Embed Size (px)
DESCRIPTION
Ultrasound-Guided Shoulder Injections in the Treatment of Subacromial BursitisChen, MaxJ.L>MD; Lew, Henry L..MD,PhD; Hsu, Tsz-Ching MD,PhD;Tsai, Wen-ChungMD,PhD; Lin, Wei-ChingMD; Tang, SimonF.T MD; Lee, Ya-Chen MD; Hsu, Rex C.H.MD; Chen, Carl P.C.MD
Citation preview
AMERICAN JOURNAL OF PHYSICAL MEDICINE &REHABILITATION :
JANUARY 2006-VOLUME 85-ISSUE 1-PP31-35RESEARCH ARTICLE: INJECTIONS
ULTRASOUND-GUIDED SHOULDER INJECTIONS IN THE TREATMENT OF SUBACROMIAL BURSITIS
C H E N , M A X J . L > M D ; L E W , H E N RY L . . M D , P H D ; H S U , T S Z - C H I N G M D , P H D ; T S A I , W E N -C H U N G M D , P H D ; L I N , W E I - C H I N G M D ; TA N G , S I M O N F. T M D ; L E E , YA - C H E N M D ; H S U , R E X C . H . M D ; C H E N , C A R L P. C . M D
BACKGROUND
Subacromial bursitis is
The inflamed subacromial bursa
• The clinical picture is charaterized by
- anterior shoulder pain
- restriction of the range of motion of the
shoulder
• Develops in athletes who throw
THE OBJECTIVE
To investigate the treatment effectiveness between ultrasound-guided and blind injection technique in the treatment of subacromial bursitis
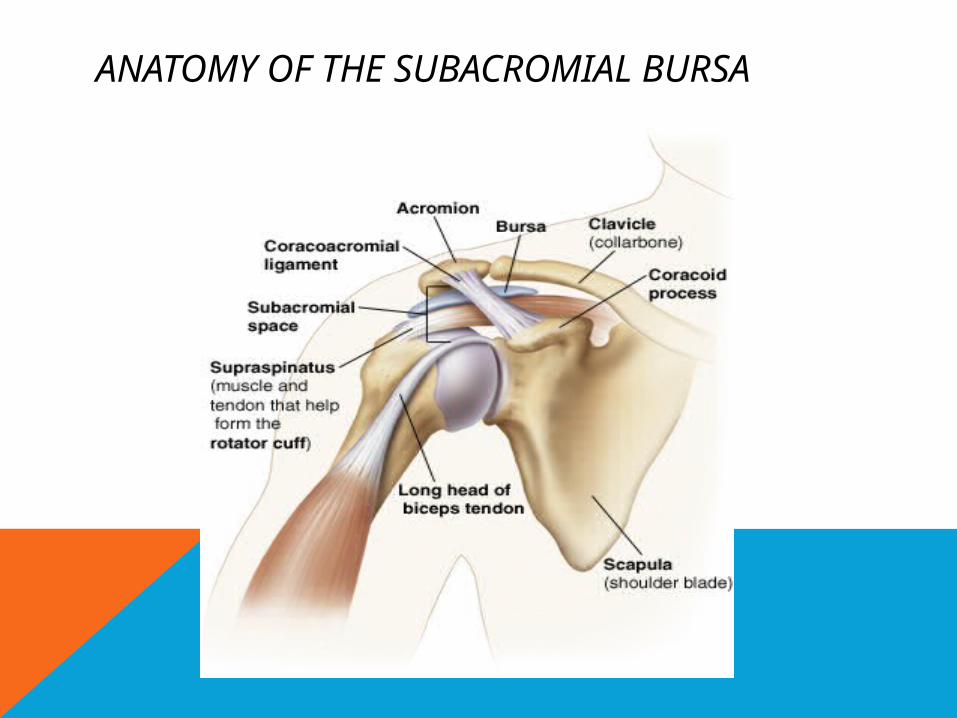
ANATOMY OF THE SUBACROMIAL BURSA
• The diagnosis of subacromial bursitis :
1. Direct palpation over the subacromial
bursa
2. Subacromial arthrography and magnetic
resonance imaging (MRI)
3. Ultrasound
• The treatment is:
- Rest, icing, anti-inflammatory medications
- In refractory patients---local injection of a
steroid into the bursa maybe necessary
In this study :
To investigate the treatment effectiveness between ultrasound-guided and blind injection techniques in the treatment of subacromial bursitis
METHODE
A total of 40 patients with sonographic confirmation of subacromial bursitis
The age from 30 - 66 yrs (average 53 yrs)
The duration was 2-10 mo
The ratio of men –women was 2:1
Px divided into 2 group : 20 px in each group
The inclusion criteria were:
- History of shoulder pain > 1 mo
- Shoulder pain that could be elicited during
abduction maneuvers
- Shoulder ROM limitation & the existence
of a painful are synd.
