Embed Size (px)
Citation preview

Understanding and Appraising the
New Medicine Service in England
A project funded by the Department of Health

2
Background to the NMS • 15 million patients in England have a long term medical condition, 813.3
million NHS prescriptions dispensed in 2009-10
• Adherence is poor in key prevalent diseases:
• COPD: 33% (Marsden, et al. 2009)
• Schizophrenia: 52% (Llorca 2008)
• Asthma: 67% (Cerveri, Locatelli et al. 1999)
• Diabetes: 78% (Ho, Rumsfeld et al. 2006)
• 15% people receiving a new medicine take few, if any, doses
sub-optimal medicines use (assuming appropriate Rx)
inadequate management of the LTC and poor outcomes
cost to the patient, the NHS and society
• Estimated opportunity cost (NHS England) of lost health gain from non-
adherence = £930 million p.a. in 5 diseases:(Trueman, Lowson et al. 2010)

3
Hello, it’s the pharmacist calling: an
economic evaluation of an intervention to
improve adherence
• Intervention: pharmacist telephoned 2 weeks after new Rx for chronic
illness to discuss medication
• Patients: Already on >3 medications: >74 or stroke, cardiovascular
disease, asthma, diabetes, RAs
• Results at 1 month follow-up
• Self-reported non-adherence: 8% versus 16% p=0.030
• medication related problems: 23% versus 34% p=0.019
• Mean total patient costs (NHS): £77.8 versus £113.9 p<0.05
Clifford S, Barber N, Elliott RA, Hartley E, Horne, R. P.W.S. 2006; 28: 165-170
Elliott RA, Clifford S, Barber N, Hartley E, Horne R. P.W.S. 2008; 30: 17-23

4
Cost effectiveness plane for adherence
intervention
SE quadrant

5
The New Medicine Service Service description
This service will provide support to people who are newly prescribed a medicine to
manage a long-term condition,* which will generally help them to appropriately
improve their medication adherence.
Aims and intended outcomes
The service should:
a) help patients and carers manage newly prescribed medicines for a LTC and
make shared decisions about their LTC
b) recognise the important and expanding role of pharmacists in optimising the use
of medicines
*asthma/COPD, hypertension, Type 2 diabetes or anticoagulation/antiplatelet
therapy
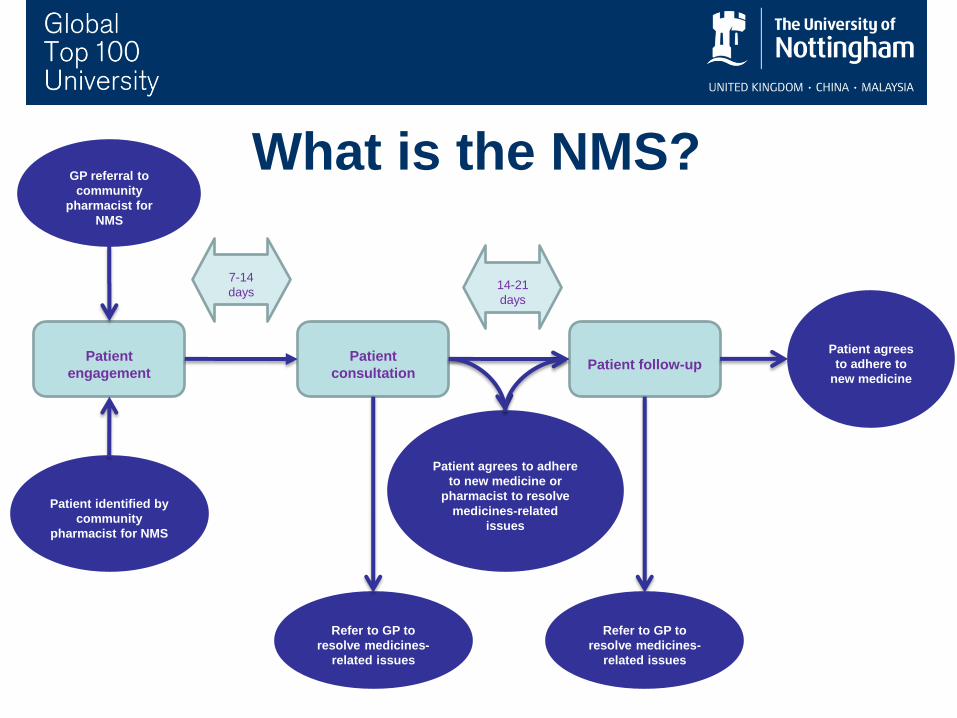
Patient
consultation
Patient
engagement Patient follow-up
GP referral to
community
pharmacist for
NMS
Patient identified by
community
pharmacist for NMS
Refer to GP to
resolve medicines-
related issues
7-14
days 14-21
days
Patient agrees to adhere
to new medicine or
pharmacist to resolve
medicines-related
issues
Patient agrees
to adhere to
new medicine
Refer to GP to
resolve medicines-
related issues
What is the NMS?

