Embed Size (px)
Citation preview

Unifying mechanism for different fibrotic diseasesGerlinde Werniga,b,1, Shih-Yu Chenc, Lu Cuib, Camille Van Nesteb, Jonathan M. Tsaia, Neeraja Kambhamb,Hannes Vogelb, Yaso Natkunamb, D. Gary Gillilandd, Garry Nolanc, and Irving L. Weissmana,b,e,1
aInstitute for Stem Cell Biology and Regenerative Medicine, Stanford University School of Medicine, Stanford, CA 94305; bDepartment of Pathology,Stanford University School of Medicine, Stanford, CA 94305; cBaxter Laboratories Department of Microbiology and Immunology, Stanford University Schoolof Medicine, Stanford, CA 94305; dFred Hutchinson/University of Washington Cancer Consortium, Seattle, WA 98109; and eLudwig Center for Cancer StemCell Biology and Medicine, Stanford University School of Medicine, Stanford, CA 94305
Contributed by Irving L. Weissman, February 9, 2017 (sent for review December 5, 2016; reviewed by Joachim Deeg, Robert Hasserjian, and Fiona M. Watt)
Fibrotic diseases are not well-understood. They represent a numberof different diseases that are characterized by the development ofsevere organ fibrosis without any obvious cause, such as thedevastating diseases idiopathic pulmonary fibrosis (IPF) and sclero-derma. These diseases have a poor prognosis comparable withendstage cancer and are uncurable. Given the phenotypic differ-ences, it was assumed that the different fibrotic diseases also havedifferent pathomechanisms. Here, we demonstrate that many end-stage fibrotic diseases, including IPF; scleroderma; myelofibrosis;kidney-, pancreas-, and heart-fibrosis; and nonalcoholic steatohepa-tosis converge in the activation of the AP1 transcription factor c-JUNin the pathologic fibroblasts. Expression of the related AP1 tran-scription factor FRA2 was restricted to pulmonary artery hyperten-sion. Induction of c-Jun in mice was sufficient to induce severefibrosis in multiple organs and steatohepatosis, which was de-pendent on sustained c-Jun expression. Single cell mass cytometryrevealed that c-Jun activates multiple signaling pathways in mice,including pAkt and CD47, which were also induced in humandisease. αCD47 antibody treatment and VEGF or PI3K inhibitionreversed various organ c-Jun–mediated fibroses in vivo. Thesedata suggest that c-JUN is a central molecular mediator of mostfibrotic conditions.
c-JUN | anti-CD47 antibody therapy | signaling pathways | fibrotic disease |scleroderma
The fibrotic response is an important component of normalrepair processes that, if uncontrolled, can lead to various life-
threatening conditions, like idiopathic pulmonary fibrosis (IPF),primary myelofibrosis, and scleroderma (1–5). It is not knownwhether similar molecular mechanisms are responsible for the fi-brotic response in different diseases, and some studies came toconflicting conclusions (6). The molecular processes driving fibro-genesis are not well-understood, involving but not limited to trans-forming growth factor B (TGFB), platelet-derived growth factor(PDGF), connective-tissue growth factor (CTGF), vasoactive pep-tide, integrin signaling, and increased tissue stiffness (7, 8). At thecellular level, efforts have been made to characterize fibroblasts bymolecular markers (9), and fibrosis is thought to involve the cross-talk of hematopoietic and mesenchymal stroma cells (4, 6).Although the few currently available animal models are useful,
all of them have certain limitations: e.g., bleomycin-induced lungor skin fibrosis develops acutely in response to chemical injuryand is self-resolving; however, human diseases such as idiopathicpulmonary fibrosis or scleroderma are not (10). A more recentgenetic mouse model showed some fibrosis features but pre-dominantly exhibited vasoocclusive alterations more reminiscentof pulmonary artery hypertension (PAH) (11).On the other hand, the genetic basis of fibrotic diseases is just
emerging but already promises to gain fundamental insights intopathomechanisms: e.g., FAN1 mutations have been associatedwith kidney fibrosis, PNLAP3 with liver fibrosis, mutations inJAK2, MPL, or calreticulin with bone marrow fibrosis in myelo-proliferative neoplasm (12), and telomerase reverse transcriptase(TERT) and mucin 5B (MUC5B) with lung fibrosis, as well asalterations in DNA methylation, and some microRNAs (5) havebeen shown to play a role in lung fibrosis. Some of these molecular
findings have guided current standard of care treatments in, e.g.,lung fibrosis and primary myelofibrosis.We previously developed mouse models of primary myelofi-
brosis associated with myeloproliferative disease (13, 14) andwished to investigate their molecular downstream effectors. Geneexpression analysis suggested the dysregulation of cJUN, an AP-1 transcription factor that is a well-established regulator of criticalcell biological processes and involved in cancer and other humandiseases (15, 16). We subsequently investigated the expression ofAP-1 transcription factors in most human fibrotic diseases andfound increased c-JUN expression in SMA+ fibroblasts. In addi-tion, c-JUN was responsible for the pathologically increased pro-liferation of fibroblasts of patients with idiopathic pulmonaryfibrosis. Based on our observations in patients with various clinicalpictures of fibrosis, we generated a mouse model with inducible c-Jun. In these mice, we were able to induce fibrosis via the c-JUNpathway, which closely resembled the various organ manifesta-tions in patients. Remarkably, we found that fibroblasts selectivelyresponded to c-Jun despite ubiquitous c-Jun expression. Single cellmass cytometry analysis in mouse fibrosis revealed that tran-scriptional effects of c-Jun lead to a profound rewiring of active
Significance
Severe human fibrotic diseases are devastating and withouteffective treatments. We found that c-JUN expression is in-creased in many human fibrotic diseases and that systemic in-duction of c-Jun in mice resulted in development of fibrosis ofmultiple organs. These results suggest that many fibrotic dis-eases share a common pathomechanism that converges on c-Juninduction. Thus, common treatment strategies could potentiallybe developed for these seemingly different fibrotic disease en-tities. Moreover, the in vivo c-Jun induction represents a mousemodel for these devastating diseases that could be used forpreclinical evaluation of candidate antifibrotic treatments. In-deed, we show that blockade of the antiphagocytotic signalCD47 and the AKT and VEGF receptor pathways reverses tissuefibrosis in mice.
