Embed Size (px)
Citation preview
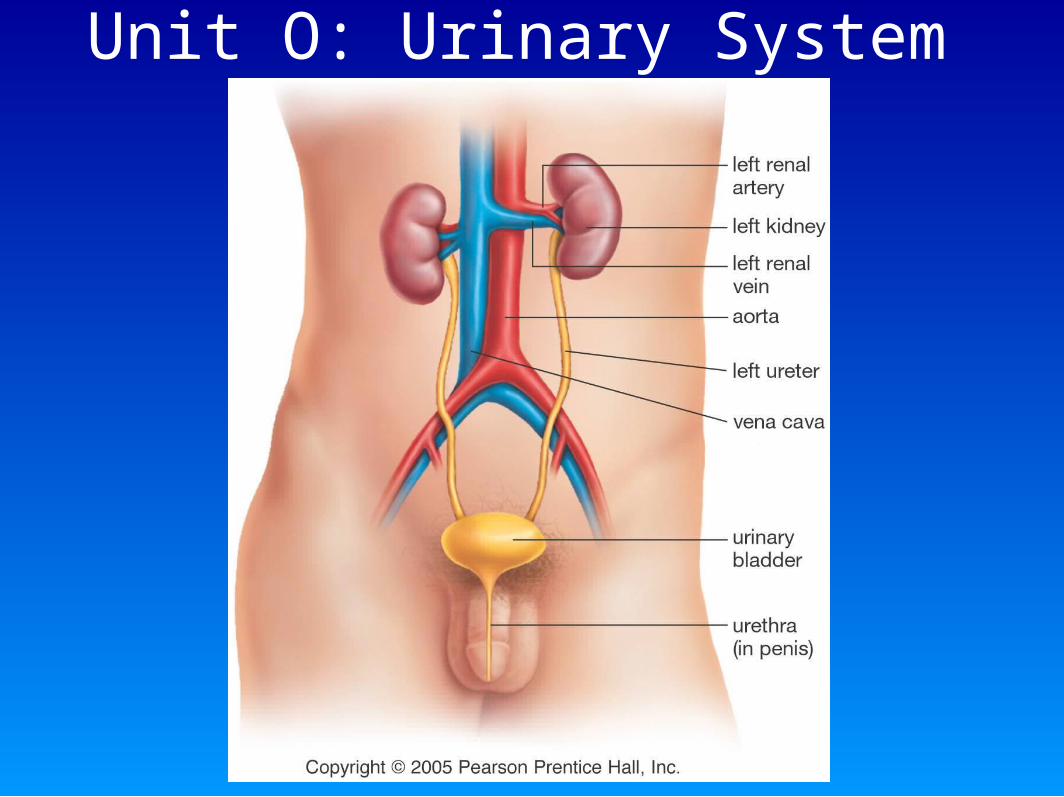
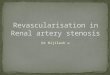
Unit O: Urinary System
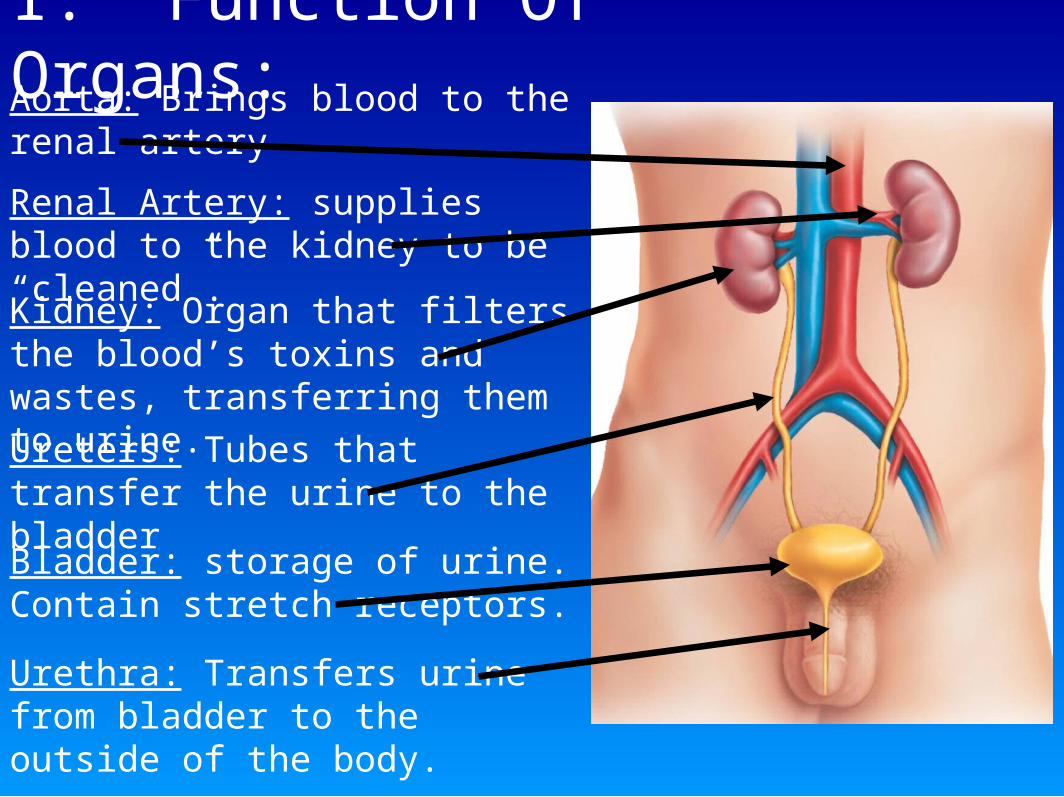
I. Function Of Organs:Aorta: Brings blood to the renal artery
Renal Artery: supplies blood to the kidney to be “cleaned”.
Kidney: Organ that filters the blood’s toxins and wastes, transferring them to urine.
Ureters: Tubes that transfer the urine to the bladder
Bladder: storage of urine. Contain stretch receptors.
Urethra: Transfers urine from bladder to the outside of the body.
