Embed Size (px)
Citation preview
Understanding psychiatric advance directives and how they work
Acknowledgment: Support from the National Institute of Mental Health,
the John D. and Catherine T. MacArthur Foundation, the Greenwall Foundation,
and the National Resource Center on Psychiatric Advance Directives (NRC-PAD) www.nrc-pad.org
Jeffrey Swanson, PhD
Department of Psychiatry &
Behavioral SciencesDuke University
School of Medicine
Definitions and overview of Definitions and overview of psychiatric advance directives psychiatric advance directives (PADs) in the USA(PADs) in the USA PurposePurpose Features Features Origins Origins
Research on the effectiveness PADsResearch on the effectiveness PADs Barriers to PADs and how to overcome themBarriers to PADs and how to overcome them PAD completion and usePAD completion and use Treatment engagement and satisfactionTreatment engagement and satisfaction Crisis preventionCrisis prevention Reduction of coercive interventionsReduction of coercive interventions
Presentation OutlinePresentation Outline
What are psychiatric advance What are psychiatric advance directives?directives?
Psychiatric advance directives (PADs) are Psychiatric advance directives (PADs) are legal instruments that allow competent legal instruments that allow competent persons to document their decisions and persons to document their decisions and preferences regarding future mental health preferences regarding future mental health treatment and/or designate a surrogate treatment and/or designate a surrogate decisionmaker in the event they lose capacity decisionmaker in the event they lose capacity to make reliable treatment decisions during to make reliable treatment decisions during an acute episode of psychiatric illness. an acute episode of psychiatric illness.
Key features of PADsKey features of PADs Two legal types of PAD instruments; in many
states can be used separately or together 1. advance instructions1. advance instructions 2. proxy decisionmaker 2. proxy decisionmaker
PADs are device for advance communication (“forecasting”) treatment decisions (consent/refusal) preferences and values to guide future decisions emergency information portable “psychiatric resume”
Proscriptive and prescriptive functions
Limited waiver of confidentiality
Sometimes viewed as “self-commitment” or Sometimes viewed as “self-commitment” or “Ulysses contract”“Ulysses contract”
PADs are a variation on medical advance directives but with key differences . . .
assume restoration of capacityassume restoration of capacity patients informed by treatment experience patients informed by treatment experience mental-health-specific issues (e.g., mental-health-specific issues (e.g.,
avoiding involuntary treatment)avoiding involuntary treatment) and in Virginia, PADs are folded and in Virginia, PADs are folded
into a comprehensive health care into a comprehensive health care advance directive, combining advance directive, combining medical and mental health medical and mental health directives.directives.
Where did PADs come from?Where did PADs come from?
Driving factors in the USA in the 1990sDriving factors in the USA in the 1990s Medical advance directives and federal Medical advance directives and federal
lawlaw Supreme Court decision in 1990 Supreme Court decision in 1990 Cruzan v. Cruzan v.
Director, Missouri Department of HealthDirector, Missouri Department of Health required “clear and convincing evidence” of a required “clear and convincing evidence” of a
patient’s wishes in order to withdraw life-patient’s wishes in order to withdraw life-sustaining medical treatment.sustaining medical treatment.
Cruzan decision defined need for written Cruzan decision defined need for written documentation as evidence of incapacitated documentation as evidence of incapacitated patients’ treatment preferencespatients’ treatment preferences
Patient Self-Determination Act 1991Patient Self-Determination Act 1991 required hospitals receiving federal funds to required hospitals receiving federal funds to
ask patients if they had an advance directive ask patients if they had an advance directive on admission, and to have a policy for on admission, and to have a policy for implementing advance directivesimplementing advance directives
Where did PADs come from?Where did PADs come from?
Driving factors in the USA in the 1990sDriving factors in the USA in the 1990s Mental health advocates adapted advance Mental health advocates adapted advance
directives to the context of mental health directives to the context of mental health crises.crises.
Way for consumers to exert more control over Way for consumers to exert more control over own treatment.own treatment.
Avoid involuntary treatment.Avoid involuntary treatment. New emphases on recovery, patient-New emphases on recovery, patient-
centered care, and shared decisionmaking centered care, and shared decisionmaking in mental health services.in mental health services.
