-
7/30/2019 Unit 1 - Cardiac Care Units
1/29
Page | 1
UNIT ICARDIAC CARE UNITS
Pace makers different types, batteries for pace makers.
ACdefibrillators, asynchronous and synchronous DC
defibrillators,
patient monitoring systems.
Pace makersdifferent types1.What is pace maker?Device that used
to apply a strong electrical shock to the heartmuscle undergoing a
fatal arrhythmia is called pace maker. Theshock changes ventricular
fibrillation to an organized ventricularrhythm or changes a very
rapid and ineffective cardiac rhythm toslower, more effective
rhythm.2.What is Normal Heart-Beat Cycle? / What are cardiac
cycles
two distinct phases? / What do you mean by heartspacemaker?
The cardiac cyclehas two distinct phasesthe diastole phase
andthe systole phase. In the diastole phase, the heart ventricles
arerelaxed and fill with blood. In the systole phase, the
ventriclescontract and pump blood around the body through a system
ofarteries. These events are triggered by the sinoatrial node
acollection of modified myocytes that acts as the hearts
pacemaker.
3.What is Ventricular Fibrillation or defibrillation?Normally
the pulse rate (heartbeat rate) is appropriate for the bodysoxygen
demand. Problems can arise if the heart rate is too low ortoo high.
If the speed is very high it can lead to ventricularfibrillation
(VF) in which the heart muscle quivers and does notpump
efficiently, if at all. This condition is generally fatal if
nottreated quickly. Normal heart-beat can be restored by delivery
of acontrolled electric shock. This process is called
defibrillation.4.What is a Defibrillator?
Defibrillators have been in use for about sixty years. The
earliermachines were comparatively large and not really
portable.Emergency portable defibrillators (also called AEDs or
automaticexternal defibrillators) are today available in many
public buildings,
-
7/30/2019 Unit 1 - Cardiac Care Units
2/29
Page | 2
schools, clubs etc. and small defibrillators can now be
implantedsurgically in patients with certain chronic heart
problems.5.What is Intelligent Defibrillators?
Over recent decades there have been major advances in the
designof defibrillators. Much of this work stemmed from efforts to
produceimplantabledevices. Modern defibrillators include
sensorsthat candetect the cardiac rhythm and are programmed to
decide whethera shock is required and to deliver it correctly.
6.Write short notes on Pacemaker.
A pacemaker is a device that helps regulate the the rhythm of
the
heart as well as the rate at which it beats. It may be
usedtemporarily, such as after open heart surgery, or
placedpermanently, with a minimally invasive procedure.
A normal heart beats at a steady pace, but there are
manyconditions that can make the heart beat irregularly. The rate
maybe too fast or too slow, or the heart may no longer beat in
thenormal "lub-dub" fashion. If the heart is not beating properly,
apacemaker can be used to regulate the rhythm.
A pacemaker sends an electrical impulse to the muscle of the
hearttelling it when to beat. If one of the chambers of the heart
isworking improperly, the pacemaker can be attached there, or
tomultiple chambers if necessary.
Conditions that can be treated with a pacemaker include
atrialfibrillation and bradycardia (slow heart rate). In some
cases, thepacemaker can help insure the left and right atrium or
ventriclescontract at the same time. There is also a
defibrillator/pacemaker
combination available, which is used to treat abnormal
tachycardia(an irregular and overly fast heart rate).
7.What are the types of Pacemakers?There are two primary types
of pacemakers:
-
7/30/2019 Unit 1 - Cardiac Care Units
3/29
Page | 3
a)A standard pacemaker that triggers the chambers of theheart,
and
b)An internal defibrillator/pacemaker combination knownas a
cardioverter defibrillator.
The standard type of pacemaker sends an electrical impulse
viaspecial wires that are attached to the heart. This replaces the
signalthat is sent by the heart, which is faulty in patients who
need apacemaker.A second type of pacemaker, the internal
defibrillator/pacemakercombination, sends an electrical impulse to
the heart to control thehearts rate and rhythm, just as a standard
pacemaker does. Inaddition to that function, it can also deliver a
shock to stop alethal rhythm, a heart rhythm that does not allow
the heart toeffectively function.The idea of the shock is the same
as the shock with paddles thatyou may have seen on television.
However, because the device isattached to the heart with wires, the
shock is much less powerfulthan what you may imagine.Single-Chamber
PacemakersThe heart has four chambers. The left and right ventricle
moveblood outside the heart; the left and right atrium move the
bloodback in. There are also four valves that keep the blood
flowingthrough the heart. Single-chamber pacemakers have just one
wire,
known as a pacing lead. Once the pacemaker is
surgicallyimplanted, the pacing lead extends from the device along
a vein.The pacing lead extends through one of the valves before
finallyattaching to a heart chamber. Since a single-chamber
pacemakercan connect to only one chamber, these devices are
normallyreserved for patients who do not have severe cardiac
problems, andonly an occasional need to stabilize their heart
rates.Dual-Chamber PacemakersDual-chamber pacemakers have two
pacing leads connecting to two
heart chambers. Most pacemakers implanted in the United
Stateseach year are dual-chamber devices. Dual-chamber
cardiacpacemakers more closely mimic the hearts natural beating
than thesingle-chamber pacemaker. Dual-chamber pacemakers are
moreexpensive than single-chamber pacemakers, but there is
someindication that they may actually be more cost effective. In
the
http://adam.about.net/encyclopedia/Implantable-cardioverter-defibrillator.htmhttp://adam.about.net/encyclopedia/Implantable-cardioverter-defibrillator.htmhttp://adam.about.net/encyclopedia/Implantable-cardioverter-defibrillator.htmhttp://adam.about.net/encyclopedia/Implantable-cardioverter-defibrillator.htmhttp://adam.about.net/encyclopedia/Implantable-cardioverter-defibrillator.htm
-
7/30/2019 Unit 1 - Cardiac Care Units
4/29
Page | 4
January 2005 issue of Circulation, Dr. David Cohen, director
ofcardiovascular research at Saint Luke's Mid America Heart
Institutein Kansas City, Missouri, writes that while the
dual-chamberdevices cost $3,000 more initially, the total lifetime
cost mirrors
that of the single-chamber devices. Patients with
dual-chambercardiac pacemakers are also less likely to be
hospitalized for heartfailure than patients with single-chamber
devices, according to Dr.Cohen.Triple-Chambered
PacemakersTriple-chambered pacemakers have three pacing leads, two
for eachventricle and one to an atrium. Typically,
triple-chamberedpacemakers are reserved for patients with
congestive heart failure,a condition that arises when the heart
experiences difficultyperforming its most basic function, pumping
blood. These devices
help improve blood flow through the heart by properly syncing
theventricles.Rate-Responsive PacemakersThanks to their special
activity and breathing sensors, rate-responsive pacemakers have the
ability to self-adjust based on apatients current level of physical
activity, emotional state andmetabolic needs. These devices respond
to physiological changes inthe body rather than to atrial rate, or
heart rhythm.