• The excluded criteria were :
Px with capsular lesions of the shoulder
All subjects signed informed consent
The LOGIQ 9 (General Electronic Company, Milwaukee, WI) was the ultrasound machine used for ultrasonographic examinations. The 10 L probe, 4-10 MHz (General Electronic Company, Milwaukee, WI) was used to assess the shoulder.
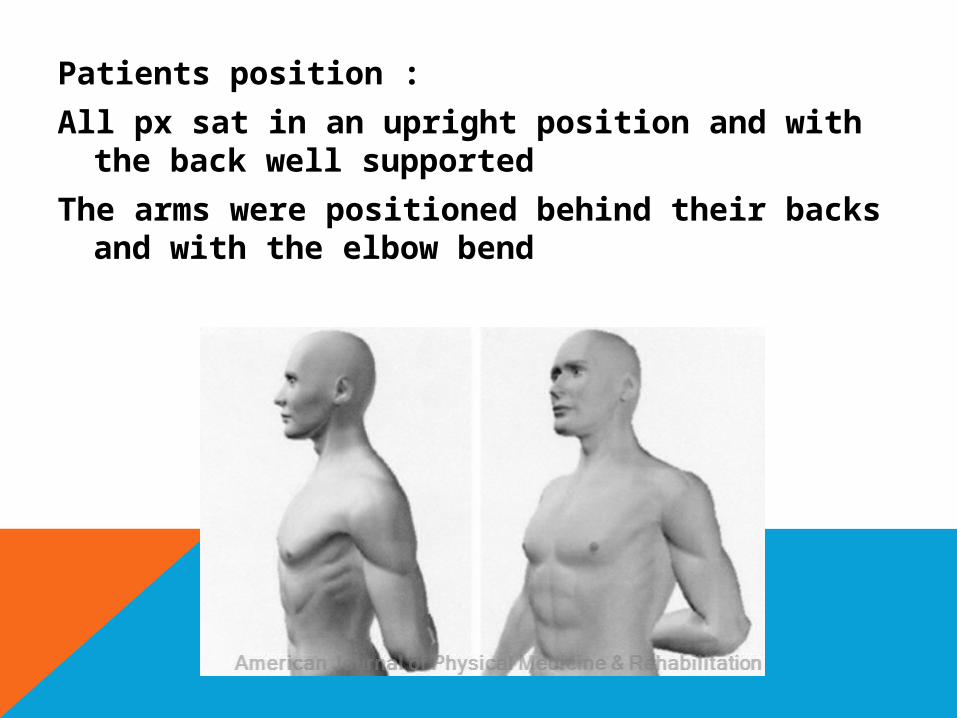
Patients position :
All px sat in an upright position and with the back well supported
The arms were positioned behind their backs and with the elbow bend
