Embed Size (px)
Citation preview

Uniform Grant Guidance
Key Changes and Impacts on Community Health Centers & FQHCs
MAY 17, 2016

Thematerialappearinginthispresentationisforinformationalpurposesonlyandisnotlegaloraccountingadvice.Communicationofthisinformationisnotintendedtocreate,andreceiptdoesnotconstitute,alegalrelationship,including,butnotlimitedto,anaccountant‐clientrelationship.Althoughthesematerialsmayhavebeenpreparedbyprofessionals,theyshouldnotbeusedasasubstituteforprofessionalservices.Iflegal,accounting,orotherprofessionaladviceisrequired,theservicesofaprofessionalshouldbesought.

Presenters
Kinman Tong, CPASenior Manager415‐677‐[email protected]
Kate Jackson, CPASenior Manager916‐503‐[email protected]
Matt Parsons, CPASenior Manager949‐221‐[email protected]
3

Objectives
• Understand the changes and developments and how they impact FQHC’s grant activities.
• Learn the key grant administrative areas such as allowable costs, time and effort reporting, procurement, internal controls, subrecipient monitoring, and audit requirements.
• Discuss best practices for the key grant administrative areas.4

5
Timing Considerations Related to the Uniform Guidance

6

Approximately how much does your Organization expend in federal awards each year?
A. <$750,000B. $750,000 to $5 millionC. $5 million to $10 millionD. $10 million to $50 millionE. > $50 millionF. No clue…that’s what a
Controller is for7
A. B. C. D. E. F.
2%
60%
5%7%
5%
21%

Most common federal grants awarded for FQHCs
• 93.217 – Family Planning Services
• 93.224 – Consolidated Health Centers
• 93.526 – ACA Grants for Capital Development in Health Centers
• 93.914 – HIV Emergency Relief Project Grants
• 93.940 – HIV Prevention Activities Health Department Based
• 10.557 – Special Supplemental Nutrition Program for Women, Infants, and Children
8

Other common federal grants awarded for FQHCs• 93.243 – Substance Abuse and Mental Health Services Projects of
Regional and National Significance
• 93.527 – Affordable Care Act (ACA) Grants for New and Expanded Services under the Health Center Program
• 93.569 – Community Services Block Grant
• 93.917 – HIV Care Formula Grants
9

How many of these awards does your Organization receive?
A. NoneB. 1 to 2C. 3 to 4D. 5 or moreE. You expect me to
remember CFDA #’s?10
A. B. C. D. E.
5%
44%
5%
20%
27%

11
0
50
100
150
200
250
Entities with funding Tested in 2014
Family Planning Svcs
Consol Health Centers
ACA Grants for Capital Dev
HIV Emerg Relief
HIV Prevention
WIC
*data obtained from the Federal Audit Clearinghouse as of March 15, 2016
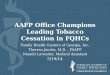
2014 Statistics for California Organizations*

Has your Organization received a single audit compliance finding in the past two years?
A. Yes
B. No
12Yes No
71%
29%

2014 Statistics for California Organizations*
13
0
5
10
15
20
25
Number with findings Qualified Opinions
Family Planning Svcs
Consol Health Centers
ACA Grants for Capital Dev
HIV Emerg Relief
HIV Prevention
WIC
*data obtained from the Federal Audit Clearinghouse as of March 15, 2016

Summary of Findings
14
21%
18%
14%14%
13%
9%
7%4%
Program Income ‐12
Reporting ‐ 10
Allowable Costs ‐ 8
Other* ‐ 8
Eligibility ‐ 7
Procurement ‐ 5
Matching ‐ 4
Cash Mgmt ‐ 2
Compliance area ‐ # of findings
*includes 1 ‐ Davis Bacon; 2 – Equipment management; 1 – Subrecipient monitoring; 3 – Special Tests

OIG Review of Submitted Single Audits for the period of 10/1/14 – 3/31/15*
15
Results NumberTotal audit reports evaluated 1,986
Requiring no changes or minor changes 1,185Requiring major changes 93
Significant technical inadequacies 8
*Data obtained from the HHS OIG Spring Semi‐Annual Report to Congress

Program income
• Not previously defined under Circular A‐133
• Health centers must• Have a schedule of fees for the provision of their health services
• Have a schedule of discounts (adjusted based on patient’s ability to pay)
• Ability to pay is determined using HHS poverty guidelines
• Make every reasonable effort to collect reimbursement through Medicare and Medicaid at gross rates (not discounted rates)
16