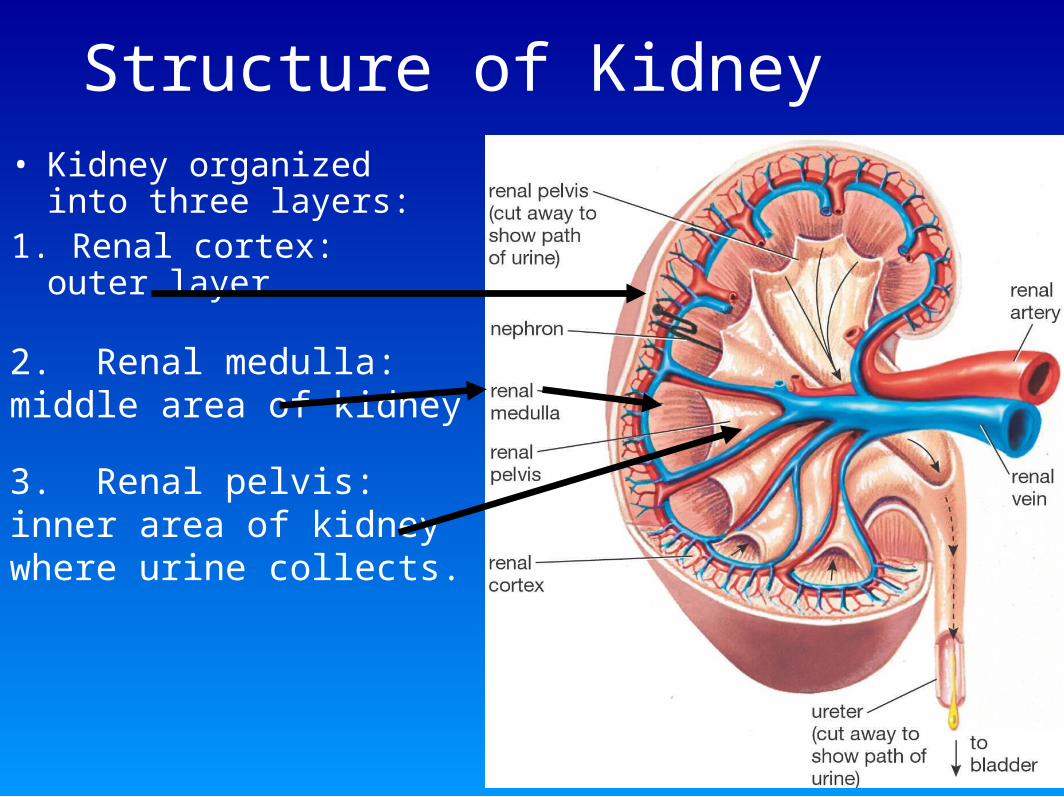
Structure of Kidney• Kidney organized into
three layers:1. Renal cortex: outer
layer
2. Renal medulla: middle area of kidney
3. Renal pelvis: inner area of kidney where urine collects.

II. Urinary System Removes Metabolic Wastes:
• The functions of the urinary system are many: the kidneys remove toxins and wastes from the blood:
H+ ionsUreaWater soluble vitaminsHistaminesPenicillin and other drugs
Salts: K+, Na+, HCO3-, if excess present.

III. Functional Unit of Kidney: The Nephron: Label your diagram:
Parts of the Nephron:1. Afferent arteriole: brings blood into the glomerulus for
pressure filtration.
2. Glomerulus: A special capillary where pressure filtration takes place.
3. Efferent arteriole: take blood to the peritubular capillary network.