Author contributions: G.W., D.G.G., and I.L.W. designed research; G.W., S.-Y.C., L.C., C.V.N.,and J.M.T. performed research; G.W., N.K., H.V., Y.N., and G.N. contributed new reagents/analytic tools; G.W., S.-Y.C., and L.C. analyzed data; N.K. reviewed liver and kidney pathol-ogy; H.V. reviewed pathology and helped with immunostainings; Y.N. reviewed bone mar-row pathology and helped with immunostainings; and G.W., D.G.G., and I.L.W. wrotethe paper.
Reviewers: J.D., Fred Hutchinson Cancer Research Center; R.H., Massachusetts GeneralHospital; and F.M.W., King’s College London.
Conflict of interest statement: I.L.W. and G.W. have filed a patent, Docket No. S14-256:“(CD47) CD47 as potential single or combinatorial treatment in idiopathic lung fibrosisand systemic sclerosis.” I.L.W. cofounded 47Inc, a company developing anti-CD47antibody treatment as anticancer therapy.
Data deposition: The microarray data displayed in Fig. 3 in this paper have been depositedin the Gene Expression Omnibus (GEO) database, https://www.ncbi.nlm.nih.gov/geo (ac-cession no. GSE84838).1To whom correspondence may be addressed. Email: [email protected] or [email protected].
This article contains supporting information online at www.pnas.org/lookup/suppl/doi:10.1073/pnas.1621375114/-/DCSupplemental.
www.pnas.org/cgi/doi/10.1073/pnas.1621375114 PNAS | May 2, 2017 | vol. 114 | no. 18 | 4757–4762
MED
ICALSC
IENCE
S
Dow
nloa
ded
by g
uest
on
Oct
ober
25,
202
0

signaling pathways, which we exploited for effective therapeuticintervention in mice.
Resultsc-JUN Is Expressed in All Major Human Fibrotic Conditions. Previously,we had observed the up-regulation of AP-1 transcription factors in amouse model of polycythemia vera that also recapitulated featuresof bone marrow fibrosis (14). We therefore sought to analyze theexpression of c-JUN in human fibrotic conditions. Given the cel-lular heterogeneity in fibrotic lesions, we performed a thoroughimmunohistochemical analysis. A total of 454 biopsies from patientswith different fibrotic conditions were stained with H&E, with tri-chrome, and with antibodies against Collagen1, c-JUN, and SMA(Fig. 1). Then, 148 biopsies were analyzed from patients withscleroderma [skin lesions (n = 104), gastrointestinal (n = 38), andheart (n = 6)], 36 biopsies from patients with idiopathic lung fi-brosis, 57 biopsies from patients with primary myelofibrosis,164 biopsies from patients with liver fibrosis [related to nonalcoholicsteatohepatitis (NASH)/hemochromatosis, ethanol (ETOH)/hepa-titis C (HCV), alpha-1-anti-trypsin (A1A) deficiency, and chronicrejection], and biopsies from kidneys [systemic lupus erythematosus(SLE)-related and reflux-related) and the bladder, the pancreas,and the heart, but also biopsies involving intraabdominal andpleural adhesions; biopsies were matched with normal tissues ifavailable (Fig. 1 A and B and Fig. S1 A and C). Quantification ofthe immunofluorescence analysis demonstrated that a much higherfraction of SMA+ fibroblasts expressed nuclear c-JUN in all thesefibrotic diseases compared with three control conditions (P <0.0001) (Fig. 1C and Fig. S1A). Costaining of c-JUN with SMA(smooth muscle, fibroblasts), CK7 (bronchoepithelium), and CD31(blood vessel endothelium) demonstrated that c-JUN is pre-dominantly expressed in fibroblasts and a subset of bronchoepi-thelial cells and macrophages but only rarely detected in other celltypes in lung biopsies of lung fibrosis patients (Fig. 1 A and D).
Nuclear c-JUN Is the Predominant AP-1 Transcription Factor Identifiedin Pathogenic Fibroblasts in Fibrotic Plaques of Human Lung Fibrosisand Other Fibrotic Diseases. Because the c-JUN–related factorFRA-2 has been previously described in a murine model of pul-monary vasoocclusion and subsequent fibrosis (11), we testedwhether FRA-2 would be coexpressed with c-JUN in lung fibrosisand other fibrotic conditions. Indeed, resembling the describedmouse model remarkably closely, nuclear FRA2 was readily de-tectable in biopsies of pulmonary artery hypertension (PAH), inparticular in pathologically thickened PAH vessels (Fig. S2A,Upper). However, we failed to detect nuclear FRA-2 staining inthe majority of fibroblasts in other fibrotic diseases, including themost common interstitial pneumonia-type of idiopathic pulmo-nary fibrosis (IPF) (Fig. S2A, Lower).This finding prompted us to systematically investigate the ex-
pression of additional AP-1 transcription factors. Immunohisto-chemical stains of lung, liver, kidney, bladder, pancreas, and heartfibrosis and visceral adhesions confirmed strong nuclear c-JUNexpression. c-JUN was coexpressed with FOS and FOS-B occa-sionally in IPF, but not nuclear FRA-2 (Fig. S1 D and E). None ofthe remaining AP-1 transcription factors JUNB, JUND, andFRA-1 were detectable (Fig. S1B).
