Embed Size (px)
Citation preview
Delivering high quality multidisciplinary research in primary care.
Ultrasound in Rheumatology
Alison Hall Consultant MSK Sonographer
Research Institute for Primary Care & Health Sciences, Keele University
Department of Rheumatology, Cannock Hospital, Royal Wolverhampton Trust

Objectives
• Introducing arthritis
• Diagnosis
• Role of Ultrasound
• Technique
• Ultrasound appearances
• Pitfalls
• Managing IA
• Take home messages
Introducing arthritis
‘Acute or chronic inflammation of one or more joints,
usually accompanied by pain and stiffness, resulting
from infection, trauma, degenerative changes,
autoimmune disease, or other cause’
The American Heritage® Science Dictionary
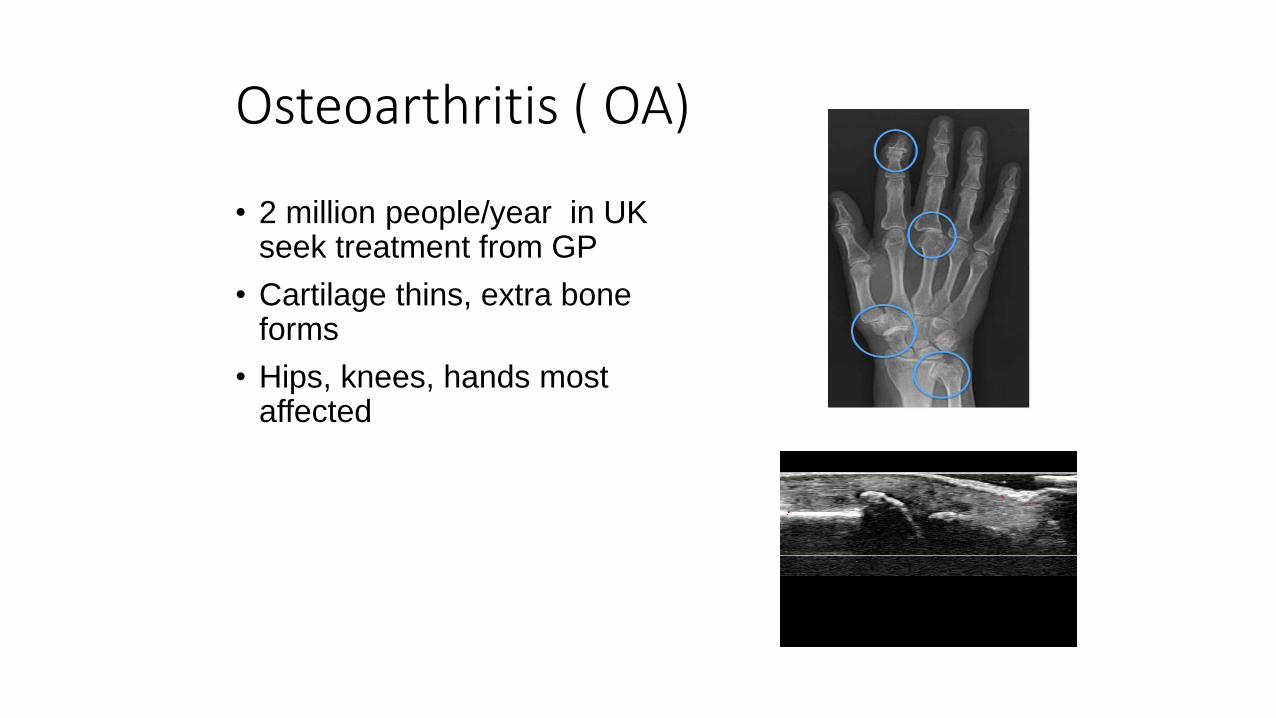
Osteoarthritis ( OA)
• 2 million people/year in UK seek treatment from GP
• Cartilage thins, extra bone forms
• Hips, knees, hands most affected
Inflammatory Arthritis (IA)
Presentations to GP/year
• Rheumatoid arthritis – 350,000
• Gout – 250,000
• Ankylosing spondylitis – 115,000
• Juvenile Idiopathic arthritis – 12,000
• Rarer inflammatory disorders – Lupus, temporal arteritis, polymyalgia rheumatica
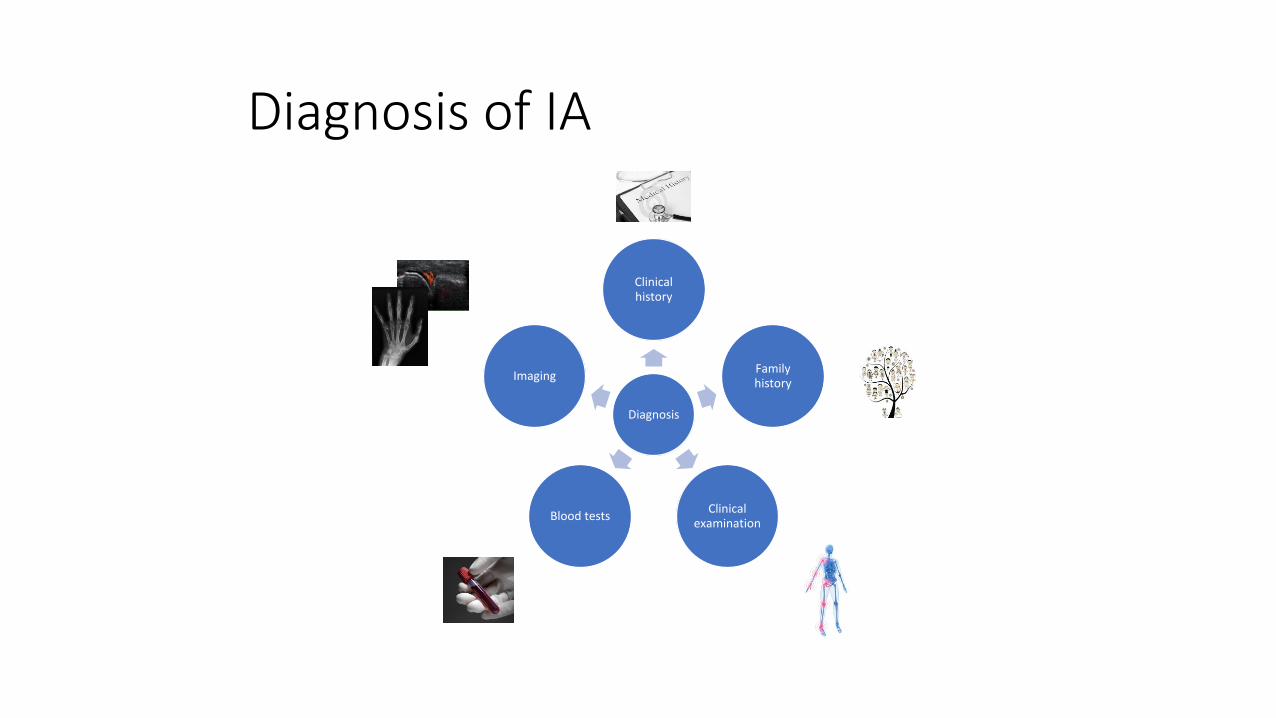
Diagnosis of IA
Diagnosis
Clinical history
Family history
Clinical examination
Blood tests
Imaging
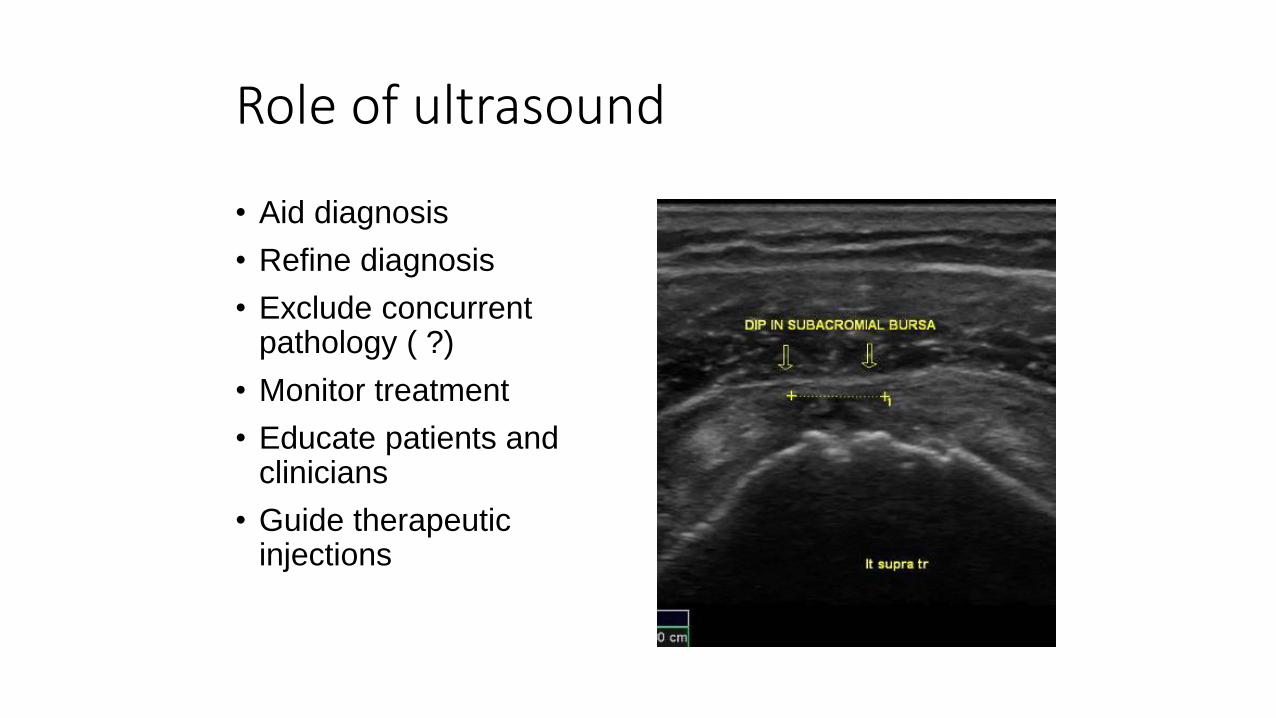
Role of ultrasound
• Aid diagnosis
• Refine diagnosis
• Exclude concurrent pathology ( ?)
• Monitor treatment
• Educate patients and clinicians
• Guide therapeutic injections
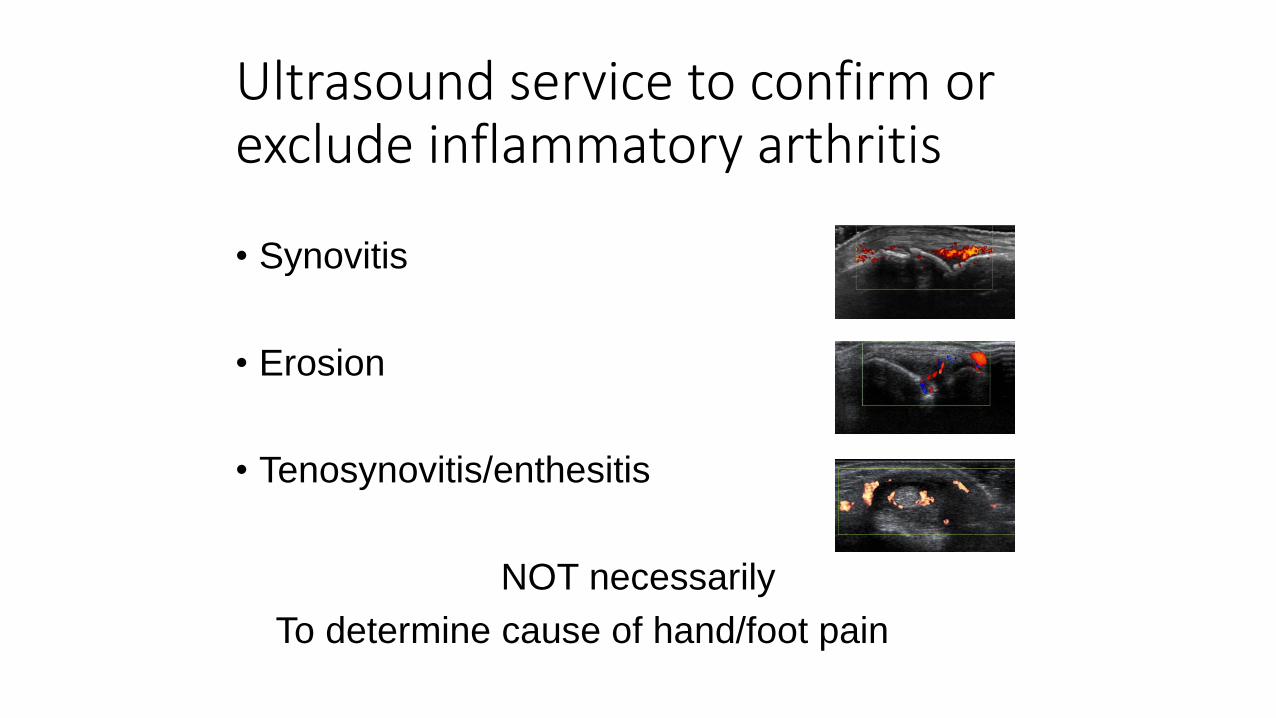
Ultrasound service to confirm or exclude inflammatory arthritis
• Synovitis
• Erosion
• Tenosynovitis/enthesitis
NOT necessarily
To determine cause of hand/foot pain
So…who should be scanning these patients?
