Embed Size (px)
Citation preview
Universal health cover for IndiaEvolving a framework for healthcare reimbursement methodologies
September 2013
Contact us:
FICCI, Federation HouseTansen Marg, New Delhi - 110 001Tel: 011 23357246 (D), 011 2373 8760 - 70 (Ext. 220/ 438/ 246)Fax: 011 2332 0714, 011 2372 1504Email: [email protected]
Visit us at: www.ficci-heal.com

ForewordIn 2012, FICCI carried out a study to examine the global and Indian scenario on healthcare financing and suggested a way forward to achieve universal health coverage (UHC), keeping in view the intent of our government to move towards it during the twelfth plan period. Our study substantiated, that focus on rationalising cost of care is one of the critical factors for an effective and sustainable UHC.
In its endeavour to make healthcare accessible and affordable, increasingly, the Government is seen to be moving from being a provider to payor, with initiation of Government Sponsored Health Insurance schemes with estimations of covering 500 million people by 2015. This trend has encouraged forging of public private partnerships with new private hospitals being set up to cater to scheme insured patients, along with existing hospitals enhancing their capacities to empanel with these schemes.
However, there is immense confusion and dissatisfaction amongst all stakeholders in terms of cost of care as the healthcare scenario in the country is still evolving and is rife with lack of standard practices. Also, variation in quality of healthcare delivery is dependent on a multitude of factors, such as availability of clinical expertise, infrastructural capabilities, geographic locations etc., both in the government and private healthcare set ups.
This joint working paper by FICCI and EY endeavours to demystify the cost of care by studying the methodologies followed in countries like USA, England, France, Germany, Korea etc., analysing the current practices in schemes like ESIS, CGHS, RSBY, Rajiv Arogyasri and private and public hospitals and diagnostic companies and to suggest a way forward. We hope to carry on this work to develop a sustainable economic model for healthcare, where the public and private sectors could work in collaboration and also help to understand the price leverage that the health sector can attain in terms of medical tourism and consumables, as compared to other countries.
FICCI as a change agent has been working diligently in supporting the government to bring about the requisite policy changes for providing the right impetus to the growth of the health services sector that would reach out to the masses. We are grateful to Ministry of Health and Family Welfare, Government of India for supporting FICCI – HEAL 2013 on the theme “Sustainable Quality Healthcare” on September 2 & 3, 2013 in FICCI, New Delhi. We hope that the deliberations in the conference will help us in coming up with concrete recommendations that will be submitted to the Government at the highest level for consideration.
Rajen PadukoneCo-Chair, FICCI Health Services Committee
Sangita ReddyChair, FICCI Health Services Committee
G S K VeluCo-Chair, FICCI Health Services Committee
Last year, we had released a paper on Universal health cover that covered the basic framework for the effective implementation of UHC in India with a detailed focus on financing requirements. For UHC’s dream to be become a reality, what is needed is political will, an enhanced focus on primary care, an effective PPP framework, robust governance for patient safety and a pricing proposition relevant for India. The focus of this year’s report is on PPP, and what we have attempted to do is put in place a comprehensive framework aimed at facilitating effective, practical and sustainable public procurement of private services.
In the recent past, the Government has been increasingly focusing on health financing, particularly to provide access to health care to the underprivileged BPL section of our fellow citizens. However, such programs are also frequently extended to the larger portion of the population. It is a fair estimate that around 50% of our country’s population will be availing this facility in days to come. While there are multiple schemes in operation at the Central and state levels, where private providers are contracted for providing health care services paid by the Government, one key point of contention has been and continues to be the reasonableness of existing reimbursement programs. Currently, there are several issues that may compromise patients’ safety and dis-incentivize quality conscious providers in their quest to actively participate in making affordable and quality care for all a reality.
While the Government’s focus on providing health care to the underprivileged is a laudable initiative, this is the long overdue right of all Indian citizens and not a provision to oblige them. Therefore, it is crucial that we have a sharp focus on first setting right the gaps that can compromise patients’ safety and access to quality health care in the long run.
The report is a sincere attempt to suggest means of addressing some such gaps. We are grateful to FICCI for providing us this opportunity to collaborate with it as well as all individuals who have contributed their valuable insights on the subject.
It has been an enriching experience for us to work on this report, and we hope it further strengthens our country’s provider payment mechanism for government-sponsored health schemes.