Pathogenic but Not Normal Fibroblasts Require c-JUN for RapidProliferation. To further investigate a functional role of c-JUN inpathogenic fibrosis, we knocked down c-JUN in primary lung-derived fibroblasts isolated from patients with idiopathic pulmo-nary fibrosis and normal lung tissue with two different hairpins.First, we confirmed that both hairpins achieved substantial de-crease of c-JUN mRNA (Fig. S2C). Both hairpins substantiallyreduced the proliferation of IPF fibroblasts compared with thecontrol hairpin at various time points after plating (Fig. 1E, filledbars). Surprisingly, we found that normal healthy lung-derived fi-broblasts do not require c-JUN; they continue to grow upon c-Junknockdown (Fig. 1F, open bars).
c-JUN–Positive Fibroblasts Are Surrounded by Macrophages and Expressthe CD47 “Don’t-Eat-Me” Signal in Idiopathic Pulmonary Fibrosis Lungs.A complex interplay between the immune system and mesenchymalcells is considered important for the pathogenesis of fibroticconditions (5, 6). We therefore analyzed lung samples of pa-tients with idiopathic lung fibrosis for the presence of immunecells and observed large numbers of CD68+ macrophages in-terspersed with c-JUN–expressing fibroblasts (Fig. S2B, Bot-tom) (Fig. S2D demonstrates specificity of the human c-JUNantibody). This finding raised the question why fibroblasts arenot phagocytized by macrophages. We therefore investigatedthe expression levels of antiphagocytic don’t-eat-me signals andfound that CD47 was up-regulated on fibroblasts. In contrast,
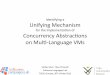
Fig. 1. Elevated c-JUN expression in various human fibrotic diseases. (A) SMA+
fibroblasts in lung fibrosis strongly expressed nuclear c-JUN (red) in fibroticplaques as revealed by trichrome, Collagen1, and SMA staining. Shown arerepresentative patient biopsies of lung fibrosis (n = 43) stained for indicatedmarkers. (Scale bar: 100 μm.) (B) Example micrographs showing high c-JUNexpression in trichrome+, fibrotic plaques of various indicated fibrotic condi-tions. Arrows indicate examples of nuclear c-JUN expression. (C) Quantificationof c-JUN expression in SMA+ fibroblasts in various fibrotic conditions, includingscar tissue (49 patient biopsies), scleroderma (104 patient biopsies of sclero-derma, diffuse proliferative type), and lung fibrosis (43 patient lung biopsies)and in marrow fibrosis (57 patient marrow biopsies) but not in normal skin,lung, and marrow. ****P < 0.0001; ANOVA test. We quantified coexpressionof c-JUN and SMA in the entire tissue of each sample. (D) Nuclear c-JUN isstrongly expressed in mesenchymal cells in fibrotic plaques in lung fibrosis butonly weakly in a small subset of bronchoepithelia (CK7 in green) and endo-thelia (CD31 in green). DAPI, nuclear counterstain in gray. Asterisks indicateauto fluorescence; one out of seven lung fibrosis and one out of six normallung patient biopsies are shown. Three biological replicates for each stain wereperformed. (Scale bar: 100 μm.) (E) Lung fibroblasts from lung fibrosis patientsrequire c-JUN to proliferate. Filled bars show cell numbers at indicated timepoints after c-JUN hairpin induction with doxycycline, open bars after doxy-cycline of control infections. (F) Normal lung fibroblasts do not require c-JUNto proliferate, unlike lung fibrosis fibroblasts. Shown are relative cell numbersbefore and after doxycycline-induced c-JUN knockdown normalized to thecondition before knockdown. Patient lung fibroblast cultures were infectedwith one of two lentiviral shRNA hairpins also expressing RFP or a controlvector expressing GFP. Infected cells were sorted by FACS and plated at adensity of 6,000 cells per well, and the number of red and green fluorescentcells was counted 24, 48, and 72 h after plating. Data (mean ± SEM) representfour replicates (Student’s t test). *P < 0.05, **P < 0.01, ***P < 0.001.
4758 | www.pnas.org/cgi/doi/10.1073/pnas.1621375114 Wernig et al.
Dow
nloa
ded
by g
uest
on
Oct
ober
25,
202
0

calreticulin, considered an “eat-me” signal, was expressed inmacrophages and a subset of bronchoepithelial cells (Fig. S2B,Top, Middle, and Bottom).
c-Jun Induces Widespread Fibrosis in Many Organs. In addition tobone marrow fibrosis (Figs. S3 and S4), detailed histopathologicanalysis of systemically c-Jun–induced mice revealed severe fi-brosis of the skin, which is illustrated by the blue trichromestaining that reveals that over 80% of the dermis is replaced withextracellular collagen deposition (Fig. 2D, Upper). Moreover,several gastroenteric organs displayed similarly severe fibrosis in
the distal esophagus, stomach, and small intestine (Fig. 2D,Lower). Other organs were much less affected, such as the lungthat showed only a mild interstitial fibrosis. Fibrotic alterationsof the skin, gastroesophageal junction, and lung are character-istic diagnostic criteria for the human condition of scleroderma.Given the short time window of analysis due to rapid death
with systemic induction, we next asked whether tissue-restrictedinduction of c-Jun may cause fibrosis also in additional organs.We subsequently established fibrosis restricted to the lung by
c-Jun induction via dox aerosol administration. Indeed, this treat-ment resulted in striking fibrosis, with over 30% of the lung pa-renchymal tissue replaced with extracellular collagen as shown bytrichrome stain (Fig. 2C). The collagen was distributed in a patchyinterstitial pattern peripleurally and surrounding the major airways.This process was reversible when dox administration was dis-continued after 21 d, and animals completely resolved the fibrosisand demonstrated normal histopathology at 300 d at study endpoint (Fig. S5E). In addition, we did not notice any fibrotic changesafter PBS aerosol administration in c-Jun–inducible mice or withdox aerosol in littermate controls lacking c-Jun (Fig. S5D). In micewith lung fibrosis, inflammatory cells were admixed and comprisedof abundant CD68+ macrophages with fewer lymphocytes, plasmacells, and neutrophils (Fig. 2C, Inset, Lower Left). Because con-ventional volumetric assessment of lung function proved chal-lenging in these sick mice, we measured CO gas diffusion, whichshowed a functional impairment in gas exchange (Fig. S5C). Thus,the characteristic histopathological abnormalities and clinical pre-sentation of mice after lung-restricted c-Jun induction closely re-capitulated the human condition of idiopathic pulmonary fibrosis,in particular the most common usual interstitial pneumonia-type.Next we crossed the tetO-c-Jun allele to Pax8-rtTA mice to ac-
complish kidney-specific c-Jun induction. After 8 wk on dox water,animals appeared moribund. Histopathologic analysis demon-strated 30 to 40% interstitial fibrosis of the kidney, with abundantabnormal extracellular collagen matrix deposition labeled in bluewith trichrome stain and tubular atrophy consistent with a primarytubulointerstitial nephropathy. In addition, serologic markers forkidney function, such as blood urinary nitrate (BUN) and creati-nine, were significantly increased (Fig. 2E and Fig. S5F).cJUN expression caused drastic thickening and fibrosis of the
bladder wall (80% fibrosis after 38 d of dox in the drinking waterin c-Jun BDF1 mice) (Fig. S4B) and uterus fibrosis (Fig. S4C).
