Embed Size (px)
DESCRIPTION
For assignment help please contact at [email protected] or [email protected]
Citation preview

Unique selling proposition for community pharmaciesFor assignment help please contact
at [email protected] or [email protected]
Despite community pharmacies crucial job of advising customers, and
providing medication and healthcare products, they are coming under
increased pressure from larger retail pharmacy chains (Schmidt and
Pioch, 2005). However, it is not only pressure from large retail
pharmacies that is affecting them, some of the pressure also comes from
supermarket chains that have their own in store pharmacists. The real
issue that community pharmacists face is developing a unique selling
proposition that meets the needs and requirements of the pharmacies
current and future clientele while at the same time developing
relationships with them, and therefore strengthening their loyalty with
the store (Schmidt and Pioch, 2005). This unique selling proposition can
be communicated by the pharmacy to the public through branding.
Kapferer (2008) states that there is more to branding than just naming a
product or service and letting the public see that it has been stamped
with the logo and imprint of a certain organisation. Instead he insists that
branding involves long-term association, a large amount of commitment
as well as good resources and skills. Wood (2000) states that it is
essential that the management of brands is carried out strategically
because when a consumer is making a purchase decision a brand is
regularly the main reason for differentiation between competitive
offerings, therefore the branding of a product is crucial to the success of
a company. Kapferer (2008) believes that brands make the choice for the
consumer easier, the leading brand on the market is obviously well
known, used, and purchased by a lot of people therefore it is presumed
that the product is very good if not the best on the market, this reduces
the likelihood of customers choosing alternative brands. Kara et al.
(2009) shares this belief by stating that brands can give confidence to
customers when making purchase decisions; purchasing a well known
brand implies a lower risk to the customer.
Brands are developed in ways to promote positive images, values and
prestige, if a customer uses a certain brand it is saying something about

what kind of lifestyle they have and can generate a positive identity for
them (Ginden, 1993, Cited in Rooney, 1995). Woods (2000) adds that a
brands image is customized to meet a target markets need and wants by
using the four P's of marketing (product, place, price, and promotion).
Consequently, the success of the use of this method depends on the
customer's loyalty to the brand. In addition, the value of a brand is also
depending on loyalty; if customers are loyal to your brand then this will
guarantee future sales and therefore future cash flows (Wood, 2000).
From Woods' (2000) belief of using the four P's of marketing to position
your brand he points out that each element of the marketing mix is
important when sending out your brands message. For example the price
of a brand says a lot about the prestige associated with it. However,
Jenkinson (1995, p.116) believes that "real brand quality comes from an
emotional bond created by trust, dialogue, frequency, ease of use and a
sense of value and added satisfaction. Loyalty is the reflection of a
customer's subconscious emotional and psychological need to find a
constant source of value, satisfaction and identity". To create a brand
image the customers must first of all be made aware that the brand exists
and once you have distinguished your particular brand from the others, it
is easier to develop its image (Rooney, 1995).
If we wish to examine how successful a particular brand is it is important
to look at its brand equity. "Brand equity is the current financial value of
the flow of future profits attached to the brand itself" (Kapferer, 2008,
p.143). Kapferer (2008) states that brands have developed their financial
value because they have created a lasting impression in the minds and
hearts of influential characters as well as customers. Spence and
Essoussi (2010) proposes that differences in consumers' knowledge of a
certain brand changes their responses to marketing activities, for
example; a strong brand is one in which customers respond more
favourably to marketing activities when the brand is identified, compared
to when it is not. Therefore, to build a successful brand the management
must create and develop a positive brand identity (Spence and Essoussi,
2010).
In 1993, Wentz and Suchard pointed out that firms were applying
branding to more unfamiliar settings where the role of branding is
becoming more popular (Cited in Rooney, 1995). This is obvious in the
area of pharmacy branding, Schmidt and Pioch acknowledged in 2005

