguishing ultrasound featuresto indicate sarcomatous change in these tumors (Figs. 5 and6). The only notable feature was that neither of these tu-mors was subcutaneous in location, while all other DFSPtumors were confined to the subcutaneous tissues.
Follow-up
On clinical follow-up for a median of 76 months (range8e151 months), no clinical or imaging evidence of tumorrecurrence was documented. No metastatic disease wasdocumented.
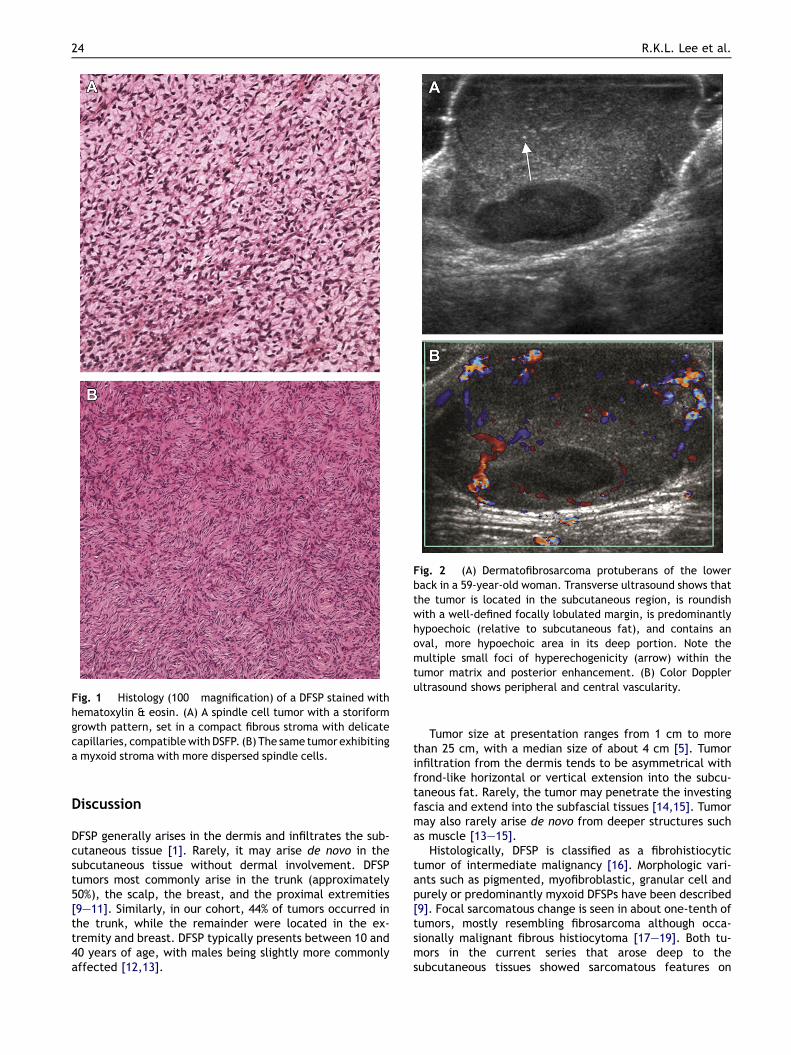
Fig. 1 Histology (100� magnification) of a DFSP stained withhematoxylin & eosin. (A) A spindle cell tumor with a storiformgrowth pattern, set in a compact fibrous stroma with delicatecapillaries, compatiblewithDSFP. (B) The same tumor exhibitinga myxoid stroma with more dispersed spindle cells.
Fig. 2 (A) Dermatofibrosarcoma protuberans of the lowerback in a 59-year-old woman. Transverse ultrasound shows thatthe tumor is located in the subcutaneous region, is roundishwith a well-defined focally lobulated margin, is predominantlyhypoechoic (relative to subcutaneous fat), and contains anoval, more hypoechoic area in its deep portion. Note themultiple small foci of hyperechogenicity (arrow) within thetumor matrix and posterior enhancement. (B) Color Dopplerultrasound shows peripheral and central vascularity.
24 R.K.L. Lee et al.
Discussion
DFSP generally arises in the dermis and infiltrates the sub-cutaneous tissue [1]. Rarely, it may arise de novo in thesubcutaneous tissue without dermal involvement. DFSPtumors most commonly arise in the trunk (approximately50%), the scalp, the breast, and the proximal extremities[9e11]. Similarly, in our cohort, 44% of tumors occurred inthe trunk, while the remainder were located in the ex-tremity and breast. DFSP typically presents between 10 and40 years of age, with males being slightly more commonlyaffected [12,13].