Development of Steatohepatosis-Like Alterations After c-Jun Induction.Steatohepatosis is associated with increased fat accumulation inliver cells and considered a precursor of liver cirrhosis/fibrosis.Indeed, 7 to 10 d after systemic c-Jun induction, we noticed smalland large vacuoles in the majority of hepatocytes (Fig. 2F and Fig.S5G) (which were positive by oil-red O, a stain that highlightslipids) but no fibrosis. We qualitatively assessed liver fat contentafter cJUN expression in mice and detected 60% micro- and 40%macrovesicular changes in contrast to less than < 5% in non-induced controls. A recent report showed similar liver changes inmice mediated by distinct AP1 dimers; however, unlike our find-ings, the steatohepatic abnormalities required liver injury (17).In summary, these findings demonstrate that c-Jun expression
results in fibrosis in virtually all organs.
c-Jun Induces Feedback Loops to Rewire Signaling Pathways in a CellContext-Specific Manner. To further explore the molecular pathwaysinvolved in c-Jun–induced fibrosis, we performed genome-wide tran-scriptional profiling. We profiled whole bone marrow 24 h after doxtreatment of c-Jun–inducible and control mice in vivo. Strikingly, al-ready at this early time point, many fibrogenesis-associated genes wereinduced, such as Cdc42, Cxcl12 (also known as Sdf1), Tgfbr1 and -2,Ccl3, Ccl4, Collagen1a1, Collagen1a2, Collagen5a2, and Adiponectin,some of which are involved in migration (Fig. 3A and Fig. S6A).Among the top 100 up-regulated genes were other representatives ofthe AP1 family, most notably c-Fos (Fig. S6A). To confirm our RNAexpression data, we tested 43 cytokines and surface epitopes by directimmunofluorescence or flow cytometry and found Cxcl12 (Sdf1),
Fig. 2. Development of multiple organ fibrosis in mice after induction of c-Junin vivo. (A) c-Jun–induced lethality in mice in a strain-dependent manner. B6, F1129/C57BL/6; Bdf1, F1 129/BDF1. The red curve represents c-Jun B6 mice (n = 10,P < 0.0001), and the blue curve c-Jun Bdf1 mice (n = 7 mice, P < 0.0001 byKaplan–Meyer survival analysis and two independent experiments). (B) Mice(B6) released many pro- and antiinflammatory cytokines in the blood 48 h afterdox-mediated ubiquitous c-Jun induction. We quantified 38 mouse cytokines/chemokines by multiplex assay and found 13 to be increased significantly (**P <0.01; ns, not significant) as indicated (n = 3 animals per group, repeated once,P values have been calculated by Student’s t test). (C) Dox-mediated c-Jun ex-pression in the lung led to “honeycomb” fibrosis reminiscent of human idio-pathic lung fibrosis. Fibrotic plaques with extensive interstitial collagen (bluestained areas on trichrome) and intermixed with interstitial macrophages(CD68+, Inset) were identified peribronchial and subpleural and represented34% of the surface area. We quantified the trichrome+ areas of 10 high powerfields (40x), n = 3 animals per group (***P < 0.001). (D) Dox-mediated ubiqui-tous c-Jun expression led to thickening and fibrosis of the dermal skin and thegastroesophageal junction, a pattern of fibrosis reminiscent of human sclero-derma. We quantified fibrosis in the trichrome+ areas of 10 high power fields(40x) of trichrome-stained sections (Insets) and detected 89% in the dermal skinand 67% in the stomach wall, n = 5 animals. (E) Kidney-restricted c-Jun ex-pression using a Pax8-rtTA strain resulted in interstitial fibrosis and tubular at-rophy (quantified at 30 to 40%) with elevated kidney enzymes as indicated inthe table reminiscent of a primary tubulointerstitial nephropathy in patients.(Insets) High power views (40x) of the abnormal areas. A PASd stain (Top) labelsintact basement membranes of glomeruli and tubuli, the H&E stain demon-strates increased interstitial fibrosis (Middle), and a trichrome stain (blue stain)shows abundant abnormal extracellular collagen matrix deposition (Bottom).n = 4 animals. (F) Systemic c-Jun expression caused fatty liver changes of themicro- and macrovesicular type in mice as shown by the small and large intra-hepatic orange deposits on Oil-red O and the intracellular vesicles on H&Estains. We quantified 400 hepatocytes for intracellular lipid droplets in repre-sentative areas of Oil-Red O-stained liver sections as indicated. ****P < 0.0001;paired Student’s t test. All data (Fig. 2 C–F) (mean ± SEM) represent two rep-licates of two independent experiments. Representative histology at 20xmagnification, n = 4 animals. (Scale bars: 100 μm.)