Hitesh SharmaPartnerEY LLP
Muralidharan M NairPartnerEY LLP
Sumit GoelAssociate DirectorEY LLP
2 Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
Executive summary
BackgroundLast year’s EY and FICCI’s report, for HEAL 2012, focused on understanding the challenges and imperatives for delivering Universal Health Coverage (UHC) in India and attempted to demystify certain aspects of financing needs in the context. One of the key observations of the report was that neither the Government nor the private sector may alone have the capacity and resources to effectively respond to the agenda of UHC in India. Hence active collaboration between Government and private sector was envisaged as a non-negotiable imperative for achieving UHC. In the same context it was also envisaged that the trend of the Government acting as health financier rather than health care provider, already being seen in several state and central Government schemes, will gain further strength in times to come. This will happen for the following three reasons:
a) Providing access to health care services, especially for underprivileged segments of society, emerging as a strong political agenda. Between 2004 and 2010, the number of people covered by different government-sponsored health insurance schemes increased from 37 million to 243 million and is expected to cross 500 million people by 20151.
b) The Government may not be in a position to invest the capital required to create public health care infrastructure to address the supply gap (estimated at between INR1265 billion and INR2493 billion over the next 10 years).
c) Consumer preference for private health care (65% of in-patients opt for treatment from private providers) and asymmetry of infrastructure and human resources (55% of in-patient beds in public hospitals with 80% of human resources employed by the private sector) necessitates public-private partnership to deliver the universal health coverage agenda.
Hence public purchase of health care services from private providers will be an important feature of operationalising the UHC agenda. This will necessitate a robust provider-reimbursement mechanism to be in place.
Given that most government-sponsored health insurance schemes in India focus primarily on reimbursement of in-patient care, for the purpose of this paper our focus has also been on provider reimbursement mechanisms for in-patient care.
Current context – provider reimbursement mechanismsWhile there are multiple challenges that affect provider reimbursement methodologies employed by government- sponsored health insurance schemes in India, the most significant is the lack of attention towards patient safety. Provider reimbursement rates are currently fixed by most government-sponsored health insurance schemes using economics-focused models such as L1-based competitive tendering by participating hospitals, which assumes that all providers are equivalent in terms of the quality of care they provide. However, when it comes to assurance on quality, while there are basic eligibility criteria for empanelment of providers under these schemes, there is negligible monitoring of quality standards post empanelment. This is illustrated by a study conducted as part of a small survey of 26 RSBY empanelled hospitals in Kerala, generally credited as one of the most progressive states in terms of health indicators, which found that only 19%, 31%, 38%, 46% and 50% of hospitals reported the availability of pediatricians, gynecologists, surgeons, radiologists and exclusive nurses for OT/ delivery rooms respectively2. Accredited provider capacity in India is also in extremely short supply with less than 1% of the ~25,000 (with more than 50 beds each) healthcare providers accredited by NABH.
Global experiences have demonstrated that along with preventive and primary care, patient safety is crucial for effective management of health care costs in the long run.
1. “Government Sponsored Health Insurance in India”, Gerard La Forgia and Somil Nagpal, World Bank, 2012
2. “RSBY-CHIS Evaluation Survey“ , Research Institute, Rajagiri College of Social Sciences, Kerala, India, 2009
3Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
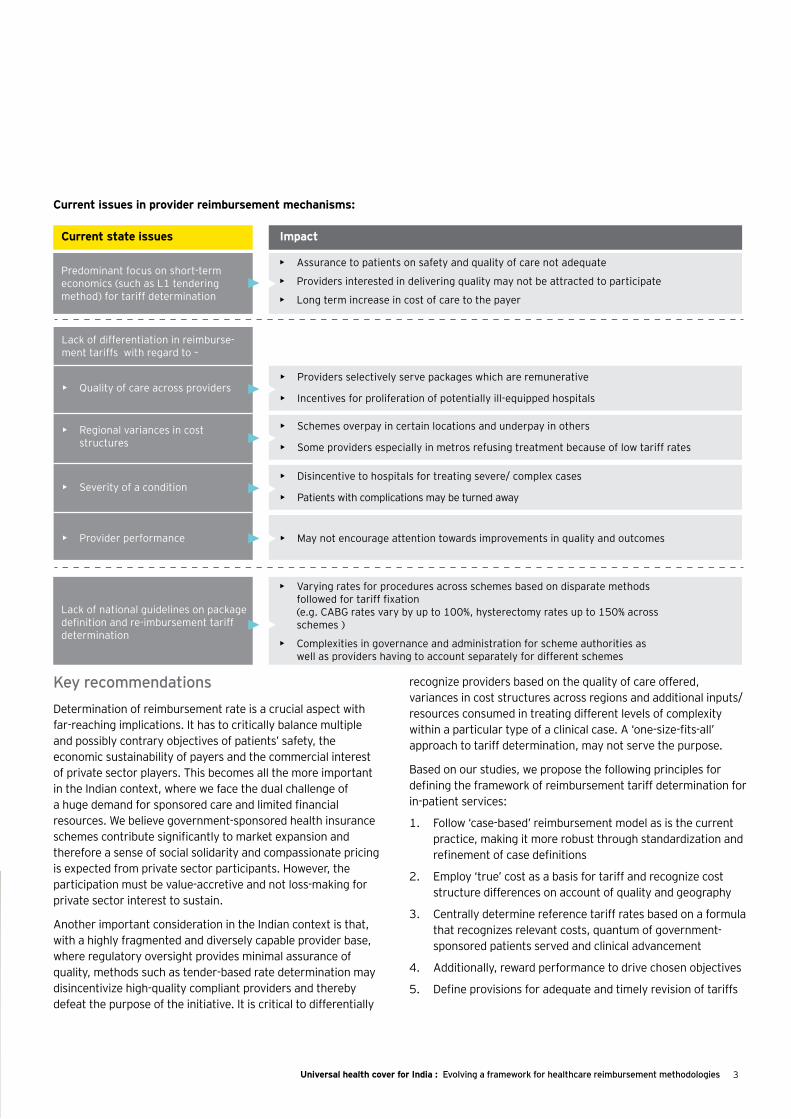
Current issues in provider reimbursement mechanisms:
Key recommendations Determination of reimbursement rate is a crucial aspect with far-reaching implications. It has to critically balance multiple and possibly contrary objectives of patients’ safety, the economic sustainability of payers and the commercial interest of private sector players. This becomes all the more important in the Indian context, where we face the dual challenge of a huge demand for sponsored care and limited financial resources. We believe government-sponsored health insurance schemes contribute significantly to market expansion and therefore a sense of social solidarity and compassionate pricing is expected from private sector participants. However, the participation must be value-accretive and not loss-making for private sector interest to sustain.
