Embed Size (px)
Citation preview

UNDERSTANDING THE BASIC
FEATURES AND MANAGEMENT IN THE
SCHOOL SETTING
CHRISTINE HERTLER RN BSN CDE
& MARY MCCARTHY RN CDE




The insulin pump
◦ Replaces injections
◦ Delivers insulin through a soft cannula under the skin
◦ Infuses rapid acting insulin in precise
programmable doses to meet
individual patient needs
The insulin pump closely mimics normal pancreatic insulin
delivery

6
Insulin
Cannula
Subcutaneous
Tissue
Skin

The insulin pump delivers basal and bolus insulin
precisely and can be easily customized as needed to
meet individual requirements.
Schematic representation only
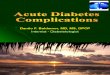
Programmable Insulin Delivery with Medtronic MiniMed Pump Therapy
0
1.0
2.0
3.0
4.0
5.0
6.0
12am 4am 8am 12pm 4pm 8pm 12am
Bolus insulin delivery
Basal insulin delivery
Basal programmed
to help prevent
dawn phenomenon
Dual Wave™
Bolus for brunch
Temporary basal during walking
to help prevent hypoglycemia
Dinner bolus
Basal reduced
to help prevent nocturnal
hypoglycemia
Un
its
of
ins
ulin

It works more like a healthy pancreas
It has more predictable insulin absorption
It offers more flexible basal rates
It offers more accurate bolus dosing
Bode B, Sabbah H, Gross T, Fredrickson L, Davidson P. Diabetes management in the new
millennium using insulin pump therapy.
Diabetes Metabolism Research and Reviews. 2002; 18 (Suppl. 1): S14-S20.

Basal
Bolus
Insulin carb ratio -ICR
Insulin sensitivity or correction factor-ISF
Target
Active insulin or insulin on board -IOB

Basal Rate – (background insulin) -provides insulin continuously
Pre-programmed
Continuous flow of fast-acting insulin
Matches variable metabolic needs
May be overridden by temporary basal rate

Bolus - provides insulin for: ◦ Food Intake
◦ High blood sugars
Bolus is not automatic.
User determines bolus amount based on:
- Carbohydrate content of meal or snack
- Current blood sugar reading

Active insulin is the amount of insulin (remaining from previous boluses) that is still working to lower glucose
The pump tracks active insulin even if not using the Bolus Wizard feature
Tracking active insulin helps avoid:
◦ Giving too much insulin and over-correcting highs
◦ Lows that occur from over-correcting highs



Change infusion site every 2-3 days
Rotate site with every set change
◦ Recommended sites:
Abdomen- 2 inches from umbilicus
Buttocks- away from midline
Perform hand hygiene and use clean technique when inserting/removing catheter
Clean skin with alcohol or IV prep wipe
Allow to dry thoroughly before insertion

Remove set at first sign of discomfort
Place new set away from original site
At the first sign of infection advise family to contact primary care provider ◦ Signs of infection include:
Redness
Hardness
Tenderness
Oozing from cannula
Area warm to touch

Monitor site for any leakage, this may indicate displacement of cannula
Monitor site for lipohypertrophy and lipodystrophy- benign lesions which can affect absorption of insulin
If these occur stop using existing site for 4 weeks to allow healing

REVEL • Basal 0.025
increment • Bolus 0.025
increment 530G with Enlite Sensor • First phase artificial
pancreas • Integrated sensor
with pump • Low glucose
suspend • Linking meter

• Only tubeless pump
• PDM is linking meter and pump manager
• Insulin and pump in POD
• Bolus must be given with PDM
• Holds 200 units
• Basal .05 units

• Dose from ping linking meter/remote
• Low dosing basal .025
• Waterproof
• Holds 200 units

First touch screen
• Small
• Waterproof • Rechargeable-
green
Holds 300 units No linking meter








Hyperglycemia
Hypoglycemia
What to do for Exercise
What to do in an Emergency

Forgot to bolus? (Press Esc for last bolus)
Miscounted carbs? Illness or infection? Blocked insulin flow (No Delivery) Kinked Cannula at the infusion site?

When blood sugar is over 300 mg/dl for long periods of time, the body burns other energy sources to provide food for the body’s cells
Cells begin to break down to provide this energy
This cell breakdown can cause ketones to be released into the bloodstream

Risk of Ketoacidosis
increases on pump because no
long acting insulin is in the body • Monitor 4-6 times daily • Never ignore an unexplained
high glucose

Early-loss of appetite, nausea
Later-vomiting, abdominal pain
Late-difficulty breathing, confusion

Is my infusion site red or irritated
Is my site wet or does it smell like insulin
Are there bubbles in the tubing
Is there blood in the tubing
Are there any leaks or breaks
Is connection loose, easily moved Is reservoir loaded correctly?
Is reservoir empty?

Are there excessive bubbles in reservoir?
Has insulin vial expired?
Has insulin been exposed to extreme temp?
Was last meal bolus missed (check bolus history)
Are basal rates set incorrectly?
Is time (am or pm) set correctly?
Is insulin pump not working????