Wernig et al. PNAS | May 2, 2017 | vol. 114 | no. 18 | 4759
MED
ICALSC
IENCE
S
Dow
nloa
ded
by g
uest
on
Oct
ober
25,
202
0

Cxcr4, Thrombospondin-1, CD51, Vegfr, and CD47 to be increasedin c-Jun–expressing cells (SI Results, SI Materials and Methods, andDataset S1). Specific interrogation of a fibrosis signature using geneset enrichment analysis (GSEA) revealed a significant enrichment inthe c-Jun–induced cells (Fig. 3B). We next asked whether c-Jun, atarget of the MAPK/JNK pathway itself, may in turn control thetranscription of genes involved in upstream signaling pathways. Tothat end, we performed ingenuity pathway analysis and found tran-scriptional up-regulation of the MAPK pathway 24 h post–c-Jun in-duction (Fig. S6B).These transcriptional changes indicated that c-Jun once stimu-
lated by upstream mechanisms may induce feedback loops torewire the intracellular signaling networks that in turn may lead
to fibrogenesis. To trace the origin and consequences of c-Jun–mediated signaling in primary bone marrow stroma, we performedCyTOF (mass cytometry) analysis. Primary bone marrow stromacells with or without 48 h of c-Jun induction were fixed andstained with 34 metal-conjugated antibodies against fibrogenesis-associated proteins (such as CD104, CD26, Sca1, Pdgfra, Fgfr,Vegfr, AdipoqR2, CD49b, and CD49e), genes up-regulatedfrom transcriptional analysis (such as CD47, Npm1, Dusp1,and thrombospondin), and major signaling pathways related toc-Jun [such as the ERK1/2 MAPK pathway (pERK1/2 and pS6),the p38 pathway (pMAPKAPKII), pJNK, the AKT-mTOR path-way (pAKT and pS6), and Dusp1] (Dataset S1, SI Results, and SIMaterials and Methods). The visualizing data using t-DistributedStochastic Neighbor Embedding (t-SNE) algorithm (viSNE) mapsgenerated based on all 11 surface markers to the dataset showedtwo clearly distinct subpopulations. One was characterized by highexpression of macrophage lineage markers, including CD172a andF4/80. The other subpopulation, CD172a and F4/80-negative cells,exhibited a much higher induction of phospho-c-Jun and c-Jun–induced molecules, such as Dusp1 (Fig. 3C and Fig. S6C). Tobetter understand the effect of c-Jun induction on signaling net-works in both subpopulations, we took advantage of the inherentstochasticity at the phosphor-c-Jun level between individual cellswithin each subpopulation and asked whether the state of a de-pendent signaling node could be correlated with the abundance ofphospho-c-Jun. A conditional density-based algorithm, DREVI,was recently developed for this purpose to provide a way to visu-alize relationships between signaling nodes, which is well-suited tocharacterize the rewired signaling network after c-Jun induction(18, 19). As we show in Fig. 3D and Fig. S6D, this method com-puted the conditional density of the dependent signaling nodes onthe y axis for the corresponding pospho-c-Jun values on the x axis.Among the measured signaling molecules, the DREVI plotrevealed a digital type of response in the relationship betweenphospho-c-Jun and phospho-Akt only 48 h after c-Jun induction inCD172a and F4/80-negative cells, where a sharp transition betweenlow and high phospho-Akt was observed (Fig. 3D). In contrast,components of MAPK pathways were the major up-regulatedgenes in the transcriptomic analysis at 24 h. We did not detectany increase in the phospho-Erk phospho-c-Jun relationship beforeand after c-Jun induction, and our data suggest that c-Jun increasedDusp1 levels, which negatively regulate the MAPK pathway. Re-markably, the F4-80+ cells showed only little response to c-Juninduction. These results demonstrate that the induction of transcrip-tional regulator c-Jun can rewire intracellular signaling networks byrobustly activating the PI3K-Akt pathway while maintaininghomeostasis in the MAPK pathway.
Functional Evaluation of Signaling Pathways Mediating the FibroticResponse. We next wished to assess the functional relevance of thesignaling pathway rewiring induced by transcriptional activation of c-Jun. To enable systematic pharmacological interrogation, we sought todevelop a c-Jun–dependent in vitro assay. We assessed two cell bi-ological parameters in cultured bone marrow-derived stromal cellsfrom c-Jun–inducible mice. First, we assessed cell growth and observeda shortening of the cell doubling time from about 22 d in control toabout 2 d in c-Jun–induced fibroblasts (Fig. 4A). Second, we measuredcell migration of marrow-derived stromal cells in a transwell migrationassay as a functional readout of c-Jun induction and observed a 100-foldincrease in migration at 2 h and 24 h in dox-mediated c-Jun–expressingcells compared with noninduced cells (Fig. 4B).Given its much greater dynamic range, we then tested a series of
small molecule inhibitors in the transwell migration assay. Consis-tent with our mass cytometry findings, the c-Jun–induced migrationwas reduced to almost baseline levels in the presence of PI3Kpathway inhibitors but not blockers of MAPK (such as MEK, p38),Jak, mTOR, Notch, hedgehog, GSK3, and EGFR (Fig. 4C).
Blockade of the VEGF and PI3K Pathways Reverses Marrow and SkinFibrosis in Vivo. Encouraged by these findings, we sought to evaluatethe efficacy of blocking the PI3K-AKT pathway in c-Jun–mediated
Fig. 3. c-Jun rewires transcriptional and signaling pathways in fibroblastsin vivo. (A) Genome-wide transcriptional profiling in mouse marrow after24 h of dox-mediated c-Jun expression in vivo demonstrated up-regulationof c-Jun and Fos and indicated genes, many of which were previously asso-ciated with fibrotic conditions. We selected 1,144 probes out of 45,101 basedon greater than ±2-fold change. Gene expression studies were performed intriplicate per each time point, and bone marrow of three mice was pooledper array. (B) Fibrosis signature genes are significantly enriched by gene setenrichment analysis (GSEA) in the up-regulated genes 24 h after dox-mediated c-Jun expression. (C) ViSNE maps of primary, marrow-derived fi-broblast cultures before (Ctrl, 0 h dox) and after c-Jun induction (48 h dox)were generated by considering all 12 surface markers and represent its de-gree of F4_80 (Upper) or Dusp1 (Lower) expression; blue colors represent lowexpression and yellow to red colors high expression. (D) Conditional densityvisualization (DREVI plots) of the relationship between Phospho-c-Jun (pc-Jun) and Phospho-Akt (pAkt) (Top), pc-Jun and pErk (Middle), and pc-Junand Dusp1 (Bottom) in F4_80-negative (subset B) versus F4_80-positive(subset A) marrow-derived adherent cells 48 h after c-Jun induction. Thevisualization method described how the y axis molecule changes as a func-tion of the x axis molecules. Dark red (maximal color) represents the mostlikely y axis molecule value in the corresponding x axis molecular value. Aresponse function (white curve) is fit to the region of highest conditionaldensity. Representative data of two independent series are shown.