Another important consideration in the Indian context is that, with a highly fragmented and diversely capable provider base, where regulatory oversight provides minimal assurance of quality, methods such as tender-based rate determination may disincentivize high-quality compliant providers and thereby defeat the purpose of the initiative. It is critical to differentially
recognize providers based on the quality of care offered, variances in cost structures across regions and additional inputs/ resources consumed in treating different levels of complexity within a particular type of a clinical case. A ‘one-size-fits-all’ approach to tariff determination, may not serve the purpose.
Based on our studies, we propose the following principles for defining the framework of reimbursement tariff determination for in-patient services:
1. Follow ‘case-based’ reimbursement model as is the current practice, making it more robust through standardization and refinement of case definitions
2. Employ ‘true’ cost as a basis for tariff and recognize cost structure differences on account of quality and geography
3. Centrally determine reference tariff rates based on a formula that recognizes relevant costs, quantum of government-sponsored patients served and clinical advancement
4. Additionally, reward performance to drive chosen objectives
5. Define provisions for adequate and timely revision of tariffs
Current state issues Impact
Predominant focus on short-term economics (such as L1 tendering method) for tariff determination
• Assurance to patients on safety and quality of care not adequate
• Providers interested in delivering quality may not be attracted to participate
• Long term increase in cost of care to the payer
Lack of national guidelines on package definition and re-imbursement tariff determination
• Varying rates for procedures across schemes based on disparate methods followed for tariff fixation(e.g. CABG rates vary by up to 100%, hysterectomy rates up to 150% across schemes )
• Complexities in governance and administration for scheme authorities as well as providers having to account separately for different schemes
Lack of differentiation in reimburse-ment tariffs with regard to –
• Providers selectively serve packages which are remunerative
• Incentives for proliferation of potentially ill-equipped hospitals
• Schemes overpay in certain locations and underpay in others
• Some providers especially in metros refusing treatment because of low tariff rates
• Disincentive to hospitals for treating severe/ complex cases
• Patients with complications may be turned away
• May not encourage attention towards improvements in quality and outcomes
• Quality of care across providers
• Regional variances in cost structures
• Severity of a condition
• Provider performance
4 Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
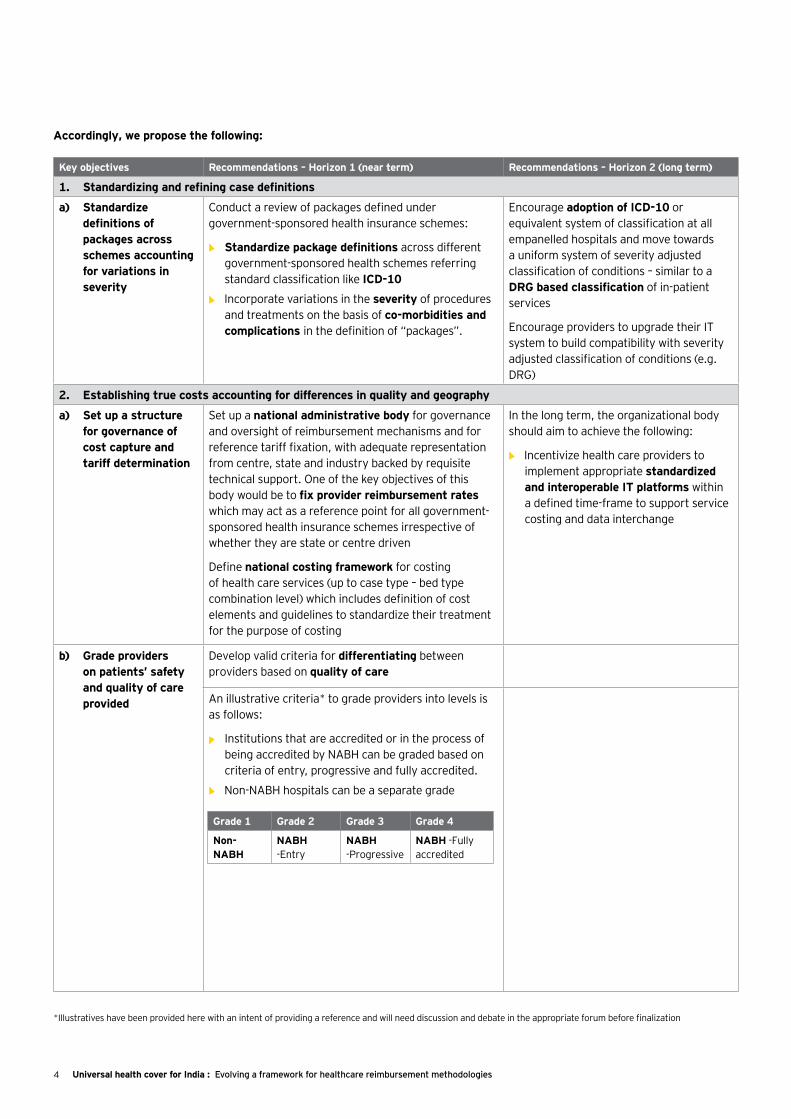
Accordingly, we propose the following:
Key objectives Recommendations – Horizon 1 (near term) Recommendations – Horizon 2 (long term)
1. Standardizing and refining case definitions
a) Standardize definitions of packages across schemes accounting for variations in severity
Conduct a review of packages defined under government-sponsored health insurance schemes:
• Standardize package definitions across different government-sponsored health schemes referring standard classification like ICD-10
• ►Incorporate variations in the severity of procedures and treatments on the basis of co-morbidities and complications in the definition of “packages”.