8.How Does a Defibrillator Work?
In essence the shock circuit in a defibrillator has three
keycomponents: a high voltage source, a capacitor and switches.The
Voltage SourceModern defibrillators use direct current (dc) rather
than thealternating current(ac) which earlier models used. This
poses a problem for designers
of battery-operated devices. Transformers cannot step up
directcurrent.The problem is solved as follows.
-
7/30/2019 Unit 1 - Cardiac Care Units
5/29
Page | 5
A battery drives an oscillator circuit; in effect this produces
acurrent that is switched on and off at a high frequency (e.g.
1000times per second), although it is still going in one direction
only. Ifthis pulsed direct current is fed into a suitable
transformer therequired output voltage can be generated. The factor
by which thevoltage is stepped up is the ratio of the number of
turns on theinput and output coils of the transformer. For example,
if the inputcoil (primary) has 200 turns and the output coli
(secondary) has20,000 turns then the voltage is stepped up by a
factor of 100. A 5V input would then result in a 500 V output. The
alternating outputvoltage is rectified by means of a diode and fed
into a capacitorwhich stores the high voltage charge.
The CapacitorA capacitor consists of two flat conductors or
plates (usually ofaluminium foil) with an insulator between them. A
conducting leadis attached to each plate. In practice the whole
capacitor assembly
is often rolled and inserted in a can with two connections.
CircuitThe diagram shows a simplified version of a defibrillator
circuit.With all switches open the paddles are attached across
thepatients chest. S1is then closed in order to charge the
capacitor. S1is then opened and S2 is closed; this causes the
capacitor to
-
7/30/2019 Unit 1 - Cardiac Care Units
6/29
Page | 6
discharge through the patient, hopefully restoring normal
cardiacrhythm.Energy ConsiderationsThe capacitance of a capacitor
is the amount of electric charge it
can store for every volt applied to it. The unit of electric
charge isthe coulomb (symbol: C). The unit of capacitance is called
a farad(symbol: F). One farad = 1 coulomb per volt. With regard
todefibrillators the amount of energy stored in a capacitor is
veryimportant. It can be calculated as follows: E = C V2, where E
isthe energy in joules, C the capacitance in farads and V the
electricpotential (voltage) measured in volts. This energy, which
may bemore than 100 J, is dissipated in the patients body over a
smalltime interval (about 10 milliseconds or one hundredth of a
second).For example, if the capacitance is 1000 F (microfarad) and
thevoltage is 500 V then the stored energy is 125 J [E = C V2 =
(1000 106)(5002) = 125 J]. Early defibrillators delivering about400
joules sometimes caused further cardiac injury.Electric CurrentThe
electrical resistance of the skin is the main contributor to
thehuman bodys resistance. If the skin is dry the resistance from
onehand to the other might be over 100, 000 ohms. This
isdramatically reduced if the area of contact is large and the skin
ismoistened with a suitable conductive paste or gel. The
electrodes
provided with AEDs are generally self-adhesive and are
pre-coatedwith conductive gel. They can reduce the bodys resistance
(acrossthe chest) to about 20 ohms. Using V=IR we can calculate the
peakdefibrillation current. If V = 500 volts then the current is
25amperes. The pulse lasts only about a hundredth of a second
(10ms) and so the risk of surface burns to the skin is
reduced.WaveformsAs a capacitor discharges its voltage falls and so
does the currentthrough the patient. Plotting the voltage or the
current against time
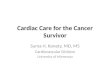
gives a characteristic graph or waveform. The waveform
resultingfrom a single capacitor discharge is monophasic, i.e. the
current ison one direction only. Modern defibrillators are
generally biphasic;successive current pulses are in opposite
directions. Biphasicdefibrillators are considered to be more
effective and today virtuallyall new defibrillators are of this
type.
-
7/30/2019 Unit 1 - Cardiac Care Units
7/29
Page | 7
Monophasic (left) and Biphasic (right) waveforms
Batteries for pace makersBatteries used in Implantable cardiac
pacemakers-present uniquechallenges to their developers and
manufacturers in terms of highlevels of safety and reliability. In
addition, the batteries must havelongevity to avoid frequent
replacements. Technological advances inleads/electrodes have
reduced energy requirements by two orders ofmagnitude.
Micro-electronics advances sharply reduce internal
current drain concurrently decreasing size and
increasingfunctionality, reliability, and longevity. It is reported
that about600,000 pacemakers are implanted each year worldwide and
thetotal number of people with various types of implanted
pacemakerhas already crossed 3 million. A cardiac pacemaker uses
half of itsbattery power for cardiac stimulation and the other half
forhousekeeping tasks such as monitoring and data logging. The
firstimplanted cardiac pacemaker used nickel-cadmium
rechargeablebattery, later on zinc-mercury battery was developed
and used
which lasted for over 2 years. Lithium iodine battery invented
andused by Wilson Greatbatch and his team in 1972 made the
realimpact to implantable cardiac pacemakers. This battery lasts
forabout 10 years and even today is the power source for
manymanufacturers of cardiac pacemakers. This paper briefly
reviewsvarious developments of battery technologies since the
inception ofcardiac pacemaker and presents the alternative to
lithium iodinebattery for the near future.Introduction
Cardiac PacemakerThe pacemaker unit delivers an electrical pulse
with the properintensity to the proper location to stimulate the
heart at a desiredrate. The cardiac pacemaker comprises of a pulse
generator and alead system. The pulse generator houses electrical
componentsresponsible for generating the pulse (via output
circuits) at the
-
7/30/2019 Unit 1 - Cardiac Care Units
8/29
Page | 8
proper time (via timing and control circuits) based on events
sensed(via sensing circuits). It also contains a power supply
(battery) andmay include other elements such as telemetry for
testability andprogrammability and memory (ROM or RAM) to store
data for
diagnostic purposes.Impulses are transmitted to the heart by
means of a lead, which isattached to the pulse generator via the
connector block. A lead iseither unipolar or bipolar; a unipolar
lead contains one insulatedcoil, whereas a bipolar lead contains
two coils, separated by aninner insulation. An outer insulation
shields a lead from theenvironment. The tip of a lead, which
contains an electrode, isimplanted into the inner, endocardial
surface of the heart, theactual location depends on the type of
pacemaker. The pacemakerunit is usually implanted in the pectoral
region, with the lead
running through the right subclavian vein to the internal
surface ofthe heart. A pacemaker is programmed by means of a
programmer,a computer with a special user interface for data entry
and display,and with special software to communicate with the
pacemaker. Thetelemetry head is placed above the location of the
pacemaker;information from the programmer to the pacemaker, and
back, istransmitted by means of telemetry.The casing of the pulse
generator functions as housing for thebattery and all other
electronic and electrical circuits. A connector
block, made of polyurethane, (glass materials were used to
comprisethe connector block in earlier models) is located at the
top of thepacemaker. It serves to attach the pacemaker to the
pacemakerlead(s). The present day pulse generator case is made of
titanium, ametal that is ten times as strong as steel, but much
lighter.Titanium and two of its alloys, niobium and tantalum,
arebiocompatible, they exhibit physical and mechanical
propertiessuperior to many other metals. The modulus of elasticity
(measureof stiffness) of titanium and its alloys range between
100-120GPa.