4760 | www.pnas.org/cgi/doi/10.1073/pnas.1621375114 Wernig et al.
Dow
nloa
ded
by g
uest
on
Oct
ober
25,
202
0

fibrosis in vivo. Wortmannin, a potent PI3K inhibitor, was systemi-cally administered to mice (for 14 d) that were induced to express c-Jun 2 d before drug. Remarkably, this treatment resulted in com-plete suppression of bone marrow and skin fibrosis (Fig. 4G,H, andI). In addition to the PI3K-AKT pathway, we also tested the effect ofblocking the VEGF pathway on c-Jun–induced phenotypes bothin vitro and in vivo because we found that VEGF was highly
expressed in the primary bone marrow-derived adherent cells (Fig.S6C). As shown in Fig. 4 C, J, and K, the specific VEGFR inhibitorPD173074 was able to abolish c-Jun–mediated migration in vitro andsignificantly decreased bone marrow fibrosis, but not skin fibrosis,in vivo (SI Results and SI Materials and Methods).
Prophagocytic Anti-CD47 Treatment Reduces Fibrosis in Vivo.We hadnoticed the prominent appearance of infiltrating macrophages inlung fibrosis, both in patient biopsies and in c-Jun–induced mice(Fig. S2B and Fig. 2C), which enclosed pathogenic fibroblastsexpressing the antiphagocytotic CD47 signal (Fig. S2B). This pat-tern was reminiscent of macrophages surrounding CD47+ cancercells or atherosclerotic plaques and raised the question of whetherblocking the CD47 signal may stimulate phagocytosis of pathogenicfibroblasts by these infiltrating macrophages (20). Anti-CD47 an-tibodies have been shown to eliminate various human cancer cellsand atherosclerosis in different preclinical models (21), but elimi-nation of nontransformed normal cells has not been observed yet.To evaluate whether macrophages could be stimulated to phago-cytose fibroblasts, we first tested the effect of blocking anti-CD47 antibodies in vitro. We cocultured primary mouse macro-phages with c-Jun–induced primary fibroblasts and observed that,in the presence of anti-CD47 antibodies, the percentage ofphagocytosed fibroblasts was indeed significantly increased (Fig.4D). These compelling results prompted us to assess the effects ofCD47 antibody treatment in our lung-restricted c-Jun fibrosismodel. Indeed, daily i.p. injections for 21 d with an anti-CD47 antibody substantially reduced fibrosis (Fig. 4 E and F). Mostimportantly, animals administered anti-CD47 antibody treatmentsurvived longer than control group, and their lung function wassignificantly improved as indicated by normalized carbon monoxidediffusion (Fig. S5C). These data suggest that macrophages caneliminate even nontransformed cells that contribute to diseaseformation when antiphagocytotic stimuli are blocked.
DiscussionHere, we report that c-JUN, a well-characterized AP1 transcrip-tion factor, is expressed in many different fibrotic diseases. Wefound decreased proliferation of patient fibroblasts from fibroticlungs after knockdown of c-JUN. We detected activated c-Jun andAkt as well as up-regulation of CD47 expression in vivo in end-stage fibrosis lungs. We further showed that c-Jun can inducerapid and widespread fibrosis in all organs in mice and is alsoexpressed in fibrotic areas of abdominal adhesions in WT mice.c-JUN is widely expressed in skin epithelium and many otherepithelial cells, but not highly in stromal cells. c-JUN is also part ofthe acute phase response cascade, has a role in bone formation,and has a reputation as an oncogene, and its up-regulation hasbeen shown in various cancers (16). Although c-JUN’s role in cellcycle promotion has been well established primarily in vitro (16,22), we observed a striking cell context-dependent fibrotic re-sponse in vivo. Despite ubiquitous c-Jun induction, we observedprimarily fibrotic changes, indicating that the proproliferative andpromigratory effects of c-Jun require the specific cellular contextof tissue fibroblasts. Systemic induction of c-Jun in hematopoieticprecursors caused rapid apoptosis; induction in the liver caused apronounced hepatosteatosis. This unique c-Jun responsivenessseems to be shared among fibroblasts of many different tissuesalthough fibroblasts are considered highly heterogeneous andtissue-specific (23). The fibrogenic response in multiple tissuesand organs also contrasts with previously developed fibrosismodels, suggesting that induction of c-Jun could be a commonmolecular mechanism across different human fibrotic conditions.We further provide evidence that the transcription factor
c-Jun, which is a downstream target of MAPK-signaling cas-cades, can itself rewire and stabilize a specific pattern of multiplesignaling pathways. We assume that the remodeling of signalingpathways will be different in different cell types, leading to theopposing cell biological effects of c-Jun in different cell types.Importantly, our mouse model also confirmed the functional
relevance of several signaling pathways, some of which were
Fig. 4. Anti-CD47, PI3K and VEGF inhibitors block c-Jun–mediated fibrosis.(A) Assessment of the doubling time (in days) of primary bone marrow fi-broblasts with or without c-Jun induction revealed an about 10-fold increasedproliferation rate upon c-Jun induction. Data (mean ± SEM) represent threereplicates and two independent experiments; ****P < 0.0001; paired Student’st test. (B) Transwell migration of primary marrow fibroblasts from c-Jun–inducible mice increased about 100-fold upon dox treatment at both 2 and24 h after seeding. Data (mean ± SEM) represent three replicates and twoindependent experiments; **P < 0.01; paired Student’s t test. (C) c-Jun–mediated transwell migration of primarymarrow fibroblasts in the presence ofindicated small molecule inhibitors. Migration was impaired by PI3K, Vegf,Pdgfr, and Tgfb pathway inhibitors. Data (mean ± SEM) represent two repli-cates and two independent experiments; ***P < 0.001; paired Student’s t test.(D) In vitro phagocytosis assay of primary c-Jun–expressing fibroblasts andprimary macrophages in the presence or absence of anti-CD47 antibodies.Anti-CD47 increased the phagocytosis rate. Data (mean ± SEM) represent tworeplicates and two independent experiments; **P < 0.01; paired Student’st test. (E) H&E stain of lung sections of anti-CD47–treated (Left) and untreated(Right) mice after airway-restricted doxycycline delivery, which resulted inc-Jun–induced honeycomb-type lung fibrosis. The fibrosis was histomorpho-logically reversed with anti-CD47 antibody (MIAP 410, also known as clone 3).(F) Quantification of the extent of fibrosis in lung sections revealed that theresidual fibrosis in the treatment group was 5%. n = 3 mice per experiment,two independent experiments; **P < 0.01, paired Student’s t test. (G and J)H&E histological analysis revealed that c-Jun–mediated bone marrow fibrosiswas eliminated and replaced with normal hematopoietic cells after systemictreatment of PI3K and VEGF pathway antagonists. (H) Quantification ofmarrow fibrosis of PI3K inhibitor-treated and control mice revealed almostcomplete absence of fibrosis in treated animals. N = 3 animals, two in-dependent experiments; ***P < 0.001. BM, bone marrow. (K) Quantificationof marrow fibrosis of VEGF inhibitor-treated and control mice. n = 3 animals,two independent experiments; **P < 0.01. (I) c-Jun–mediated scleroderma-type dermal skin thickening was substantially reduced with PI3K inhibitortreatment. Data (mean ± SEM) represent n = 3 replicates, two independentexperiments; *P < 0.05; paired Student’s t test. (Scale bars: 100 μm.)