Tumor size at presentation ranges from 1 cm to morethan 25 cm, with a median size of about 4 cm [5]. Tumorinfiltration from the dermis tends to be asymmetrical withfrond-like horizontal or vertical extension into the subcu-taneous fat. Rarely, the tumor may penetrate the investingfascia and extend into the subfascial tissues [14,15]. Tumormay also rarely arise de novo from deeper structures suchas muscle [13e15].
Histologically, DFSP is classified as a fibrohistiocytictumor of intermediate malignancy [16]. Morphologic vari-ants such as pigmented, myofibroblastic, granular cell andpurely or predominantly myxoid DFSPs have been described[9]. Focal sarcomatous change is seen in about one-tenth oftumors, mostly resembling fibrosarcoma although occa-sionally malignant fibrous histiocytoma [17e19]. Both tu-mors in the current series that arose deep to thesubcutaneous tissues showed sarcomatous features on
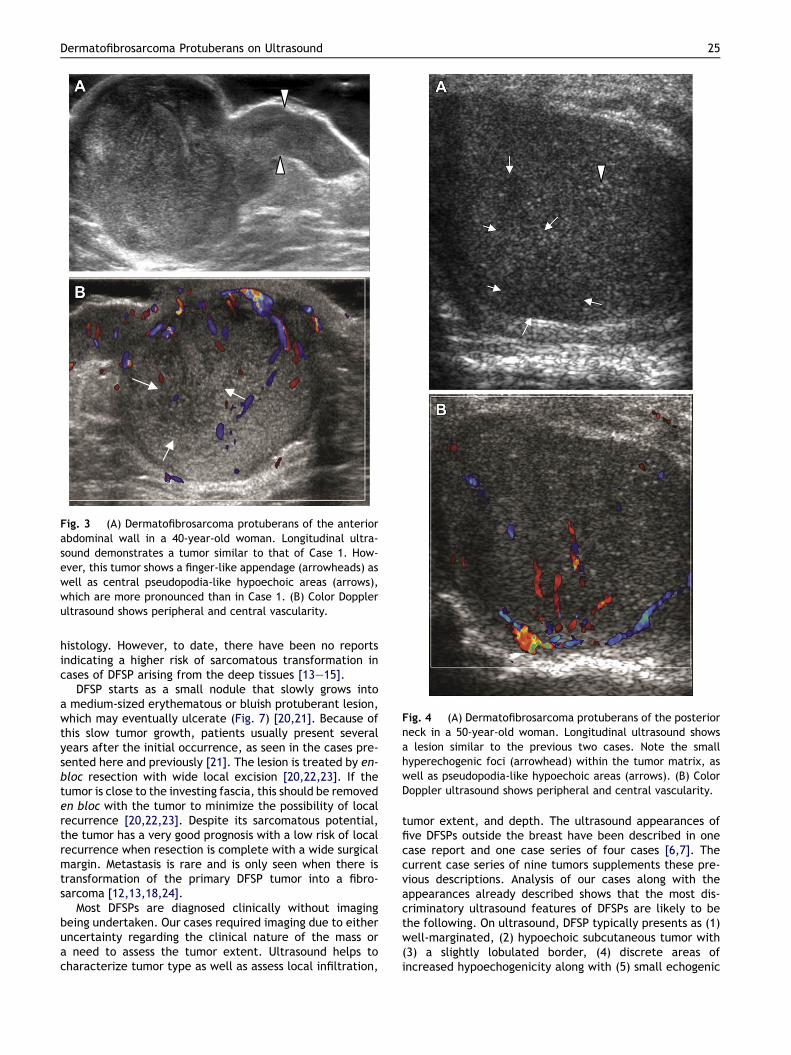
Fig. 3 (A) Dermatofibrosarcoma protuberans of the anteriorabdominal wall in a 40-year-old woman. Longitudinal ultra-sound demonstrates a tumor similar to that of Case 1. How-ever, this tumor shows a finger-like appendage (arrowheads) aswell as central pseudopodia-like hypoechoic areas (arrows),which are more pronounced than in Case 1. (B) Color Dopplerultrasound shows peripheral and central vascularity.