Extreme resistance to corrosion and durability make titanium
andits alloys ideal materials for hermetically sealed pulse
generatorcases for cardiac pacemakers.Titanium replaced ceramics
and epoxy resin with silicone rubber,which were used for
encapsulation of some pacemakers in the past.To assemble the pulse
generator, the hybrid circuits and the battery
-
7/30/2019 Unit 1 - Cardiac Care Units
9/29
Page | 9
are placed in the titanium case (ASTM Grade 1) in a
speciallydesigned clean room that has no static charge (less than
1%moisture) and no dust in it. Once the hybrid circuits and
thebattery are in the casing, the casing is welded shut with a
high-
powered laser beam. This laser beam gives the pulse generator
ahermetic seal, which means that the device is airtight and
liquid-tight. After welding, the top, or header of the pacemaker is
attachedand the entire device is covered in a thin layer of plastic
(epoxyplastic). This plastic coating further seals the
pacemaker.The casing is a given a kind of elliptical shape and a
typicalpacemaker diagram is shown in Figure 1. This upgrade to
titaniumallowed patients to safely use appliances such as microwave
ovensbecause titanium helps to shield the internal components
andreduce the external electromagnetic interference. In
addition,
titanium casing shields from ground level cosmic radiation.
Figure 1: Typical Pacemaker DiagramBatteries for Cardiac
PacemakersIn 1958, Ake Senning, a thoracic surgeon at the
KarolinskaHospital in Stockholm, implanted myocardial electrodes
and a pulsegenerator with a rechargeable nickel-cadmium battery in
a 40-year-old patient. Senning and his associate, Rune Elmquist, an
engineerwith the Swedish firm Elema Schonander, had developed and
testedthis pacemaker between 1956 and 1958. The pulse generator
failed
within a few hours; a successor lasted about 6 weeks. The
history ofthe implantable cardiac pacemaker is traced from its
inception in1951, through its development and trials in 1958, to
its successfulimplantation in 10 patients in 1960, and on to its
commercialrealization. The usage of implanted pacemakers has been
everincreasing since then. The battery occupies major portion of
the
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1502062/figure/F1/http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1502062/figure/F1/http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1502062/figure/F1/http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1502062/figure/F1/http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1502062/figure/F1/http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1502062/figure/F1/
-
7/30/2019 Unit 1 - Cardiac Care Units
10/29
Page | 10
pulse generator in terms of weight, volume, and size. The
mostimportant factor for a cardiac pacemaker battery is its
reliability.Unlike many consumer products, batteries in implantable
devicescannot be replaced. They are hard wired at the time of
manufacture
before the device is hermetically sealed. From that point on,
thebattery is expected to power the device during final testing at
thefactory, during the shelf life and throughout the useful life of
thedevice while it is implanted. In general the power source of
theimplantable device is the only component, which has a
knownpredictable service life, which in turn determines the service
life ofthe implanted device itself.It is indeed fascinating to see
the breadth and the vision of the earlyinvestigators of implantable
power sources in the almost desperatesearch for a power source that
would enable the pacemaker to last
as long as the expected lifetime of the average patient. This
paperpresents a brief history and review of various types of
batteries usedin cardiac pacemakers since beginning. The smooth
transition fromzinc-mercury, nuclear batteries to the
lithium-iodine batteries arepresented along with product
information obtained from themanufacturers. The technical
advantages of lithium iodine batteryin terms of its longevity, no
gas generation, adaptable shapes andsizes, corrosion resistance,
minimum weight, excellent currentdrain characteristics suitable to
cardiac pacemakers are highlighted
in this paper. The future of cardiac pacemaker batteries in
terms ofalternatives to lithium iodine battery is also
presented.Electrochemical Power sourcesWe need to generate
electrical energy from some other source ofenergy. Chemical energy
is the most practical source and isgenerally used in one of two
possible ways. Fuels can be burnt in aheat engine or fuel cells can
be used. Fuel cells have no movingparts and do not require the
mechanical energy to generateElectrical energy. Chemical energy can
also be stored in two types
of electrochemical power sources, primary cells or batteries,
andsecondary cells or batteries. Primary cells are those used once
andthen discarded, whereas secondary cells can be discharged
andrecharged many times. In theory, many electrochemical
reactionsare reversible. In practice, only a few systems are
worthwhile and
-
7/30/2019 Unit 1 - Cardiac Care Units
11/29
Page | 11
safe. In general, electrochemical power sources have developed
inan evolutionary manner.Battery Performance ParametersThe
definitions for some of the important parts of a battery and
its
performance parameters like voltage, duty cycle, temperature,
shelflife, service life, safety and reliability, internal
resistance, specificenergy (watt-hours/kg), specific power
(watts/kg), etc are wellknown. A good battery design is a
compromise between variousperformance parameters to meet the
requirements of the specificapplication. Critical factors in
selecting a cardiac pacemaker batterytechnology are: minimum and
maximum voltage, initial, average,and maximum discharge current,
continuous or intermittentoperation (size and duration of current
pulses), long shelf andservice life, high specific energy and
specific power, impact, and
good performance in a variety of conditions (temperatures,
dutycycles, etc.). Cardiac pacemaker battery design poses
specialchallenges in development of biocompatible materials,
corrosionand sealing, light weight and flat type, high reliability,
accurate endof life battery predictions, etc.Early
DevelopmentsRechargeable (secondary batteries) nickel-cadmium
batteries wereused in the beginning (in 1958) of pacemaker implants
in humanbeings. They were inductively recharged by the transmission
of
energy to the implanted receiver. The cell voltage was 1.25 V
andthe capacity was 190 mAh. The major problems were two fold,
thefirst being very short life time and the second was to place
theresponsibility for recharging in the hands of patients, which is
not agood medical practice. It was well known that primary or
non-rechargeable batteries would give longer lifetime compared
tosecondary batteries. There are still some rechargeable
pacemakersin use though not sold any more.Some of the early pulse
generators constructed mainly from discrete
components were powered by series-wired mercury-zinc
batteries.Three to six cells in series provided 4-8 V. They were
widely used atthat time (around 1960s). Such mercury-zinc batteries
were cast inepoxy, which was porous to the discharge of the battery
releasedhydrogen and permitted its dissipation, which required
venting andhence could not be hermetically sealed. This allowed
fluid leakage
-
7/30/2019 Unit 1 - Cardiac Care Units
12/29
Page | 12
into the pacemaker at times that caused electrical shorting
andpremature failure. The terminal voltage decay characteristic of
themercury-zinc battery is such that normal battery depletion
resultsin little change in the terminal voltage until the end of
batterys
useful life. This makes failure difficult to anticipate. This
batterywas improved in its design and still the life was only about
twoyears with an abrupt drop in voltage as they become depleted.