Wernig et al. PNAS | May 2, 2017 | vol. 114 | no. 18 | 4761
MED
ICALSC
IENCE
S
Dow
nloa
ded
by g
uest
on
Oct
ober
25,
202
0

previously associated with fibrosis and were targeted in past clinicaltrials (23), and idiopathic pulmonary fibrosis is currently treated witha combination of small molecule inhibitors targeting four differentpathways: VEGF/FGFR/PDGFR and TGFBR (1). This findingsuggests that c-Jun may be a central node controlling these essentialpathways. Although combination therapy is in principle an attractivestrategy, in practice, it is difficult to identify the right combination ofpathways to target. In particular, for clinical trials, it is not feasible toevaluate combination therapy in a systematic manner. Our discoverythat c-Jun coordinates several signaling pathways leading to fibrosisin vivo provides a unique opportunity to identify all relevant sig-naling pathways and predict the most effective therapeutic drugcombinations. Moreover, it may be possible to develop therapeuticstrategies interfering with the activity of c-Jun directly, which wouldeliminate the need to search for the most effective combination byeliminating the key disease-driving element.Several other mouse models have been established previously
and have served to gain important insight into some specific as-pects of disease (4). The most widely used model is a bleomycin-induced lung fibrosis isolated or in combination with the geneticmodel of Marfan syndrome. This model suggested the involvementof the TGFBR pathway in fibrosis, which we could confirm to alsoplay a role in our c-Jun–induced model. In particular, the geneticmodel of Marfan syndrome was very instructive regarding thedissection of the contribution of dendritic helper cells toward thepathomechanism of skin and pulmonary fibrosis (4). Anothermodel system uses carbon tetrachloride (CCl4) or bile duct ligationto study fibrosis in the liver, which has been shown to be linked toloss or constitutive activation of PDGFR-β in stellate cells.Unlike these mouse models, the c-Jun–induced model is a
purely genetically driven model. Importantly, it recapitulates manyaspects of the respective human disease conditions and is notlimited to one organ system (such as only lung or skin) akin to themultiorgan disease of scleroderma. Furthermore, c-Jun is highlyexpressed in all human fibrotic conditions analyzed, and thusin vivo c-Jun induction is likely more physiologically relevant thanchemical or infectious conditions that are not involved in thepathogenesis of human disease. We would argue for these reasonsthat our mouse model will be an important tool to further dissectthe pathomechanisms leading to human disease.One such application was our surprising discovery that endog-
enous macrophages can be exploited to eliminate pathologic fi-broblasts. We showed that fibrogenic cells expressed high levels ofthe self-protective don’t-eat-me epitope CD47. It had been shownin various solid cancers and hematopoietic malignancies, and most
recently in atherosclerosis, that blockade of CD47 by antibodies orartificial, high-affinity Sirpα analogs prevents this repressive signalin macrophages, leading to their activation and active phagocytosis(24). The remarkable low toxicity of anti-CD47 treatments, how-ever, suggested that additional alterations in cancer cells are re-quired to induce phagocytosis (21, 25). Here, we show that thisproperty is not limited to cancer cells because fibrosis was effec-tively reversed with anti-CD47 treatment by elimination of fibro-blasts by macrophages. Studies are needed to identify the commonmechanisms between fibrotic cells and cancer cells that allow ef-fectiveness of the anti-CD47 treatment and to identify which othernoncancerous diseases may benefit from such a therapy.In conclusion, our study revealed the unexpected role of c-Jun
as a key and selective driver of organ fibrosis in most humanfibrotic diseases. Our findings suggest that diverse fibrotic syn-dromes may have different etiologies but share common patho-mechanisms centered around activation of c-Jun. The c-Junmouse model may well be suitable to further dissect the patho-genesis of all types of pathologic fibrotic conditions and to de-velop new and effective therapies.
Materials and MethodsAnimal studies were approved by Stanford University Administrative Panels forLab Animal Care (SU-APLAC 30911, 30912, 31026) and human research underIRB11177. We generated the flp-in tetO-c-JUN or flp-in tetO-JUNB transgenicmice as previously described (25) and induced themicewith tetracycline. CyTOFstudies were performed in vivo exactly as described (18, 19). Details can befound in SI Materials and Methods.
