Embed Size (px)
Citation preview
Understanding Substance Abuse & Addiction:What Research, Psychology & Medicine Have to Teach Us
TRUST Clinic Speaker SeriesOakland, Ca. June 20, 2014
Joan Zweben, Ph.D. Executive Director, East Bay Community Recovery
Projectwww.EBCRP.org
Clinical Professor of Psychiatry, UCSF
Disclosures Dr. Zweben has no conflict of interest to
disclose. Dr. Zweben’s bias is that evidence-
supported, safe treatment for SUDS should be equally available throughout our system of care, including medication treatment.
Dr. Zweben’s bias is that evidence-based interventions are only one component of individualized treatment planning, not a substitute for comprehensive care.
Evolution of Substance Abuse Treatment in the U.S.
How Did We Get Here?
National Institute on Alcoholism & Alcohol Abuse (NIAAA)
Founded 1970 as a center within NIH
Research on the biology of alcoholism, psychosocial issues, treatment (1990’s)
Produced educational materials for prevention, but initially not a leader in the treatment field.
Pressure from community groups led to more treatment research
National Institute on Drug Abuse (NIDA)
Founded 1972 to promote creation of tx system + research on clinical issues
Goal: what programs were contributing to reducing social costs of addiction
Tx system developed for the indigent (uninsured), funded by federal, state and local entities
Research emphasis on tx modalities

Chronology AA – 1935. Bill Wilson, Dr. Bob Smith in
Akron, Ohio Minnesota Model – 1950’s (Hazelden) Therapeutic Communities – 1958,
Synanon; proliferated rapidly Methadone maintenance – 1965, Dole &
Nyswander Drug Courts 1989, Miami-Dade County,
Florida
Treatment Modalities:Therapeutic CommunitiesTreatment Modalities:Therapeutic Communities long term (6-18 months)
residential tx the community is the agent of
change peer relationships, open
communication and feedback are basic tools
“must function” model activities to maintain daily
operations a primary element in therapeutic interactions

TC’s, ContinuedTC’s, Continued
change self-image and behavior self-examination and confession extended family concept possibility of ascendancy within
the system re-entry outcome data supports its efficacy
Methadone MaintenanceMethadone Maintenance
most misunderstood, stigmatized modality
most highly regulated modality rationale for maintenance therapy: Dole,
receptor system dysfunction strong empirical support for efficacy and
safety (50 years of data) valuable tool in reducing the spread of
AIDS not a cure-all, but makes the patient
accessible to intervention for other problems
Opioid Maintenance Therapy: Hot Button IssuesOpioid Maintenance Therapy: Hot Button Issues
Dosing: politics, blood levels, etc. Diversion Opioid addicted pregnant women Medical maintenance Tapering off methadone Methadone “vs” buprenorphine
“vs” naltrexone (Vivitrol)
Minnesota ModelMinnesota Model
Hazelden, Wilmar (1950’s) AA principles replace mental
health model; alcoholism as a primary disorder
multidisciplinary team approach respect for the alcoholic; respite
from environment need and value of aftercare
Minnesota ModelContinuedMinnesota ModelContinued
origin of 28-day length of stay CATOR: document outcomes controlled studies do not support
efficacy, with some exceptions managed care
Social/Community ModelSocial/Community Model
Influence on treatment & prevention
Emphasis on the micro & macro community
AA principles Experiential knowledge essential;
everyone both gives and receives help
Positive sober environment is crucial
One ancestor of ROSC
Drug Courts (1)Drug Courts (1)Goal: integrate substance abuse
treatment with legal case processing (pretrial)
K EY PRINCIPLES: Identification/referral as soon as
possible after arrest Early professional dx of treatment needs Matching needs to appropriate tx
Drug Courts (2)Drug Courts (2) Making treatment a court-monitored
requirement; provide judicial review and supervision of progress in treatment
Holding defendants accountable through a series of graduated sanctions and rewards
Providing appropriate follow-up and support services following treatment
(Sherin & Mahoney, 1996; TIP #23)
Drug Courts (3)Drug Courts (3) NIJ (2003) study of 17,000 graduates
found only 16.4% had been rearrested and charged with a felony one year later (Roman et al, 2003).
Reduced cost to victim and criminal justice system
Increase retention in treatment Others: juveniles, DWI, family, mental
health (Huddleston et al, 2004)
Treatment PhilosophiesTreatment Philosophies