Nodevice of this type is currently in use.Biological batteries
(which use power from within the human body)were experimented
unsuccessfully1 for practical use in pacemakers.Nuclear
batterieswere tried successfully for some period. Practicalnuclear
batteries use plutonium (238Pu). It has a half-life of 87 yearsso
the output degrades only by 11% in 10 years. However it ishighly
toxic and 1g in the blood stream could be fatal. Early
pacemakers used metallic plutonium whereas later ones
usedceramic plutonium oxide. The plutonium emits alpha
particles,which impact upon the container and generate heat.
Thermopiles ofdissimilar p- or n-doped bismuth telluride generate
the electricityfor the pacemaker circuits. Though these nuclear
power sourceshad very long life, they were large and created
problems whentravelling between states and countries due to the
presence of theirradioactive fuel. They also must be removed at the
time of deathand returned for proper disposal. Nuclear powered
pacemakers are
no longer sold but still a small number of implanted nuclear
devicesthat remain in use. Nuclear power sources became obsolete
withthe development of lithium batteries.Lithium BatteriesLithium
has the highest specific energy of all but it has only
becomepossible since mid 1970s to manufacture practical
batteries.Because lithium reacts violently with water,
non-aqueouselectrolytes must be used. Organic solvents such as
acetonitrile andpropylene carbonate, plus inorganic solvents such
as thionyl
chloride (SOCl2) are typical, with a compatible solute to
provideconductivity. Many different materials such as sulfur di,
thionylchloride, manganese dioxide, and carbon monofluoride, are
used forthe active cathode material.
-
7/30/2019 Unit 1 - Cardiac Care Units
13/29
Page | 13
IntroductionIntroduction of a lithium iodine battery in 1975
greatly extendedthe pacemaker battery life (more than 10 years for
some models)and replaced the mercury-zinc battery. Lithium Primary
batteries
are used in pacemakers since they meet the requirements of
longlife, low drain current and voltage characteristics. The shelf
life ofprimary lithium cells is typically equivalent to a 10% loss
ofcapacity over five years. This compares with a similar loss
foralkaline cells over only one year. The long shelf life of
lithiumbatteries arises from the lithium metal surface becoming
passivatedby reaction with the electrolyte. All lithium systems are
said to bethermodynamically unstable but kinetically stable. They
produce nogas and hence they can be hermetically sealed. In
addition, theterminal voltage decay characteristic is well behaved,
falling slowly
enough for battery end-of-life(EOL) to be anticipated in
routinefollow up.Lithium batteries are categorized under liquid
cathode cells, solidcathode cells, and solid electrolyte cells.The
liquid cathodesystems, Li/SO2, Li/SOCl2 and Li/SO2Cl2, plustheir
derivatives, are capable of higher discharge rates than thesolid
cathode systems such as Li/MnO2 and Li/CFX. These are notsuitable
for applications in implanted cardiac pacemakers. Howeverlithium
sulfur dioxide batteries are used in automated external
defibrillators (AEDs) that can restore a normal cardiac rhythm
tovictims of sudden cardiac arrest. Solid Cathode Lithium Cells
usesolid cathode materials such as MnO2, CuO, V2O5 and
carbonmonofluoride, (CF)n. They have the advantage of not
beingpressurized, although they cannot be discharged as rapidly
asliquid cathode cells. They are available in button and
cylindricalforms. About 80% (by number) of all lithium batteries in
use are ofthe Li/MnO2 type. The energy density is similar to that
of theLi/SO2 cells when discharged slowly and their slow
self-discharge
characteristic make them suitable for memory backup,
watches,calculators, cameras, mines and munitions, etc. Voltage
delayappears to be less of a problem with solid cathode cells.The
solid cathode cells do not support currents as high as the
liquidcathode ones. This is because the liquid cathode undergoes
adischarge at the surface of the electrode (which comprises a
high
-
7/30/2019 Unit 1 - Cardiac Care Units
14/29
Page | 14
surface area carbon supported on a metal mesh) where
thedischarge products are deposited. In contrast, discharging at a
solidcathode involves diffusion of lithium ions into the bulk of
thecathode, which is a slower process.
Continuous operation of liquid and solid cathode cells above 2A
willlead to a significant rise in cell temperature, so this needs
to beborne in mind for a particular battery application, the
temperaturerise being of more importance for the high pressure
Li/SO2 cells.Possible hazards, like explosions associated with
lithium liquid andsolid cathode batteries are still a concern for
absolute safety and lotof research is still going on to stipulate
the rules and regulations asto how they must be disposed off
towards the end of their life.Solid electrolyte lithium
cells:Several solids, such as lithium iodide,are electronic
insulators but reasonably good ionic conductors and
can be used as the electrolyte in solid electrolyte batteries.