• Radiology• Huge ultrasound experience
• Less clinical rheumatology knowledge
• Best equipment/setup
• Less accessible – waiting times, other commitments
• Rheumatology• Variable ultrasound experience
• Huge clinical rheumatology knowledge
• Variable equipment/difficult setup
• Immediately accessible – one stop shops
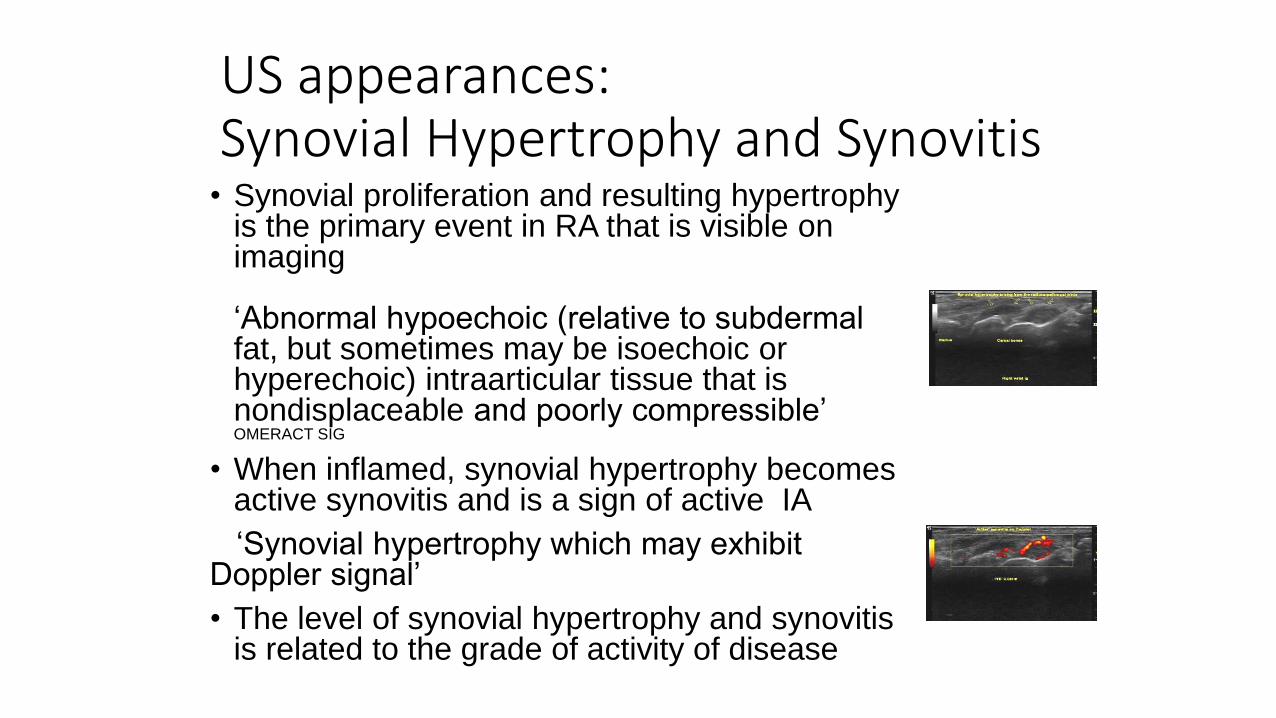
US appearances:Synovial Hypertrophy and Synovitis
• Synovial proliferation and resulting hypertrophy is the primary event in RA that is visible on imaging
‘Abnormal hypoechoic (relative to subdermal fat, but sometimes may be isoechoic or hyperechoic) intraarticular tissue that is nondisplaceable and poorly compressible’ OMERACT SIG
• When inflamed, synovial hypertrophy becomes active synovitis and is a sign of active IA
‘Synovial hypertrophy which may exhibit Doppler signal’
• The level of synovial hypertrophy and synovitis is related to the grade of activity of disease
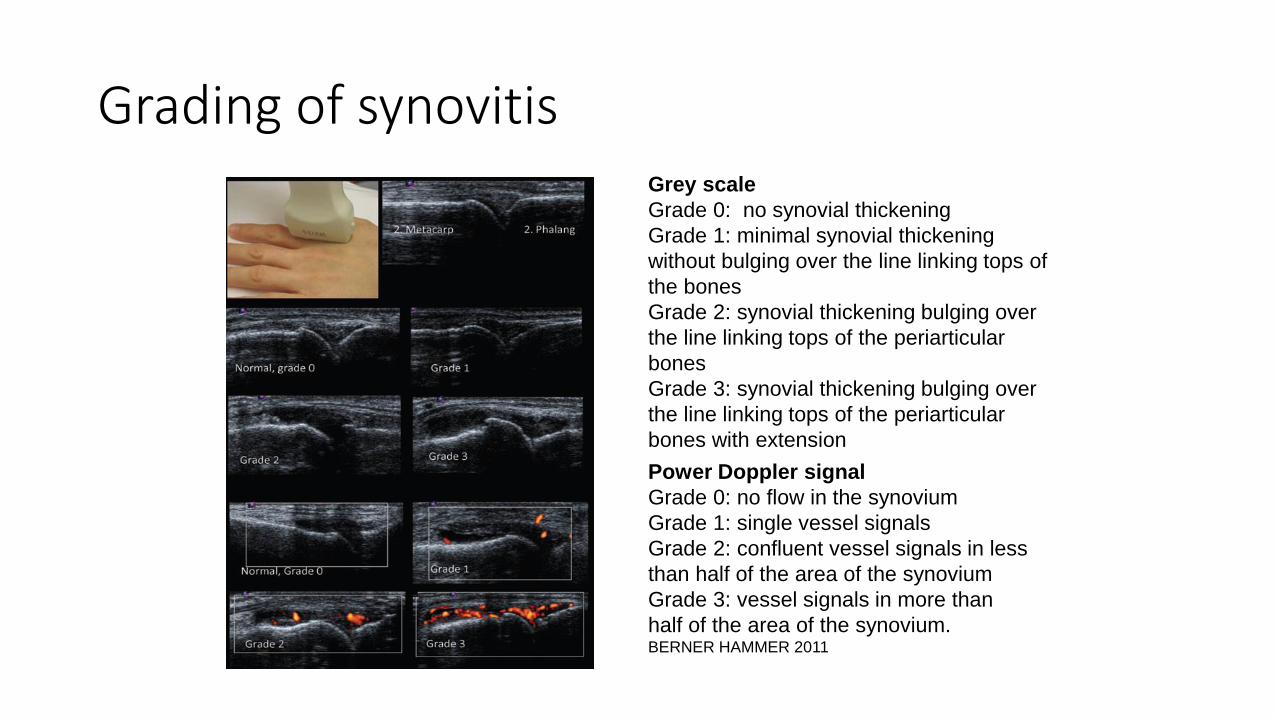
Grading of synovitis
Power Doppler signal
Grade 0: no flow in the synovium
Grade 1: single vessel signals
Grade 2: confluent vessel signals in less
than half of the area of the synovium
Grade 3: vessel signals in more than
half of the area of the synovium.BERNER HAMMER 2011
Grey scale
Grade 0: no synovial thickening