Encourage adoption of ICD-10 or equivalent system of classification at all empanelled hospitals and move towards a uniform system of severity adjusted classification of conditions – similar to a DRG based classification of in-patient services
Encourage providers to upgrade their IT system to build compatibility with severity adjusted classification of conditions (e.g. DRG)
2. Establishing true costs accounting for differences in quality and geography
a) Set up a structure for governance of cost capture and tariff determination
Set up a national administrative body for governance and oversight of reimbursement mechanisms and for reference tariff fixation, with adequate representation from centre, state and industry backed by requisite technical support. One of the key objectives of this body would be to fix provider reimbursement rates which may act as a reference point for all government-sponsored health insurance schemes irrespective of whether they are state or centre driven
Define national costing framework for costing of health care services (up to case type – bed type combination level) which includes definition of cost elements and guidelines to standardize their treatment for the purpose of costing
In the long term, the organizational body should aim to achieve the following:
• ►►Incentivize health care providers to implement appropriate standardized and interoperable IT platforms within a defined time-frame to support service costing and data interchange
b) Grade providers on patients’ safety and quality of care provided
Develop valid criteria for differentiating between providers based on quality of care
An illustrative criteria* to grade providers into levels is as follows:
• Institutions that are accredited or in the process of being accredited by NABH can be graded based on criteria of entry, progressive and fully accredited.
• ►Non-NABH hospitals can be a separate grade
Grade 1 Grade 2 Grade 3 Grade 4
Non-NABH
NABH -Entry
NABH -Progressive
NABH -Fully accredited
*Illustratives have been provided here with an intent of providing a reference and will need discussion and debate in the appropriate forum before finalization

5Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
Key objectives Recommendations – Horizon 1 (near term) Recommendations – Horizon 2 (long term)
c) Capture cost data for each grade of provider and regions
Determine cost of delivering health care services based on actual cost collected from a representative sample of providers:
• Collect procedure/treatment-wise detailed cost data from a sample of hospitals (refer to Annexure 1 for illustrative cost sheet template)
• Use a stratified sample to ensure adequate representation of different grades of providers in different regions. Ensure coverage of at least 10% of empanelled providers in each grade
Under the aegis of the national administrative body for provider reimbursement:
• Drive implementation of costing systems in all empanelled hospitals
• Implement mechanism of data checks/audits to ensure authenticity of data collected from providers
d) Group regions based on homogeneity of cost structures
Group regions into categories based on the homogeneity of cost structures.
• Illustrative criteria for region groups* include:
• Metros, tier 1 cities and tier 2 cities
• Key cities forming separate groups
• Costs that vary in regions and need to be checked for homogeneity include staff cost, doctor payouts, land, building, power, fuel and taxes.