4.Bowman’s Capsule (Glomerular capsule) Catches the fluids removed from blood with pressure filtration.
5. Proximal convoluted tubule: The location of selective reabsorption., where nutrients are returned to the blood.
6. Loop of Henle: Allows water to leave and reabsorb into blood.
7. Distal convoluted tubule: Where Tubular secretion occurs.
8. Collecting Duct: Urine collects here at end of tube and is passed to the renal pelvis of Kidney.
Animation:
Kidneyb.ram
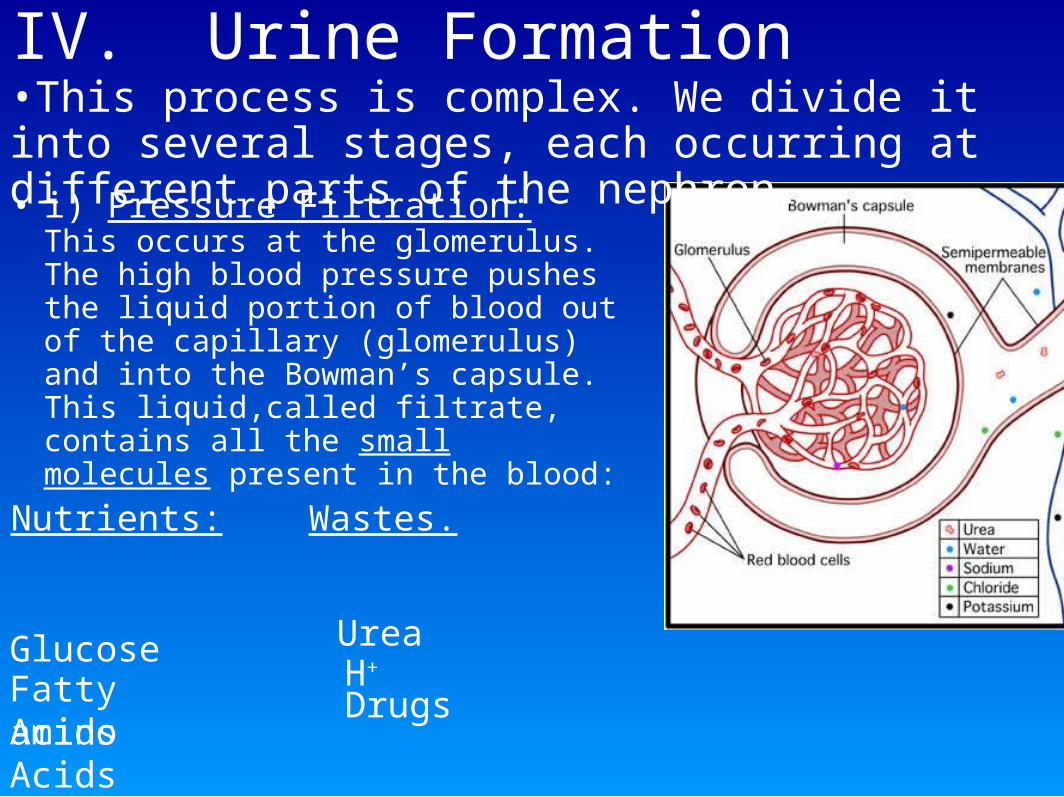
IV. Urine Formation
• i) Pressure Filtration: This occurs at the glomerulus. The high blood pressure pushes the liquid portion of blood out of the capillary (glomerulus) and into the Bowman’s capsule. This liquid,called filtrate, contains all the small molecules present in the blood:
Nutrients: Wastes.