Treatment Philosophies: AbstinenceTreatment Philosophies: Abstinence
abstain from drug of choice abstain from other intoxicants
drug substitutionrole in precipitating relapse
dependable control not possible; hence detach
widest margin of safety
What is Abstinence? A person is abstinent if he/she is
not drinking or using illicit drugs, and using legal ones as prescribed. Thus, medications are compatible with recovery.
Physical dependence ≠ addiction Note: medications are tools, not
solutions

Treatment Philosophies:Harm ReductionTreatment Philosophies:Harm Reduction
“Harm reduction is a set of strategies that encourage substance users and service providers to reduce the harm done to drug users, their loved ones and communities by their licit and illicit drug use.”
The Harm Reduction Working Group & Coalition, 1995
Arenas for Harm ReductionArenas for Harm Reduction
HIV/ STD outreach and education needle exchange homeless populations: wet, damp housing SMI clients - Harborview model methadone maintenance (damage control
component) drop in centers users’ support groups money management/payee community HR education
Pitfalls of Abstinence-Oriented TreatmentPitfalls of Abstinence-Oriented Treatment Failure to assess motivation level before
pushing abstinence commitment Failure to understand factors promoting
continued use Unrealistic timetables Power struggle vs clinical approach Failure to recognize fluctuating
motivation Inappropriate termination of treatment

Pitfalls of Harm Reduction ApproachPitfalls of Harm Reduction Approach
Inappropriately low expectations for what client can achieve
Difficulty setting clear goals Reluctance to ask client to abstain
completely Underestimate risks/lethality Clinician alcohol and/or illicit drug
use

The Substance Abuse Treatment System: Finding Good Care
The Substance Abuse Treatment System: Finding Good Care

Paradigm Shift
Chronic Care Model: When treated as a chronic illness, relapse rates are as good or better than other chronic illnesses (McLellan et al. 2005)
Recovery Oriented System of Care (ROSC): Support person centered and self-directed approaches to care that build on the strengths and resilience of individuals, families and communities to take responsibility for their sustained health, wellness and recovery from alcohol and drug problems (CSAT)
(Rawson & Freese. 2010)25
Recovery Oriented System of Care (ROSC)
ROSCs are founded on a chronic care model of substance use treatment and recovery services that use recovery management approaches to engage and treat, and provide recovery support services that help individuals/families sustain their recovery.
(Rawson & Freese. 2010)
26


Broadening Our Target Population
The Changing Health Care Landscape
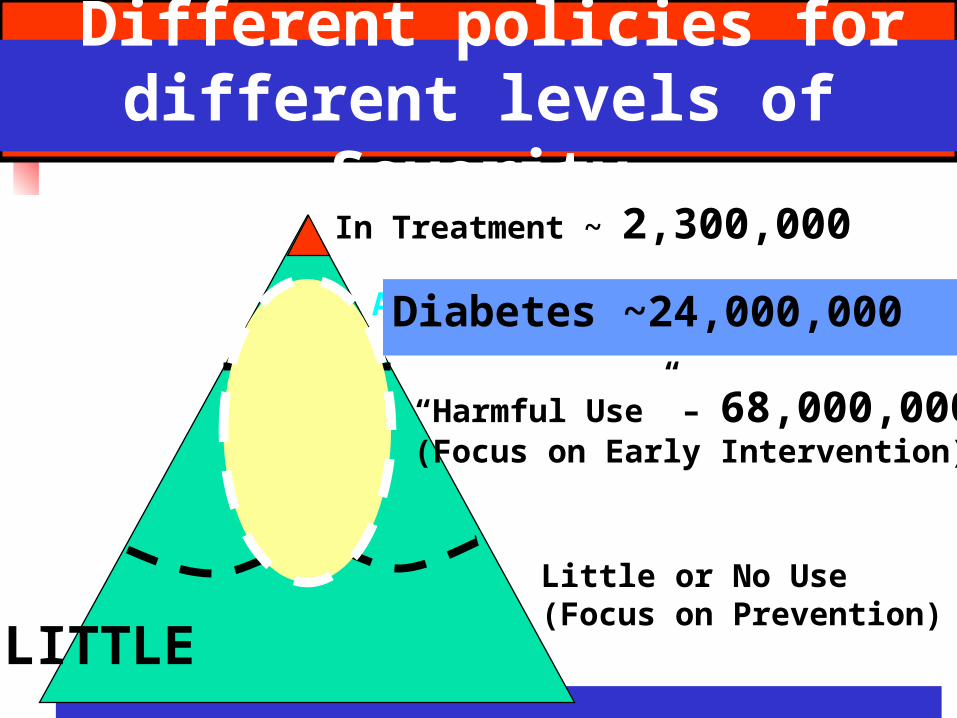
Different policies for different levels of
Severity
Addiction ~ 25,000,000(Focus on Treatment)
“Harmful Use” – 68,000,000(Focus on Early Intervention))
Little or No Use(Focus on Prevention))
Diabetes ~24,000,000
LITTLE
LOTS In Treatment ~ 2,300,000