The national administrative body should formally intervene in cases where the cost structures in particular regions are inordinately high relative to other regions and evaluate reasons for the same. An adjustment factor could be used for such regions to bring down costs to a rational level with the clear directional input to providers in these regions to improve efficiencies
3. Determination of tariff rates based on a formula that recognizes relevant costs, quantum of government sponsored patients served and clinical advancement
a) Determine base tariff rates based on weighted average of full costs
Fix payment rates for each package across provider categories and region groups based on average of ‘full cost’^ data collected, weighted by volumes of patients served under government sponsored schemes
Define tariff structure across provider grades such that there are significant incentives for Non-NABH and early-NABH providers to improve patient safety and quality systems and seek higher levels of accreditation.
Under the oversight of the national administrative body for provider reimbursement
• Deploy information management and IT systems to assist in converting costs to reimbursement tariffs
Region group*
Provider grades*
Non-NABH
NABH - early
NABH - progressive
NABH – full
Metro O O O O
Tier 1 O O O O
Tier 2 O O O O
...
O – Weighted average of full costs from data collected = Base payment rates for each provider-region group
*Illustratives have been provided here with an intent of providing a reference and will need discussion and debate in the appropriate forum before finalization
^’Full cost’ or ‘Absorption cost’ method expenses all costs associated with delivering a healthcare service including direct, indirect and overhead costs
6 Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
Key objectives Recommendations – Horizon 1 (near term) Recommendations – Horizon 2 (long term)
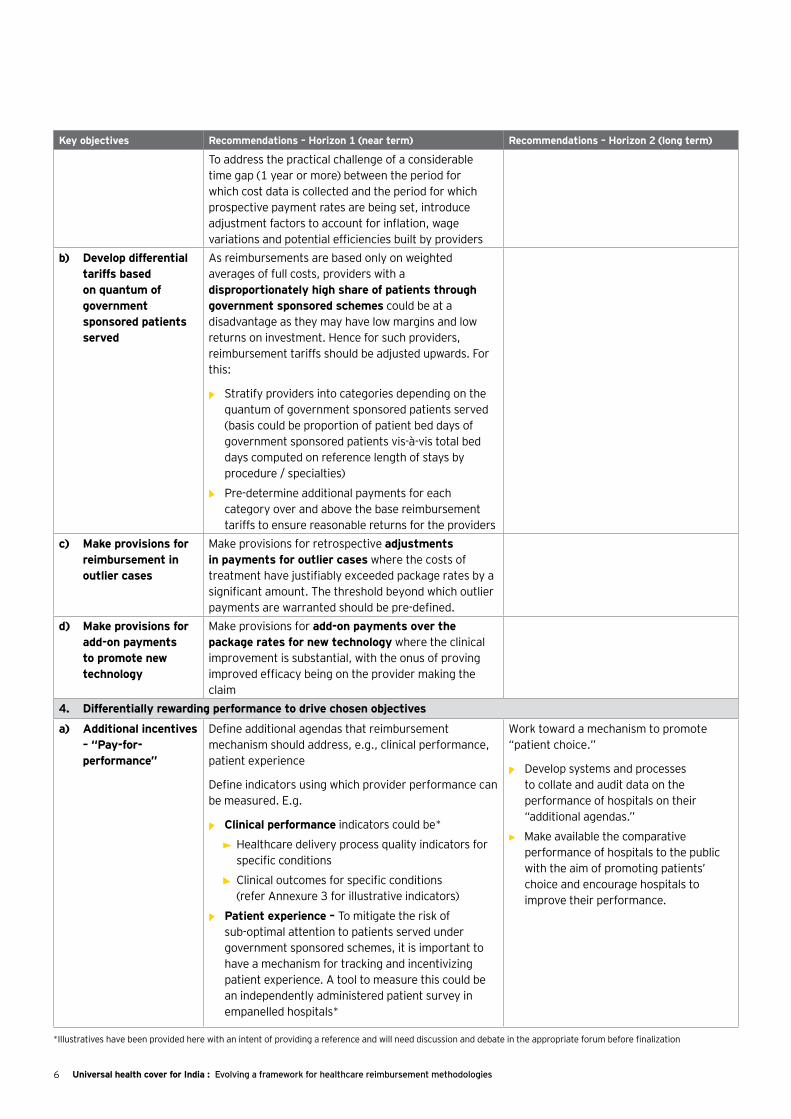
To address the practical challenge of a considerable time gap (1 year or more) between the period for which cost data is collected and the period for which prospective payment rates are being set, introduce adjustment factors to account for inflation, wage variations and potential efficiencies built by providers
b) Develop differential tariffs based on quantum of government sponsored patients served
As reimbursements are based only on weighted averages of full costs, providers with a disproportionately high share of patients through government sponsored schemes could be at a disadvantage as they may have low margins and low returns on investment. Hence for such providers, reimbursement tariffs should be adjusted upwards. For this:
• Stratify providers into categories depending on the quantum of government sponsored patients served (basis could be proportion of patient bed days of government sponsored patients vis-à-vis total bed days computed on reference length of stays by procedure / specialties)
• Pre-determine additional payments for each category over and above the base reimbursement tariffs to ensure reasonable returns for the providers
c) Make provisions for reimbursement in outlier cases
Make provisions for retrospective adjustments in payments for outlier cases where the costs of treatment have justifiably exceeded package rates by a significant amount. The threshold beyond which outlier payments are warranted should be pre-defined.