Ultrasonographic position ;
• The sonogram coracoacromial window was obtained by placing the probe on the counter of the shoulder lateral and parallel to axis of the underlying supraspinatus tendon
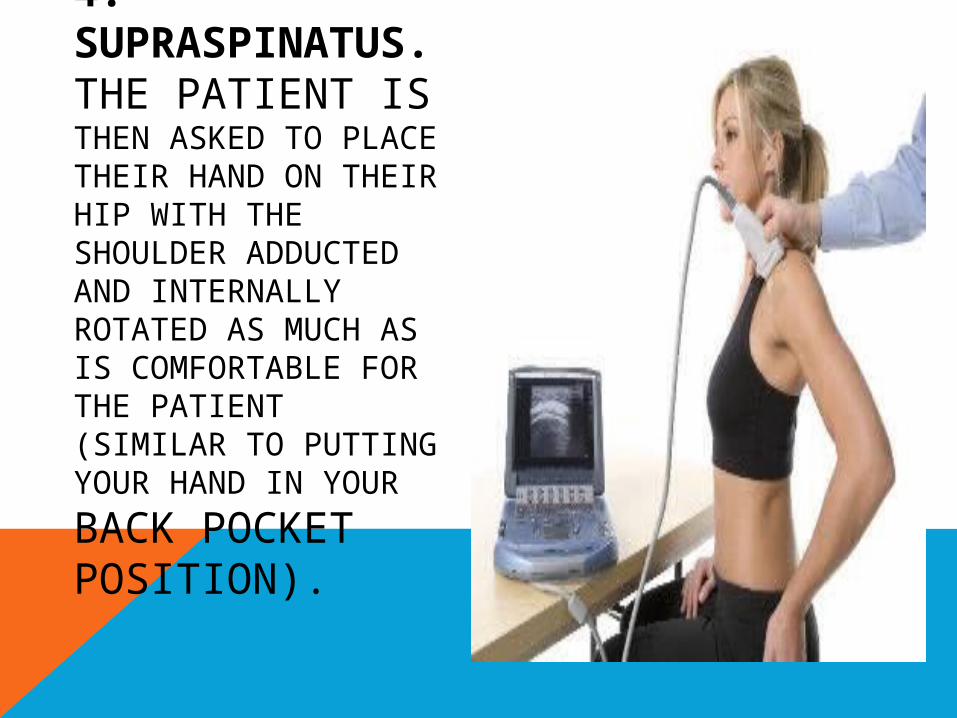
4. SUPRASPINATUS.THE PATIENT IS THEN ASKED TO PLACE THEIR HAND ON THEIR HIP WITH THE SHOULDER ADDUCTED AND INTERNALLY ROTATED AS MUCH AS IS COMFORTABLE FOR THE PATIENT (SIMILAR TO PUTTING YOUR
HAND IN YOUR BACK POCKET POSITION).
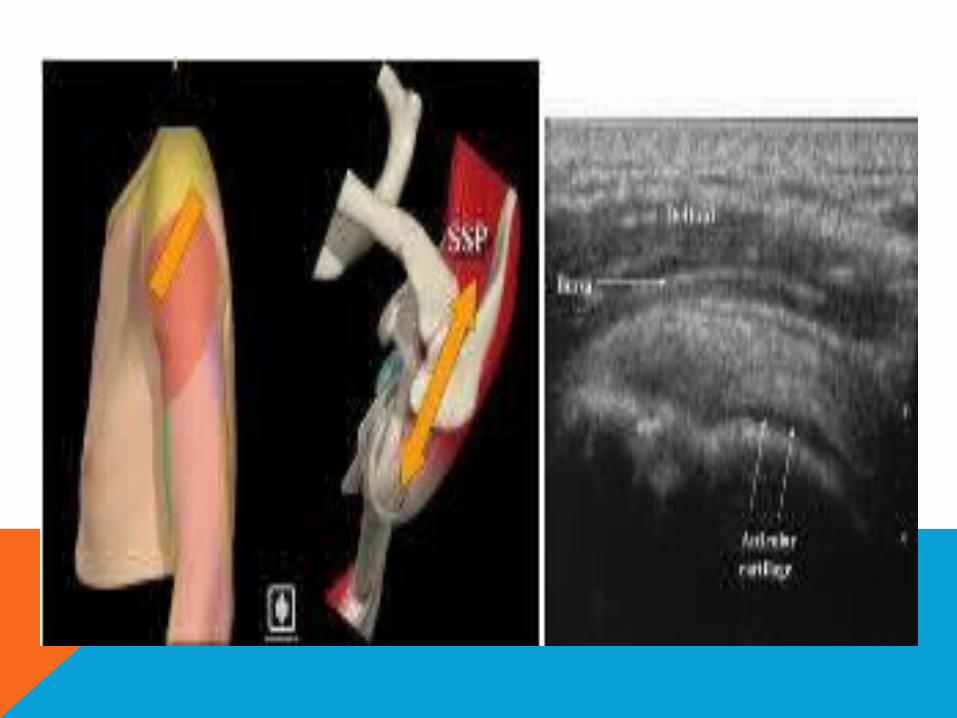