Suchbatteries are characterized by extremely long service life at
lowdrain currents, even at high temperatures. They are very
muchsuitable for applications such as cardiac pacemakers, and
forpreserving volatile computer memory.Since 1972, a variety of
lithium batteries have been used. Theseinclude Li/SOCI2,
Lithium-silver chromate cell [Li/Ag2CrO4],lithium copper-sulfide
cell[ Li/CuS], lithium thionyl chloride
cell,Li/I2-Polyvinylpyridine (PVP), and, in more limited use,
Li/LiI(Al2)3/PbI2,PbS, Pb. In addition to their widespread use
inconsumer products, lithium primary batteries are the power
sourceof choice for a range of medical implants.The lithium
iodine-polyvinylpyride (PVP) is the principal cardiacpacemaker
battery that has been in long use. The internalimpedance (The
resistance of a cell to an alternating current of aparticular
frequency) of the lithium iodine cell is an importantfactor in
battery performance. The greater the impedance, the moredifficult
it is to pass current through the cell. Increased cell
impedance corresponds to a decreased power source at the
cellterminals. The beginning-of-life (BOL) impedance ranges from 50
to100 Ohms. The impedance increases during service to values
from20,000 to 30,000 Ohms during the accumulation of
dischargeproduct.
-
7/30/2019 Unit 1 - Cardiac Care Units
15/29
Page | 15
Lithium Iodine Battery for Cardiac PacemakerThe lithium /
iodine-polyvinylpyridine battery, first implanted in1972 has become
the power source of choice for cardiac pacemaker.Since then,
improvements in cell chemistry, cell design, and
modeling of cell performance have been made. Cells today
exhibitan energy density over three to four times as great as cells
producedin 1972. Well over 3 million pacemakers have been implanted
withthis chemistry, and the system has exhibited excellent
reliability.The battery chemistry provides a long shelf life and
high energydensity. Lithium cupric sulfide was used in some
pacemakersmanufactured by the Cordis Corporation due to its
excellent energydensity. However, due to the corrosive nature of
this compoundmany abrupt pacemaker failures occurred when the
batterychemicals ate through their containment. It is still present
in some
of the already implanted pacemakers but lithium cupric sulfide
isno longer used.Lithium Iodine has two characteristics that make
it an excellentpower source for cardiac pacemaker applications. The
self-discharge rate is very low resulting in a long shelf life. It
has astable voltage through much of the useful life then tapers
down in agradual and predictable manner. This makes predicting the
electivereplacement time safe and easy.The cathode is a complex of
iodine and poly-2-vinyl pyridine (P2VP).
Neither conducts electricity, but when mixed and heated at
149Cfor 3 days, they react into a black viscous paste that
conductselectricity. This is poured into the battery when molten
and cools toform a solid. When this paste contacts metallic
lithium, amonomolecular layer of crystalline lithium iodine forms.
It is amolecular semiconductor that passes lithium ions, as
required forcurrent flow, but not iodine moleculesChemical
ReactionsConventional current flows through a device from anode to
cathode.
For a battery, the current flows from the negative anode,
throughthe battery, to the positive cathode. Oxidation of metal
occurs at theanode,
and reduction of halide occurs at the cathode,
-
7/30/2019 Unit 1 - Cardiac Care Units
16/29
Page | 16
. The combined reaction is,
Conventional current flows from anode to cathode. The
lithiumreacts with iodine to form lithium-iodide, which grows in
volume
and increases the resistance.Internal ResistanceThe internal
cell resistance (Rdc, The resistance to flow of anelectric current
within a cell; the sum of the ionic and electronicresistance of the
cell components) as a function of capacity for PVP-coated and
uncoated (see below) lithium anode are shown in Figure2. The open
circuit voltage (OCV) and voltage at 20 A loadcharacteristics are
shown in Figure 3. It is seen that the voltageabove 2.2V (required
minimum by the pacemaker electronics) is wellmaintained until the
2.5 Ah rating of the battery.
Figure 2: Capacity vs Internal resistance
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1502062/figure/F2/http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1502062/figure/F2/http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1502062/figure/F3/http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1502062/figure/F3/http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1502062/figure/F2/http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1502062/figure/F2/http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1502062/figure/F2/http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1502062/figure/F3/http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1502062/figure/F2/http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1502062/figure/F2/http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1502062/figure/F2/
-
7/30/2019 Unit 1 - Cardiac Care Units
17/29
Page | 17
Figure 3: Run down characteristicsManufacturingLithium is easily
formed into sheets that can be cut to the requiredsizes. It is
easily pressed into specific anode shapes. The lithiumanode is
coated three times with a solution of PVP. The solvent isevaporated
to leave a contiguous film of pure PVP on the anodesurface. The
precoated central lithium anode is corrugated toincrease its area
and lower battery impedance. To obtain lower
impedance, newer designs use more concentrated active
materialsand larger anode surface areas. Multiple anode surfaces
may beused to lower the impedance. The complex of iodine and
poly-2-vinyl pyridine (P2VP) is poured into the cathode case and
allowed tocool.TestingTo maintain high reliability (of the order of
0.005 % failures permonth), cells are designed conservatively. They
are manufacturedunder stringent quality controls, as demanded by
the GoodManufacturing Practices (GMP) issued by the Food and
DrugAdministration (FDA), USA. The qualification testing is
performedunder accelerated test conditions specified for Li/I2-PVP
cells. Thelist includes Non-destructive examinations, thermal
cycling, highpressure, mechanical vibration, temperature /
humidity,mechanical shock, voltage / temperature, seal terminal
strength,
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1502062/figure/F3/http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1502062/figure/F3/http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1502062/figure/F3/
-
7/30/2019 Unit 1 - Cardiac Care Units
18/29
Page | 18
elevated temperature discharge, destructive analysis, and
solventresistance.Longevity and Battery life
estimationLongevity
The pacemaker battery provides energy required for the operation
ofthe circuitry of a pacemaker, which includes the control,
sensingand pulse-generating units. A major concern in using battery
is itslongevity. Longevity of a battery can be determined knowing
batterycapacity (Ah) and current drain (microamperes). The current
drainis dependent on the type of electrode as well as the circuitry
andtype of pulse generation of the pacemaker.Life EstimationSince
the longevity of a cardiac pacemaker means its battery life, itis
essential to have the circuitry to identify the remaining useful
life
of battery in a simple and reliable manner. Monitoring of
internalresistance is a convenient tool for estimation of discharge
level andfor predicting the approaching end-of-service.In many
pacemaker systems, circuits are provided to measure theinternal
resistance of the battery to deduce the remaining life. Withthis
circuit1, the pacemaker is first switched to test mode and
aresistive load is applied to the battery to measure the voltage
drop.The status of the battery is indicated by generating a series
of testpulses. Depending on the internal voltage drop, and thus
the
internal resistance, the frequency of the stimulation pulse
ischanged, which is measured externally. However, this circuit
canonly be used for batteries with increasing internal resistance
as thebattery discharges.To overcome the limitations of the above
technique and to measurethe life expectancy of a battery with
constant internal resistance,another technique was proposed. The
battery test circuit is providedwith a pulse counter and input
logic to measure the consumedcharge from the operating parameters
of the pacemaker and the
number of pulses delivered over a period of time. During each
test,the charge delivered since the last battery test is calculated
basedon the count in the pulse counter, which is then summed to
thecontents of the charge counter in memory. The content of
thecharge counter is a measure of the total charge consumed
andprovides information about the remaining life of the
battery.