Glucose
Amino AcidsFatty acids
UreaH+
Drugs
•This process is complex. We divide it into several stages, each occurring at different parts of the nephron.
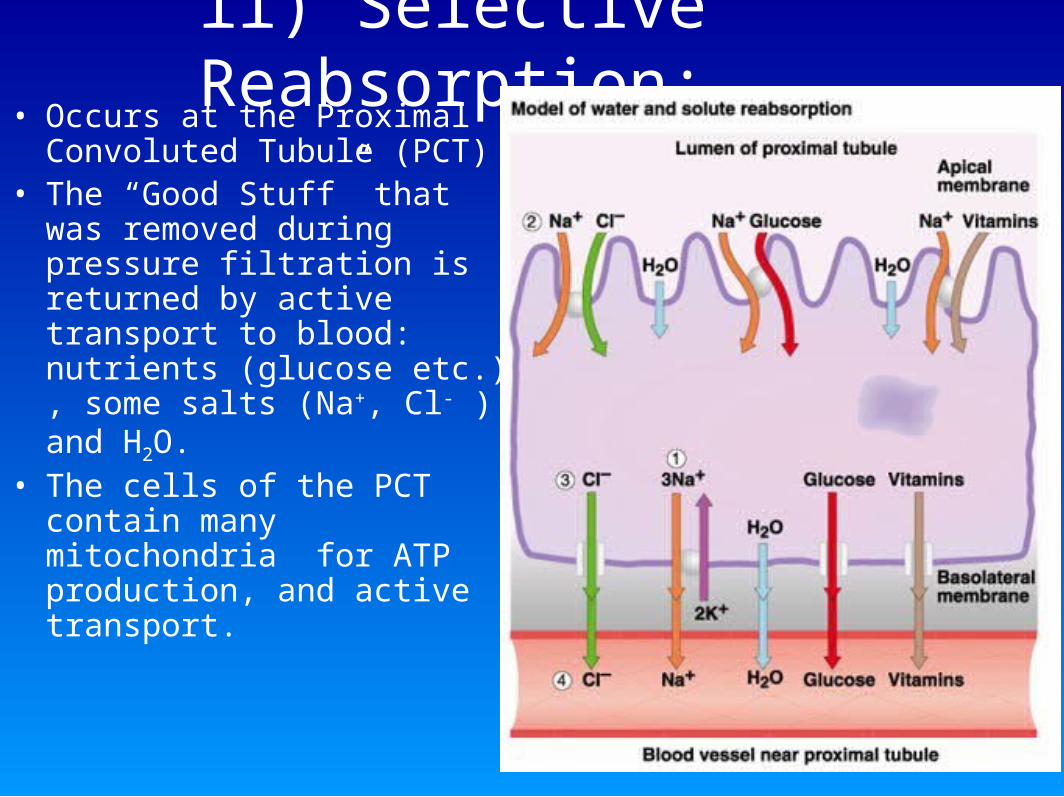
ii) Selective Reabsorption:• Occurs at the Proximal
Convoluted Tubule (PCT)• The “Good Stuff” that was
removed during pressure filtration is returned by active transport to blood: nutrients (glucose etc.) , some salts (Na+, Cl- ) and H2O.