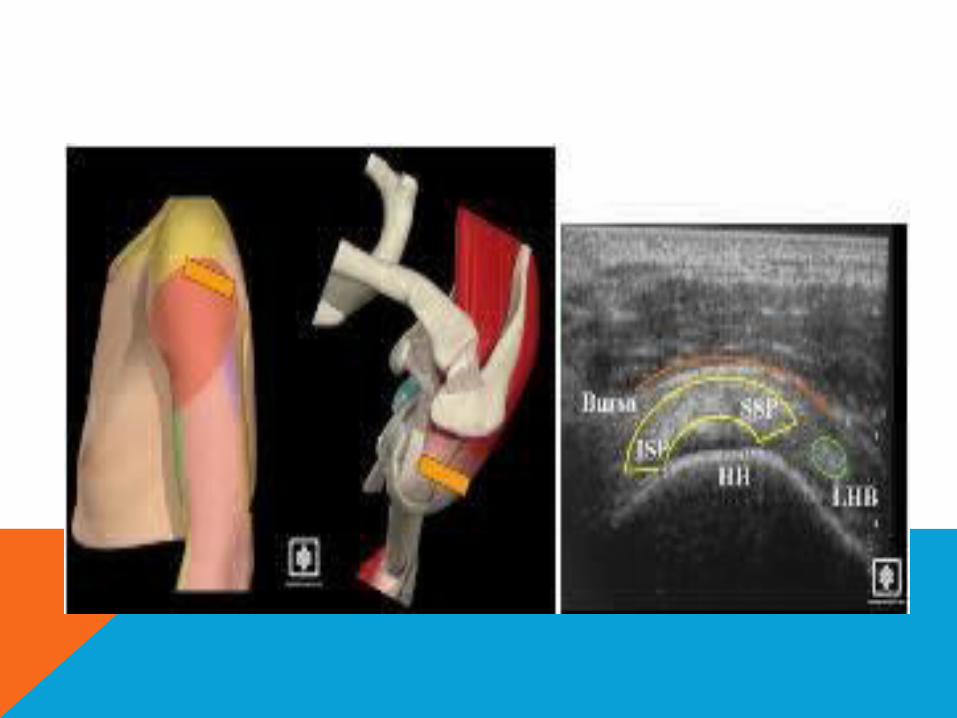
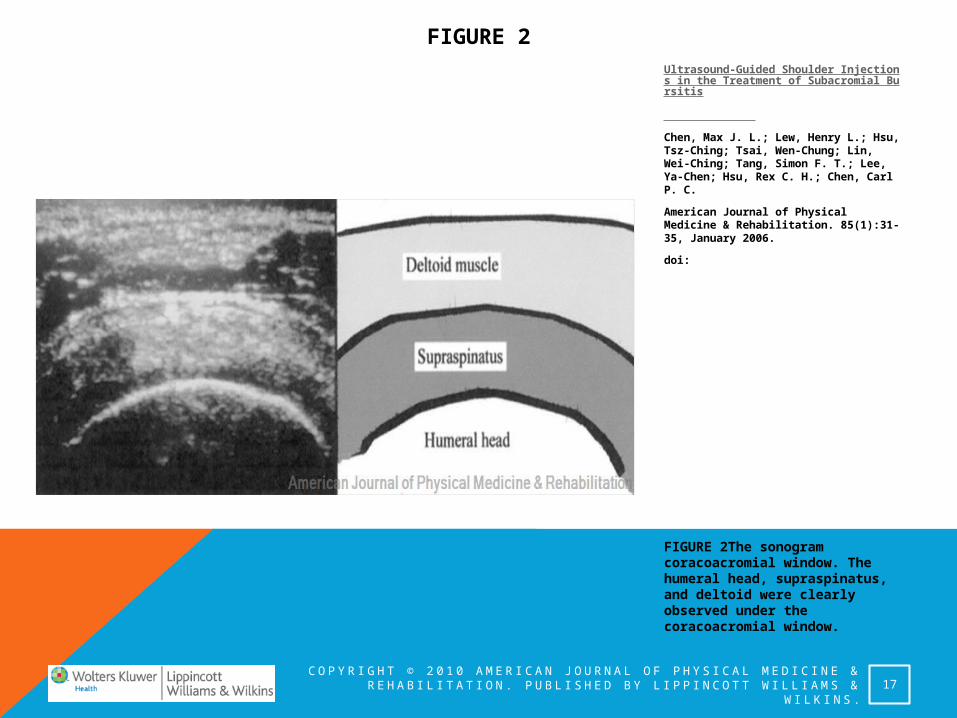
The humeral head, supraspinatus, deltoid were clearly observed under the coracoacromial window
C O P Y R I G H T © 2 0 1 0 A M E R I C A N J O U R N A L O F P H Y S I C A L M E D I C I N E & RE H A B I L I TAT I O N . P U B L I S H E D B Y L I P P I N C O T T W I L L I A M S & W I L K I N S .
FIGURE 2
FIGURE 2The sonogram coracoacromial window. The humeral head, supraspinatus, and deltoid were clearly observed under the coracoacromial window.