Family involvement in treatment Family involvement in treatment decisionmaking.decisionmaking.
Political collaboration: Protection & Political collaboration: Protection & Advocacy attorneys, state-level NAMI, and Advocacy attorneys, state-level NAMI, and mental health consumer advocacy mental health consumer advocacy organizations came together to support organizations came together to support PAD legislation in several states. PAD legislation in several states.

Increasing interest in PADs in Increasing interest in PADs in the US: the US:
new laws in 26 states since new laws in 26 states since 19911991 MONTANA
NEW JERSEY NORTH CAROLINA OREGON OHIO OKLAHOMA SOUTH DAKOTA TEXAS UTAH VIRGINIA WASHINGTON WYOMING NEW MEXICO
ALASKA ARIZONA HAWAII IDAHO INDIANA ILLINOIS KENTUCKY LOUISIANA MAINE MARYLAND MICHIGAN MINNESOTA PENNSYLVANIA
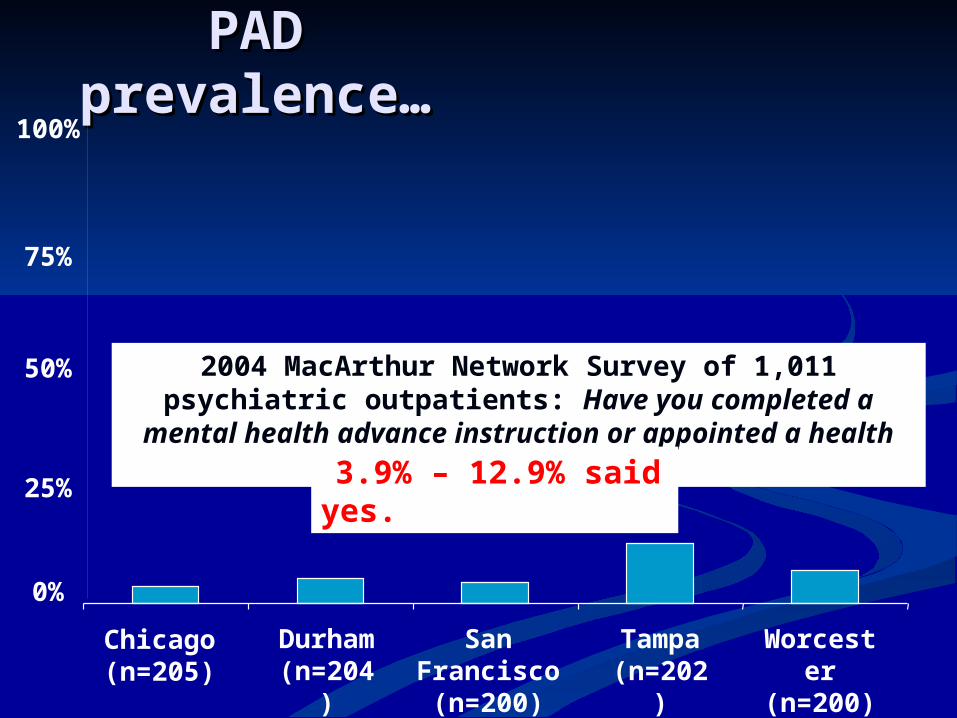
PAD PAD prevalence…prevalence…
Chicago
(n=205)
Durham
(n=204)
San Francisco(n=200)
Tampa
(n=202)
Worcester
(n=200)
2004 MacArthur Network Survey of 1,011 psychiatric outpatients: Have you completed a
mental health advance instruction or appointed a health care agent? 3.9% – 12.9% said
yes.