Fig. 4 (A) Dermatofibrosarcoma protuberans of the posteriorneck in a 50-year-old woman. Longitudinal ultrasound showsa lesion similar to the previous two cases. Note the smallhyperechogenic foci (arrowhead) within the tumor matrix, aswell as pseudopodia-like hypoechoic areas (arrows). (B) ColorDoppler ultrasound shows peripheral and central vascularity.
Dermatofibrosarcoma Protuberans on Ultrasound 25
histology. However, to date, there have been no reportsindicating a higher risk of sarcomatous transformation incases of DFSP arising from the deep tissues [13e15].
DFSP starts as a small nodule that slowly grows intoa medium-sized erythematous or bluish protuberant lesion,which may eventually ulcerate (Fig. 7) [20,21]. Because ofthis slow tumor growth, patients usually present severalyears after the initial occurrence, as seen in the cases pre-sented here and previously [21]. The lesion is treated by en-bloc resection with wide local excision [20,22,23]. If thetumor is close to the investing fascia, this should be removeden bloc with the tumor to minimize the possibility of localrecurrence [20,22,23]. Despite its sarcomatous potential,the tumor has a very good prognosis with a low risk of localrecurrence when resection is complete with a wide surgicalmargin. Metastasis is rare and is only seen when there istransformation of the primary DFSP tumor into a fibro-sarcoma [12,13,18,24].
Most DFSPs are diagnosed clinically without imagingbeing undertaken. Our cases required imaging due to eitheruncertainty regarding the clinical nature of the mass ora need to assess the tumor extent. Ultrasound helps tocharacterize tumor type as well as assess local infiltration,
tumor extent, and depth. The ultrasound appearances offive DFSPs outside the breast have been described in onecase report and one case series of four cases [6,7]. Thecurrent case series of nine tumors supplements these pre-vious descriptions. Analysis of our cases along with theappearances already described shows that the most dis-criminatory ultrasound features of DFSPs are likely to bethe following. On ultrasound, DFSP typically presents as (1)well-marginated, (2) hypoechoic subcutaneous tumor with(3) a slightly lobulated border, (4) discrete areas ofincreased hypoechogenicity along with (5) small echogenic
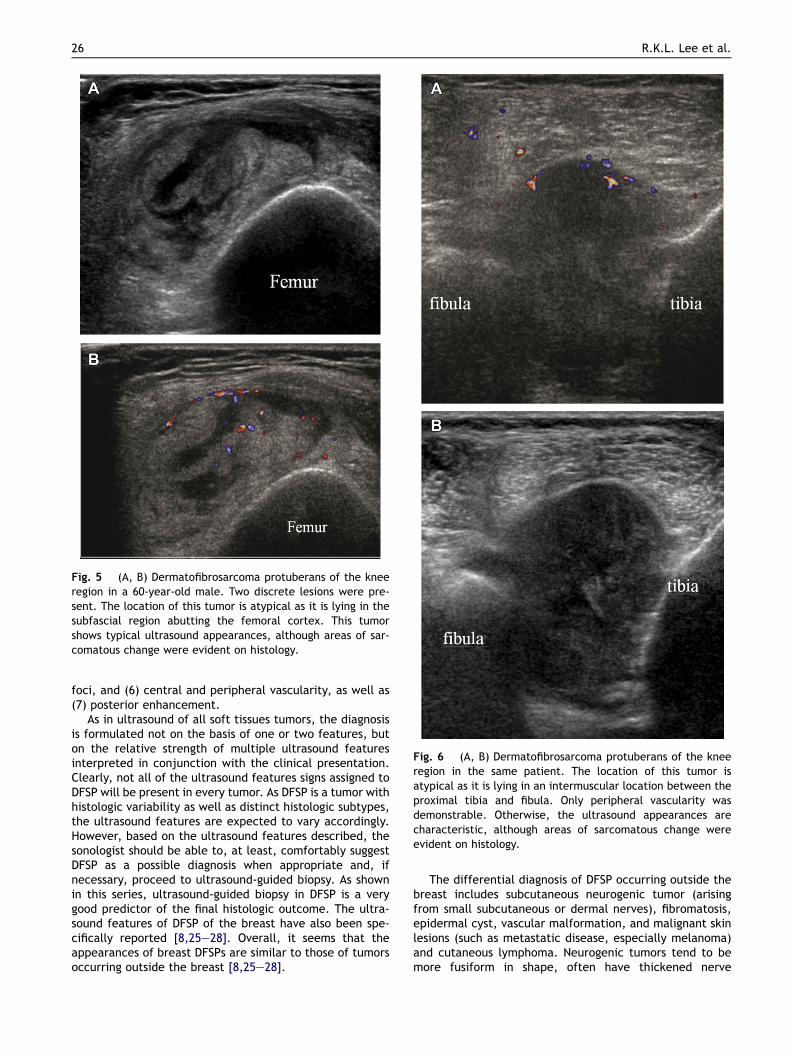
Fig. 5 (A, B) Dermatofibrosarcoma protuberans of the kneeregion in a 60-year-old male. Two discrete lesions were pre-sent. The location of this tumor is atypical as it is lying in thesubfascial region abutting the femoral cortex. This tumorshows typical ultrasound appearances, although areas of sar-comatous change were evident on histology.