Grade 1: minimal synovial thickening
without bulging over the line linking tops of
the bones
Grade 2: synovial thickening bulging over
the line linking tops of the periarticular
bones
Grade 3: synovial thickening bulging over
the line linking tops of the periarticular
bones with extension
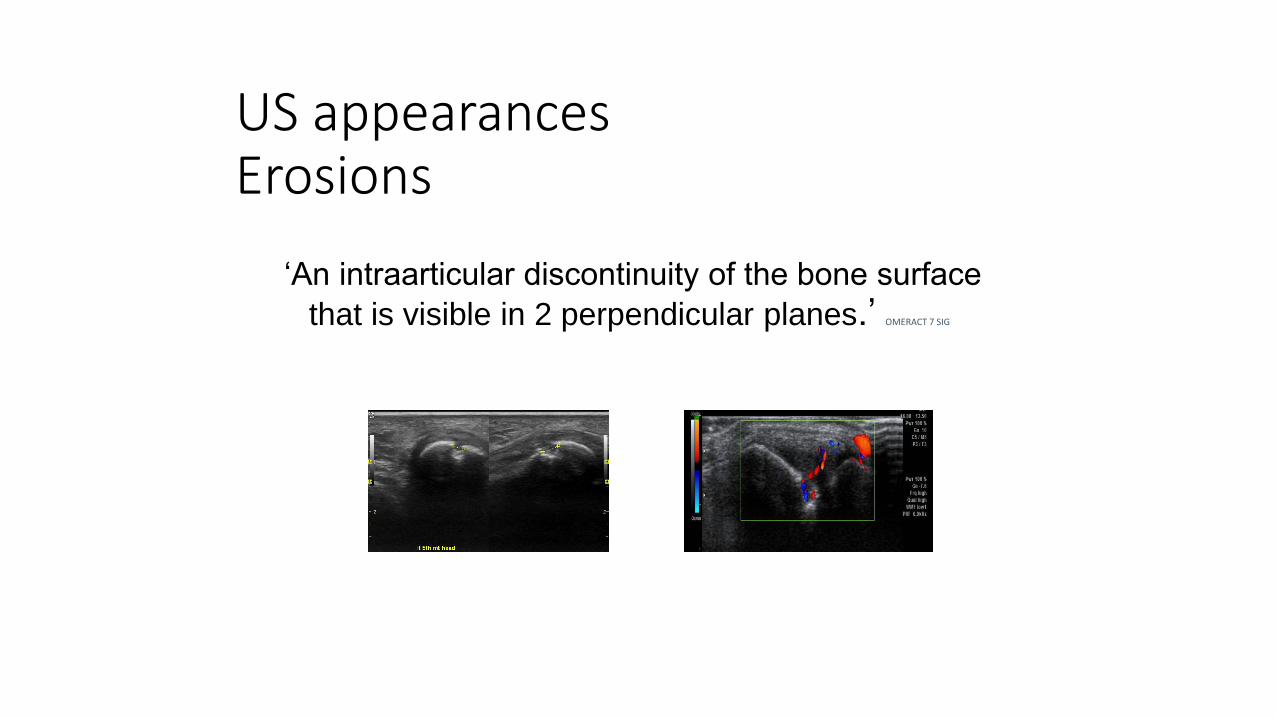
US appearancesErosions
‘An intraarticular discontinuity of the bone surface
that is visible in 2 perpendicular planes.’ OMERACT 7 SIG
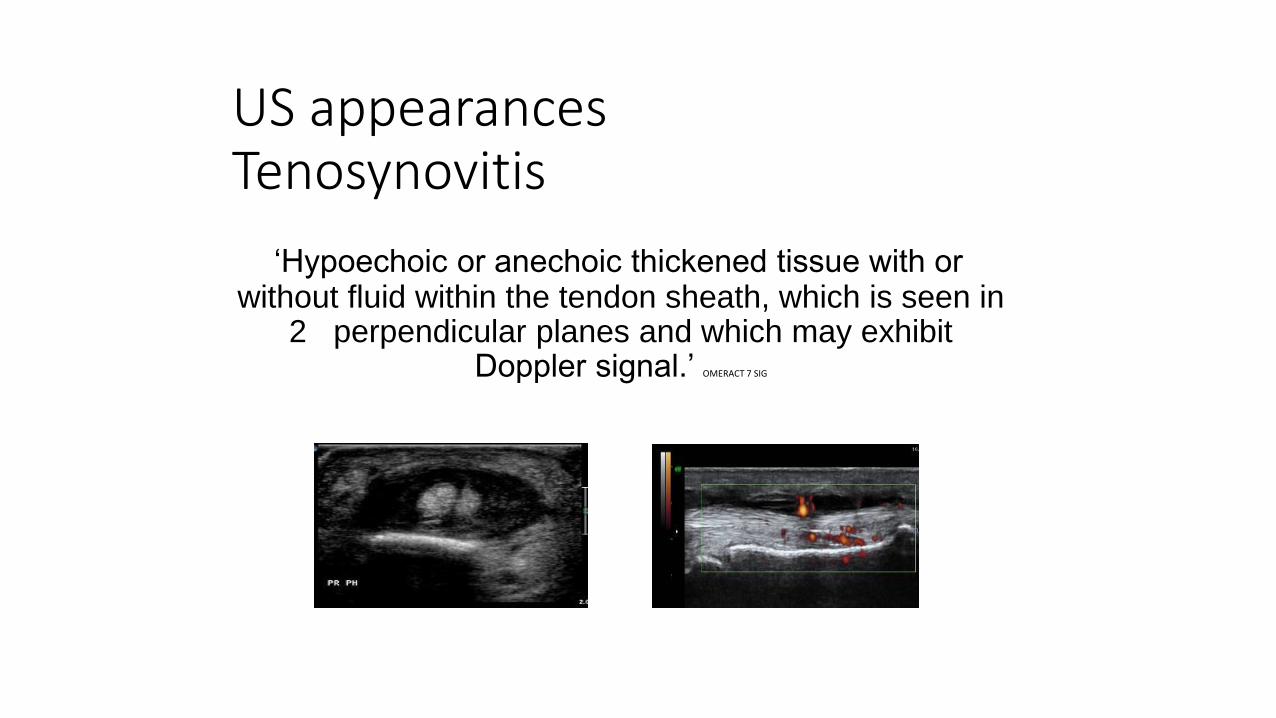
US appearances Tenosynovitis
‘Hypoechoic or anechoic thickened tissue with or without fluid within the tendon sheath, which is seen in
2 perpendicular planes and which may exhibit Doppler signal.’ OMERACT 7 SIG
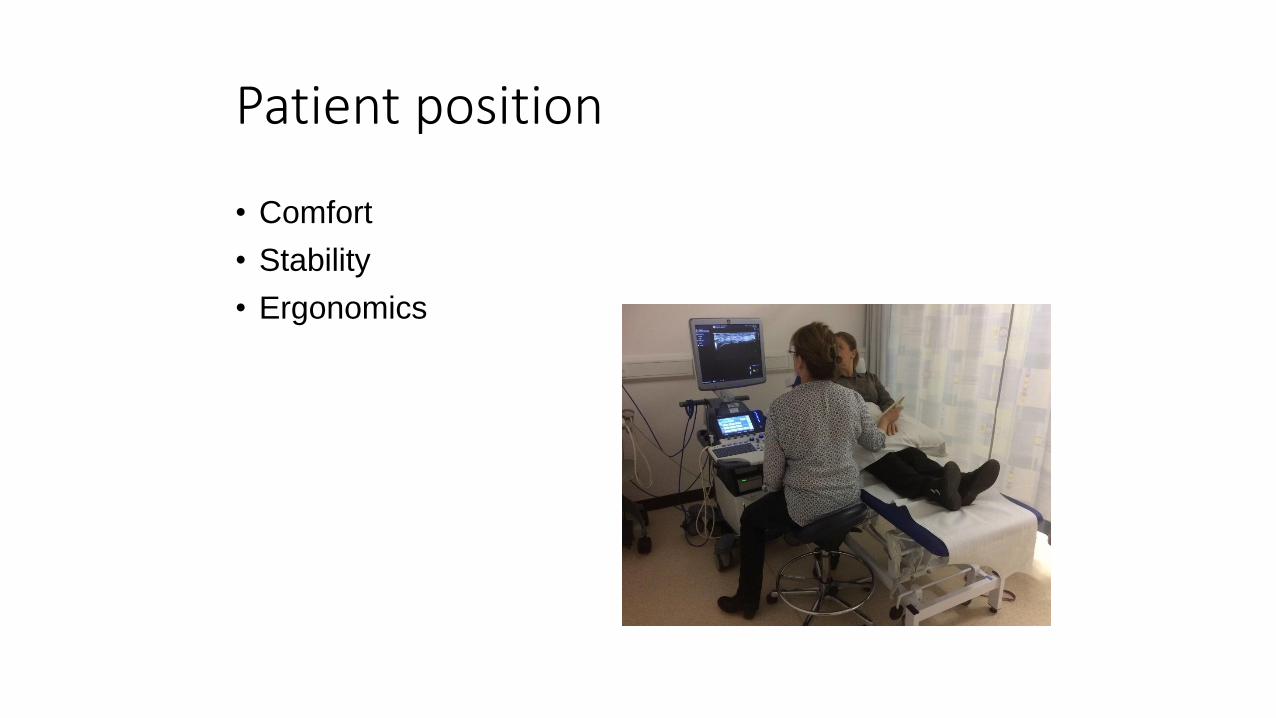
Patient position
• Comfort
• Stability
• Ergonomics
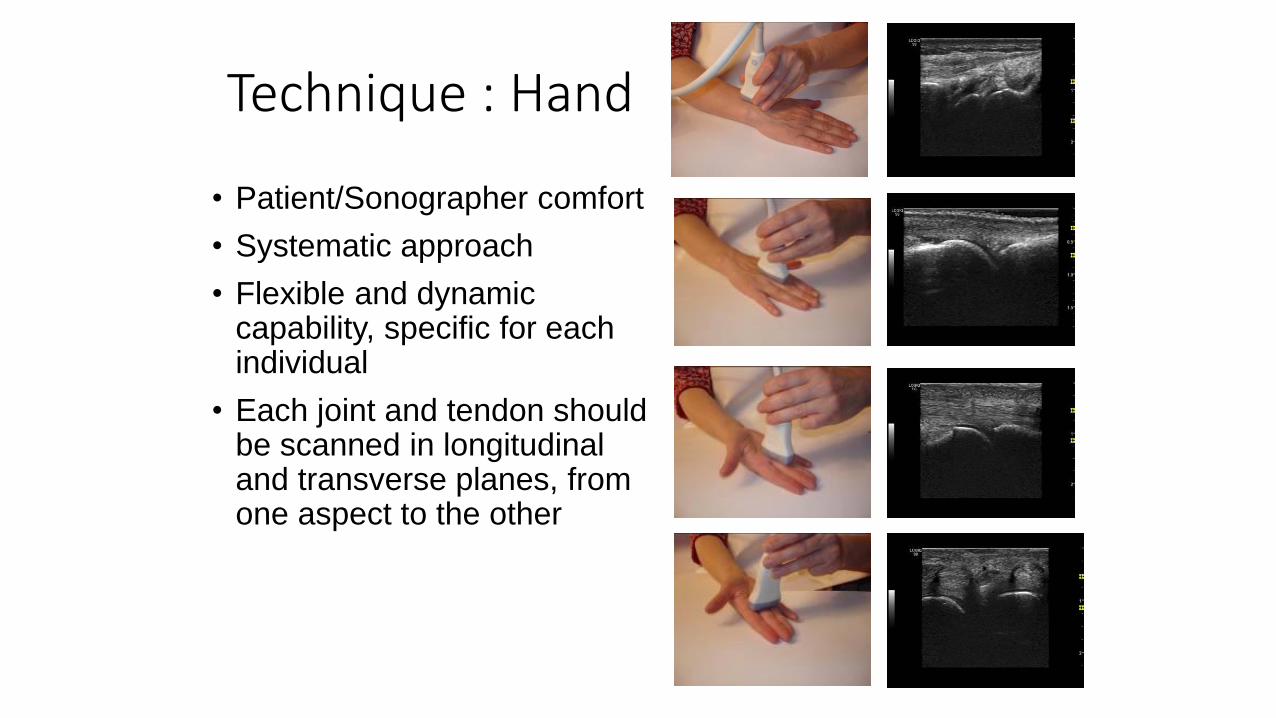
Technique : Hand
• Patient/Sonographer comfort
• Systematic approach
• Flexible and dynamic capability, specific for each individual
• Each joint and tendon should be scanned in longitudinal and transverse planes, from one aspect to the other
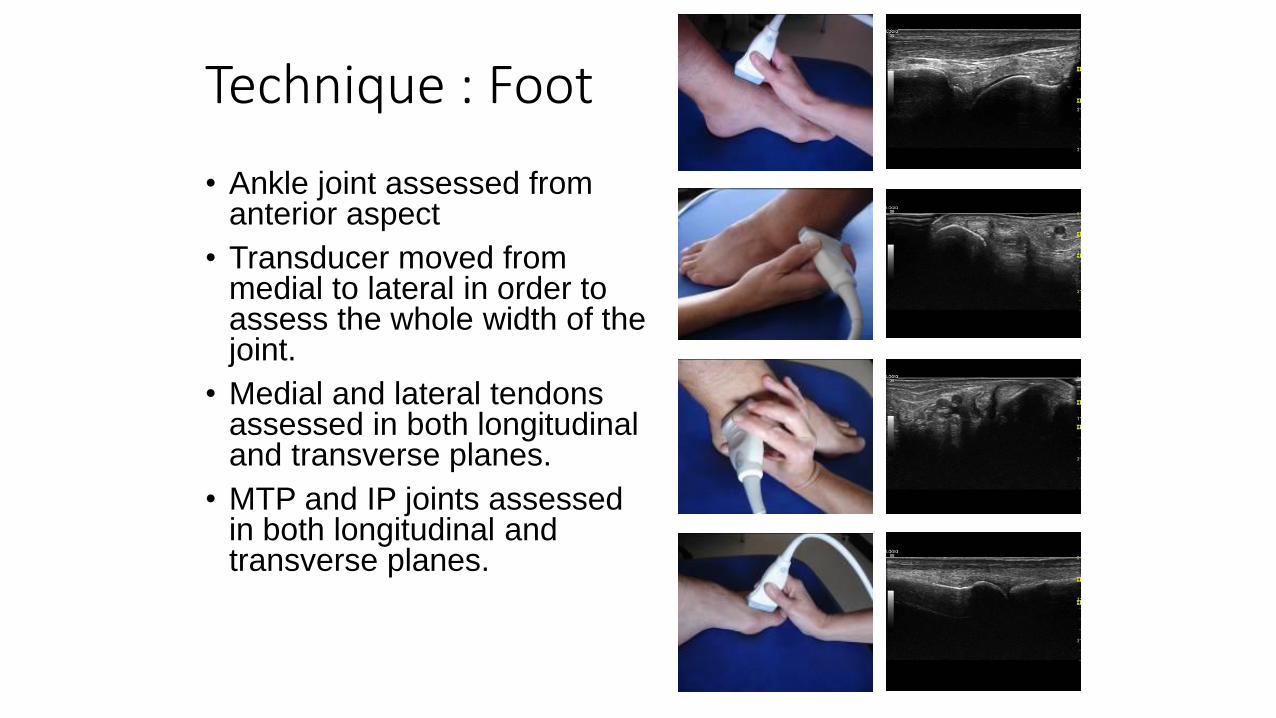
Technique : Foot
• Ankle joint assessed from anterior aspect
• Transducer moved from medial to lateral in order to assess the whole width of the joint.