100%
50%
25%
75%
0%
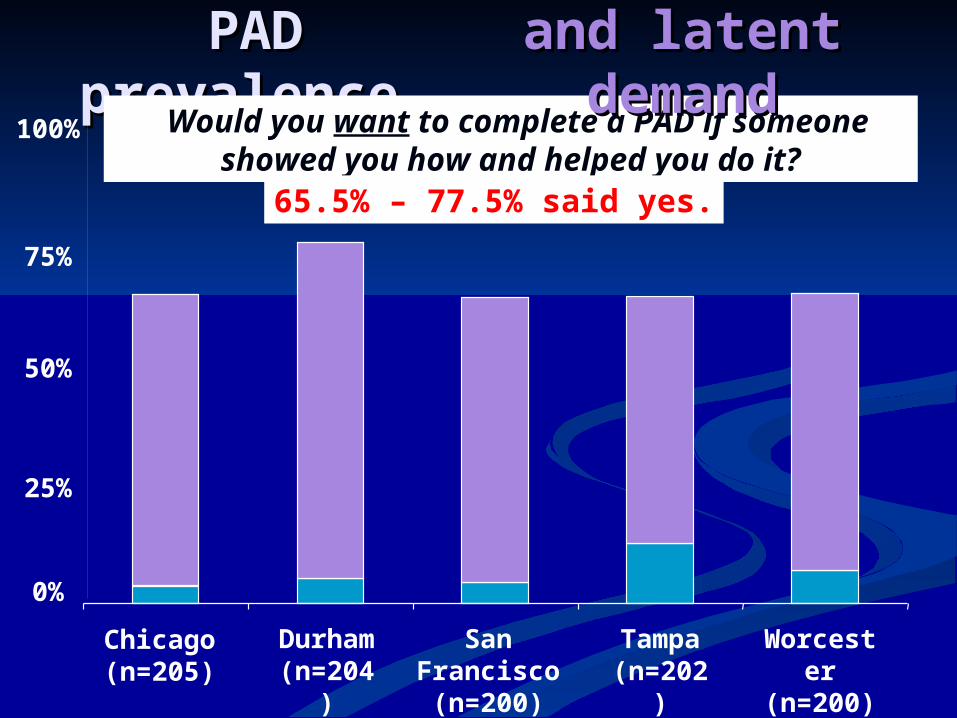
PAD PAD prevalence…prevalence…
Chicago
(n=205)
Durham
(n=204)
San Francisco(n=200)
Tampa
(n=202)
Worcester
(n=200)
Would you want to complete a PAD if someone showed you how and helped you
do it?
and latent and latent demanddemand
65.5% – 77.5% said yes.
100%
50%
25%
75%
0%
Research questionsResearch questions What are the barriers to PADs? What are the barriers to PADs?
Barriers to completion and useBarriers to completion and use Different barriers perceived by consumers Different barriers perceived by consumers
and cliniciansand clinicians
Does PAD facilitation work for Does PAD facilitation work for people with serious mental illness? people with serious mental illness?
Address barriers and help them complete Address barriers and help them complete PADs?PADs?
When consumers do complete When consumers do complete PADs, what do these documents PADs, what do these documents contain?contain?
Are PAD instructions feasible and Are PAD instructions feasible and consistent with clinical practice standards?consistent with clinical practice standards?
Do PADs work as intended? Do PADs work as intended? Might they have other, indirect benefits?Might they have other, indirect benefits?
What do clinicians think of What do clinicians think of PADs?PADs?
Survey of 591 North Carolina Survey of 591 North Carolina mental health professionals mental health professionals psychiatristspsychiatrists psychologistspsychologists social workerssocial workers
Knowledge and attitudes Knowledge and attitudes regarding PADs and perceived regarding PADs and perceived barriers to implementing PADsbarriers to implementing PADs
NC clinicians’ perceived barriers to NC clinicians’ perceived barriers to implementation of PADs implementation of PADs
Operational barriersOperational barriers lack of communication between staff across lack of communication between staff across
service sectors; inpatient/outpatient service sectors; inpatient/outpatient discontinuitydiscontinuity
lack of access to the document in a crisislack of access to the document in a crisis
Perceived clinical barriersPerceived clinical barriers inappropriate treatment requests/refusalsinappropriate treatment requests/refusals consumers’ desire to change their mind about consumers’ desire to change their mind about
treatment during crisestreatment during crises concerns with competency to complete concerns with competency to complete
documentdocument
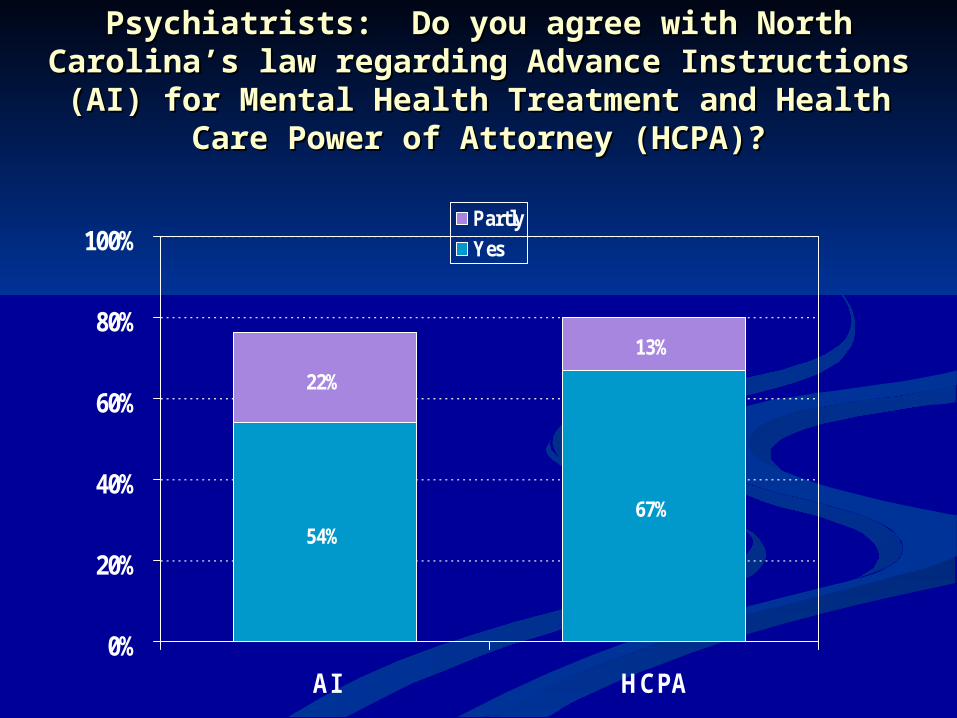
Psychiatrists: Do you agree with North Carolina’s law regarding Psychiatrists: Do you agree with North Carolina’s law regarding Advance Instructions (AI) for Mental Health Treatment and Advance Instructions (AI) for Mental Health Treatment and
Health Care Power of Attorney (HCPA)?Health Care Power of Attorney (HCPA)?
54%67%
22%
13%
0%
20%
40%
60%
80%
100%
AI HCPA
Partly
Yes