Program income: How am I likely to get in trouble?• No documentation to demonstrate how the schedule of fees
covers a reasonable cost of operation.
• Discounts not updated using annual HHS guidelines
• Improper billing (not using updated schedule of fees)
17

Reporting: How am I likely to get in trouble?
• Requirements vary by program
• Most common deficiencies:• Reporting is not timely
• Line items not supported at the time of the reporting
• No evidence of review
• Calculation errors
18

What am I most likely to get a finding for in the future under the Uniform Grant Guidance?
AreasofConcern
InternalControl
Procurement
SubrecipientMonitoring
AllowableCosts• IndirectCosts• CompensationforPersonalServices
19

“Must” vs. “Should”
• Must = required
• Shows up 844 times in 2 CFR 200
• COFAR FAQ 303‐1, 2, and 3 clarifies that should indicate a “best practice” and is not a presumptively mandatory requirement.
• Shows up 140 times in 2 CFR 200
20

Internal controls
• The non‐federal entity must: (a) Establish and maintain effective internal control over the Federal award that provides reasonable assurance that the non‐federal entity is managing the Federal award in compliance with Federal statutes, regulations, and the terms and conditions of the Federal award. These internal controls should be in compliance with guidance in “Standards for Internal Control in the Federal Government” [Green Book] issued by the Comptroller General of the United States or the “Internal Control Integrated Framework”, issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO).
21

Internal controls
• Internal controls are referenced 48 times in 2 CFR 200
• Opportunity to revisit internal controls.
• Update policies and procedures.
• Not just general controls, but also compliance requirements.
• Changes from the Uniform Guidance need to be reflected in internal controls.
22

• Do you have written procedures?
• Written procedures are required for:• Implementation of the payment system according to §200.305.
• Procedures for determining the allowability of costs in accordance with Subpart E (Cost Principles) and the terms and conditions of the Federal award.
• Standards of conduct covering conflicts of interest governing performance of employees engaged in selection of award and administration contracts.
• Standards for procurement transactions.
Internal controls: How am I likely to get in trouble?
23

How many of these policies does your Organization have in written form already?
A. None
B. 1
C. 2
D. 3
E. 424No
ne 1 2 3 4
5%
19% 17%
24%
36%

Internal controls: How am I likely to get into trouble? • Does your Organization have the following control activities?
• Reporting
• Supervision
• Documentation
• Separation of duties
• Safeguarding of assets
• Approval and authorization
• Verification/reconciliation25

Internal controls: What have we seen so far?
• Control procedures exist – but not well documented.
• Risk assessment is not clear or comprehensive. How would your controls actually prevent or detect errors or fraud?
• Review procedures are not detailed
• Training is not frequent enough for reviewers to remember their responsibility.
26

Internal controls: Best Practices• Get credit for what you’re already doing – DOCUMENT.• There are 5 elements of COSO. A simple memo with bullet points
under each of these elements will go a long way to impress auditors. • Control Environment• Risk Assessment• Control Activities• Information and Communication• Monitoring
27

COSO – Control Environment Examples:
• Ethics policy.• Fraud hotline.• Annual e‐mail from CEO emphasizing values and the
importance of following policies and procedures.• Serious consequences for policy violations.• HR’s use of policies and procedures to promote strong ethical
values.• Use of an audit committee.
28

COSO – Risk Assessment Examples:
• Does management hold bi‐weekly or monthly department head meetings?
• When information arises that affects reporting or transactions does management act on that? Is there a strong chain of communication?
• Every 6 months, ask every person in Finance and Grants Management to provide errors they see in their department or others
• Start developing a checklist to detect those errors.
• Do concerns from performance evaluations get followed up on to ensure that behaviors haven’t impacted reporting or compliance?
29

COSO – Control Activity Examples:
• Review policies and procedures and highlight the key controls.
• Discuss each transaction cycle associated with the grants: • Is payroll charged directly to the grant?
• Support for disbursements is reviewed by two individuals knowledgeable of how it benefitted the grant (so usually two people outside of Finance).
• Federally acquired equipment is properly secured.
30