• The cells of the PCT contain many mitochondria for ATP production, and active transport.
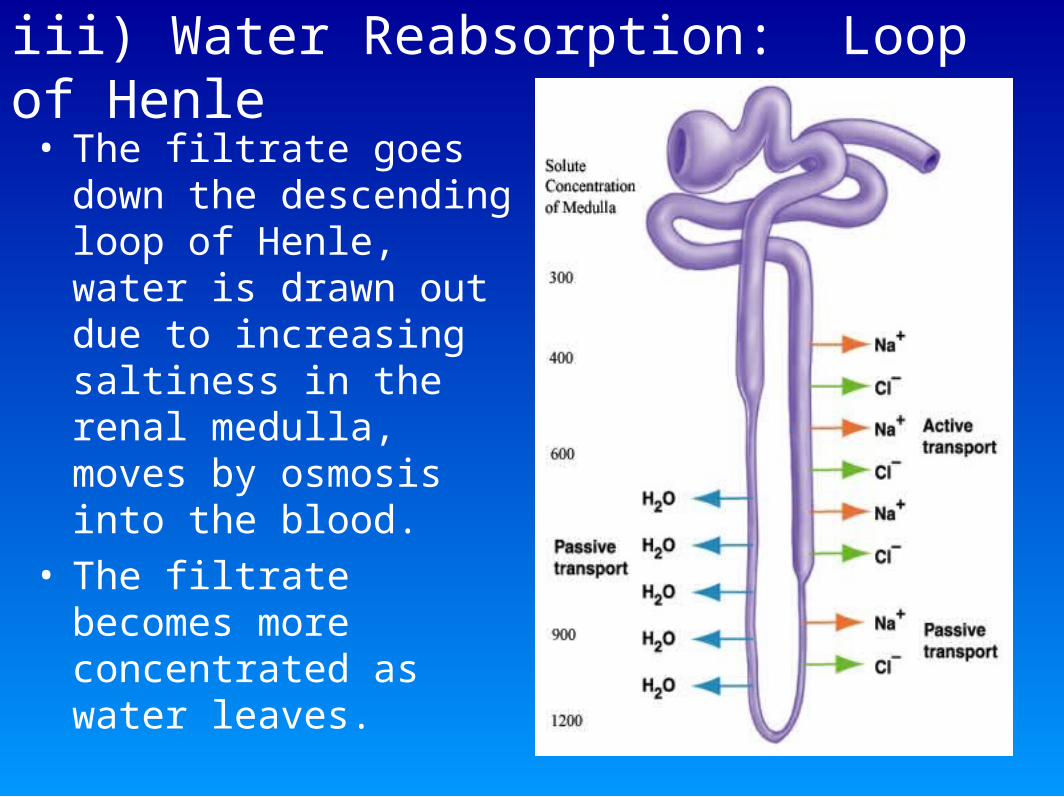
iii) Water Reabsorption: Loop of Henle• The filtrate goes down
the descending loop of Henle, water is drawn out due to increasing saltiness in the renal medulla, moves by osmosis into the blood.
• The filtrate becomes more concentrated as water leaves.
iv) Salt Balance• The ascending loop of Henle moves Na+ out of the
filtrate, initially by diffusion, then by active transport. This causes the medulla of kidney to be very salty. Chloride ions follow sodium.
• The ascending loop is impermeable to water, therefore filtrate remains concentrated.
• As filtrate reaches the cortex, most of the Na+ has been removed by active transport and the filtrate is isotonic with the extracellular fluid at the distal convoluted tubule.