Fig. 6 (A, B) Dermatofibrosarcoma protuberans of the kneeregion in the same patient. The location of this tumor isatypical as it is lying in an intermuscular location between theproximal tibia and fibula. Only peripheral vascularity wasdemonstrable. Otherwise, the ultrasound appearances arecharacteristic, although areas of sarcomatous change wereevident on histology.
26 R.K.L. Lee et al.
foci, and (6) central and peripheral vascularity, as well as(7) posterior enhancement.
As in ultrasound of all soft tissues tumors, the diagnosisis formulated not on the basis of one or two features, buton the relative strength of multiple ultrasound featuresinterpreted in conjunction with the clinical presentation.Clearly, not all of the ultrasound features signs assigned toDFSP will be present in every tumor. As DFSP is a tumor withhistologic variability as well as distinct histologic subtypes,the ultrasound features are expected to vary accordingly.However, based on the ultrasound features described, thesonologist should be able to, at least, comfortably suggestDFSP as a possible diagnosis when appropriate and, ifnecessary, proceed to ultrasound-guided biopsy. As shownin this series, ultrasound-guided biopsy in DFSP is a verygood predictor of the final histologic outcome. The ultra-sound features of DFSP of the breast have also been spe-cifically reported [8,25e28]. Overall, it seems that theappearances of breast DFSPs are similar to those of tumorsoccurring outside the breast [8,25e28].
The differential diagnosis of DFSP occurring outside thebreast includes subcutaneous neurogenic tumor (arisingfrom small subcutaneous or dermal nerves), fibromatosis,epidermal cyst, vascular malformation, and malignant skinlesions (such as metastatic disease, especially melanoma)and cutaneous lymphoma. Neurogenic tumors tend to bemore fusiform in shape, often have thickened nerve

Fig. 7 Typical clinical appearance of the dermatofi-brosarcoma protuberans seen in Case 1. There is a large, su-perficial, fleshy-colored mass protruding from the skin of theposterior lumbar region. The majority of tumors in this seriesdid not have this typical clinical appearance.
Dermatofibrosarcoma Protuberans on Ultrasound 27
segments immediately proximal or distal to the tumor, andhave a fairly characteristic echopattern and vascularity [29].Fibromatosis is usually less well defined, more infiltrative innature, and less vascular [30]. The small hyperechoic foci ofDFSP may mimic the “internal floating echogenicity” ofepidermal cysts, although the presence of internal vascu-larity in DFSPs helps to differentiate these two conditions[31]. In addition, the small echogenic foci in DFSPs are fixedrather than mobile as occasionally seen in epidermal cysts.Vascular malformations typically comprise numerous vas-cular channels interspersed with variable echogenic stroma,calcified phleboliths, and moderate compressibility. Theseappearances set them apart from those of DFSP. Malignantskin lesions such as metastasis and cutaneous lymphomawould be more infiltrative in appearance than DFSPs, butsometimes these can only be differentiated by biopsy. Thus,is important to consider DFSP as a differential diagnosis priorto surgery since wide local excision is necessary for DSFP inorder to avoid local recurrence [1].
In most of the cases presented, a clinical diagnosis ofDFSP was not made at the time of the ultrasound request,nor was this diagnosis reported as a possibility after ul-trasound examination. As these lesions tend to be small,superficial, and slow growing, sarcomatous lesion are usu-ally considered. All cases underwent percutaneous biopsy,allowing a correct preoperative diagnosis. The quite char-acteristic ultrasound appearances described here mayallow a preoperative diagnosis of this tumor to be made, orat least suggested, which would encourage appropriate en-bloc surgical resection with wide margins [6e8].