that independent pharmacies constitute more than half of the pharmacy
retail market in the UK. Extreme polarisation is seen in the market: it is
greatly concentrated on one side, with the highly branded Boots, Lloyds
and other big names at the forefront of the market, and on the other side
divided into a great number of small and medium sized enterprises
(Schmidt and Pioch, 2005). See Figure 1 for a detailed view of the market
concentration.
(Figure 1: Source: Schmidt and Pioch, 2005)
A study by Clark and White (2009) examined the attitudes of members of
the Australian retail pharmacy industry) to potential entry by one or
more powerful competitors. This study showed that the retail pharmacy
market in Australia is similar to that in the UK (see figure 1). However,
unlike the UK market the Australian pharmacy guild has an agreement
with their government which ensures that retail pharmacies are the only
channel for distribution of prescription drugs (Clark and White, 2009).
They state that in Australia "approximately 45 per cent of pharmacies are
members of a branded chain or banner group" whereas approximately
80% of their grocery industry is held by only 3 companies- making it the
most highly concentrated industry in the developed world (Clarke and
White, 2009, p.281). Factors like these cause many small businesses to
close and discourage new pharmacies from opening. Clark and White
(2009) add that the Australian supermarket industry has pressured the
government to open the supply of prescription pharmaceuticals to them
but have so far not been successful. This would lead to supermarket
chains becoming powerful players in the distribution of medicines,
similar to the UK market. "A dominant brand is an entry barrier to
competitors because it acts as a reference in its category" (Kapferer,
2008, p.24). In other words the dominating and leading brand sets the
standards for new competitors on the market.
Schmidt and Pioch (2005) found that small to medium sizes retail
pharmacies were not making use of branding and add that branding,
when thought of in respect to retail, can take many different forms, for
example, store brands, store sub-brands, and use of national brands.
Perhaps this is one of the reasons that supermarkets in store pharmacies

are becoming more successful. In 2007, sales of own-brands accounted
for 49% of grocery sales in the UK and over 20% in the USA (marketing,
2007). Distributors' brands, in the past, were thought of as 'non-brands',
and these seamed to attract only price sensitive customers (Kapferer,
2008). However, retailer own-brands are now ranked as top brands in
many categories (Huang and Huddleston, 2009). Huang and Huddleston
(2009) suggest that the change we see today in relation to own brands
comes from the fact that retailers are now keen to develop and market
their own-brands rather than just passively distributing the main national
brands. Researchers seem to agree on an emerging pattern when
referring to own-brands and even though the old variety of low price, low
quality retailer own-brands do still exist, the new general trend has been
to go form low price, low- to high-quality products (Huang and
Huddleston, 2009). In the current era own brands now vary their range
to attempt to cover different price levels from low to high compared to
national brands, they also make use of new emerging needs known as
'trends' for example Tesco Fair Trade, Tesco Organic, and Tesco Healthy
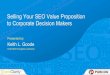
Eating (Kapferer, 2008). According to Huang and Huddleston's (2009)
positioning of retailer own-brands graph (see figure 2) there are 3 types
of retailer own brands.
ImageFigure 1Positioning of retailer own-brands
(Figure 2: Source: Huang and Huddleston, 2009)
According to Corstjens and Corstjens (1995) generics give consumers the
lowest possible price by cutting out all expenses on advertising,
packaging, and marketing. Corstjens and Corstjens (1995) state that the
majority of generic goods are basic, functional products and often have a
commodity-style presentation with minimalist black and white packaging.
Generics do not compete with national brands; instead they are available
as product alternatives for them, and usually have lower quality and
inferior image compared to national brands (Laaksonen and Reynolds,
1994).
Mimic brands are the largest group on the market; these were made to
directly compete with national brands on the market by mimicking them
(Huang and Huddleston, 2009). Mimic brands aim to have an acceptable
quality while at the same time being cheaper than national brands, they