-
7/30/2019 Unit 1 - Cardiac Care Units
19/29
Page | 19
The-circuit is implemented internally in the pacemaker unit and
ameans is provided to report the value of the charge counter
wheninterrogated by telemetric methods. The advantage of this
method isthat there is no need to alter the frequency of
stimulation pulses
while testing the battery.In some models-of pacemakers,
approximately twice per day thedevice evaluates the battery status,
which is reported during follow-up; where as in some other models,
battery status is automaticallyevaluated every 11 hours. Battery
status may be displayed in theform of a gauge (showing BOL, ERT,
and EOL) and longevityremaining (> 5 years to < 0.5 years in
0.5 year increments) at 100%pacing.SpecificationsThe battery should
meet the pacemaker pulse requirements in therange of 25 J, a very
small power (compared to 15-40 J forImplantable Cardioverter
Defibrillators). The following are broadspecifications.
a.Open Circuit Voltage: 2.8 Voltb.Control Circuit minimal
voltage: 2.2 Voltc. Control Circuit current drain: 10 Ad.EOL
battery resistance: 10 k Ohmse. Chold: 10 Ff. Oscillator frequency:
167 Hzg. Duty Cycle; 16.7 %h.Ah rating: 2 Ah (typical rating)i.
Reliability: 99.6% probability of survival beyond 8 yearsj. Failure
Rate: 0.005 % failures/month
Weight, Volume, Shape and SizeWeightHalf of the occupied space
is consumed by the internal battery14 incardiac pacemaker.
Therefore the energy density (energy/volume)and specific energy
(energy/mass) are important considerations for
implantable batteries. Compared with lead, the same volume
oflithium provides eight times as much electricity, at
one-thirtieth theweight. The weight of a lithium-iodine battery
varies from about12.5 grams to 15.5 grams for different
manufacturers of thepacemaker unit. The variation in weight is
primarily due to thelongevity and current drain capabilities of the
battery.
-
7/30/2019 Unit 1 - Cardiac Care Units
20/29
Page | 20
VolumeThe volume occupied by the battery in a pacemaker
(pulsegenerator unit) is also about half the total volume. This
varies from5 to 8 cc for the units manufactured by different
manufacturers.
ShapeMost of the cardiac pacemakers are shaped as variations
oncircular or elliptical objects1 to avoid having sharp corners
thatmight penetrate the skin or damage surrounding tissues.
Therefore,the batteries in these devices are shaped to conform to
the overalldevice geometry, and often approximate a semicircle with
a radiusof about 3cm and a depth of 6 to 8mm.SizeTypical dimensions
of an implantable cardiac pacemaker are in therange of 49 mm x 46
mm x 6 mm / 47 mm x 41 mm x 7 mm / 45
mm x 52 mm x 7 mm / 44 mm x 42 mm x 8 mm / 41 mm x 50 mmx7 mm.
The dimensions vary from one model to an another as wellas from one
manufacturer to an another. The battery occupiesabout half of the
size, and volume given in the table. Most of thecompanies use the
lithium iodine battery developed first by WilsonGreat Batch.Future
BatteriesNewer designs are aimed at lowering impedance by using
moreconcentrated active materials and increasing anode surface
area9.
Any increase in service life of implantable medical
devices,including cardiac pacemakers is highly desirable and
important. Inthis connection it seemed worthwhile to use power
sources withhigher energy densities and lower internal resistance.
Indeed,batteries based on other lithium systems were also
proposed;lithium-silver chromate, lithium-cupric sulfide,
lithium-thionylchloride being among them. However all these
batteries wererejected.With several features being added to the
implantable cardiac
pacemakers and other implanted medical devices, manufacturersare
going to need to pull more energy out of the battery morequickly.
Today's pacemakers typically use lithium iodine batteriesand
defibrillators employ lithium silver vanadium oxide,
next-generation systems may slowly migrate toward a newer type
oflithium battery: lithium carbon monofluoride (CFx). CFx
batteries
-
7/30/2019 Unit 1 - Cardiac Care Units
21/29
Page | 21
reportedly offer higher energy density and can be pulsed at
currentsabove 20 mA, which is slightly better than today's
competingbatteries. Such innovations will be necessary,
particularly if OEMvisions of patient management come to fruition.
Medtronic, for
example, has already embarked on a decade-long program, knownas
Vision 2010, which calls for far-reaching use of
deviceconnectivity. Ultimately, engineers say they can foresee a
day whenan implanted heart monitor will detect a problem and call
anambulance; all while the patient lies sleeping.Lithium / carbon
monofluoride (Li / CFx): a new pacemakerbatteryThe reduction in
pacemaker size coupled with addition of morecurrent demanding
functions have motivated the development ofbatteries that can
supply higher current densities at useful voltages
than lithium / iodine batteries in use today while retaining
thevolumetric energy density of that system. The battery can
delivercurrents in the milliampere range without significant
voltage drop.The system is compatible with titanium casing,
allowing a 50%reduction in weight over the same size lithium /
iodine battery.Cells have been designed and tested in these
laboratories and havebeen shown to be suitable for advanced
pacemaker applications.Lithium-polycarbon fluoride batteryThis type
of battery possesses very high energy density and is
capable to ensure pulse discharge current as high as tens
ofmilliamps. At the same time, in contradiction to
lithium-iodinebatteries, lithium-polycarbon fluoride ones use a
liquid electrolyte,specifically 1 M LiBF4 in gamma- butyrolactone.