17
Ultrasound-Guided Shoulder Injections in the Treatment of Subacromial Bursitis
Chen, Max J. L.; Lew, Henry L.; Hsu, Tsz-Ching; Tsai, Wen-Chung; Lin, Wei-Ching; Tang, Simon F. T.; Lee, Ya-Chen; Hsu, Rex C. H.; Chen, Carl P. C.
American Journal of Physical Medicine & Rehabilitation. 85(1):31-35, January 2006.
doi:
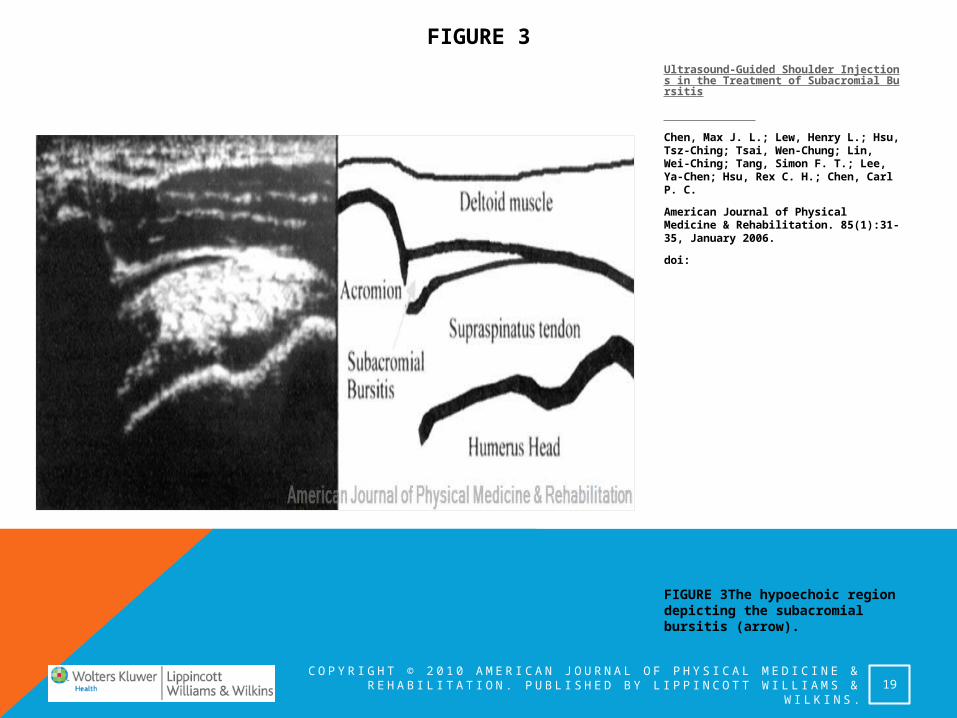
The subacromial bursitis was observed under the sonogram as a region of hypoechoic effusion between the deltoid and the humeral head.