• The water that left the filtrate in the loop of Henle diffuses by osmosis back into the blood at the peritubular capillaries.
v) Tubular Secretion:• At the distal convoluted tubule
(DCT) last minute adjustments are made.
• Penicillin, histamines, vitamins that are in excess in blood are added to filtrate by active transport (called secretion).
• Potassium and sodium concentrations are similarly adjusted.
• pH is balanced by secreting excess H+ ions if blood is acidic, or secreting HCO3
- if blood is too basic (high pH). Reabsorption of H+ ions from filtrate to blood also occurs here if pH of blood is too high.
BloodTubule
vi) Collecting Duct:• The urine is collected here and last minute
adjustments are made according to the concentration.
• Water can be reabsorbed (added to blood) or secreted under the action of antidiuretic hormone (ADH)
• Urine from millions of collecting ducts transfers to the renal pelvis and eventually to the ureters.
V) Hormones: ADH• Hypothalamus detects low blood volume (and low
pressure) and makes Antidiuretic Hormone (ADH), also known as vassopressin, which is stored in the posterior pituitary gland.
• Pituitary releases ADH into blood supply.• ADH binds to receptors on the collecting duct’s cells,
causing more water pores (aquaporin) to be made in cell membranes of duct.
• Results in more water reabsorbed into the blood and blood volume increases.
• When blood volume increases -so does pressure. Higher pressure shuts down ADH production.
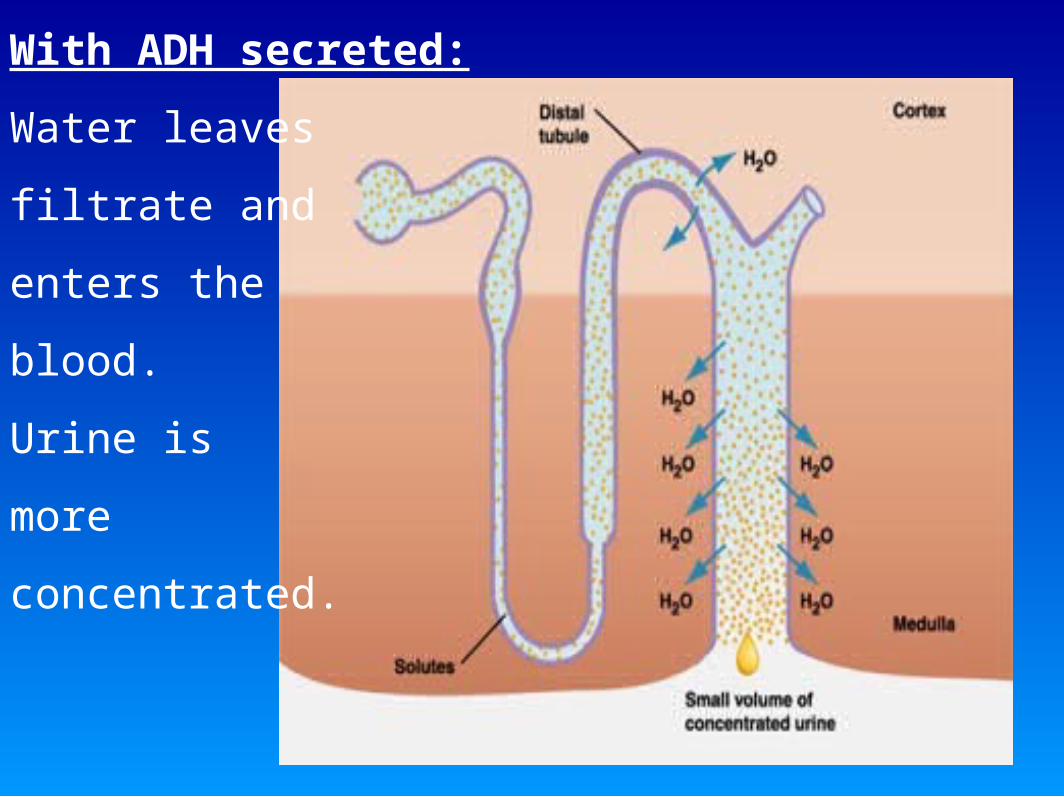
With ADH secreted:
Water leaves
filtrate and
enters the
blood.