• Medial and lateral tendons assessed in both longitudinal and transverse planes.
• MTP and IP joints assessed in both longitudinal and transverse planes.
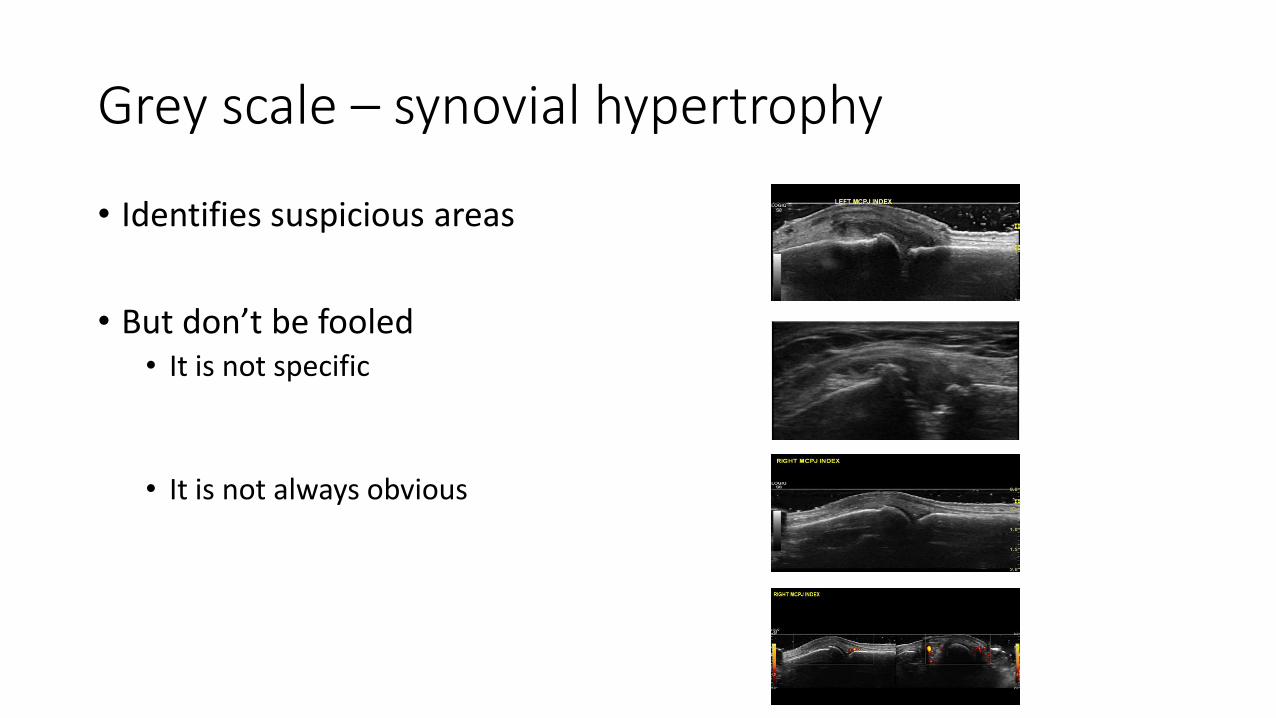
Grey scale – synovial hypertrophy
• Identifies suspicious areas
• But don’t be fooled• It is not specific
• It is not always obvious
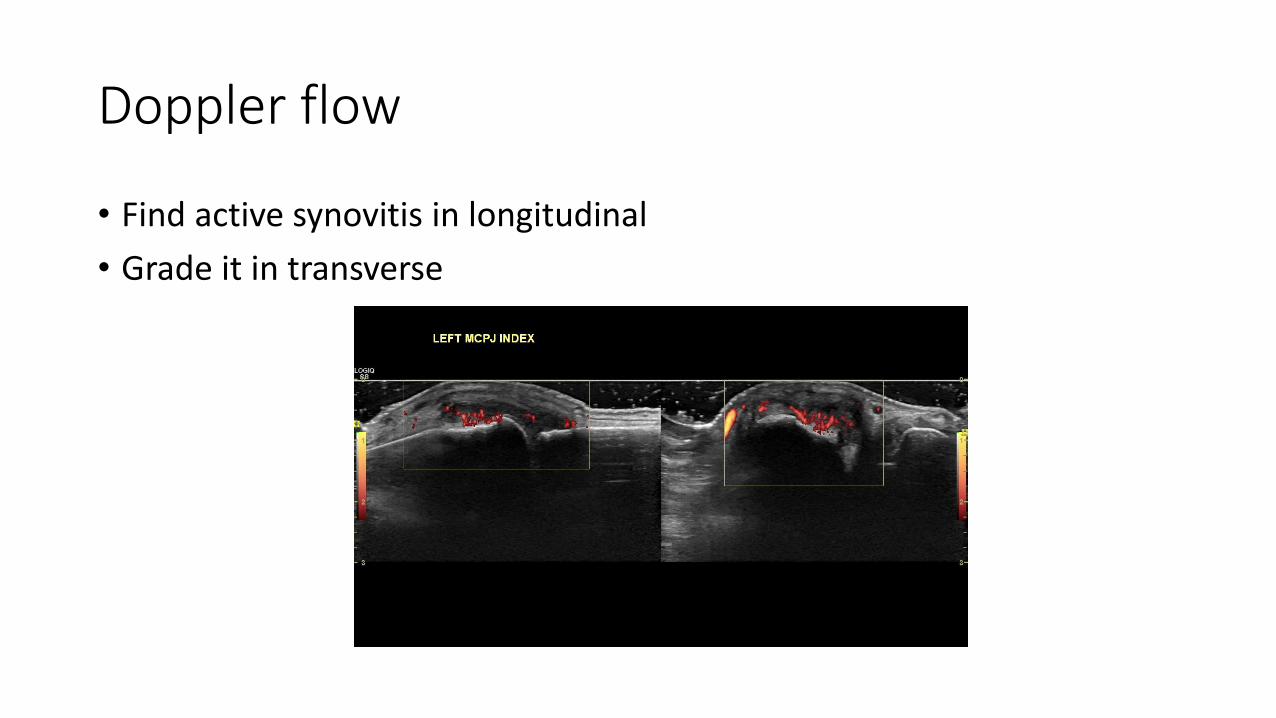
Doppler flow
• Find active synovitis in longitudinal
• Grade it in transverse
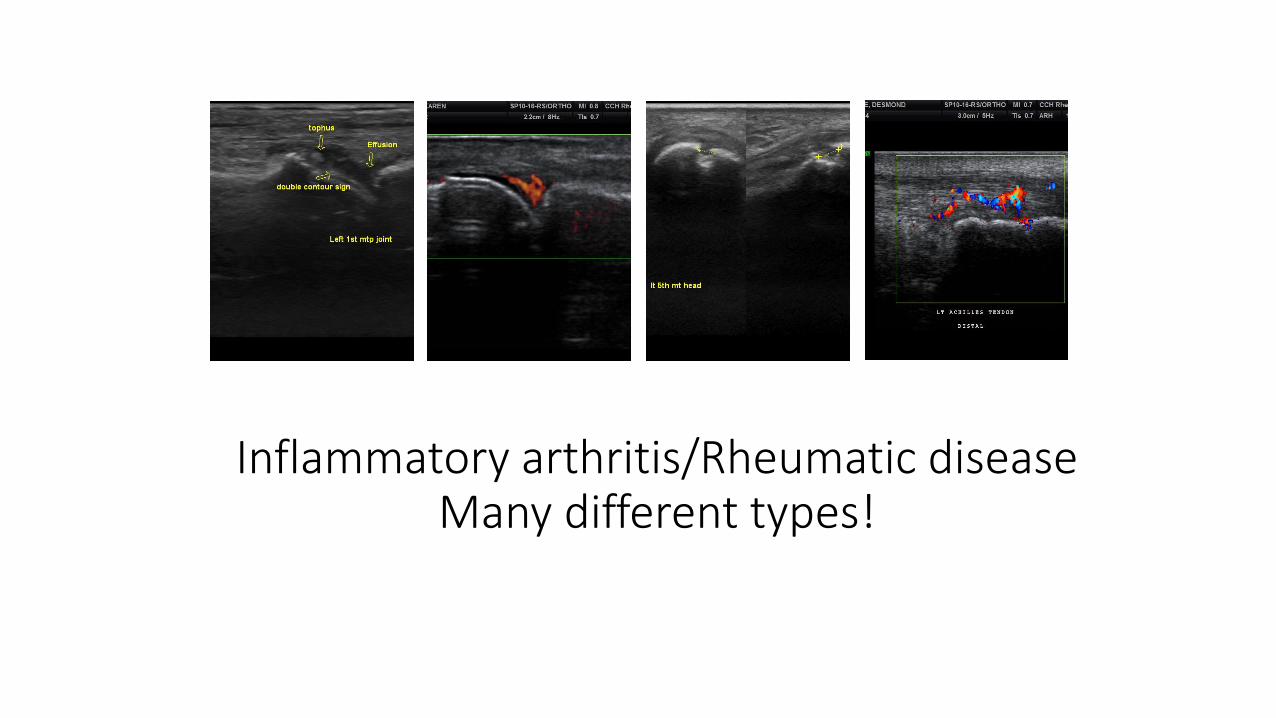
Inflammatory arthritis/Rheumatic diseaseMany different types!
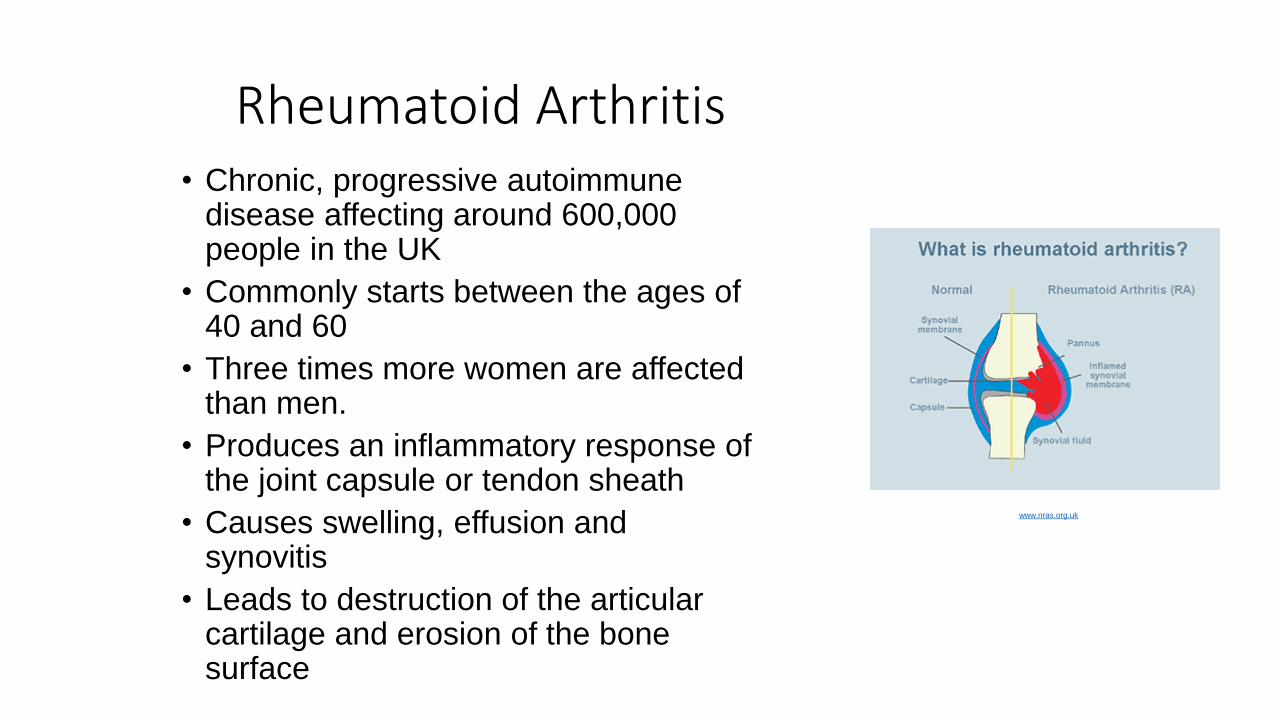
Rheumatoid Arthritis• Chronic, progressive autoimmune
disease affecting around 600,000 people in the UK
• Commonly starts between the ages of 40 and 60
• Three times more women are affected than men.