Distribution of AOD Problems
2M people (.08%) receiving treatment
21M people (7%) have problems but are not receiving treatment 1.1% made effort to get tx 3.7% felt they needed tx but made no
effort to get it 95.2% did not feel they needed tx
60-80 M (20-25%) using at risky levels
(UCLA/ATTC
2013)
Using at Risky Levels (60-80 million)
Do not meet diagnostic criteria Level of use indicates risk of
developing problems Examples:
Drinks 3-4 glasses of wine several times per week Pregnant woman occasionally uses vodka to relieve
stress Adolescent to smokes mj with friends on weekends Occasionally takes 1-2 extra vicodin to help with pain
(UCLA/ATTC 2013)
ImplicationsAs long as the specialty care programs (AOD treatment programs) are the only places which address SUD: most people with severe problems will
not receive treatment. virtually all with risky use will not
receive professional attention.(UCLA-ATTC 2013)

Value of Behavioral Health
Source: Wyatt Matas, 2013
Value of Behavioral Health
49% of Medicaid Beneficiaries with disabilities have a psychiatric illness. Top 3 behavioral dyads: 1. Psychiatric/Cardiovascular 2. Psychiatric/Central Nervous System 3. Psychiatric/ Pulmonary
Healthcare Settings for Locating Individuals with SUD Primary care settings Emergency rooms/
Trauma centers Prenatal clinics/OB/Gyn offices Medical specialty settings for
diabetes, liver and kidney disease, transplant programs
Pediatrician offices College health centers Mental health settings
(UCLA-ATTC 2013)
Workforce Implications MH/AOD clinicians will be working in
many different settings where teamwork is key
Holistic, integrative perspective and approach; Sick care + wellness care
Screening & brief intervention integral
MI principles and skills essential Availability for drop in or scheduled
meetings; “hallway consults”
Evidence-Based Practices and Treatment Interventions
Evidence-Based Practices and Treatment Interventions
Rationale, Challenges & Perils
Why Use Evidence-Based Principles and Practices?Why Use Evidence-Based Principles and Practices?
To go beyond our preferences and biases
To improve the effectiveness of what we do: what works best, for whom
Because funders will increasingly insist on optimum utilization of inadequate resources
Evidence Based Principles & Practices vs Evidence Based Treatment Interventions
Evidence Based Principles & Practices vs Evidence Based Treatment Interventions
Principles and practices are derived from different types of research.
Rigor often trumps relevance in determining what type of research is valued.
Policy makers must be educated on these issues.
Important DistinctionsImportant Distinctions Evidence-based principles and
practices guide system development Example: care that is appropriately
comprehensive and continuous over time will produce better outcomes
Evidence-based treatment interventions are important elements in the overall picture. They are not a substitute for overall adequate care.
Types of StudiesTypes of Studies
Quasi-experimental studies – some control over confounding factors; less rigorous than RCT’s
Correlational studies – systematic observation across cases or programs
Longitudinal studies Naturalistic studies
Evidence-Based PrinciplesEvidence-Based Principles Retention improves outcomes; we need to
engage people, not discharge them prematurely.
Addicts/alcoholics are a heterogeneous population, not a particular personality type.
Addiction behaves like other chronic disorders Problem-service matching strategies improve
outcomes. (Other matching strategies disappointing.)
Harm reduction approaches yield benefits in terms of public health and safety.
Pts in methadone maintenance show a higher reduction in morbidity and mortality and improvement in psychosocial indicators than heroin users outside treatment or not on MAT.
Policies and Practices Not Supported by ResearchPolicies and Practices Not Supported by Research Requiring abstinence as a condition of
access to substance abuse or mental health treatment
Denying access to AOD treatment programs for people on prescribed medications
Arbitrary prohibitions against the use of certain prescribed medications
Discharging clients for alcohol/drug use