Psychiatrists’ support for Psychiatrists’ support for PADs increases significantly PADs increases significantly when they are aware that the when they are aware that the law does not require them to law does not require them to follow advance instructions follow advance instructions when those instructions when those instructions deviate from accepted deviate from accepted clinical standards of care.clinical standards of care.
Importance of having accurate Importance of having accurate knowledge of the law’s actual knowledge of the law’s actual
provisions regarding clinicians’ provisions regarding clinicians’ compliance with PADscompliance with PADs
Design of core study: Effectively Design of core study: Effectively Implementing PADs (R01 MH63949 Implementing PADs (R01 MH63949
and and
MacArthur Network funded)MacArthur Network funded) Enrolled sample of 469 persons with serious Enrolled sample of 469 persons with serious
mental illnessmental illness from 2 county outpatient mental from 2 county outpatient mental health centers and 1 regional state psychiatric health centers and 1 regional state psychiatric hospital in North Carolinahospital in North Carolina
Random assignment:Random assignment: 1. Experimental group: Facilitated Psychiatric Advance 1. Experimental group: Facilitated Psychiatric Advance
Directive (F-PAD) (n=239)Directive (F-PAD) (n=239) 2. Control group: receive written information about PADs 2. Control group: receive written information about PADs
and referral to existing resources (n=230)and referral to existing resources (n=230) Structured interview assessmentsStructured interview assessments at baseline, 1 at baseline, 1
month, 6 months, 12 months, 24 months; record month, 6 months, 12 months, 24 months; record reviewsreviews
Short-term outcomesShort-term outcomes PAD completion rate; change in PAD completion rate; change in
perceived barriers to completionperceived barriers to completion PAD document structure & contentPAD document structure & content
Intermediate outcomesIntermediate outcomes Outpatient treatment engagementOutpatient treatment engagement Working alliance with cliniciansWorking alliance with clinicians
Long-range outcomesLong-range outcomes Frequency of mental health crisesFrequency of mental health crises Reduction of coercive crisis Reduction of coercive crisis
interventions and involuntary interventions and involuntary treatment treatment
PAD study outcomesPAD study outcomes
Consumers’ perceived Consumers’ perceived barriers to completing barriers to completing
PADsPADs Did not understand enough about PADs. Did not understand enough about PADs. Difficult to find someone or somewhere Difficult to find someone or somewhere
to get help to complete the PAD. to get help to complete the PAD. Did not know what to write in the PAD. Did not know what to write in the PAD. Did not have anyone they trusted enough Did not have anyone they trusted enough
to make decisions for them. to make decisions for them. Did not have a doctor they trusted. Did not have a doctor they trusted. Did not like to sign legal documents (or Did not like to sign legal documents (or
did not trust legal documents). did not trust legal documents).