d) Make provisions for add-on payments to promote new technology
Make provisions for add-on payments over the package rates for new technology where the clinical improvement is substantial, with the onus of proving improved efficacy being on the provider making the claim
4. Differentially rewarding performance to drive chosen objectives
a) Additional incentives – “Pay-for-performance”
Define additional agendas that reimbursement mechanism should address, e.g., clinical performance, patient experience
Define indicators using which provider performance can be measured. E.g.
• Clinical performance indicators could be*
• Healthcare delivery process quality indicators for specific conditions
• Clinical outcomes for specific conditions (refer Annexure 3 for illustrative indicators)
• Patient experience – To mitigate the risk of sub-optimal attention to patients served under government sponsored schemes, it is important to have a mechanism for tracking and incentivizing patient experience. A tool to measure this could be an independently administered patient survey in empanelled hospitals*
Work toward a mechanism to promote “patient choice.”
• Develop systems and processes to collate and audit data on the performance of hospitals on their “additional agendas.”
• ►Make available the comparative performance of hospitals to the public with the aim of promoting patients’ choice and encourage hospitals to improve their performance.
*Illustratives have been provided here with an intent of providing a reference and will need discussion and debate in the appropriate forum before finalization
7Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
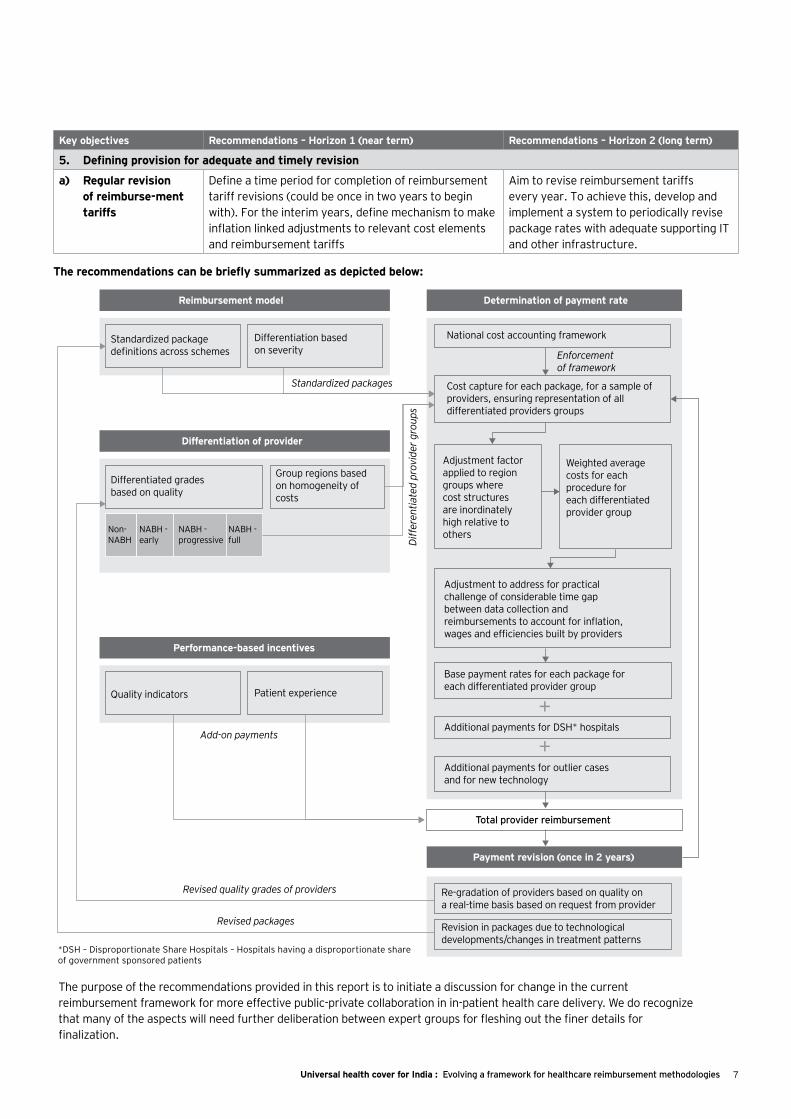
The recommendations can be briefly summarized as depicted below:
Key objectives Recommendations – Horizon 1 (near term) Recommendations – Horizon 2 (long term)
5. Defining provision for adequate and timely revision
a) Regular revision of reimburse-ment tariffs
Define a time period for completion of reimbursement tariff revisions (could be once in two years to begin with). For the interim years, define mechanism to make inflation linked adjustments to relevant cost elements and reimbursement tariffs
Aim to revise reimbursement tariffs every year. To achieve this, develop and implement a system to periodically revise package rates with adequate supporting IT and other infrastructure.