Evidence-Based Practices:Key Issues in the Debate
Efficacy StudiesEfficacy StudiesSpecific psychosocial interventions
are usually investigated in random assignment studies using manualized treatments in carefully controlled trials. Samples and settings are homogeneous and treatment is standardized. Specific procedures assure fidelity to the model.
Random Assignment Controlled Trials (RCT’s)Random Assignment Controlled Trials (RCT’s)
Gold standard for pharmacological and many psychosocial interventions
Examples with strong efficacy: Cognitive behavioral therapy Motivational enhancement therapy Behavioral marital therapy Community reinforcement approach Relapse prevention Social skills training
(see Miller et al, 2005)
Adaptive Designs:An Emerging ParadigmAdaptive Designs:An Emerging Paradigm Individualize treatment using decision
rules that recommend when and for whom tx should change
Utilize a sequence of treatments, randomizing S’s based on clinical response
Starts with consensus-based clinical guidelines and fine tunes the sequence
Example: The STAR-D study

Are RCT’s Over-rated?
Are RCT’s Over-rated?
QUERI
Mark Willenbring MD (ASAM 2006)
Issues with RCT’s Is the research question an
appropriate question? Example: CBT A compared with CBT
B, vs CBT A compared with TAU Are the treatment effects modest
or robust? What is the cost to achieve and
maintain the intervention? Are the results worth it?

What About the Therapeutic Alliance?What About the Therapeutic Alliance? Studies outside substance abuse
show this accounts for a greater % of the variance than specific techniques
Different “specific” therapies yield similar outcomes, but there is wide variability across sites and therapists
More therapist education/experience does not improve efficacy
(Adapted from W.R. Miller, Oct 06)
Practice-Based EvidencePractice-Based Evidence Studies and meta-analyses report
moderate to large effects of indiv therapists
Gather client outcome data from routine practice
Give real-time feedback & suggestions to improve performance
Flag pts at risk for treatment failure or dropout
(Glassner-Edwards & Rawson, 2010)
IMPLEMENTATION ISSUESIMPLEMENTATION ISSUES

Levers for ChangeLevers for Change Financing Infrastructure development Legislation Regulation Accreditation (education programs,
service delivery organizations) Certification and licensure Performance based contracting
Degrees of Implementation:Process
Degrees of Implementation:Process
Putting new operating procedures in place:
Conducting workshops Providing supervision Change information reporting forms New innovation-related language is
adopted Is this functionally related to new
practices or merely lip service? (Dean Fixsen, 2005)
Can we assume that interventions with documented efficacy will be effective in the community if we only implement them correctly?
Rethinking the Efficacy-to-Effectiveness TransitionRethinking the Efficacy-to-Effectiveness Transition Assumption that effectiveness research
naturally flows from efficacy research is faulty.
The tight controls of efficacy studies limit their generalizability.
Focus more on intervention reach, adoption, implementation, and maintenance.
Published studies should include more info on external validity.
(Glasgow et al, AJPH, 2003)