COSO – Information and Communication Examples:• Finance is involved at the beginning when the Organization is
applying for a grant.
• Meetings with Department Heads to discuss budgets / changes to grant compliance.
• Staff meetings are open to provide opportunity for staff to share questions / concerns.
31

COSO – Monitoring Examples:
• Periodic comparison of actual expenses to grant budgets.
• Management responds right away to information on unusual occurrences or trends.
• Interaction with vendors that provide third party services• (i.e. obtaining a SOC 1 report from payroll processors and
understanding the controls described in the report).
• Implement best practices from monitoring reviews/visits.
32

Procurement• Not for profit and health care entities follow the five
procurement methods. • These entities will likely be affected more significantly.
• Auditees should review carefully to determine the impact on their procurement procedures• Think special considerations for procurement card programs.
33

34

Has your Organization already implemented procedures for these procurement levels?
A. Yes.B. No, but planning to.C. I’m retiring before it’s
effective – good luck to the rest of you!
35
A. B. C.
33% 33%33%

Procurement
o Review procurement card/credit card purchasing policies to ensure policies are consistent with new procurement methods.
o Procurement implementation given a grace period of two full fiscal year after effective date of Uniform Guidance. (§200.110)
36

Procurement: How am I likely to get into trouble?
o Need to start now (if not already started)o Policieso Procedureso Internal controlo Training of staff
37

Procurement: What have we seen so far?• Procrastination of implementation• Management trying to break up invoices to avoid bidding
• Staff are not sufficiently trained
38

Procurement: What have we seen so far?• Suspension and debarment
• Reviewed for at the time of procurement but no documentation was retained. During the audit, management struggles to produce documentation and runs the search the day of the audit.
39

Procurement: Best Practices• Start reviewing requirements now!
• Review overall budget, not just current invoice, in considering whether it might need to follow a different procurement procedure.
• Work with other FQHCs to piggy‐back off their procurement procedures (as long as you can prove to auditors the legitimacy of the original procurement).
• Maintain procurement details in grant folders. 40

Subrecipient monitoringChanges in Audit Threshold that Can Affect Subrecipient Monitoring• Audit threshold increased to $750,000. • Type A/B threshold is a sliding scale
with new minimum.• Minimum increases from $300,000 to
$750,000.
41

Subrecipient monitoringSubrecipient / Contractor Determination• Contractor replaces the term “Vendor”
from OMB Circular A‐133.• All characteristics need not be present.• Judgment should be used in the
determination process. • Substance of the agreement is more
important than the form.42

Subrecipient monitoring
Checklist: http://www.mossadams.com/articles/2015/november/uniform‐guidance‐subrecipient‐monitoring
Subrecipient ContractorCreates a Federal assistance relationship. Purpose is to obtain goods and services for the
non‐Federal entity’s own use. Creates a procurement relationship.
Determines who is eligible to receive what Federal assistance.
Provides the goods and services within normal business operations.
Has its performance measured in relation to whether objectives of a Federal Program were met.
Provides similar goods or services to many different purchasers.
Has responsibility for programmatic decision making.
Normally operates in a competitive environment.
Responsible for adhering to Federal program compliance requirements.
Is not subject to Federal program compliance requirements.
43

Subrecipient monitoring: How am I likely to get into trouble?• The sub‐award agreement / contract does not:
• Clearly identify award – see 13 required information list in 200.331(a)(1).
• Clearly identify requirements imposed originally.
• Clearly identify additional requirements imposed so the Pass‐Through Entity (PTE) can meet responsibilities to federal awarding agency.
44

Subrecipient monitoring: How am I likely to get into trouble?• The sub‐award agreement / contract does not:
• Clearly identify indirect cost information.
• Subrecipient permission for PTE and auditors to access records.
• Closeout terms and conditions.
• May use fixed award up to simplified acquisition threshold ($150,000).
45

Subrecipient monitoring: How am I likely to get into trouble?• No evidence that you evaluated the subrecipient’s risk of
noncompliance with Federal statutes, regulations, and terms and conditions of the award:
• Prior experience
• Results of previous audits
• Consider if there is new personnel or systems
• Extent and results of Federal awarding agency monitoring
46

Subrecipient monitoring: Best Practices• Monitor if subaward used appropriately.
• Subaward Agreement Templates: http://sites.nationalacademies.org/PGA/fdp/PGA_063626
• Consider if results indicate adjustment to the PTEs’own records.
• Issue management decision for audit findings.47