often have similar packaging and are available mainly to offer
alternatives to the more expensive national brands (Burt and Davis,
1999). There have been many occasions in the past were the
manufactures of national brands have taken legal action against the
mimic brand manufacturers because the product was so similar to the
national brand (Huang and Huddleston, 2009).
The third types are retailer own-brands. The most common of retailer
own-brands, are premium own-brands (Huang and Huddleston, 2009).
According to Huang and Huddleston (2009) the introduction of premium
own-brands was aimed to provide customers with a high value-added
product with a modern design and sometimes even better quality than
leading national brands. Often premium own-brands are not priced lower
that national brands (Laaksonen and Reynolds, 1994). Huang and
Huddleston (2009) state that in the UK the use of these premium own-
brands is increasing rapidly, they are earning widespread acceptance
and they can now compete with leading national brands which gives the
consumers a range of brands to choose from. Davies (1998) states that
when the store brand name is based on quality appeal then it will be
easier to market the own-brand as a premium product (Cited in Schmidt
and Pioch, 2005); an example of this is the branding of Marks and
Spencer's own-brand products.
However, Rao and Monroe (1989) provided a model form a study relating
price, perceived quality, perceived sacrifice, perceived value, and
willingness to buy. In this model they confirmed that price has both
objective external properties and subjective internal representations that
are derived from the perception of price: higher prices lead to a higher
perceived quality and to greater willingness to buy (Cited in Kara et al.
2009). Therefore consumers may be wary about the quality of a product
if the price is too low. According to Kim and Sung (2009) when customers
are purchasing a drug such as a pain reliever they often question
whether they should choose a generic or a brand name drug. They say
that if pharmacists were asked about the differences between generic
and brand drugs they might say there is little difference, except for the
name and price. This is because, according to the US Food and Drug
Administration 'a generic drug is identical or bioequivalent to a brand
name drug in dosage form, safety strength, route of administration,
quality, performance characteristics and intended use' (Cited in Kim and

Sung, 2009). Therefore when purchasing branded drugs like these the
consumer is clearly only choosing the brand name because of their
loyalty to the brand or perception of quality they have built around the
brand. Geuens (2004) also believes that store brand and private labels
are becoming increasingly popular and there is continued decreasing
differentiation between competitive offers these days, therefore having a
strong brand name can make a huge difference in customer purchase
decisions.
In consumer behaviour research, a considerable amount of attention has
been given to the construct 'brand personality'; this refers to the set of
human characteristics associated with a brand (Aaker, 1997). Halliday
(1996) says that practitioners view brand personality as a key way to
differentiate a brand in a product category (Cited in Aaker, 1997).
Research has shown that brand personality can even be applied to
medicines; doctors and specialists can attribute human personality traits
to different medicines. Kapferer (2008) found that some of the
personality traits the experts attributed to drugs were linked with
prescription levels. Kapferer (2008) states that; a product (an active
ingredient) cannot be given personality traits whereas a brand can.
Therefore, brands of drugs do have a mental existence and influence in
the minds of the prescribers (Kapferer, 2008). The study also found that
although experts recognised that products themselves are identical and
that brands of these products are the same in the functional benefits they
deliver the experts still prescribed one brand three times more
frequently than the other (Kapferer, 2008). This shows that even in
professional sectors, brands are a psychological reality, which are
present even in the minds of rational decision makers (Kapferer, 2008).
Another factor to consider when examining a company's branding is its
corporate social responsibility. This is a growing concern among firms
due to the populations increased interest in eco-friendly goods. Ethics
show that buyers are expecting, more and more, responsible behaviours
from their brands (Kapferer, 2008). Companies are showing willingness
to demonstrate socially responsible behaviour, as this may have an effect
on the socio-economic context in which they operate, as well as on their
own performance (Morsing and Perrini, 2009). Of course it matters

greatly whether multi-national companies have good ethical business
practices and strong social responsibility however it is also an issue for
small business to address. There are many ways SMEs can engage in
corporate social responsibility: "formal engagement, networking within
and across sectors, volunteerism and giving to charity provide an
extremely fruitful opportunity to invest in social capital, cultivating close
relationships within the social and business environment" (Morsing and
Perrini, 2009, p.3).
Customers may choose to shop in larger stores in comparison to small
chains to take advantage of their loyalty/ Club cards. Loyalty cards are
even more valuable to shoppers since the economic downturn. According
to Colloqy (a US loyalty marketing research and education firm) retail
pharmacy sales have increased 1.5% last year (according to data
published in 2009) despite the fact that sales were declining in most
retail sectors. Experts in the US suggest that this industry is strong and
will see continued growth due to the ageing of the population and the
increase of chronic conditions such as diabetes and high blood pressure
Blank, 2009). Reward and loyalty cards are becoming increasingly
popular in all types of retail environments. Customers can collect 'points'
from purchasing goods or services from pharmacies (Boots advantage
card), Supermarkets (Tesco club card), airlines (Virgin Atlantic airlines
flying club), as well as hotels, clothing stores, hardware stores etc. Blank
(2009) states that, in the US, membership of drug chains in retail reward
programs now account for the largest share of all US loyalty programs
and that these schemes expand the sales of both pharmacy orders and in-
store products.
Liesse (1990) states that; brands that constantly advertise and regularly
change and update their product will excel in their industries and;
companies that believe in outstanding advertising are those who build
leadership brands (Cited in Rooney, 1995). A study carried out by Kim
and Sung (2009) about purchase-decision involvement stated that if
brand names carry a great weight for consumers looking at a certain
product category then they will make their purchase decision based
mainly on brand names and in this case product-decision involvement
would be high because of the importance of the brand. They also stated
that when a customer is loyal to a brand and purchases the brand
regularly the person's product-decision involvement will still be high