C O P Y R I G H T © 2 0 1 0 A M E R I C A N J O U R N A L O F P H Y S I C A L M E D I C I N E & RE H A B I L I TAT I O N . P U B L I S H E D B Y L I P P I N C O T T W I L L I A M S & W I L K I N S .
FIGURE 3
FIGURE 3The hypoechoic region depicting the subacromial bursitis (arrow).
19
Ultrasound-Guided Shoulder Injections in the Treatment of Subacromial Bursitis
Chen, Max J. L.; Lew, Henry L.; Hsu, Tsz-Ching; Tsai, Wen-Chung; Lin, Wei-Ching; Tang, Simon F. T.; Lee, Ya-Chen; Hsu, Rex C. H.; Chen, Carl P. C.
American Journal of Physical Medicine & Rehabilitation. 85(1):31-35, January 2006.
doi:
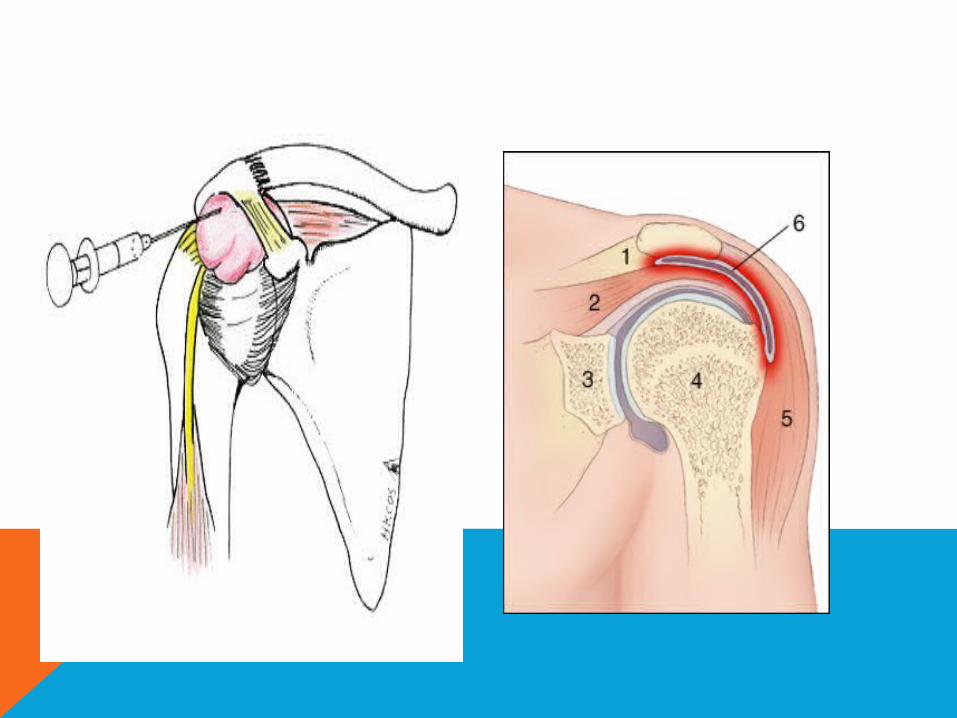
THE BLIND INJECTION TECHNIQUE
• palpation of the acromial by thumb, and then the needle wa was inserted in a horizontal approach.
• The needle was first adjusted in different depths and angle in trying to aspirate the effusion
• If no effusion could be aspirated, injected the steroid lidocaine suspension into the subacromial bursa
THE ULTRASOUND-GUIDED INJECTION TECHNIQUE
The needle was inserted into the subacromial bursa under ultrasound guidance.