Subrecipient monitoring: Best Practices• Other PTE Monitoring Tools Depending on Risk
• Providing training and technical assistance.
• Performing on‐site reviews of program operations.
• Arranging for agreed‐upon procedures (AUP) engagements that meet certain requirements.
• Verifying each subrecipient is audited as required by Subpart F.
48

Allowable costsRefresher – Is it…?• Necessary & Reasonable
• Allocable to the federal award
• Limited or excluded (unallowed costs)
• Consistent with Policies & Procedures and Treatment (direct vs indirect)
• In accordance with GAAP
• Not included as part of cost sharing or matching requirement
• Net of any credits
• Adequately documented49

How does your Organization recover indirect (F&A) costs?
A. Simplified Allocation Method (one pool).
B. Multiple Allocation Method (multiple pools, i.e. interest, operations and maintenance, admin).
C. Direct Allocation Method (all costs get directly charged somewhere).
D. I can charge for indirect costs?
50
A. B. C. D.
0% 0%0%0%

Indirect (F&A) costsNEW (under Subpart E) (200.412‐.414)
• Federal agencies must accept negotiated IDCR unless:• statute or regulation allows for an exception or approval by federal
agency.
• A de minimis rate of 10% accepted if no IDCR• Based on modified total direct costs
• May be used indefinitely.
51

Indirect (F&A) costs• NEW Any Non‐federal entity that has a federally
negotiated IDCR: • May apply for a one‐time extension (for a period up to four
years).
• If extension granted, may not request a rate review until extension period ends.
• At the end of the extension period, MUST re‐apply to negotiate a rate.
52

What is your current approved indirect cost rate?
A. <10%
B. Between 10% and 15%
C. Between 15% and 25%
D. >25%
E. We’re going to use the new 10% de minimis rate
53
A. B. C. D. E.
0% 0% 0%0%0%

Indirect (F&A) costs ‐ How am I likely to get into trouble?• Direct costs also included in the allocation pool.• Capital costs included in the base.• Costs charged using a rate with old data or data with unallowable costs included in the pool.
54

Indirect (F&A) costs – What have we seen?
• Many grants have rates stated below the 10% de minimis.
• Direct allocation of administrative employees is hard to support through documentation.
55

Compensation • Principles based.
• Internal Controls are KEY.
• Same concept as current but less prescriptive on documentation.
• “Confirmation”, “statement…signed by employee” REMOVED.
Purpose is to reduce the burden of time and effort reporting
56

Compensation ‐ How am I likely to get into trouble?1. Not supported by a system of I/C (meaningful reviews and
approvals of time).
2. Not incorporated into official record.
3. Does not total activity for employee.
4. Does not encompass all activities.
5. Distribution of salary not supported.
6. Budget estimates alone do not qualify.57

CompensationEffort Reporting vs. Payroll Certification
Description Current Practice Effort Reports Payroll Certification
Certification focus Individuals. Grant/Contract (award).
Certification Cycle Semi/annual fiscal periods. End of each award budgetyear (every 12 mos.) and at the end of the award.
Approver Individual or manager. Manager.
Confirmation focus Individual’s percentage ofeffort is reasonable basedon overall effort.
All salaries/wages directlycharged to the award arereasonable based on workPerformed.
Type of funds All sponsored funds. Federal funds.58

Changes in audit requirements• Increases audit threshold from $500,000 to $750,000.• Type A/B threshold – minimum increases from $300,000 to
$750,000.• Loan/loan guarantee treatment in major program determination.• High‐risk Type A program criteria.• High‐risk Type B program criteria.• Percentage of coverage from 50/25% to 40/20%.• Low‐risk auditee criteria.• Audit findings (threshold from $10,000 to $25,000).
59

Schedule of Expenditures of Federal Awards
• Amounts provided to subrecipients from each federal program.
• Loan programs (loans outstanding at the beginning of period plus loans disbursed during the period.
• Loan guarantee programs.• Noncash assistance (free rent, food commodities, and
donated property, for example).• Total for each cluster of programs.
60

Schedule of Expenditures of Federal Awards
• Opportune time to revisit SEFA.
• Often areas where not compliant with regulations, but not materially wrong.
• Federal programs by federal agency.
• Show federal clusters.
• Special options for research & development.
• Pass‐through information.
• Footnotes to SEFA.61