7
NMS Evaluation Study cast list Project Team
Nottingham: Tony Avery, Matthew Boyd (co PI), Loraine Buck, Chris Craig,
Rachel Elliott (co PI), Georgios Gkountouras, Asam Latif, Rajnikant Mehta,
Ndeshi Salema, Lukasz Tanajewski, Justin Waring, Deborah Watmough
London: Nick Barber, James Davies
PPI: Antony Chuter
Additional Patient Representation: Ember Vincent, Clancy Williams
NMS Evaluation Advisory Group: Nick Mays (chair), Alistair Buxton,
Sarah Clifford, Ailsa Donnelly, Alan Glanz, Sally Greensmith, Jeanette
Howe, Carmel Hughes, Danny Palnoch, Gil Shalom, Gary Warner

8

9
Primary objectives of appraisal
Evaluate the impact of the new medicines service (NMS) on
• patient medicines-taking behaviour,
• patient outcomes,
• and cost-effectiveness from an NHS perspective.
10
Technology Appraisal: RCT methods
• 504 participants from 47 pharmacies (EMSY/London)
• Aged >14, eligible for NMS, identified in a community pharmacy on
presentation of prescription for a new medicine for asthma/(COPD),
hypertension, type 2 diabetes or an anticoagulant/antiplatelet agent.
• Interventions: Randomised to NMS or current practice.
• Main outcomes: Adherence to new medicine 10 weeks post recruitment.
• The NMS question: ‘Since we last spoke have you missed any
doses of your new medicine, or change when you take it (prompt:
when did you last miss a dose)?’
• Morisky Medication Adherence Scale (MMAS-8)
• Also: EQ-5D 3L, NHS costs, BMQ
• Analysis: ITT, outcome adjusted for pharmacy clustering, NMS disease
category, age, sex and medication count, multiple imputation for missing
data.

11
Technology Appraisal: RCT results
• Follow up: At 10 weeks 85% patients contacted by telephone
(n=443), 60% of questionnaires were returned (n=321), 53 patients
withdrawn from study.
• Adherence:
In the unadjusted intention-to-treat analysis of 378 patients still taking
the initial medicine:
115/190 (60.5%) and 133/188 (70.7%) (p=0.037) patients were
adherent in the current practice and NMS arms, respectively, yielding
an odds ratio (95% CI) of 1.58 (1.03, 2.42, p=0.037).
In the adjusted analysis:
Adherence yielded an odds ratio (95% CI) of 1.67 (1.06, 2.62,
p=0.027), in favour of the NMS arm.

12
Technology Appraisal: RCT results
Health status:
• Mean (SD) EQ-5D at baseline and follow-up:
• current practice: 0.73 (0.28) and 0.75 (0.26);
• NMS 0.76 (0.28) and 0.77 (0.30).
NHS costs at 10 weeks:
• Mean (median, range) total NHS cost:
• Current practice: £260.87 (121.2, 0-1668.45)
• NMS: £215.16 (110.78,0-1458.7)
• Difference: £45.71 (95% CI: -33.41- 124.84, p= 0.1281).
• This difference reduces to £21.11 once the cost of the NMS
intervention is included.

13
Using economic evaluation to determine the
impact of a cross-therapeutic adherence
intervention
• Economic models can tell you the long term health consequences and
costs incurred by diseases and treatments.
• Need to understand (and therefore need data on):
• Disease and treatment pathways
• Probability of moving from one disease state to another, and the
effect of treatment on that
• The quality of life of a person in each disease state
• The costs of treating the person in each disease state
• Economic models are disease-specific
• Safety and adherence interventions are often cross-therapeutic
• Use of errors and adherence as proxy outcomes
• OR…………..