• Produces an inflammatory response of the joint capsule or tendon sheath
• Causes swelling, effusion and synovitis
• Leads to destruction of the articular cartilage and erosion of the bone surface
www.nras.org.uk
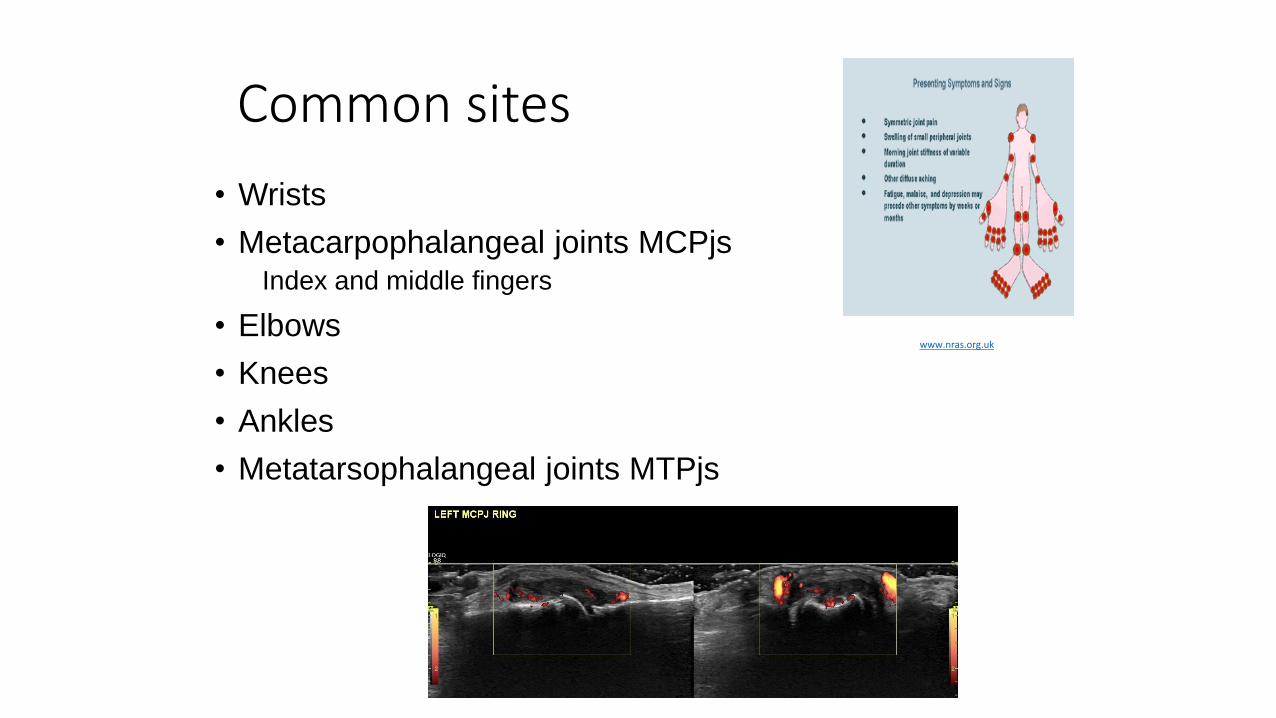
Common sites
• Wrists
• Metacarpophalangeal joints MCPjsIndex and middle fingers
• Elbows
• Knees
• Ankles
• Metatarsophalangeal joints MTPjs
www.nras.org.uk
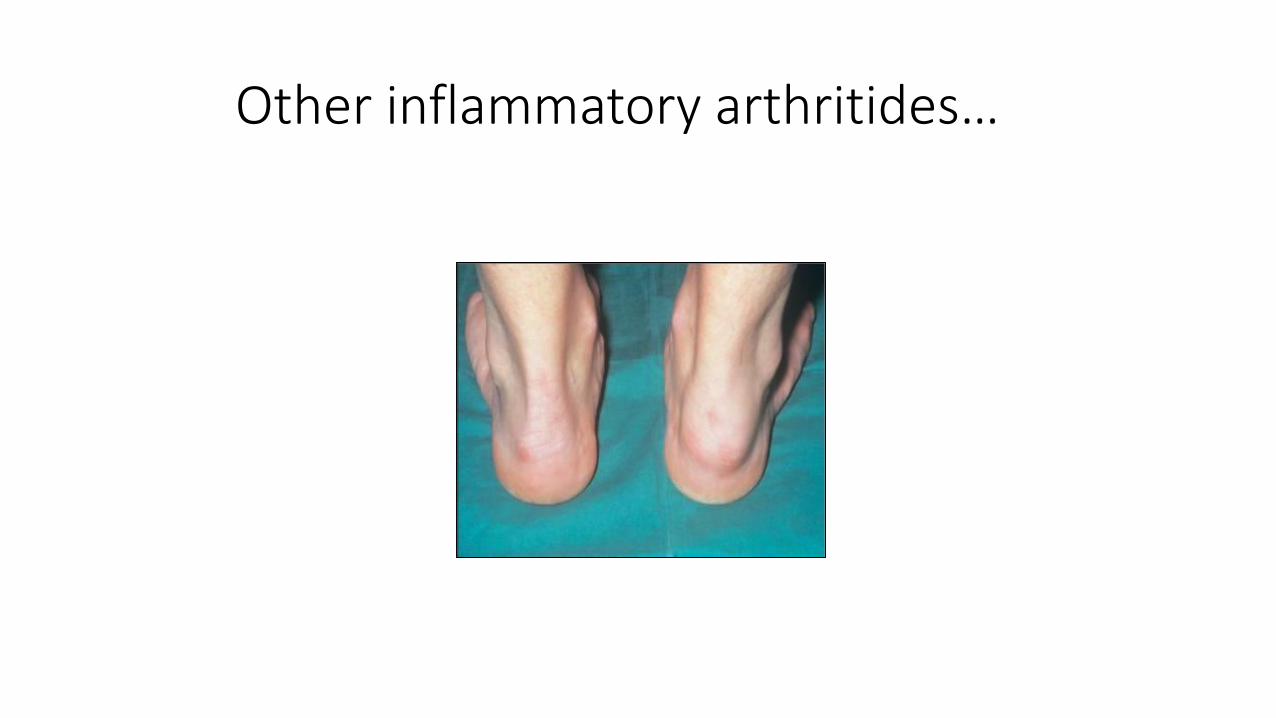
Other inflammatory arthritides…
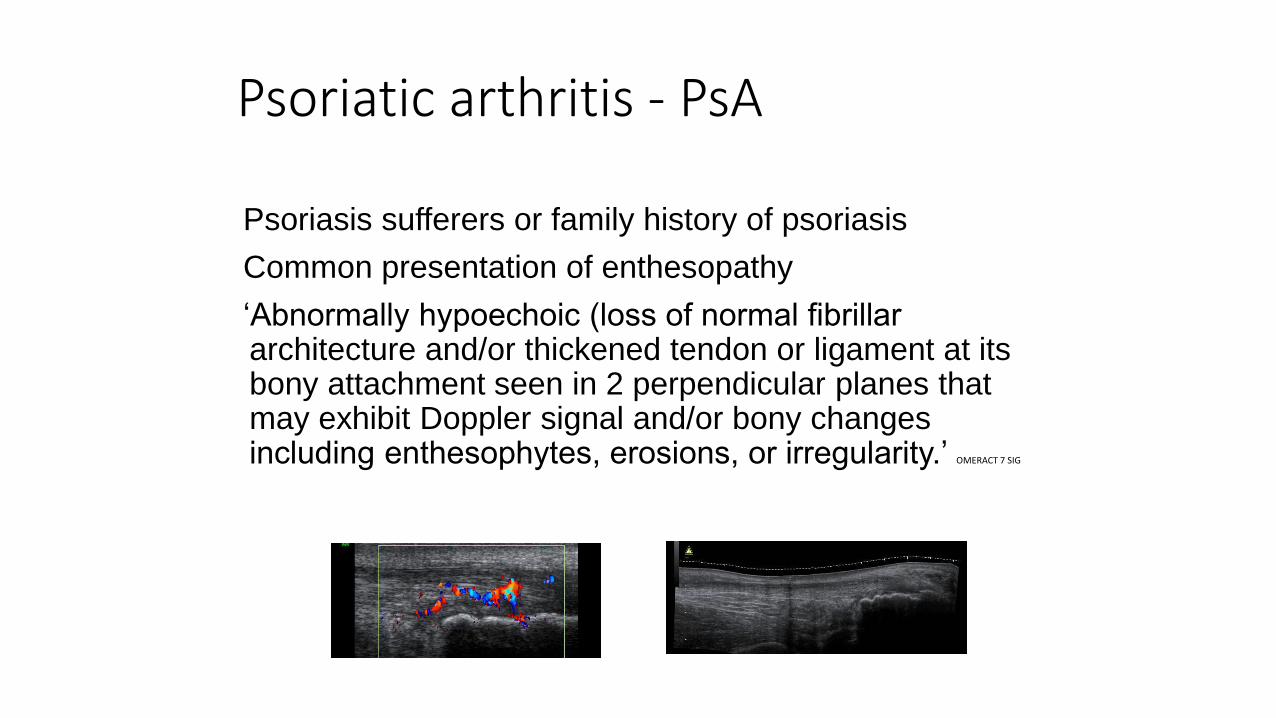
Psoriatic arthritis - PsA
Psoriasis sufferers or family history of psoriasis
Common presentation of enthesopathy
‘Abnormally hypoechoic (loss of normal fibrillar architecture and/or thickened tendon or ligament at its bony attachment seen in 2 perpendicular planes that may exhibit Doppler signal and/or bony changes including enthesophytes, erosions, or irregularity.’ OMERACT 7 SIG
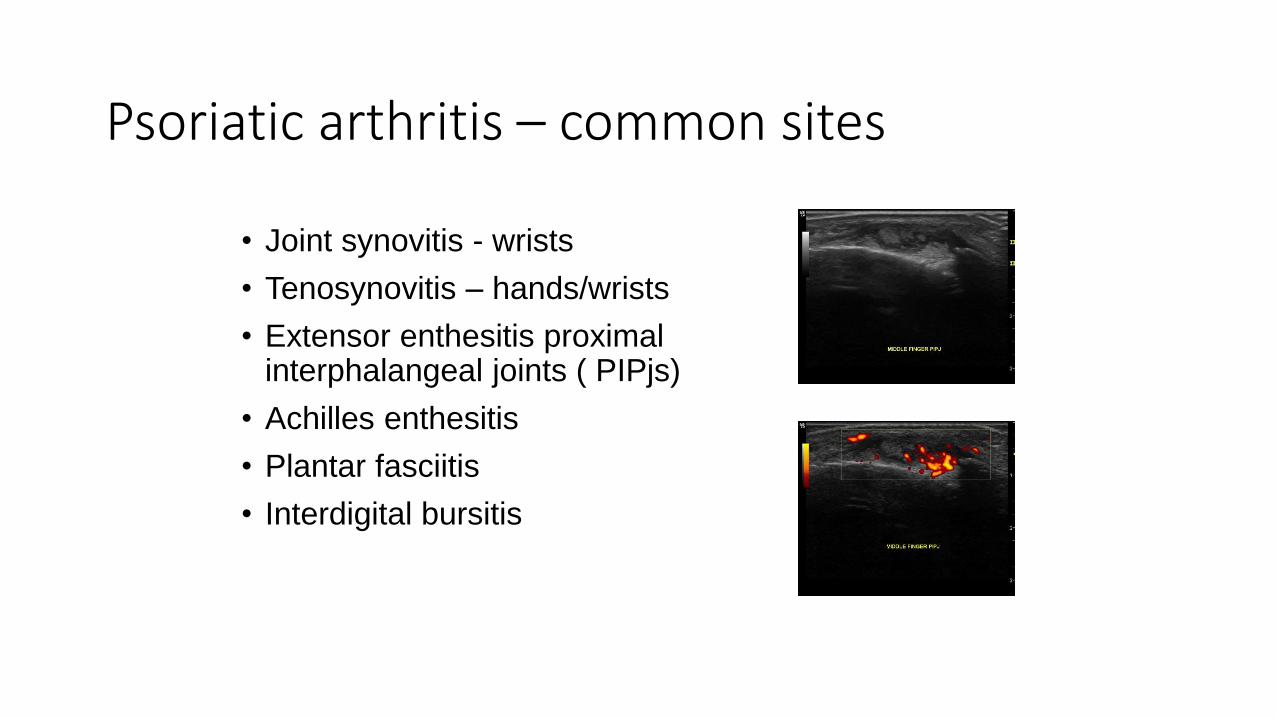
Psoriatic arthritis – common sites
• Joint synovitis - wrists
• Tenosynovitis – hands/wrists