WHEN BLOOD GLUCOSE IS 300 OR HIGHER CHECK FOR KETONES AND FOLLOW THESE
GUIDELINES
Give correction dose by injection
Change infusion set, reservoir
and insulin
Monitor blood sugar every hour
to make sure until BG is
lowering
Check ketones with every void
until negative
Force fluids
Never exercise when ketones are
positive
Positive Ketones Negative Ketones
Give correction dose via
insulin pump
Recheck blood sugar in 1 hour
If blood sugar has not
decreased:
-give ½ dose by syringe
-change infusion set,
reservoir and insulin
Continue to check for ketones
Check blood glucose 2 hrs
from correction dose

If moderate to large ketones present, there is an increased resistance to insulin---CALL HOTLINE
•The insulin given for correction may need to be increased by 50%
–Example:
•If 151-200mg/dl = 1 unit
•1 divided by 2 = 0.5
•1 unit + 0.5 units = 1.5 units (correction increased by 50%)
•This increase in correction can only be done twice, unless recommended by the hotline
32

Muscles will use glucose during exercise and activity – this can affect BG levels for several hours
Disconnecting from the pump
Using a temporary basal rate decrease
Consuming extra carbs before exercise per physician order
Discuss which plan to use with parents (504) and follow
physician school orders

Manage hypoglycemia the same way as you would if child were on injections
◦ 15 and 15 rule=15gm recheck in 15 min
◦ follow physician school order and parents’ guidelines
◦No need to disconnect pump

Fast acting carbohydrates for low blood sugar
Insulin and syringes
Extra infusion set and reservoir (plus inserter if necessary)
Extra batteries
Alcohol or skin prep
Phone # of student’s diabetes clinician
Blood glucose meter
Keto-stix
Glucagon kit


42
BENEFITS OF CGM
• Aids in the detection of highs and lows allowing for adjustments
for minimizing excursions
• Identifies patterns that otherwise would not be detected by
fingerstick alone
• Provides info about the effects of food intake, EXERCISE and
timing of insulin
• Provides glucose direction and rate of change
• Accuracy within 10-15 % at this time
• Complements but does not replace monitoring


Medtronic Enlite 530G-pump integrated
Dexcom
G4 -pump -integrated with Animas Vibe an T-Slim
G5 -stand alone sensor

530G with Enlite Sensor • First phase
artificial pancreas
• Integrated sensor with pump
• Low glucose suspend
• Linking meter

• BLUE TOOTH COMMUNICATION FROM DEXCOM G4 SENSOR TO PUMP
• NO METER
REMOTE • SEPARATE
DEXCOM RECEIVER MAY BE USED TO ALLOW FOR COMMUNICATION TO CELL PHONE
• STUDENT WILL ALSO HAVE TO CARRY CELL PHONE FOR CLOUD

CGM enabled Large capacity Rechargeable Watertight Touch Screen

Enlite® glucose sensor
MiniLink® transmitter
MiniMed® 530G insulin pump


50
DEXCOM SENSOR COMPONENTS


Recommended sites:
◦ Abdomen & Buttocks
◦ At least 2 inches away from insulin pump site
Change sensor site every 6-7 days
May encounter issues with tape adherence and skin sensitivity
Products that may help
◦ Skin Tac
◦ Bard Barrier Wipe
◦ Mastisol
◦ IV 3000
◦ Tegaderm
◦ Tincture of Benzoin

53
LOW
ALERT
HIGH ALERT
TARGET GLUCOSE
RANGE
CURRENT GLUCOSE READING
WHEN IN ACTIVE SESSION
TREND GRAPH
VIEWS BY TIME



My CGM IS TALKING TO ME!
WHY ARE YOU USING YOUR CELL PHONE IN SCHOOL?

When glucose is rising, then the difference between the Sensor Glucose and Blood Glucose readings tends to be greater

Blood Glucose tends to be ahead of the Sensor Glucose Both SG and BG readings will be similar

Focus on the direction and speed of your sensor glucose Arrows mean the sensor glucose has been changing rapidly




RESPONDING TO ALERTS




Dexcom receiver and/or cell phone must be within 20 foot range for communication
Medtronic enlite sensor, will communicate directly to pump and is already in range-if using a uploader, it must be within 6 foot range of body and cell phone
The sensor is worn continuously-the cell receiver, pump or cell phone has audible alerts warning to indicate glucose level out of range

When an alarm or alert sound is sounding, student, teacher or other designated person will need to clear alarm and check blood glucose by fingerstick
ALL ALERTS MUST BE CONFIRMED WITH A FINGERSTICK BEFORE TREATING ANY GLUCOSE READINGS
The nurse (or other designated person) should the low glucose as per protocol, notify parent as usual, and document both the fingerstick and sensor glucose results, along with the necessary treatment given
Please note that looking at TREND ARROW DIRECTION is helpful If the glucose sensor becomes detached from the body, store the device
safely without discarding any components-return this to the parent
THIS IS NOT AN EMERGENCY AND DOES NOT REQUIRE ANY SPECIAL INTERVENTION OR EXCUSING THE CHILD FROM SCHOOL ACTIVITY


Physician school orders still take precedence
Monitoring at regular intervals
Confirming alerts with fingersticks before treatment
504 plans will need to be updated which address parental concerns, use of cell phones, and accountability of student to report to health office

QUESTIONS???