because of the perceived strong difference between brands within a
product category (Kim and Sung, 2009). In contrast to this the state that
"if brand names do not meaningfully differentiate (in terms of value-
expressive motives) from other competing brands within a product
category (for example, some popular over-the-counter drugs), consumers
will make purchase decisions based on the utilitarian and functional
features of the product, regardless of brand names (Kim and Sung, 2009
p.511). Their research suggested that purchase- decision involvement
should be measured in terms of four different involvement constructs:
cognitive Vs affective involvement and product Vs brand involvement.
The cognitive Vs affective involvement is similar to the think product Vs
Feel products in the FCB (Foote, Cone, and Belding) grid for analysing
consumer product relationships (Vaughn, 1980). Kara et al. (2009)
suggest that the purchase and use of a product may evoke feeling,
emotions, or provide a means for a person's self expression and identity
formation. Kim and Sung (2009) describe the product Vs brand
involvement as 'utilitarian Vs value -expressive' (Kim and Sung, 2009).
They use the following example to further explain what is meant by this
type of involvement: a customer may be involved in their MP3 player
purchase decision out of many types and features (storage, sound,
design) of the products in the market, and he may also be involved in his
brand decision out of many different brands (Apple, Sony, etc.) (Kim and
Sung, 2009). Their study emphasises that if marketers know the varying
level and kind of involvement their customers have with their brands and
how (cognitively or affectively) their customers are involved with what
product attributes (product functionality or brand) then they could
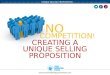
develop optimal and effective marketing strategies (Kim and Sung, 2005).
Figure 2 shows the affective-cognitive purchase-decision involvement
plot.
http://imageserver.ebscohost.com/img/imageqv/actual/g0u/
20090701/9039940.jpg?ephost1=dGJyMNLe80Sepq84v
%2bbwOLCmr0iepq5Srqa4SK6WxWXS
(Figure 2: Source: Kim and Sung, 2009)
The Cognitive-Affective purchase- decision involvement is a tool which
allows researchers and practitioners to compare certain areas of

involvement not only within a product category but also across product
categories (Kim and Sung, 2009).
However, Schmidt and Pioch (2005) found that when pharmacists are
selling medicines they are guided by the ethics of not overcharging their
clients who are looked at as patients rather than consumers. In their
study they found that pharmacists are more focused on improving and
maintaining the services they offer as therapeutic experts than
maintaining a good retail environment. The respondents to their study
agreed that they were healthcare providers first and foremost, and the
retail side of thing come in with a poor second. Pharmacists see
themselves as service providers with a retail element, rather than as
retailers with a service element, which might be a more fitting
description of the competing brands of the multiples where typically the
pharmacy is the smaller section within a much larger commercially
oriented retail shop (Schmidt and Pioch, 2005). Similarly, Brower (2009)
states that one of the biggest sources of conflict between pharmacists
and store managers is a misunderstanding about their respective roles
and goals. Store managers may not understand the very strict rules
governing the pharmacy department and pharmacist practice. On one
hand, store managers often do not recognise customers as patients and
on the other, pharmacists do not recognise each patient as a store
customer (Brower, 2009). Brower (2009) states that the lack of business
education and experience often leaves pharmacists unprepared to meet
non-patient-orientated tasks like preparing a budget or managing
employee relations and suggests that pharmacists should complete a
management course while store managers in turn should understand the
legalities involved with operating a pharmacy.