• Extensor enthesitis proximal interphalangeal joints ( PIPjs)
• Achilles enthesitis
• Plantar fasciitis
• Interdigital bursitis
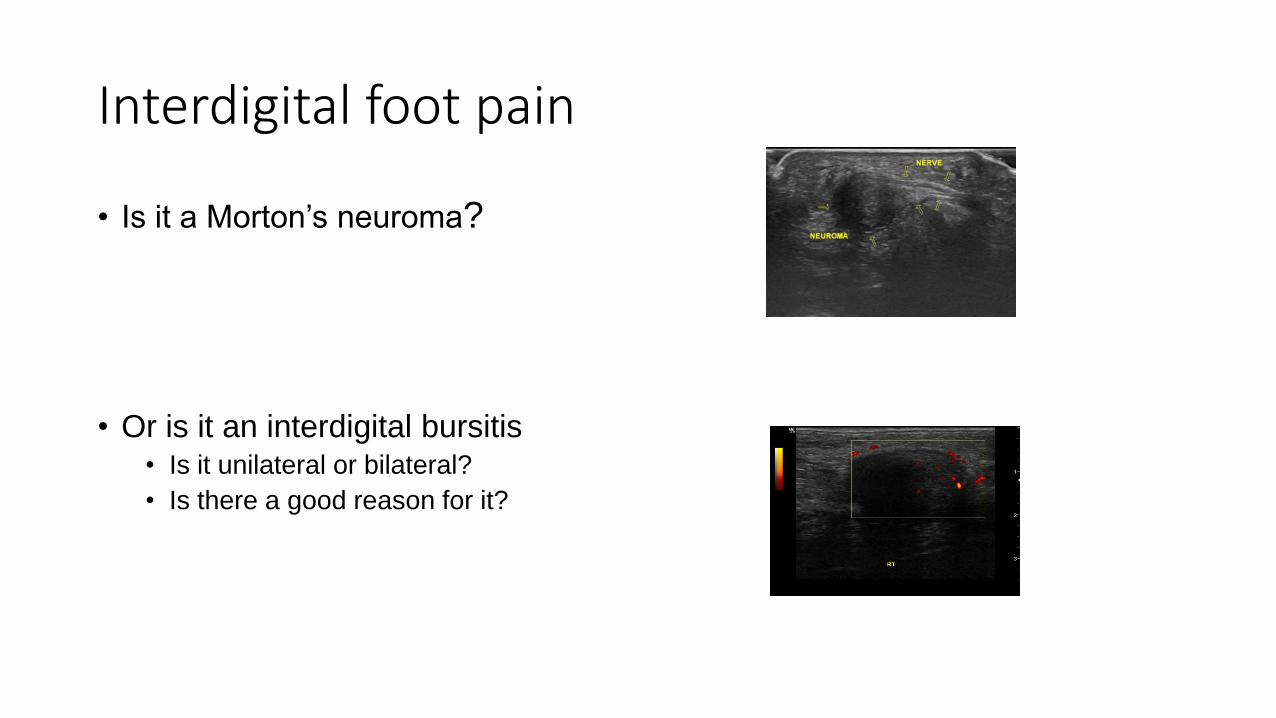
Interdigital foot pain
• Is it a Morton’s neuroma?
• Or is it an interdigital bursitis• Is it unilateral or bilateral?
• Is there a good reason for it?
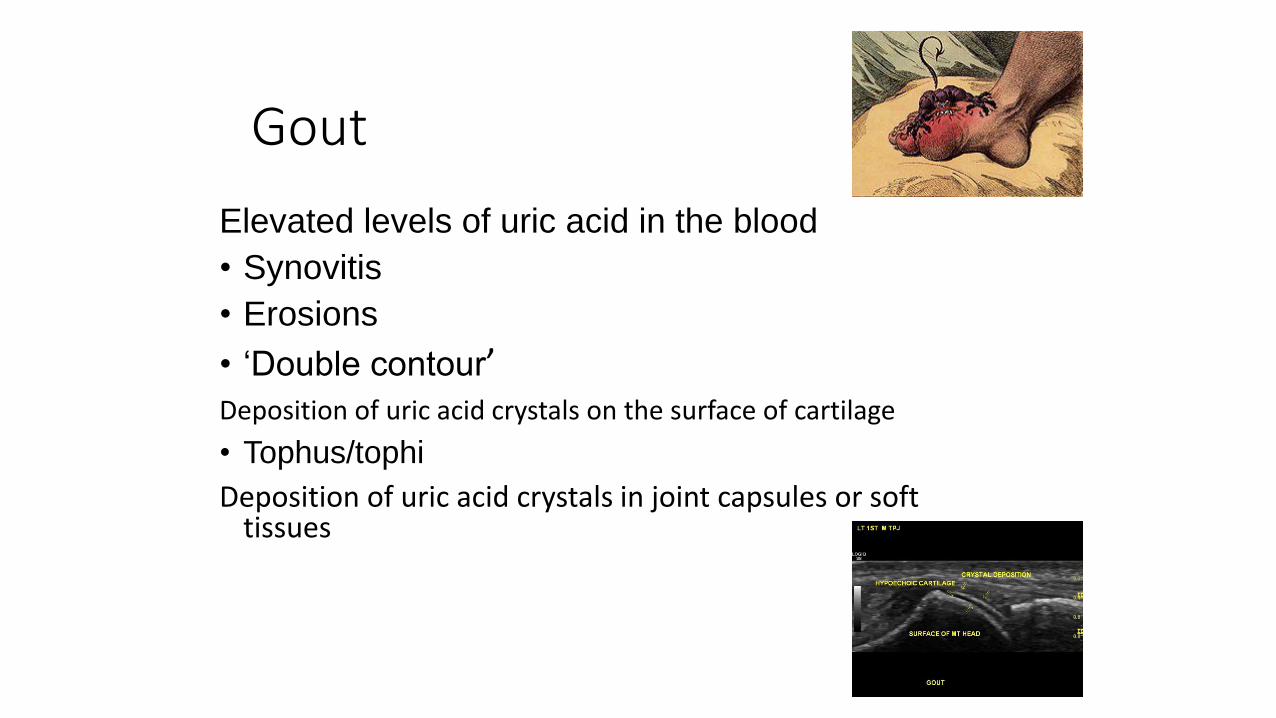
Gout
Elevated levels of uric acid in the blood
• Synovitis
• Erosions
• ‘Double contour’Deposition of uric acid crystals on the surface of cartilage
• Tophus/tophi
Deposition of uric acid crystals in joint capsules or soft tissues
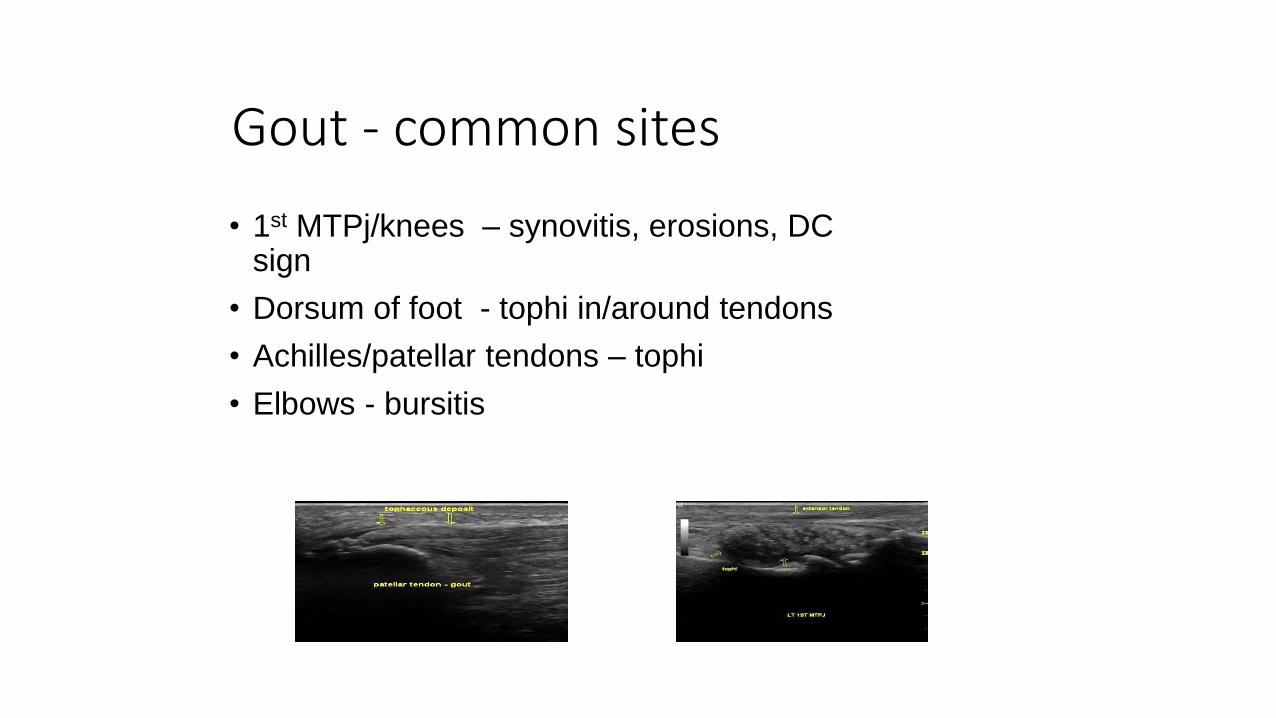
Gout - common sites
• 1st MTPj/knees – synovitis, erosions, DC sign
• Dorsum of foot - tophi in/around tendons
• Achilles/patellar tendons – tophi
• Elbows - bursitis
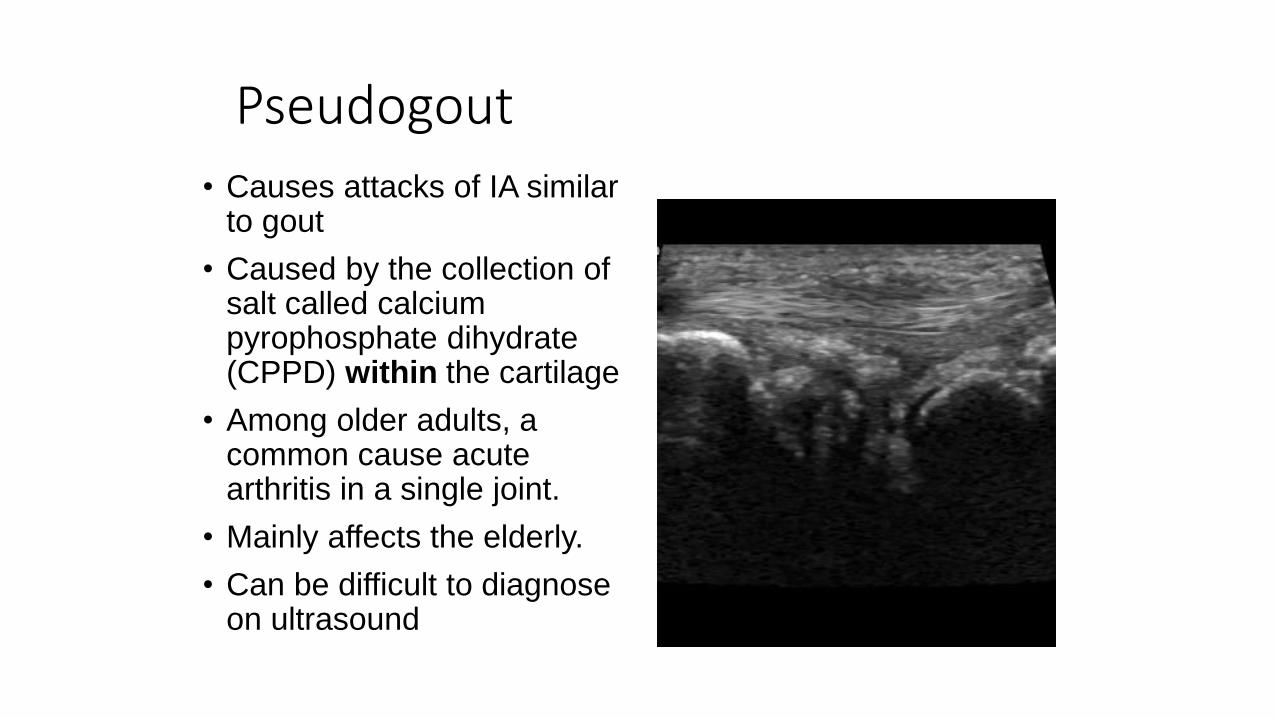
Pseudogout
• Causes attacks of IA similar to gout
• Caused by the collection of salt called calcium pyrophosphate dihydrate (CPPD) within the cartilage
• Among older adults, a common cause acute arthritis in a single joint.