Reimbursement model Determination of payment rate
Payment revision (once in 2 years)
Total provider reimbursement
Additional payments for outlier cases and for new technology
Additional payments for DSH* hospitals
Base payment rates for each package for each differentiated provider group
Adjustment to address for practical challenge of considerable time gap between data collection and reimbursements to account for inflation, wages and efficiencies built by providers
Adjustment factor applied to region groups where cost structures are inordinately high relative to others
Weighted average costs for each procedure for each differentiated provider group
Re-gradation of providers based on quality on a real-time basis based on request from provider
National cost accounting framework
Standardized packages
Add-on payments
Revised quality grades of providers
Revised packages
Diffe
rent
iate
d pr
ovid
er g
roup
s
Enforcement of framework
Cost capture for each package, for a sample of providers, ensuring representation of all differentiated providers groups
Standardized package definitions across schemes
Differentiation based on severity
Performance-based incentives
Quality indicators Patient experience
Differentiation of provider
Differentiated grades based on quality
Non-NABH
NABH - early
NABH - full
NABH - progressive
Group regions based on homogeneity of costs
Revision in packages due to technological developments/changes in treatment patterns
+
+
*DSH – Disproportionate Share Hospitals – Hospitals having a disproportionate share of government sponsored patients
The purpose of the recommendations provided in this report is to initiate a discussion for change in the current reimbursement framework for more effective public-private collaboration in in-patient health care delivery. We do recognize that many of the aspects will need further deliberation between expert groups for fleshing out the finer details for finalization.

8 Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
9Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
Chapter 1
Chapter 2
Chapter 3
Context and need for a rationalized reimbursement tariff framework .................................................... 10
Prevalent models of provider reimbursement ...................................................................................... 16
Recommendations ............................................................................................................................. 34
List of abbreviations .................................................................................................................... 46
Annexures ....................................................................................................................................... 42

10 Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
Context and need for a rationalized reimbursement tariff framework
1

11Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
In their report, Universal health cover for India — demystifying financing needs, EY and FICCI deliberated on the case for Universal Health Coverage (UHC) in India and attempted to demystify aspects related to financing of UHC in India. The report also provided a conceptual framework for financing UHC in the country.
As a quick recap, UHC is an evolved form of health franchise, where the government guarantees equitable access to key promotive, preventive, curative and rehabilitative health interventions at affordable costs for all its citizens. In 2005, the World Health Assembly urged its member states to work toward UHC after considering the particular macroeconomic, socio-cultural and political context of each country.
In India, expenditure on health care has often been cited as one of the top three reasons for India’s population sinking into poverty with a vast number of its citizens either struggling to or failing to access high-quality care. Studies have shown that utilization of health care services depends on affordability with the number of people reporting the use of in-patient care increasing by 2 times (urban) and 3.5 times (rural) between the bottom-most decile and the highest decile of MPCE classes3. Furthermore, the cost of treatment largely continues to be unaffordable, and consequently, a significant part of the country’s population remains untreated. Apart from financial hardships, expenditure on health care also causes emotional as well as physical suffering for many more people, who are unable to spend adequately to procure the extent of care required for themselves or for people for whom they care. While health care should not be considered a privilege available only to those who can afford it rather than it being the basic right of all citizens, it has been treated more like an economic good rather than
a social or public obligation. For any developed society, it is a moral imperative to work toward reducing these hardships.
Given the scale of implementation and infrastructure constraints in the sector, it was suggested in last year’s report that a 10-year timeframe should be considered to accomplish implementation of UHC in totality in India. It was estimated that the Government’s expenditure on health would need to increase to ~4.5% of the country’s GDP in 2022 for complete implementation of the UHC program, which covers out-patient (consultation fees, drugs and diagnostic tests) and in-patient (ailments covered under RSBY and Aarogyasri) services for India’s entire population, assuming that hospitalization rates increase to match the hospitalization rate of the top MPCE urban classes (that have potential access to and the ability to afford most of their health care needs). It was estimated that including OoP expenditure, total spending on health should be between 5.5% and 6% of the country’s GDP.
There are five critical success factors for the implementation of an effective and sustainable UHC program. These include:
1. Acute focus on health outcomes: This is required, not only to limit wasteful expenditure but also to ensure that the focus is on health and not merely on sickness. The key levers of focus should include:
a) Reducing the disease burden through a robust and functioning primary care system including prevention and/or early detection of diseases and adequate out-patient care: In the Indian context, this is all the more crucial considering that primary health care is known to be inadequate and ineffective in large parts of the country.