Urine is
more
concentrated.
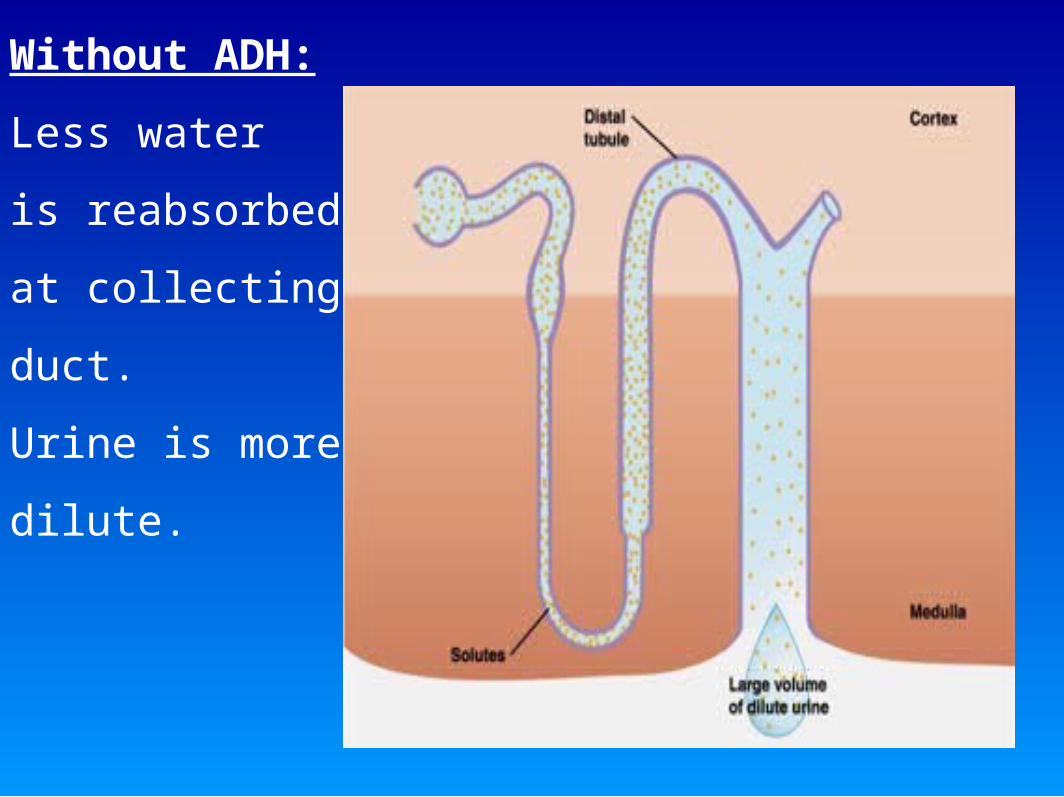
Without ADH:
Less water
is reabsorbed
at collecting
duct.
Urine is more
dilute.

VI) Hormones: Aldosterone• Low blood pressure, detected at the
juxtaglomerular apparatus, initiates a series of complex hormone interactions.
• Results in a steroid hormone: aldosterone:made in adrenal gland (cortex region) to be released.
Aldosterone action:
• Targets the cells of the distal convoluted tubule resulting in more Na+ reabsorption (and K+ excretion) with Na+/K+ pump.
• Results in blood plasma being more salty, therefore water is also reabsorbed by osmosis and blood volume goes up.
VII) Substances Affecting Urine Formation:
• Diuretics: A substance that increases urine flow. Eg. Alcohol which inhibits ADH synthesis therefore urine is dilute. (A hangover is dehydration brought on by too much urination combined with the need for H2O for alcohol metabolism).
• Diabetes: excess glucose is secreted in the urine of diabetics. The glucose also causes more H2O to be excreted so urine flow is frequent and high in hyperglycemia.