14
Economic evaluation
State 1 State 2
Death
Markov model*
Probability and resource use
data from trial Probability, resource use and utility
data from published sources *number and type of health states will depend on the disease/drug group

15
NMS economic models
• The resultant six treatment pathway models are:
• Hypertension-amlodipine
• Hypertension-ramipril
• Asthma-inhaled corticosteroid (beclometasone)
• COPD-tiotropium
• Diabetes-metformin
• Anticoagulants-aspirin
• Lifetime time horizon, NHS perspective
• Combined with
• effect size, age, disease severity, drug being prescribed and
health status from NMS RCT
• Proportion of disease groups covered by NMS
• Intervention costs
`

16
Hypertension-amlodipine model

17
Combining the data from the RCT and the
treatment pathway models
Model % NMS cohort
CCB* 25.3%
ACE* 24.1%
Aspirin 8.5%
Asthma 17.5%
COPD 5.8%
Diabetes 18.9%
Overall 100%
Adherence: 10-week ITT analysis
incorporating imputed missing values,
for MMAS-8 composite adherence
outcome: odds ratio, SD (NMS
vs.current practice): 1.81 (1.07, 3.05).
p [adherence] NMS group: 63.6%
p [adherence] current practice: 49.1%
Cost of NMS intervention: £24.60
Composite economic evaluation
Cost & QALY caused by
non-adherence from models

18
Incremental economic analysis
• NMS generated a mean of 0.06 (95%CI: 0.00, 0.16) more QALYs per patient, at a mean reduced cost of -£190 (95%CI: -929, 87).
• NMS dominates current practice, with an ICER (95% credibility range) of -£3 005 (-17 213, 4 543)

19
Incremental cost effectiveness ratio

20
Some qualitative findings (20 interviews)
• NMS consultations were found to be mutually respectful and polite
encounters with discussions generally centred on the new medicine
within which issues of use and adherence featured alongside other
health-related matters.
• Consultations were led from the onset by the pharmacist who routinely
dominated the discussion by asking most questions; patients were
found to ask fewer questions.
• For many pharmacists, their intention was to approach the NMS as an
information providing exercise, to support patient use of new
medicines.
• Not all pharmacists used the NMS interview schedule, for example
failing to ask about missed doses. As a consequence, opportunities to
discuss adherence in-depth were not always taken.

21
Some qualitative findings
• Not all pharmacists used the NMS interview schedule, for example
failing to ask about missed doses. As a consequence, opportunities to
discuss adherence in-depth were not always taken.
• Generally patients had poor awareness of what the NMS could offer
them and had low expectations beforehand. They were, however,
pleasantly surprised by the experience and reassurance provided for a
course of action.
• Occasionally patients took the opportunity to raise issues that
concerned them about the new medicine and also wider health related
issues. In these situations, pharmacists were flexible and
accommodated such discussions.
• 3 patients were referred to the GP following reported medicine side
effects. The pharmacist had been a valuable source of reassurance
that their side effect warranted medical attention. The NMS and the
pharmacist’s intervention provided legitimacy for stopping medication
and for them to see the GP about the matter.
Pharmacist: So I just wanted to see how you’re doing with that one [aspirin]. Patient: The problem is I’m not going to be able to continue taking them … Because they’re giving me a really bad stomach … I’ve already on a past occasion had seven days in hospital with quite a large stomach bleed that needed five units of blood … So I don’t know really what my options are. Pharmacist: No that’s fine. What we are going to do we are going to refer you back to the doctors … I can send a letter back to the doctors saying what side effects you are experiencing and I would advise you not to take the tablets any more …
[Consultation 169 (intervention) Aspirin

22
Conclusions
The New Medicine Service (NMS) launched in 2011 was effective at
improving patients’ adherence to their new medicine at 10 weeks follow up,
by about 10%.
There was no overall cost to the NHS of providing NMS as intervention
costs were absorbed by reduced subsequent NHS contact costs.
Although baseline adherence varied across disease groups, the NMS had a
fairly consistent effect on adherence across hypertension, asthma, COPD,
diabetes and treatment with anticoagulants and antiplatelets.
NMS increased health gain at a cost per QALY well below most accepted
thresholds for technology implementation, usually about £20,000 to £30,000
in the UK

![Appraising Complementary and Alternative Medicine in ... · PDF fileand Alternative Medicine or NCCAM] ... use of gadgets such as zapper, magnets, alkaline water ionizer, clustered](https://img.pdfslide.net/doc/110x75/5a78cb337f8b9a83238c8761/appraising-complementary-and-alternative-medicine-in-alternative-medicine-or.jpg)


