85% percent endorsed at least one barrier55% reported 3 or more of the barriers
F-PAD designed as a structured but flexible F-PAD designed as a structured but flexible
session to provide orientation to PADs and session to provide orientation to PADs and direct assistance:direct assistance: gather information or input from requested gather information or input from requested
sources (e.g., clinician, family)sources (e.g., clinician, family) guided discussion of treatment choicesguided discussion of treatment choices complete statutory formscomplete statutory forms appoint proxy decisionmakerappoint proxy decisionmaker obtain witnesses & notarizationobtain witnesses & notarization file document in medical records (clinic, file document in medical records (clinic,
hospital)hospital) register document with national and state register document with national and state
electronic registrieselectronic registries PAD alert braceletPAD alert bracelet Provide consultation about PAD to proxy Provide consultation about PAD to proxy
and clinicianand clinician
Facilitated Psychiatric Advance Directive Facilitated Psychiatric Advance Directive (F-PAD) Intervention(F-PAD) Intervention
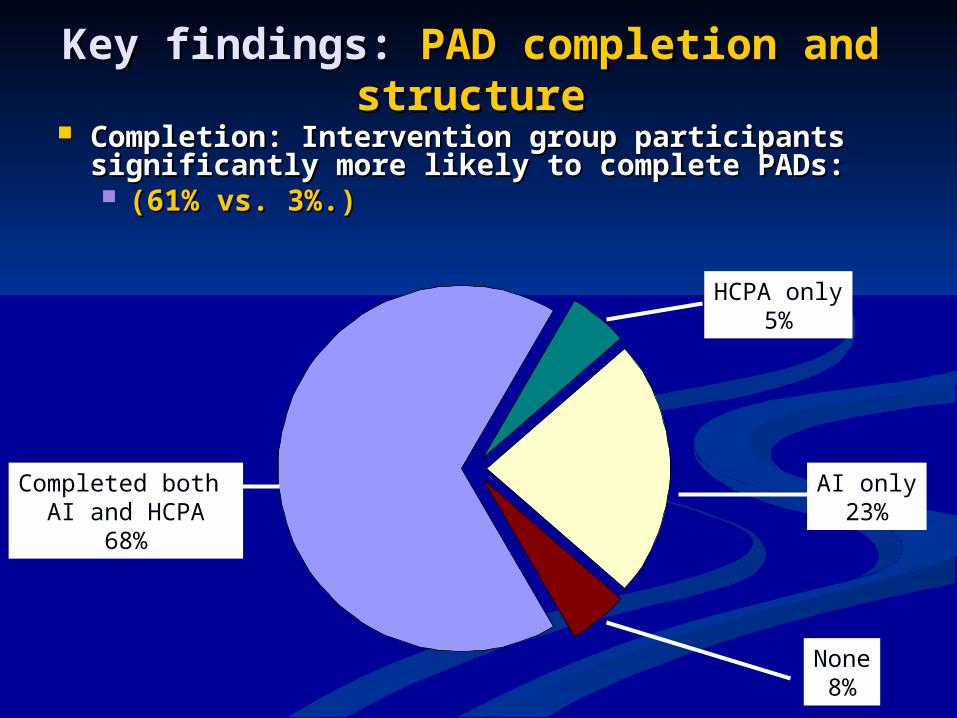
Key findings: Key findings: PAD completion and PAD completion and structurestructure
Completion: Intervention group participants Completion: Intervention group participants significantly more likely to complete PADs: significantly more likely to complete PADs: (61% vs. 3%.) (61% vs. 3%.)