• Mainly affects the elderly.
• Can be difficult to diagnose on ultrasound
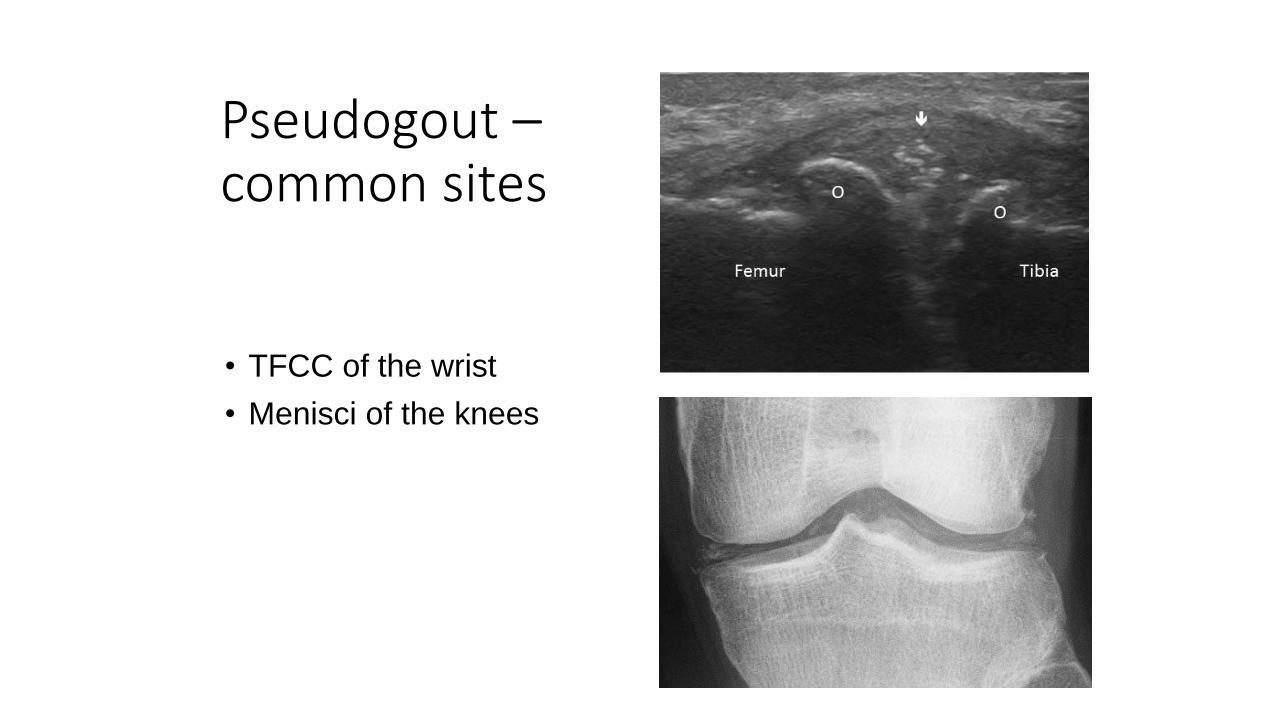
Pseudogout –common sites
• TFCC of the wrist
• Menisci of the knees
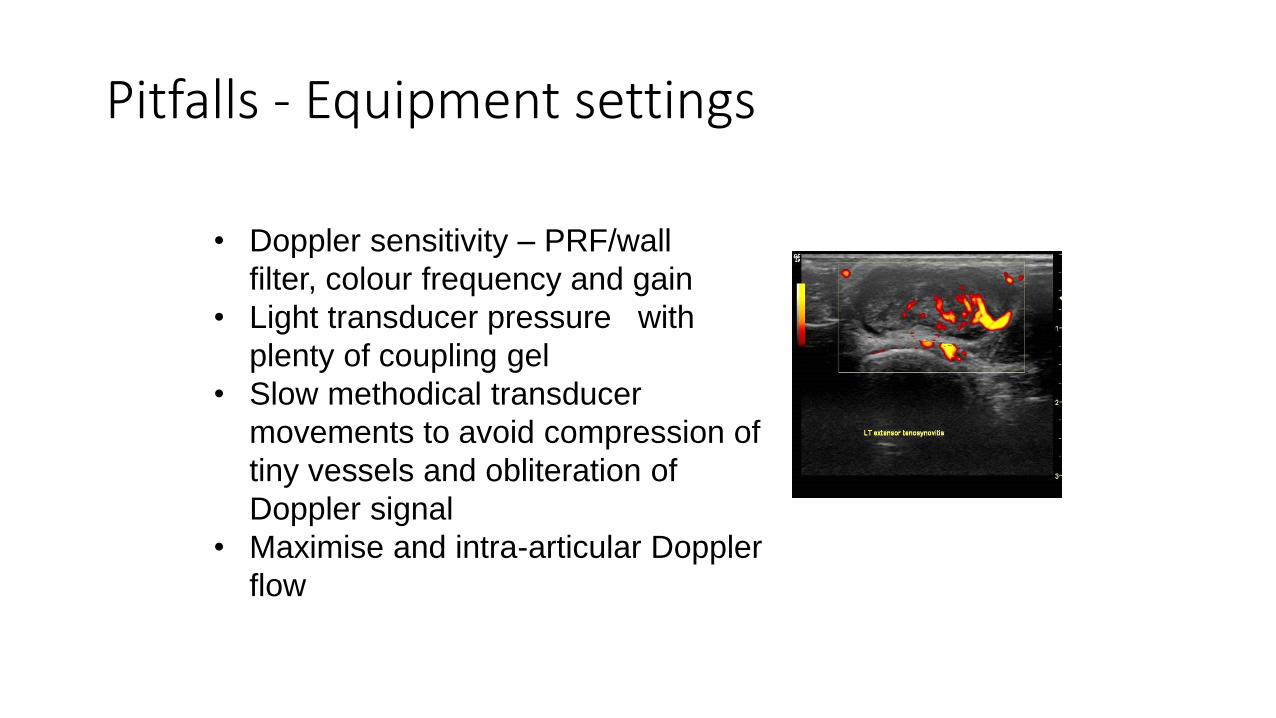
Pitfalls - Equipment settings
• Doppler sensitivity – PRF/wall
filter, colour frequency and gain
• Light transducer pressure with
plenty of coupling gel
• Slow methodical transducer
movements to avoid compression of
tiny vessels and obliteration of
Doppler signal
• Maximise and intra-articular Doppler
flow
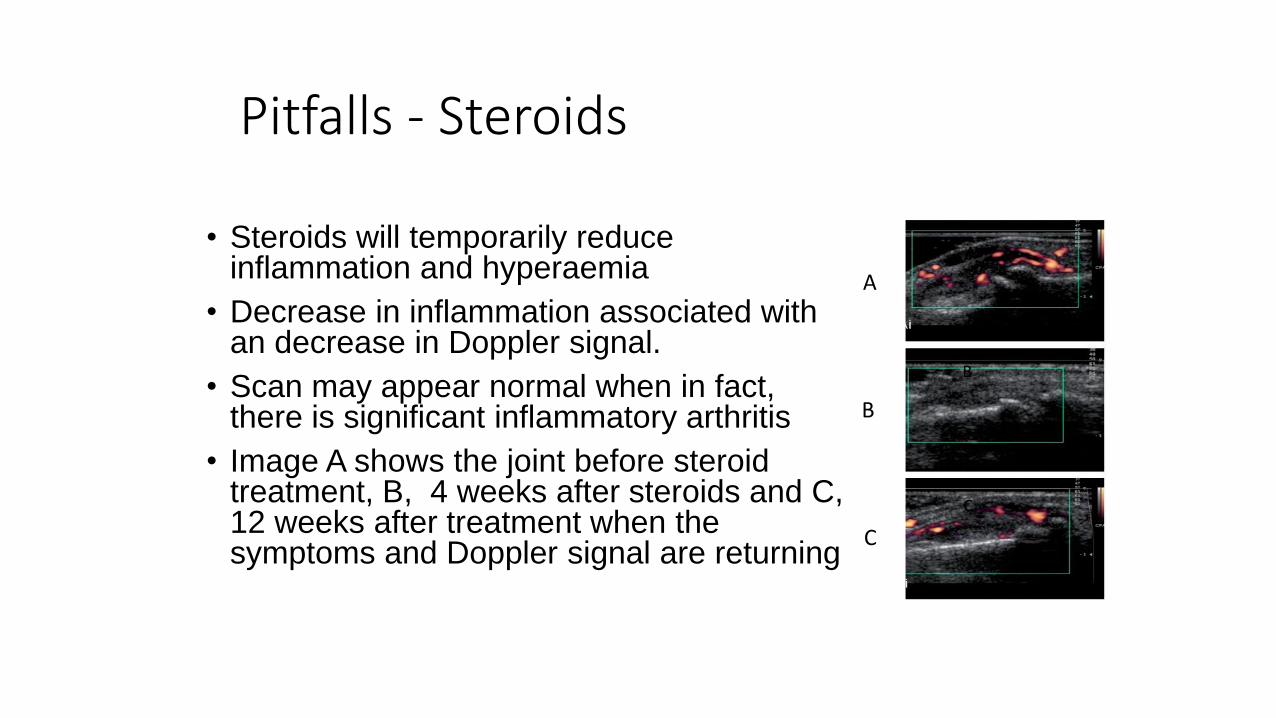
Pitfalls - Steroids
• Steroids will temporarily reduce inflammation and hyperaemia
• Decrease in inflammation associated with an decrease in Doppler signal.