This fact warrantsspecial attention to a problem of sealing
batteries for liquids andgases (due to electrolyte impurities). It
is very important to checkthe battery leak-tightness, (meeting the
reliability standards laiddown for implantable cardiac pacemakers)
which would qualify formedical applications. The only volatile
component of lithium-
polycarbon fluoride battery is gamma-butyrolactone. For
detectingvolatile substances, gas chromatography is viewed as the
mostsuitable and most accurate technique. Sadly enough,
gaschromatography is not able to be used for
gamma-butyrolactonedetection because it decomposes at a temperature
below its boilingpoint. However, liquid chromatography is suitable
for this analysis,
-
7/30/2019 Unit 1 - Cardiac Care Units
22/29
Page | 22
but it is a much more sophisticated and expensive technique.
Ofinterest, is a simple method of gamma-butyrolactone detection
thatwas developed
DefibrillatorsDefibrillators are devices that apply sharp
electrical shocks to theheart when its beating becomes dangerously
rapidly or chaotic. Theshocks can restore normal heart rhythms
before the malfunctioningheart suffers sudden cardiac arrest, a
seizure than can lead todeath within minutes.Implanted
defibrillators have become a multibillion dollar businessfor
medical device makers following clinical trials showing that
theycould save thousands of lives annually among patients with weak
or
damaged hearts who are at heightened risk of sudden
cardiacarrest. They consist of small battery-powered canisters
implantedinto muscle under the collarbone (usually on the right
side for left-handed patients and the left for those who are
right-handed), whichare connected to the heart by insulated wires
known as leads.An implantable cardioverter-defibrillator (ICD) a
pager-sizeddevice which is implanted in your chestmay reduce your
risk ofdying if your heart goes into a dangerous rhythm and stops
beating(cardiac arrest). You may need an implantable
cardioverter-
defibrillator if you have a dangerously fast heartbeat
(ventriculartachycardia) or a chaotic heartbeat that makes it so
your heart can'tsupply enough blood to the rest of your body
(ventricularfibrillation).Implantable cardioverter-defibrillators
work by detecting andstopping dangerous, abnormal heartbeats
(arrhythmias). Animplantable cardioverter-defibrillator
continuously monitors yourheartbeat and delivers electrical shocks
to restore a normal heartrhythm when necessary.
The leads are used both to sense when the heart is experiencing
arhythm that requires a shock and to deliver the shock.
Defibrillatorcanisters need to be replaced when batteries are
depleted --currently every four to seven years -- but leads are
left in placeunless fractures or infections require them to be
removed.
-
7/30/2019 Unit 1 - Cardiac Care Units
23/29
Page | 23
Many defibrillators are designed to be multi-purpose devices
thatcan also deliver low-powered stimulation to pace
slow-beatinghearts or to help the four chambers of the heart
contract in moresynchronized rhythms.
External defibrillators, which deliver life-saving jolts
throughpaddles applied to the chest, are standard equipment
inambulances and many other emergency response vehicles. In
recentyears, simpler models of such devices known as automated
externaldefibrillators, or A.E.D.'s, have been placed on commercial
aircraft,in offices and schools for public use by citizens who are
trained touse them.External DefibrillatorsExternal defibrillators
are medical devices that diagnose life-
threatening abnormal heart rhythms, or cardiac arrhythmia,
anddeliver electrical energy to the heart to restore its normal
rhythm.They are used in emergency situations on patients who
havecollapsed due to sudden cardiac arrest. When used in the first
fewminutes following collapse, these devices often save
lives.External defibrillators are used in many settings by
medicalprofessionals, emergency responders, and by trained and
untrainedbystanders. The technology is based on decades of research
andevolving knowledge.
There is risk associated with all medical devices, and
externaldefibrillators can malfunction. The defibrillator industry
hasconducted dozens of recalls for external defibrillators,
affectinghundreds of thousands of devices. Additionally, the FDA
hasreceived thousands of reports of external defibrillator
malfunctions.While the FDA continues to advocate use of these
important life-saving devices and is not recommending any change to
currentclinical practices, we believe the devices can be improved
in waysthat improve patient safety.
FDA is taking steps to foster the development of safer,
moreeffective external defibrillators.How an ICD worksWhen you
experience a rapid heartbeat, the wires from your heartto the
device transmit signals to the ICD to send electrical pulses to
-
7/30/2019 Unit 1 - Cardiac Care Units
24/29
Page | 24
regulate your heartbeat. Depending on the problem with
yourheartbeat, your ICD could be programmed for these
therapies:
Low-energy pacing therapy. You may feel either nothing or a
painless fluttering in your chest when your ICD responds to
milddisruptions in your heartbeat.Cardioversion therapy. A higher
energy shock is delivered to dealwith a more serious heart rhythm
problem. You might feel as ifyou're being thumped in the
chest.Defibrillation therapy. This is the strongest form of
electricaltherapy used to restore a normal heartbeat. During this
therapyyou may feel as if you're being kicked in the chest. It may
knockyou off your feet. The pain from this therapy typically lasts
only asecond. There should be no discomfort after the shock is
over.
Usually, only one shock is needed to restore a normal
heartbeat.Sometimes, however, you may have two or more such
shocksduring a 24-hour period. Frequent shocks in a short time
period areknown as ICD storms, and they may understandably cause
you toworry. If you experience ICD storms, you should seek
emergencycare to see if your ICD is working properly or if you have
a problemthat's making your heart beat more abnormally. If
necessary, theICD can be adjusted to deliver the appropriate number
of shocks.Additional medications may be needed to make your heart
beat
regularly and decrease the chance of an ICD storm.
Who needs an ICD?You're a prime candidate for an ICD if you've
had ventriculartachycardia, survived a cardiac arrest or have
fainted from aventricular arrhythmia. You may also benefit from an
ICD if youhave:
A history of coronary artery disease and prior heart attack that
has
led to a weak heart.A heart condition that involves abnormal
heart muscle, such asenlarged (dilated cardiomyopathy) or thickened
(hypertrophiccardiomyopathy) heart muscle.An inherited heart defect
that makes your heart beat abnormally.These include long QT
syndrome, which can cause ventricular
-
7/30/2019 Unit 1 - Cardiac Care Units
25/29
Page | 25
fibrillation and death even in young, active people with no
signs orsymptoms of heart problems. Having other rare conditions
such asBrugada syndrome and arrhythmogenic right ventricular
dysplasiaalso may mean you need an ICD.
There are three major components to consider when studying
adefibrillator: a capacitor, an inductor, and a power supply.