None8%
AI only23%
Completed both AI and HCPA
68%
HCPA only5%
Key findings: Key findings: PAD PAD completion and document completion and document
content (cont.)content (cont.) Prescriptive vs. proscriptive functionPrescriptive vs. proscriptive function
Almost all PADs included treatment requests as Almost all PADs included treatment requests as well as refusals, but no participant used a PAD well as refusals, but no participant used a PAD to refuse all medications and/or treatment. to refuse all medications and/or treatment.
Concordance with standard careConcordance with standard care PAD instructions were systematically rated by PAD instructions were systematically rated by
psychiatrists, and mostly found to be feasible psychiatrists, and mostly found to be feasible and consistent with clinical practice standards.and consistent with clinical practice standards.
PAD content: PAD content: Relapse Relapse FactorsFactors
All subjects listed at least one All subjects listed at least one risk factor for relapse risk factor for relapse (median=3).(median=3).
58% specified nonadherence with 58% specified nonadherence with medication or other treatment as medication or other treatment as a relapse factor.a relapse factor.
20% described detailed 20% described detailed behavioral patterns of behavioral patterns of decompensation.decompensation.
PAD content: PAD content: Crisis Crisis SymptomsSymptoms
98% of subjects listed at least one 98% of subjects listed at least one crisis symptom they wanted to crisis symptom they wanted to communicate to inpatient doctors communicate to inpatient doctors (median=5). (median=5).
21% listed aggression/anger as crisis 21% listed aggression/anger as crisis symptomsymptom
24% listed self-harm or suicidal 24% listed self-harm or suicidal ideation as crisis symptomideation as crisis symptom
PAD content: PAD content: MedicationsMedications
94% gave advance consent to 94% gave advance consent to treatment with at least one treatment with at least one psychotropic medication.psychotropic medication.
77% refused some medication.77% refused some medication. 76% gave reasons76% gave reasons 72% listed side effects for refused meds72% listed side effects for refused meds
No participant refused all medications No participant refused all medications and or treatment. and or treatment.
PAD content: PAD content: HospitalsHospitals
88% gave advance consent to 88% gave advance consent to hospitalization in at least one specified hospitalization in at least one specified facilityfacility
However, 62% also documented advance However, 62% also documented advance refusals of admission to particular refusals of admission to particular hospitals hospitals 51% gave reasons, such as, “I do not wish to 51% gave reasons, such as, “I do not wish to
go back to that hospital, I was thrown in a go back to that hospital, I was thrown in a dark room and am scared and was hurt by dark room and am scared and was hurt by another patient last time.” another patient last time.”
PAD content: PAD content: Other Other InformationInformation
52% wrote instructions to staff on ways to 52% wrote instructions to staff on ways to avoid or reduce reliance on restraints and avoid or reduce reliance on restraints and seclusions.seclusions.
62% refused ECT under any circumstance. 62% refused ECT under any circumstance. 72% of the sample listed a history of side 72% of the sample listed a history of side
effects to particular medications.effects to particular medications. 16% listed additional medical conditions 16% listed additional medical conditions
they wanted providers to be aware of (e.g., they wanted providers to be aware of (e.g., diabetes, hypothyroidism, hypertension). diabetes, hypothyroidism, hypertension).
28% of subjects also documented 28% of subjects also documented medication and/or food allergies.medication and/or food allergies.
Do PADs work?Do PADs work?
Key findings: Key findings: outpatient outpatient treatment engagementtreatment engagement
At 1 month follow-up, F-PAD At 1 month follow-up, F-PAD participants:participants: Significantly greater positive change in Significantly greater positive change in
working alliance with case managers and working alliance with case managers and clinicians (adjusted odds ratio=1.67)clinicians (adjusted odds ratio=1.67)
Significantly more likely to report Significantly more likely to report receiving mental health services they felt receiving mental health services they felt they needed (adjusted odds ratio=1.57)they needed (adjusted odds ratio=1.57)
Key findings: Key findings: outpatient outpatient treatment engagement treatment engagement
(cont.)(cont.) At 6 months follow-up, PAD completers hadAt 6 months follow-up, PAD completers had
Significantly greater improvement on treatment Significantly greater improvement on treatment satisfaction scale (Mental Health Support Programsatisfaction scale (Mental Health Support Program—MHSP—scale)—MHSP—scale) Adjusted odds ratio=1.71 for top quartileAdjusted odds ratio=1.71 for top quartile ““As the result of services I received, I deal more As the result of services I received, I deal more
effectively with daily problems…I am better able effectively with daily problems…I am better able to control my life…I am getting along better with to control my life…I am getting along better with my family…I do better in school and/or work.” my family…I do better in school and/or work.”