• Scan may appear normal when in fact, there is significant inflammatory arthritis
• Image A shows the joint before steroid treatment, B, 4 weeks after steroids and C, 12 weeks after treatment when the symptoms and Doppler signal are returning
A
B
C
A
B
C
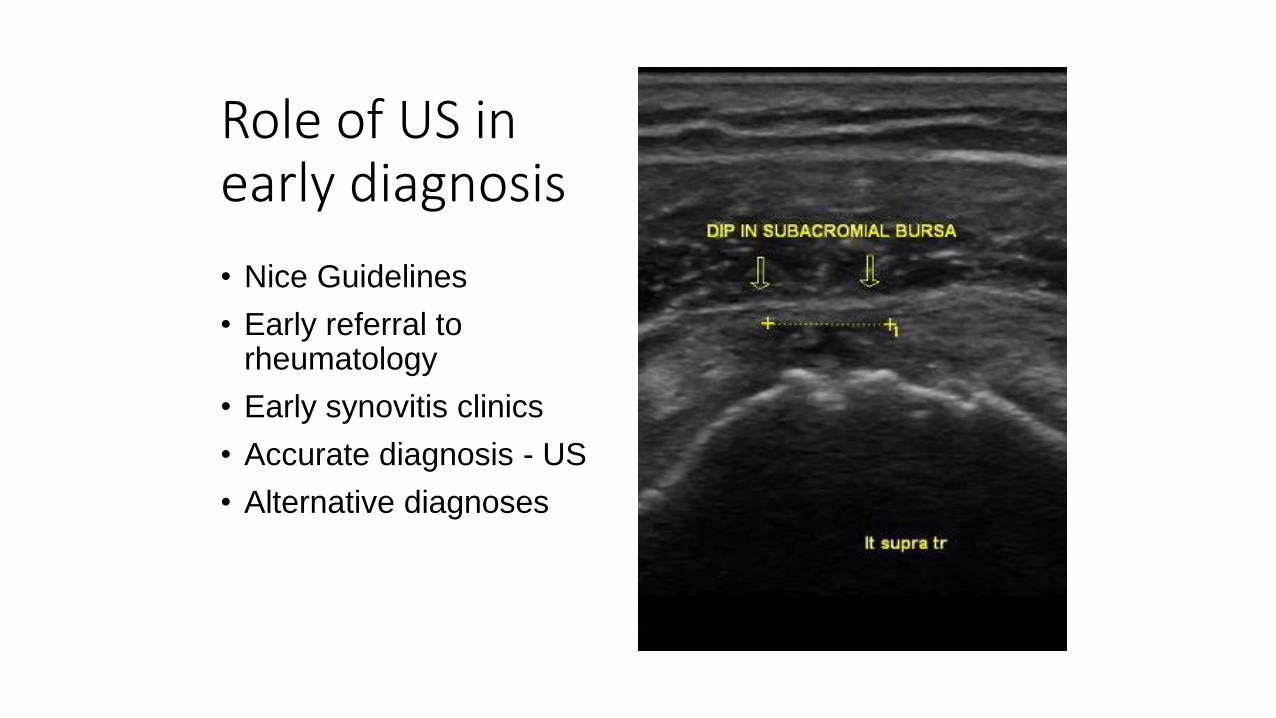
Role of US in early diagnosis
• Nice Guidelines
• Early referral to rheumatology
• Early synovitis clinics
• Accurate diagnosis - US
• Alternative diagnoses
Questions to ask the undiagnosed patient• Are you taking any steroids
or have had any steroid injections within the last 6 weeks?
• Where does it hurt?
• Is the pain bilateral?
• When does it hurt the most?
• Is it worse at any specific time of day or the more you do?
• Do you have psoriasis?
Clinical question
Patients without a diagnosis:
• Are there any inflammatory joint or soft tissue features?
• If so, where are they?
• Are there any features specific to a particular arthritis? RA, PsA, Crystal arthropathy
• If not, is there any other obvious cause for their symptoms? CTS, tumour, fracture
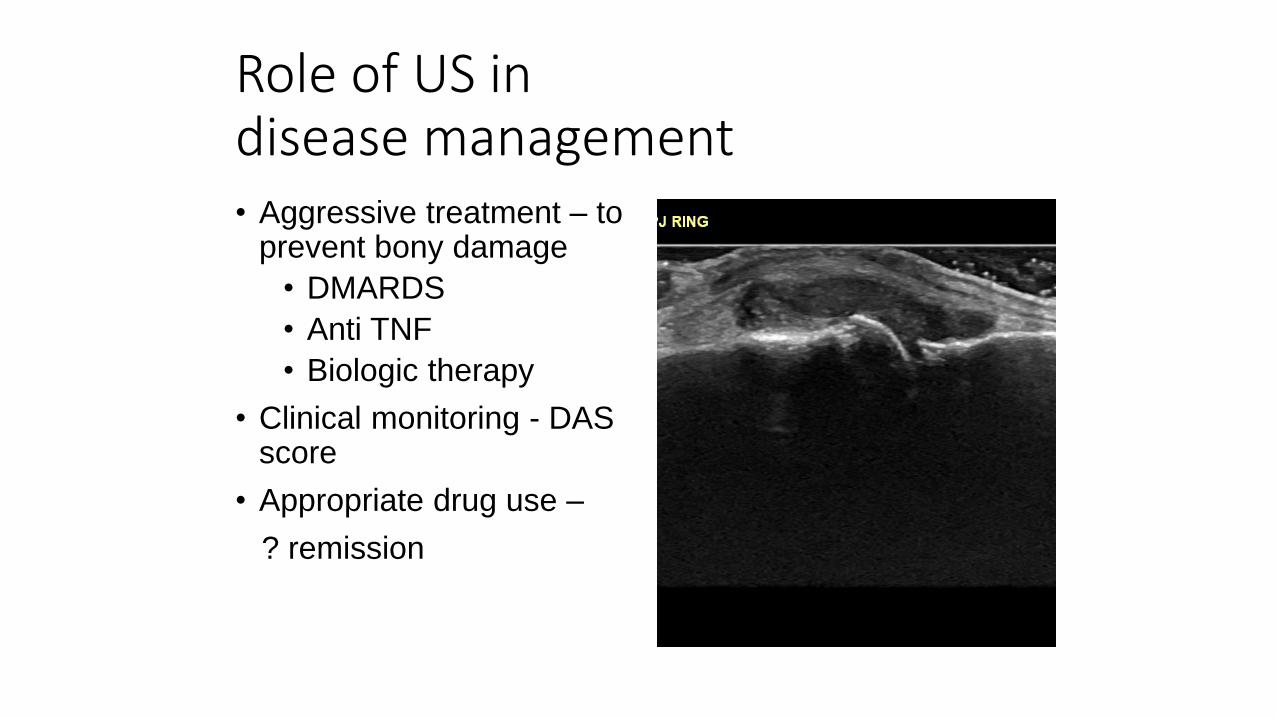
Role of US in disease management• Aggressive treatment – to
prevent bony damage
• DMARDS
• Anti TNF
• Biologic therapy
• Clinical monitoring - DAS score
• Appropriate drug use –
? remission
Clinical question
Patients with a diagnosis
• Is this patient active?
• Are there features of ongoing synovitis/tenosynovitis despite treatment?
• Do I need to increase/change drugs?
• Can I reduce drugs? Are they in remission
• Is the original diagnosis correct?
• State the question
• Answer it
• Use the correct anatomical names – index, middle etc rather than 2,3 etc
• Don’t assume…no need to conclude
• Suggest onward referral if appropriate
Reports
‘No evidence of active synovitis seen arising from the wrists or within the MCP or PIPjs. No tenosynovitis. No erosions seen.’
‘There is grade 2 active joint synovitis in the index and middle finger MCPjs bilaterally and arising from the right wrist. There is flexor tenosynovitis of the index and middle fingers on the left. No erosions seen. Ultrasound appearances would support a diagnosis of inflammatory arthritis and an urgent rheumatology opinion is suggested.’
Reports
Guided injections/aspirations
• To relieve pain• Steroid
• Local anaesthetic
• To enable mobility• As above
• Hyaluronic acid
• For diagnosis
• gout, infection
Take home messages…• GP requests – NICE guidelines
• Discuss with Rheumatology - grading
• Revise anatomy – bone and soft tissue, bursae and tendon sheaths
• Ask questions about drugs
• Suggest Rheumatology referral
• Use your wide MSK experience
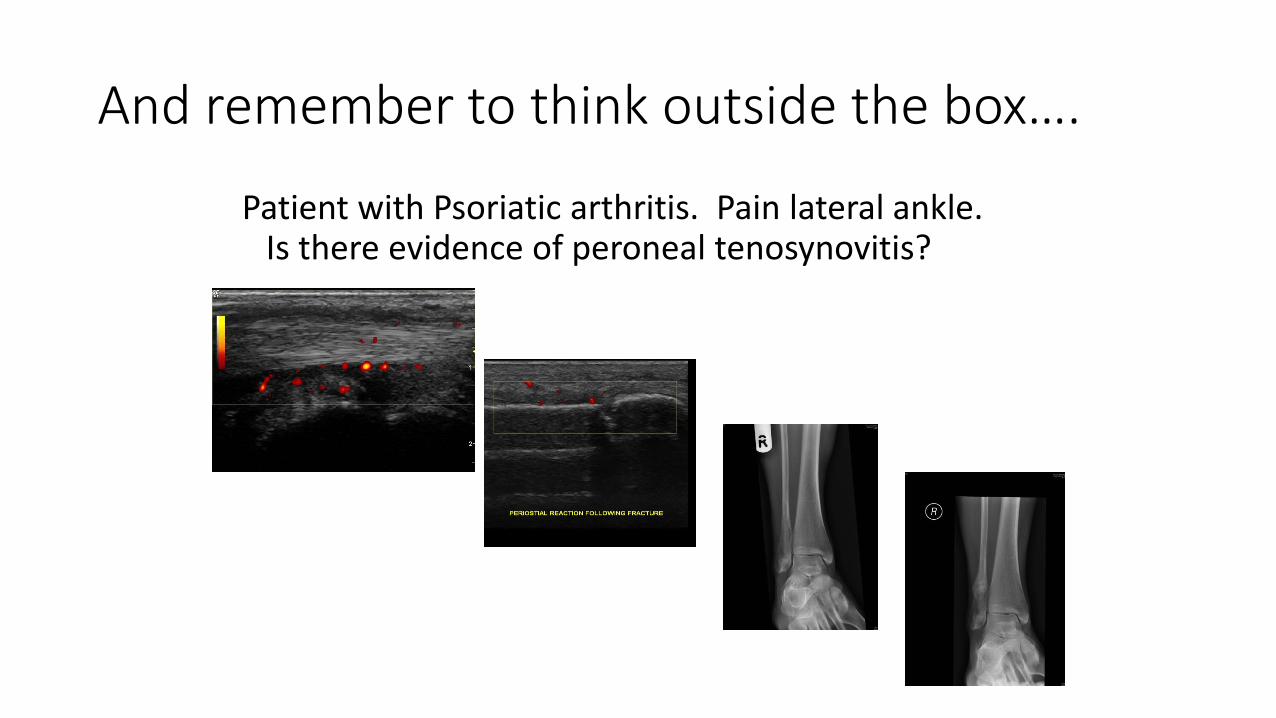
And remember to think outside the box….
Patient with Psoriatic arthritis. Pain lateral ankle. Is there evidence of peroneal tenosynovitis?
Any questions?

Thank you
Research Institute for Primary Care and Health SciencesDavid Wetherall Building Keele University Newcaslte-under-LymeST5 5BG Tel: 01782 733905Fax: 01782 734719www.keele.ac.uk/pchs
Useful referencesWakefield R J, Balint PV, Szkudlarek M, et al. Musculoskeletal ultrasound including definitions for ultrasonographic pathology. J Rheumatol 2005 ; 32 : 2485 – 7
Szkudlarek M , Court-Payen M, Jacobsen S, e t al. Interobserver agreement inultrasonography of the finger and toe joints in rheumatoid arthritis. Arthritis Rheum2003 ; 48 : 955 – 62
Naredo E , Bonilla G, Gamero F, et al. Assessment of inflammatory activity inrheumatoid arthritis: a comparative study of clinical evaluation with with grey scale and power Doppler ultrasonography. Ann Rheum Dis 2005 ; 64 : 375 – 81
Berner Hammer H et al . Examination of intra and interrater reliability with anew ultrasonographic reference atlas for scoring of synovitis in patients with rheumatoid arthritis. Ann Rheum Dis 2011;70:1995–1998
Wakefield RJ et al Musculoskeletal Ultrasound Including Definitions forUltrasonographic Pathology OMERACT SIG. Journal of Rheumatology 2005