Key changes to Data Collection Form• Clarified CFDA field and how to treat when the 3 digit extension
is unknown• Identifying numbers assigned by a pass‐through entity• The “name of the federal program” will be auto‐generated once
the CFDA number is input• Will collect cluster name instead of cluster identification number• FAC will automatically generate federal program total and cluster
total• Auditee and auditor statements
62

Other considerations • Engagements may be more complex
• Transitional auditing• Some grants may be audited under old guidance and some under new.
• New requirements
• Updated internal control
• Potential increase in time to prepare for and conduct the audit
• Potential increase in findings
• New AIPCA Single Audit certifications
• HRSA conducting more reviews / observations63

Implementation• Read the guidance• Identify what needs to changed• Create a plan/timeline• Talk with your auditors• Don’t procrastinate • Collaborate with others‐ willingness to share in the community
64

Other Resources• Council on Financial Assistance Reform (COFAR)
• https://cfo.gov/cofar/• FAQs – use latest version• Webcasts
• Office of Management and Budget (OMB)• http://www.whitehouse.gov/omb/grants_docs.• Uniform Guidance Crosswalk to Predominant Source in Existing Guidance• Uniform Guidance Cost Principles Text Comparison*• Uniform Guidance Audit Requirements Text Comparison*
*Note – these are not updated for any technical corrections65

Other Resources• Moss Adams Uniform Grant Guidance Launch Page
• http://www.mossadams.com/industries/not‐for‐profit/uniform‐guidance‐for‐federal‐awards
• Government Audit Quality Center (GAQC)• http://www.aicpa.org/InterestAreas/GovernmentalAuditQuality/Pages
/GAQC.aspx• Auditee tools• Internal control information• Open web events on Uniform Grant Guidance
• Committee of Sponsoring Organizations of the Treadway Commission (COSO)• http://www.coso.org/
66

About Moss Adams

2016 Health Care Conference: Thought Leadership & Engaged Conversation
SAVE THE DATE: Nov. 3 & 4, 2016Red Rock Resort, Spa and Casino | Las Vegas, NV
Moss Adams holds an annual two‐day health care conference designed for our clients. The conference brings together C‐suite health care professionals and provides a forum to discuss the latest topics that executives are facing – from shifting reimbursement models, population health, to retail health care. This annual platform enables executives to network, share industry best practices, and hear from industry experts.
2016 Keynotes Include:
• The Honorable Newt Gingrich & Senator Joe Lieberman give their predictions on health care policy following the election.
• Dr. Lisa Bielamowicz, Executive Director and Chief Medical Officer at The Advisory Board Company
• Roni Zeiger, M.D., former Chief Health Strategist at Google and founder of Smart Patient 68

Keeping You Informed
69
Keeping you informed about changes in the financial landscape is one of our top priorities. We closely monitor regulatory agencies, participate in industry and technical forums, and write about a wide range of general as well as industry‐specific accounting, tax, and business issues. The goal? To provide you with actionable information and guidance to help your organization succeed.
Continuing education is vitally important to us, and we’re happy to share our knowledge with you and your staff. We frequently offer a wide range of topical online seminars, many of which are archived and available on demand, allowing you to watch them on your schedule.

Our Services for Healthcare OrganizationsASSURANCE
• Agreed‐upon procedures• Audits and reviews• Single Audits• Compliance examinations pursuant to
federal reporting requirements• Employee benefit plan services• Written acknowledgments and agreed‐
upon procedure engagements in connection with tax‐exempt bond offerings
GENERAL CONSULTING
• Fraud investigation and forensic accounting
• IT consulting• Strategic business planning• Sustainability services• Wealth services
HEALTHCARE CONSULTING
• ACOs and integrated delivery models• 5010 readiness• ICD‐10 road map• Chargemaster management• Claims review and processing• Coding and chart reviews• Contract review• Data analytics• Dependent care audits• Financial modeling and forecasting• Hospital feasibility studies• Litigation support• Managed care operations• Practice operation assessments• Process improvement• Regulatory compliance• Reimbursement services• Revenue cycle assessments• Revenue recovery and enhancement• Strategic planning
70

Moss Adams by the Numbers
71

Kinman [email protected](415) 677‐8267
Kate [email protected](916) 503‐8197
Matt [email protected](949) 221‐4093