Key findings: Key findings: outpatient outpatient treatment engagement treatment engagement
(cont.)(cont.) At 6 months follow-up, PAD completers hadAt 6 months follow-up, PAD completers had
higher utilization of outpatient services higher utilization of outpatient services medication management visits (probability medication management visits (probability
41% vs. 33% per month)41% vs. 33% per month) outpatient crisis outpatient crisis preventionprevention visits (probability visits (probability
19% vs. 10% per month) 19% vs. 10% per month) At 12 months, PAD completers had significantly At 12 months, PAD completers had significantly
increased concordance between requested and increased concordance between requested and prescribed meds.prescribed meds.
Key findings: Key findings: prevention of prevention of crises and coercioncrises and coercion
By 6 months follow-up, PAD completers had By 6 months follow-up, PAD completers had fewer crisis episodes (adjusted odds fewer crisis episodes (adjusted odds ratio=0.46)ratio=0.46)
At 24 months, PAD completers had reduced At 24 months, PAD completers had reduced likelihood of coercive crisis interventions likelihood of coercive crisis interventions (adjusted odds ratio=0.50)(adjusted odds ratio=0.50)
Controlled (weighted) for propensity to Controlled (weighted) for propensity to complete PAD.complete PAD.
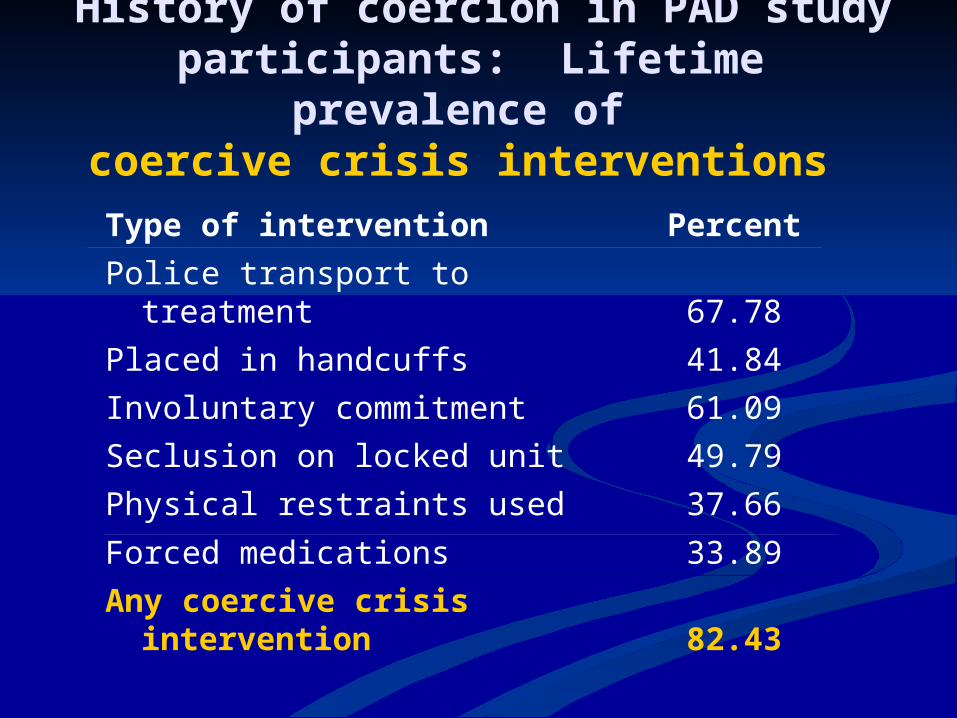
History of coercion in PAD study participants: Lifetime prevalence
of coercive crisis interventions
Type of intervention Percent
Police transport to treatment 67.78
Placed in handcuffs 41.84
Involuntary commitment 61.09
Seclusion on locked unit 49.79
Physical restraints used 37.66
Forced medications 33.89
Any coercive crisis intervention 82.43
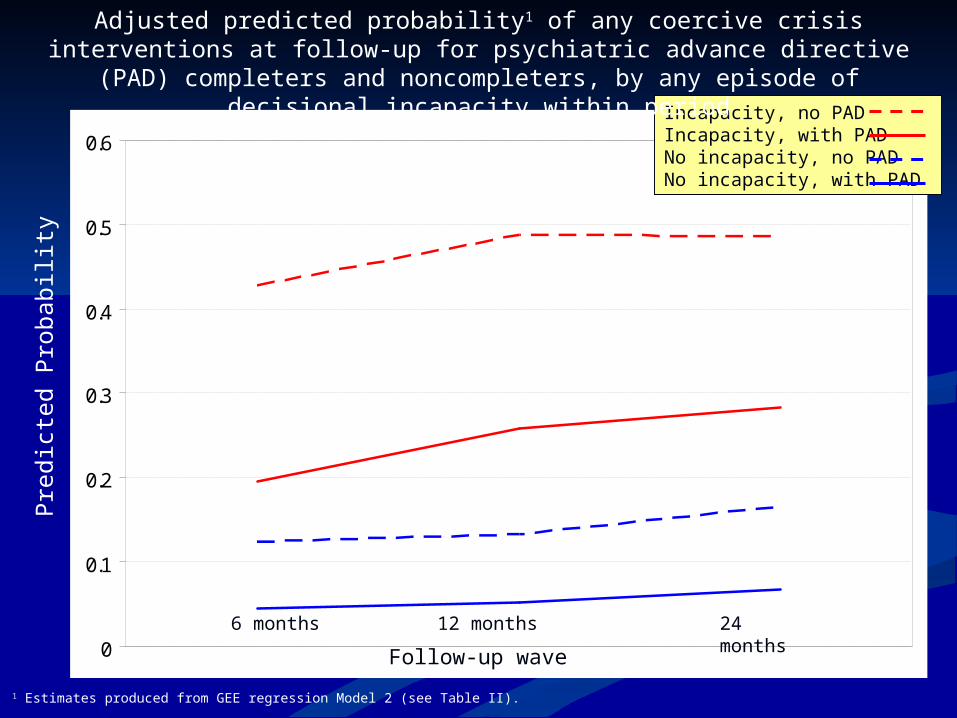
Pred
icte
d P
roba
bili
ty
0
0.1
0.2
0.3
0.4
0.5
0.6Incapacity, no PAD Incapacity, with PADNo incapacity, no PADNo incapacity, with PAD