The CT and MRI appearances of DFSP are nonspecific,with cross-sectional imaging being used to determine thedeeper extension of larger lesions [4,5,12,13,32]. Thetumor is usually well defined with a distinct lobular ornodular architecture on CT or MRI scanning [4,5,12,13]. OnCT imaging, tumor attenuation is equal to or slightly higherthan that of skeletal muscle [4,13] with no calcification andmoderate contrast enhancement [4,5,12,13]. Central cysticcomponents (either myxoid degeneration, necrotic, or
hemorrhagic) are uncommon features [4,12]. PET imagingof DFSP is mainly for staging or assessing suspicious localrecurrence with DFSP. DFSP shows variable standardizeduptake value readings, possibly related to the presence anddegree of fibrosarcomatous change [33]. Although all casesof DFSP in the current series revealed areas of myxoiddegeneration histologically, this is reported as being aninfrequent feature on CT or MRI [4,13]. In contrast, areasconsistent with myxoid degeneration were apparent onmost ultrasound examinations in this series, clear testi-mony to the superior resolution of high-frequency ultra-sound [34].
The study had several limitations. First, as this is a ret-rospective study, we relied on the sonologists’ skill to imageand report all pertinent ultrasound findings. Second, onlya relatively small number of tumors could be included asthis is an uncommon tumor, which is not always referred forimaging. Third, the referral pattern may have led to se-lection bias in that tumors with atypical clinical features orthose with suspected deep extension may have been pre-ferentially referred for imaging.
In conclusion, this analysis of nine cases of DFSP providesquite characteristic ultrasound appearances. On sono-graphic examination, as well as accurately determiningtumor extent, one should be able to either diagnose, or atleast suggest the likelihood of, this tumor based on thesecharacteristic ultrasound appearances. If the ultrasoundappearances suggest DFSP, either percutaneous biopsy oren-bloc resection with wide margins is recommended.
References
[1] Beaman FD, Kransdorf MJ, Andrews TR, et al. Superficial soft-tissue masses: analysis, diagnosis, and differential consider-ations. Radiographics 2007;27(2):509e23.
[2] Darier S, Ferrand M. Dermatofibrosacromes progressifs etricidivantes on fibrosarcomes de la peau. Ann DermatolVenereol 1924;5:54e6.
[3] Hoffman E. Liber das Knollentrichencle fibrokom der hout.Acta Derm Venereol Suppl (Stockh) 1925;32.
[4] Daly BD, Currie AR, Choi PC. Case report: computed tomo-graphic and scintigraphic appearances of dermatofi-brosarcoma protuberans. Clin Radiol 1993;48(1):63e5.
[5] Torreggiani WC, Al-Ismail K, Munk PL, et al. Dermatofi-brosarcoma protuberans: MR imaging features. AJR Am JRoentgenol 2002;178(4):989e93.
[6] Shin YR, Kim JY, Sung MS, et al. Sonographic findings of der-matofibrosarcoma protuberans with pathologic correlation. JUltrasound Med 2008;27(2):269e74.
[7] Kau T, Lesnik G, Arnold G, et al. Sonography of dermatofi-brosarcoma protuberans of the groin. J Clin Ultrasound 2008;36(8):520e2.
[8] Griffith JF, Chan DP, Kumta SM, et al. Does Doppler analysis ofmusculoskeletal soft-tissue tumours help predict tumour ma-lignancy? Clin Radiol 2004;59:369e75.
[9] Mentzel T, Scharer L, Kazakov DV, et al. Myxoid dermatofi-brosarcoma protuberans: clinicopathologic, immunohis-tochemical, and molecular analysis of eight cases. Am JDermatopathol 2007;29(5):443e8.
[10] Oliveira-Soares R, Viana I, Vale E, et al. Dermatofibrosarcomaprotuberans: a clinicopathological study of 20 cases. J EurAcad Dermatol Venereol 2002;16(5):441e6.
[11] Bague S, Folpe AL. Dermatofibrosarcoma protuberans pre-senting as a subcutaneous mass: a clinicopathological study of
28 R.K.L. Lee et al.
15 cases with exclusive or near-exclusive subcutaneousinvolvement. Am J Dermatopathol 2008;30(4):327e32.
[12] Blacksin MF, Ha DH, Hameed M, et al. Superficial soft-tissuemasses of the extremities. Radiographics 2006;26(5):1289e304.
[13] Kransdorf MJ, Meis-Kindblom JM. Dermatofibrosarcoma pro-tuberans: radiologic appearance. AJR Am J Roentgenol 1994;163(2):391e4.