ACKNOWLEDGMENTS. We thank Erika Dobos for pathology expertise, DanielHaag for ingenuity analysis and GSEA analysis, Samuele Marro for help withheat maps, Norm Cyr for help with digital images, Farnaz Khameneh for helpwith genotyping PCRs, Patrick Sweeney and Shirley Kwok for help with tissuearray assembly, and the Stanford Immuno core facility for help with cytokine/chemokine quantification. For these studies, I.L.W. was funded by the Virginiaand D. K. Ludwig Fund for Cancer Research; the National Heart, Lung, andBlood Institute; and the National Cancer Institute of the National Institutes ofHealth under Grants U01HL099999 and R01CA86017, respectively. G.W. wasfunded by the Stanford Cancer Institute Fellowship Award; the StanfordPhysician Scholar Society Award; and Institute for Immunity, Transplantationand Infection Young Investigator Award grants. The CyTOF studies weresupported by NIH Grants U19AI057229, U19AI100627, R33CA183654, R33CA0183692, R01GM10983601, R01-CA184968, R01CA19665701, R21-CA183660,R01-NS08953301, 5UH2AR067676, and R01HL120724; Northrop-GrummanCorporation; Novartis Grant CMEK162AUS06T; Pfizer Grant 123214; JunoTherapeutics Grant 122401; Department of Defense Grants OC110674 andW81XWH-14-1-0180; Gates Foundation Grant OPP1113682; and Food andDrug Administration Grant BAA-15-00121.
1. Hunninghake GM (2014) A new hope for idiopathic pulmonary fibrosis. N Engl J Med370:2142–2143.
2. Maier C, Distler JH, Beyer C (2014) Deciphering the pro-fibrotic phenotype of fibro-blasts in systemic sclerosis. Exp Dermatol 23:99–100.
3. Kuter DJ, Bain B, Mufti G, Bagg A, Hasserjian RP (2007) Bone marrow fibrosis: Path-ophysiology and clinical significance of increased bone marrow stromal fibres. Br JHaematol 139:351–362.
4. Gerber EE, et al. (2013) Integrin-modulating therapy prevents fibrosis and autoim-munity in mouse models of scleroderma. Nature 503:126–130.
5. Rockey DC, Bell PD, Hill JA (2015) Fibrosis: A common pathway to organ injury andfailure. N Engl J Med 373:96.
6. Wynn TA, Ramalingam TR (2012) Mechanisms of fibrosis: Therapeutic translation forfibrotic disease. Nat Med 18:1028–1040.
7. Tager AM, et al. (2008) The lysophosphatidic acid receptor LPA1 links pulmonary fi-brosis to lung injury by mediating fibroblast recruitment and vascular leak. Nat Med14:45–54.
8. Liu F, et al. (2015) Mechanosignaling through YAP and TAZ drives fibroblast activa-tion and fibrosis. Am J Physiol Lung Cell Mol Physiol 308:L344–L357.
9. Driskell RR, et al. (2013) Distinct fibroblast lineages determine dermal architecture inskin development and repair. Nature 504:277–281.
10. Yamamoto T (2006) The bleomycin-induced scleroderma model: What have welearned for scleroderma pathogenesis? Arch Dermatol Res 297:333–344.
11. Eferl R, et al. (2008) Development of pulmonary fibrosis through a pathway involvingthe transcription factor Fra-2/AP-1. Proc Natl Acad Sci USA 105:10525–10530.
12. Vainchenker W, Constantinescu SN, Plo I (2016) Recent advances in understandingmyelofibrosis and essential thrombocythemia. F1000 Res 5:5.
13. Wernig G, et al. (2008) Efficacy of TG101348, a selective JAK2 inhibitor, in treat-ment of a murine model of JAK2V617F-induced polycythemia vera. Cancer Cell 13:311–320.
14. Wernig G, et al. (2006) Expression of Jak2V617F causes a polycythemia vera-like dis-ease with associated myelofibrosis in a murine bone marrow transplant model. Blood107:4274–4281.
15. Jochum W, Passegué E, Wagner EF (2001) AP-1 in mouse development and tumori-genesis. Oncogene 20:2401–2412.
16. Lopez-Bergami P, Lau E, Ronai Z (2010) Emerging roles of ATF2 and the dynamicAP1 network in cancer. Nat Rev Cancer 10:65–76.
17. Hasenfuss SC, Bakiri L, Thomsen MK, Hamacher R, Wagner EF (2014) Activator Protein1 transcription factor Fos-related antigen 1 (Fra-1) is dispensable for murine liver fi-brosis, but modulates xenobiotic metabolism. Hepatology 59:261–273.
18. Krishnaswamy S, et al. (2014) Systems biology: Conditional density-based analysis ofT cell signaling in single-cell data. Science 346:1250689.
19. Mingueneau M, et al. (2014) Single-cell mass cytometry of TCR signaling: Amplifica-tion of small initial differences results in low ERK activation in NOD mice. Proc NatlAcad Sci USA 111:16466–16471.
20. Jaiswal S, et al. (2009) CD47 is upregulated on circulating hematopoietic stem cellsand leukemia cells to avoid phagocytosis. Cell 138:271–285.
21. Chao MP, et al. (2010) Anti-CD47 antibody synergizes with rituximab to promotephagocytosis and eradicate non-Hodgkin lymphoma. Cell 142:699–713.
22. Schreiber M, et al. (1999) Control of cell cycle progression by c-Jun is p53 dependent.Genes Dev 13:607–619.
23. Rinkevich Y, et al. (2015) Skin fibrosis: Identification and isolation of a dermal lineagewith intrinsic fibrogenic potential. Science 348:aaa2151.
24. Kojima Y, et al. (2016) CD47-blocking antibodies restore phagocytosis and preventatherosclerosis. Nature 536:86–90.
25. Beard C, Hochedlinger K, Plath K, Wutz A, Jaenisch R (2006) Efficient method to gen-erate single-copy transgenic mice by site-specific integration in embryonic stem cells.Genesis 44:23–28.
4762 | www.pnas.org/cgi/doi/10.1073/pnas.1621375114 Wernig et al.
Dow
nloa
ded
by g
uest
on
Oct
ober
25,
202
0