Follow-up wave
12 months 24 months
6 months
Adjusted predicted probability1 of any coercive crisis interventions at follow-up for psychiatric advance directive (PAD) completers and noncompleters, by any episode of
decisional incapacity within period
1 Estimates produced from GEE regression Model 2 (see Table II).
Summary of key findingsSummary of key findings
Large latent demand but low completion of Large latent demand but low completion of psychiatric advance directives among psychiatric advance directives among public mental health consumers in the USApublic mental health consumers in the USA
Structured facilitation (F-PAD) can Structured facilitation (F-PAD) can overcome most of these barriers: Most overcome most of these barriers: Most consumers offered facilitation complete consumers offered facilitation complete legal PADs. legal PADs.
Completed facilitated PADs tend to contain Completed facilitated PADs tend to contain useful information and are consistent with useful information and are consistent with clinical practice standards clinical practice standards
Summary of key findings Summary of key findings (cont.)(cont.)
Even though PADs are designed legally to Even though PADs are designed legally to determine treatment during determine treatment during incapacitating crises, they can have an incapacitating crises, they can have an indirect benefit of improving engagement indirect benefit of improving engagement in outpatient treatment process.in outpatient treatment process.
PADs can help prevent crises as well as PADs can help prevent crises as well as reduce the use of coercion when crises reduce the use of coercion when crises occur.occur.
Cooperation from clinicians and Cooperation from clinicians and systematic implementation is needed in systematic implementation is needed in order for PADs to succeed.order for PADs to succeed.
www.nrc-pad.org
www.nrc-pad.org