Aspiration of the effusion was done first before injecting steroid-lidocaine suspension into the subacromial bursa
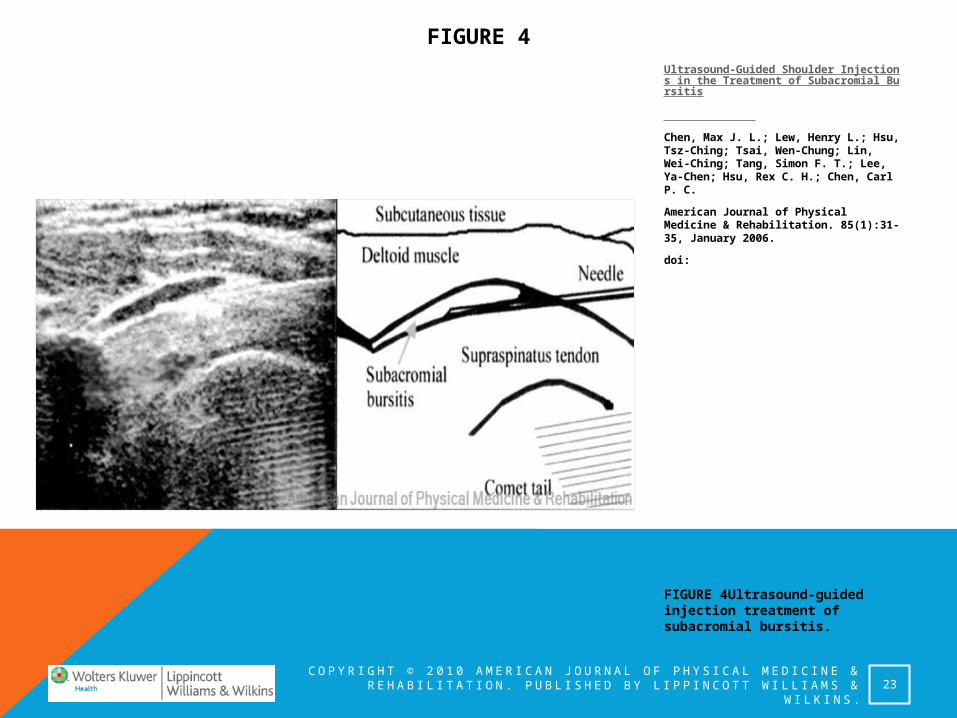
Under sonogram, the needle was observed as a hyperechoic structure.
C O P Y R I G H T © 2 0 1 0 A M E R I C A N J O U R N A L O F P H Y S I C A L M E D I C I N E & RE H A B I L I TAT I O N . P U B L I S H E D B Y L I P P I N C O T T W I L L I A M S & W I L K I N S .
FIGURE 4
FIGURE 4Ultrasound-guided injection treatment of subacromial bursitis.
23
Ultrasound-Guided Shoulder Injections in the Treatment of Subacromial Bursitis
Chen, Max J. L.; Lew, Henry L.; Hsu, Tsz-Ching; Tsai, Wen-Chung; Lin, Wei-Ching; Tang, Simon F. T.; Lee, Ya-Chen; Hsu, Rex C. H.; Chen, Carl P. C.
American Journal of Physical Medicine & Rehabilitation. 85(1):31-35, January 2006.