Important Questions to AskImportant Questions to Ask
What are the characteristics of interventions that can:
1. Reach large numbers of people, especially those who can most benefit
2. Be broadly adopted by different settings
3. Be consistently implemented by different staff with moderate training and expertise
4. Produce replicable and long lasting effects (with minimal negative impact) at reasonable costs.
(Glasgow et al, AJPH, 2003)
ConsiderationsConsiderations What is to be gained? Does the organizational culture
support adoption? Is training available? Is clinical supervision available?
Ineffective Implementation StrategiesIneffective Implementation Strategies
“…experimental studies indicate that dissemination of information does not result in positive implementation outcomes (changes in practitioner behavior) or intervention outcomes (benefits to consumers)”
(Fixsen et al, 2005)
Opinion Leaders:A Key to Knowledge Adoption
Opinion Leaders:A Key to Knowledge Adoption Identified by peers as respected for
their knowledge in a particular area Trained in the use of an evidence-based
curriculum They then train their peers and
supervise the application of the curriculum
Changes in counselor behaviors and attitudes are measured to determine the effectiveness of the implementation process
(Rugs D, Hills HA, Peters R, 2004 at www.seekingsafety.org)
Key IngredientsKey Ingredients Presenting information;
instructions Demonstrations (live or taped) Practice key skills; behavior
rehearsal Feedback on Practice Other reinforcing strategies; peer
and organizational support (Fixsen et al,
2005)
CoachingCoachingTraining and coaching are a continuous
set of operations designed to produce changes
Newly-learned behavior is crude compared to performance by a master practitioner
Such behavior is fragile and needs to be supported in the face of reactions of others
Such behavior is incomplete and will need to be shaped to be most functional in the service setting.
(Fixsen et al, 2005)
Dissemination Mechanisms
NIDA’s Clinical Trials Network (CTN)http://www.drugabuse.gov/
CSAT’s Addition Technology Transfer Centers (ATTC)
http://www.attcnetwork.org/regional-centers/?rc=pacificsouthwest
Challenges & Perils
Policy and FundingPolicy and Funding Policy makers misinterpreting research
findings; drawing inappropriate conclusions Example: buprenorphine (“transfer
methadone pts to BPN and taper them off”) Using EBT’s takes precedence over
individualizing care Funders adopting a “pick from this list”
approach Achieving fidelity takes labor intensive
supervision, and many states don’t fund supervision.
Marketing Impostors
Distinguishing evidence from marketing“We have some of the highest success rates in the country”“You should only have to do this once.”
Presenting multiple anecdotes with no comparison or control groups as “proof”
Research to Practice IssuesResearch to Practice Issues
Inadequate effectiveness studies Huge gaps in the research literature
(s.g., group interventions, therapist variables)?
High training fees for “proven” practices Fidelity vs cultural competence: What is
the tradeoff between fidelity and the need to adapt interventions for specific populations? How can we make cultural adaptations and maintain the treatment effects?
Infrastructure DevelopmentInfrastructure Development
The existing infrastructure cannot handle the expectation for data collection
Funders want data but do not want to pay the costs
Data collected by funders is often not used to improve services
Workforce crisis is a huge problem and an opportunity. Must supply resources for training.
Stay Focused on Basic PrinciplesStay Focused on Basic Principles
Maintain commitment to the principle of individualizing treatment
When an evidence-based treatment doesn't work for an individual, some staff members conclude that the problem is that the treatment isn't being implemented correctly, rather than examining the possibility that it does not fit the needs of the client.
Example from Dual Dx listserve: dualdx.treatment.org
Is There Another Way?Is There Another Way?
Fund programs to develop the infrastructure to examine how they are doing with whom
Draw on EBT’s to improve in areas where there are problems
Clarify realistic performance standards
APA DefinitionAPA DefinitionEvidence-based psychotherapy is
resources-based: best practices are built on a foundation of empirical research, comprehensible and reasoned theories, clinical observation and expertise, and patients' values, contributions and responses.
Evidence-Based Skills TrainingEvidence-Based Skills Training Establish clear goals Identify feasible objectives,
adaptable to different settings Take into account the limitations of
the current health care system Train in core evidence-based skills,
rather than emphasizing manualized EBPs
(Glassner-Edwards & Rawson, 2010)
Treatment IssuesTreatment Issues
Co-Occurring Psychiatric & Substance Use Disorders COD are the norm, not the exception “No wrong door;” guided referrals,
“warm handoffs” Assessment: distinguish between
substance induced conditions and independent disorders
Treatment should be integrated, focusing on safety, stabilization, maintenance of gains
Trauma-informed care
Cognitive Behavioral TherapiesCognitive Behavioral Therapies Based on social learning theories Identify the antecedents and
consequences of drug use Skills training – identify high risk
situations, use behavioral and cognitive strategies to avoid situations or cope effectively
Includes relapse prevention strategies
(Carroll & Onken, AJP, 2005)
Motivational Enhancement Strategies
Widely adopted Principles widely applicable outside
substance abuse treatment TIP 33: Enhancing Motivation for
Change in Substance Abuse Treatment - order from: www.ncadi.samhsa.org
Goals and BenefitsGoals and Benefits Inspiring motivation to change Preparing clients to enter treatment Engaging and retaining clients in
treatment Increasing participation and
involvement Improving treatment outcomes Encouraging a rapid return to treatment
if symptoms recur
Community Reinforcement ApproachesCommunity Reinforcement Approaches Environmental influences play a
powerful role in encouraging or discouraging substance use
Social, recreational, familial and vocational forces can be use to promote behavior change
Goal: make sober lifestyle more rewarding than the use of substances
Counselor must find and use the client’s intrinsic reinforcers
CRA: ExamplesCRA: Examples CRAFT – work with spouse/parent to
change social environment; remove inadvertent reinforcement for drinking and using; reinforce abstinence
Job seeking and keeping; improving satisfaction with job
Identify new sources of recreation Behavioral skills: communication,
problem solving, drink/drug refusal
Contingency ManagementContingency Management
Systematic delivery of positive reinforcement for desired behaviors (e.g., negative toxicology screens)
Vouchers Prizes Other privileges, rewards, etc.
Essential Ingredients in the Recovery ProcessEssential Ingredients in the Recovery Process
A community that supports the recovery process
A path for personal development that has no financial barriers
Can use alternative groups but the 12-Step system is the most comprehensive
Download Slides:Download Slides:
www.ebcrp.org