Thesethree components will be explored in depth. Specifically,
theinteraction between these three components is what
allowsdefibrillators to effectively restore proper cardiac
rhythms.
I.) Capacitors:One of the key components of a defibrillator is a
capacitor. The capacitor of
a defibrillator stores a large amount of energy in the form of
electrical charge.Then, over a short period of time, the capacitor
releases the stored energy. The
capacitor itself contains numerous components: a pair of metal
plate conductors
and an insulator. The insulator is in the middle of the
conductors and does not
loose electrons. On the other hand, conductors easily loose
electrons and promote
current flow.
To quantitatively describe a capacitor, one calculates the
capacitance, the
ability to store charge. The formula to calculate capacitance
relates charge (Q),
voltage (V), and capacitance (C):
C = Q/VA capacitor has 1 farad of capacitance if a potential
difference of 1 volt is
present across its plates, when they hold a charge of 1 coulomb.
Capacitors
typically have values of microfarads (F = 106
F). According to the equation,
capacitance is directly proportional to charge and indirectly
proportional to
voltage.For a parallel plate capacitor, as in the case of a
defibrillator, a relationship
can be established between the capacitance, the dielectric
constant, the area of plate
overlap, and the distance between plates. Capacitance is
directly proportional to
area and indirectly proportional to distance between plates:C =
(Eo x A) / d
-
7/30/2019 Unit 1 - Cardiac Care Units
26/29
Page | 26
The mechanism of action of a defibrillator is depicted below in
Figure 1.
When the switch is in position 1, direct current from the power
supply is
applied to the capacitor and electrons flow. Therefore current
flows and a charge
begin to build up on each electrode of the capacitor.
Specifically, the lower plate is
more negative and the upper plate is more positive. The build-up
of opposing
charges creates a potential difference across the plates (V)
that opposes theelectromagnetic force of the power supply (E).
Additionally, the electromagnetic force (E) can also be related
to the area of
plate overlap (A), the charge (Q), and the dielectric constant
(Eo) with the
following equation:E = Q / (Eo x A)
Charging a Capacitor:Charging a capacitor is an exponential
process. Specifically, the work done
(W) to move charge (Q) through a potential difference V is: W =
VQ. Therefore, as
the voltage increases more work is required.
-
7/30/2019 Unit 1 - Cardiac Care Units
27/29
Page | 27
The charged capacitor is a store of potential energy, which may
be released
on discharge. Thus, the amount of energy stored in a capacitor
is CV and in order
to store energy, work must be done.Discharging a Capacitor:
In a defibrillator, the circuit (depicted in Figure 2) is
completed when
paddles are applied to the patients switch. Electrons on the
negative, lower platemove through the patient and then to the upper
plate. Thus three key steps happen
in sequence: electric current flows, electrical energy is
released, and the potential
energy between the upper and lower plates is zero. As the
electrons are transferred
from the lower plate, the potential difference decreases. The
rate of discharge
declines as the potential difference between the upper and lower
plates falls.A graphical image differentiates between the
chagrining and discharging of
a capacitor. Permission was obtained to reproduce this
image.
Source:http://www.tpub.com/neets/book2/3d.htmEnergy
Delivery:
The energy that is delivered can be calculated using the
following
relationship: Energy = QV/2. Thus the energy delivered is
directly proportional to
stored charge and voltage. Additionally, the energy stored in a
capacitor can be
related to the electric field, area, and distance:U = energy =
(Eo) E
2(Ad)
Thus, the energy of a capacitor is directly proportional to area
of the plates
and distance between the plates. Additionally, if the electric
field doubles, the
energy will quadruple.
http://www.tpub.com/neets/book2/3d.htmhttp://www.tpub.com/neets/book2/3d.htmhttp://www.tpub.com/neets/book2/3d.htmhttp://www.tpub.com/neets/book2/3d.htm
-
7/30/2019 Unit 1 - Cardiac Care Units
28/29
Page | 28
II.) Inductors:Defibrillators are needed to shock the heart back
in regular rhythm. Thus,
the current that is delivered must last for a several
milliseconds. However, a
discharging capacitor delivers charge and current very fast.
Inductors, coils of wire
that produce a magnetic field when current flows through them,
prolong the
duration of current flow. Specifically, inductors generate
electricity that opposes
the motion of current passing through it. This opposition is
called inductance.
Inductors typically have values of microhenries (H).III.) Power
Supply:
Step-up transformers are transformers that increase voltage. In
the case of
defibrillators, step-up transformers are used to convert the
main voltage of 240 VAC to 5000 VAC. A step-up transformer is used
in defibrillators because this
allows the doctor to choose among different amounts of charge.
The control switch
is calibrated in energy delivered to the patient (J), because
this determines the
clinical effect or physical impact that a patient will
experience. As an additional
energy source, many defibrillators also have internal
rechargeable batteries.
What are the patient and safety issues associated with
defibrillators?I.) Patient Issues:
Successful defibrillation depends on delivery of the electrical
charge to the
myocardium. Only part of the total current delivered (about 35
A) flows through
the heart. The rest is dissipated. First, the skin and the rest
of the body counteract
the flow of the current. The skin and thoracic wall act as
resistors in series.R (eq) = R1 + R2 + R3
Other intrathoracic structures act as resistors in parallel.R
(eq) = (1/R1) + (1/R2) + (1/R3)
The total impedance is about 50150 ohms; however, repeated
administration of shocks in quick succession reduces
impedance.
-
7/30/2019 Unit 1 - Cardiac Care Units
29/29
Page | 29
II.) Safety:Key safety concerns exist regarding the use of
defibrillators. These concerns
must be taken into account before using a defibrillator on a
patient with irregular
cardiac rhythms:The patient must not already be in sinus
(normal) rhythm.The leads of the defibrillator must be properly
connected, ensuring current
flow.Placement of paddles should follow specific guidelines:
they should be
placed along the long axis of the heart, they should not cover
the transdermal
patches because they are flammable, they should not be placed
near metal
objects because currents will travel through the metal (path of
least
resistance) and cause burning.All sources of oxygen must be
removed from the patient during
defibrillation, because it supports combustion.No one from the
medical staff should touch the bed, patient or any
equipment connected to the patient during defibrillation.Fluids
may conduct electricity; therefore it is important to ensure that
the
immediate area is clean and dry.The defibrillator should not be
charged until the paddles are applied to the
patients chest, because accidental discharge from open paddles
may cause
injury.