doi:
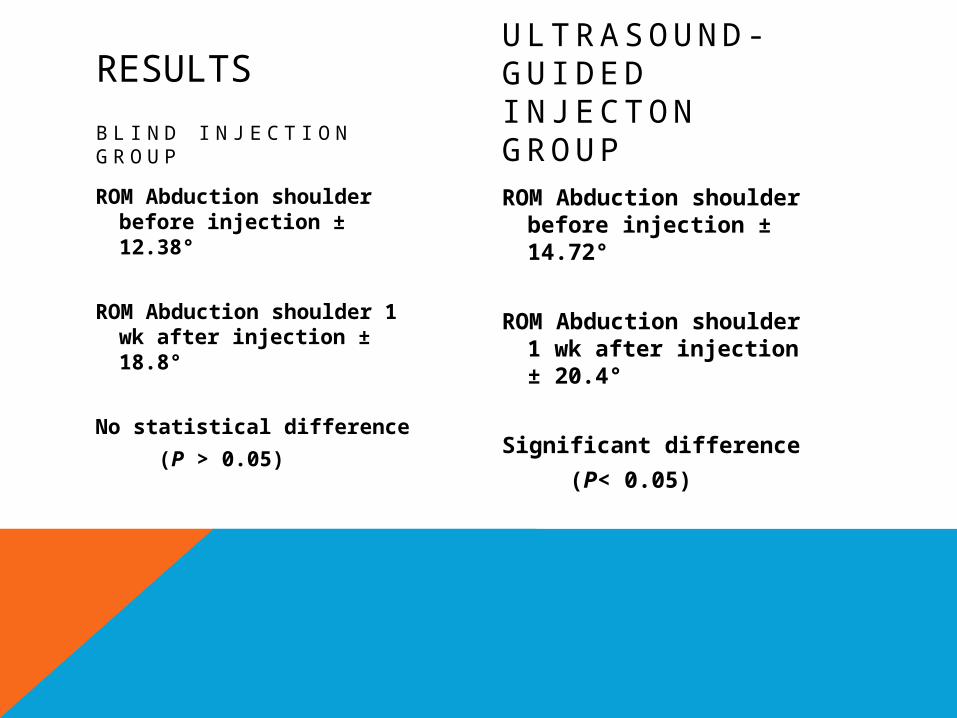
RESULTS
B L I N D I N J E C T I O N G R O U P
ROM Abduction shoulder before injection ± 12.38°
ROM Abduction shoulder 1 wk after injection ± 18.8°
No statistical difference
(P > 0.05)
U LT RA S O U N D -G U I D E D I N J E C T O N G R O U PROM Abduction
shoulder before injection ± 14.72°
ROM Abduction shoulder 1 wk after injection ± 20.4°
Significant difference
(P< 0.05)
The paired Student’s t test was used to determine whether there was a significant difference in shoulder abduction range of motion before and 1 wk after the injection in both groups.
Significant difference was defined as P < 0.05
DISCUSSION
Subacromial bursitis is often secondary to lesions in the tendinous cuff and a common cause of anterior shoulder pain and frequently develops in athletes who throw.
Soft-tissue ultrasound has proven to be an effective imaging tool in the diagnosis of subacromial bursitis
In treatment, subacromial bursitis ordinarily responds well to ice, rest, physical modality, and anti-inflammatory medications
In refractory cases, local injection of steroid suspension into the subacromial bursa may be needed
In clinical setting, most injections are performed via the blind palpation technique.
However, even an experienced physician performing the blind injection technique can never certain if the steroid-lidocaine suspension is injected accurately into the inflamed bursa
In this study, ultrasound → an effective imaging tool in performing ultrasound-guided shoulder subacromial bursitis injections & aspirations.
The significant improvement in shoulder abduction ROM after ultrasound-guided injection was accurately infiltrated into the lesion site as compare with the blind injection technique
CONCLUSION
Based on the result obtained in this study, ultrasound may be used as an adjuvant tool in guiding the needle accurately into the subacromial bursa to perform effective injection treatment
The ultrasound-guided injection technique in the treatment of subacromial bursitis can result in significant improvement in shoulder abduction ROM as compared with the blind injection technique
TERIMA KASIH
Bearing in mind that the supraspinatus runs in a plane at 30° to the coronal plane of the body the probe should be placed for a longitudinal view of the suprsapinatus between 30° and 60° to the coronal axis of the plane of the body. This should give a good view of the greater tuberosity footprint area and superior articular surface of the humeral head. The probe can then be moved from antero-medial to postero-lateral, i.e. from the anterior leading edge of supraspinatus towards the infraspinatus tendon. The commonest area for supraspinatus tears is in this region.
The probe is then rotated 90° for a transverse view of the supraspinatus and anterior portion of the infraspinatus tendons (superior cuff). The probe can then be moved medially and laterally as well as antero-medial and postero-lateral for a good impression of this area. Further medial movement is limited by the acromium.