[14] De Pasquale R, Dinotta F, Scuderi L, et al. Dermatofi-brosarcoma protuberans. G Ital Dermatol Venereol 2009;144(2):199e203.
[15] Hafner HM, Moehrle M, Eder S, et al. 3D-histological evalua-tion of surgery in dermatofibrosarcoma protuberans and ma-lignant fibrous histiocytoma: differences in growth patternsand outcome. Eur J Surg Oncol 2008;34(6):680e6.
[16] Weiss SW. Histological typing of soft tissue tumours. In:Weiss SW, editor. World Health Organization, Internationalhistological classification of tumours. 2nd ed. Berlin: Springer-Verlag; 1994.
[17] Goldblum JR, Reith JD, Weiss SW. Sarcomas arising in derma-tofibrosarcoma protuberans: a reappraisal of biologic behaviorin eighteen cases treated by wide local excision with extendedclinical follow up. Am J Surg Pathol 2000;24(8):1125e30.
[18] Bowne WB, Antonescu CR, Leung DH, et al. Dermatofi-brosarcoma protuberans: a clinicopathologic analysis of pa-tients treated and followed at a single institution. Cancer2000;88(12):2711e20.
[19] Tan AW, Tan SH. Dermatofibrosarcoma protuberans: a clin-icopathological analysis of 10 cases in Asians. Australas JDermatol 2004;45(1):29e33.
[20] Chan AYK, Luk NM, Lee KC. Dermatofibrosarcoma protuber-ans: a report of 36 cases in Hong Kong and Review of the lit-erature. Hong Kong J Dermatol Venereol 2009;17:6e11.
[21] Korkolis DP, Liapakis IE, Vassilopoulos PP. Dermatofi-brosarcoma protuberans: clinicopathological aspects of anunusual cutaneous tumor. Anticancer Res 2007;27(3B):1631e4.
[22] Mendenhall WM, Zlotecki RA, Scarborough MT. Dermatofi-brosarcoma protuberans. Cancer 2004;101(11):2503e8.
[23] Meguerditchian AN, Wang J, Lema B, et al. Wide excision orMohs micrographic surgery for the treatment of primary der-matofibrosarcoma protuberans. Am J Clin Oncol 2010;33:300e3.
[24] Erdem O, Wyatt AJ, Lin E, et al. Dermatofibrosarcoma pro-tuberans treated with wide local excision and followed ata cancer hospital: prognostic significance of clinicopathologicvariables. Am J Dermatopathol 2012;34:24e34.
[25] Liu SZ, Ho TL, Hsu SM, et al. Imaging of dermatofibrosarcomaprotuberans of breast. Breast J 2010;16(5):541e3.
[26] Lin JY, Sheen-Chen SM, Hsu W, et al. Dermatofibrosarcomaprotuberans of the breast. Tumori 2008;94(6):861e3.
[27] Djilas-Ivanovic D, Prvulovic N, Bogdanovic-Stojanovic D, et al.Dermatofibrosarcoma protuberans of the breast: mammo-graphic, ultrasound, MRI and MRS features. Arch GynecolObstet 2009;280(5):827e30.
[28] Parajuly SS, Peng YL. Sonography of dermatofibrosarcomaprotuberans in the skin over breast. J Med Ultrasound 2010;18(3):130e5.
[29] Gruber H, Glodny B, Bendix N, et al. High-resolution ultra-sound of peripheral neurogenic tumors. Eur Radiol 2007;17(11):2880e8.
[30] Haun DW, Cho JC, Kettner NW. Symptomatic plantar fibromawith a unique sonographic appearance. J Clin Ultrasound2011;40:222e46.
[31] Huang CC, Ko SF, Huang HY, et al. Epidermal cysts in the su-perficial soft tissue: sonographic features with an emphasis onthe pseudotestis pattern. J Ultrasound Med 2011;30(1):11e7.
[32] De Schepper AML, De Beuckeleer J, Vandevenne J, et al.Magnetic resonance imaging of soft tissue tumors. Eur Radiol2000;10:213e22.
[33] Basu S, Baghel NS. Recurrence of dermatofibrosarcoma pro-tuberans in post-surgical scar detected by 18F-FDG-PET im-aging. Hell J Nucl Med 2009;12(1):68.
[34] Chiou HJ, Chou YH, Chiou SY, et al. High-resolution ultraso-nography of primary peripheral soft tissue lymphoma. J Ul-trasound Med 2005;24:77e86.