3. “Universal health cover for India: Demystifying financing needs”, EY-FICCI report, Heal 2012.

12 Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
b) Quality of in-patient care: To keep UHC from becoming a farcical expenditure, it is imperative to monitor the quality of in-patient care as well as facilitate effective utilization of available infrastructure. This would necessitate putting in place a regulatory environment that assures high-quality delivery through the formulation of standard treatment guidelines, accreditation of hospitals, designing of basic health packages, auditing and monitoring of protocols and strengthening of diagnostic services at public health facilities.
c) Integrated approach: This will ensure an adequate focus on allied determinants that have a critical effect on health, mainly on nutrition, sanitation and wellness.
2. Making care accessible to patients: It is critical to ensure adequate generation and equitable distribution of supply of health services under a UHC program. The key levers of focus should include:
a) Filling the physical and human infrastructure gap: This can be achieved by a strong focus on correcting inequities in distribution.
b) Integration with other schools of medicine: The Government should promote pluralistic health care by integrating AYUSH’s vast health care delivery network (comprising 0.785mn registered practitioners, ~3,200 hospitals, ~25,000 dispensaries4).
c) Technology-enabled health care: The Government needs to leverage technology interventions to primarily address access constraints. Technology-enabled interventions such as provision of remote medical advice, health call centers, tele-radiology, emergency response and e-learning platforms can play a significant role in ensuring timely access to quality health care.
3. Ensuring a strong focus on the cost of care: To ensure that the financial burden of a UHC program is managed effectively, the UHC regime requires a strong culture of cost-consciousness. The key levers of focus should include:
a) Drug price policy and generic adoption: Given that drugs constitute nearly 70% of out-patient expenditure5, measures to control the prices of essential drugs and mandating adoption of generic
generics will become crucial for cost-effective health care delivery.
b) Indigenous medical technology: In view of the fact that nearly 75% of medical devices are imported6, it is imperative to promote indigenous medical technology in low-resource settings to drive down the cost of health care.
c) UHC reimbursement rates: The Government should formulate a rationalized policy to fix reimbursement of tariffs that define the different rates for stratified provider groups, based on objective technical and financial criteria. This is the only way of maintaining immaculate control of the UHC regime in terms of the cost of health care delivery. This should be coupled with optimal payment models that are oriented away from the “fee for service” mechanisms to reimbursement mechanisms that incentivize efficiency and outcomes (such as DRG-linked payments, and fixed and variable reimbursements with bonus payouts).
d) Administrative costs: Administrative costs in the US health care system are estimated at 14% of all health care expenditure7. While embarking on the UHC program, it would be important to first design a simple, standardized and efficient system and then implement it.
4. Enabling governance: An effective and efficient UHC regime requires optimal health system governance that ensures transparency, defines appropriate levels of checks and balances to secure integrity of delivery and provides granular epidemiological data for evidence-based decisions to be taken. The key levers of focus should include:
a) Role and accountability of Central and state governments: Given that health is a state subject and political will relating to health care may differ across states, the Central Government needs to play a dominant role in designing UHC in a manner that also recognizes state-specific differences.
b) Use of technology for implementation of transparency and managerial effectiveness: Given the scale and complexity of its implementation, interoperability and effective use of the required technology will be critical to ensure efficient
4. AYUSH website, accessed 1 August 2012.
5. “Household consumption of various goods and services in India”, NSS 66th round, NSSO, 2010.
6. “Medical Devices market in India”, Netscribes research report, 2010.
7. “The Health care imperative: Lowering costs and improving outcome”, Workshop series summary, Institute of Medicine, 2009.

13Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
transaction processing, monitoring compliance with treatment protocols, supervising contractual compliance, collecting basic health and epidemiological data, and ensuring clinical governance.
5. Building Centers of Excellence (CoEs): Adoption of UHC as a policy imperative will entail providing access and affordability to all Indian citizens in the short and medium term. Advancement of care will also be an equally important imperative to achieve implementation of UHC in the true spirit. It will necessitate seeding investments to build CoEs for medical needs that are relevant for Indian epidemiology and in designated geographic zones that are accessible to all for provision of the most complex care.
Need to take another look at reimbursement mechanismsReimbursement mechanisms in India warrant a relook for the following reasons:
• Increasing role of government as a purchaser and payer of health care services: The role of the Government is seen to be significantly shifting from a provider of health care services to a payer and purchaser of such services for citizens. Between 2004 and 2010, the number of people covered by different government-sponsored health insurance schemes has increased from 37 million to 243 million and is expected to cross 500 million people by 20158. This implies that by 2015, the Government’s purchase of health care services could be in the range of INR380 billion to INR400 billion per annum8, a significant amount that needs to be judiciously spent.
To fill the gap in physical health care infrastructure, an estimated investment ranging between INR1265 billion to INR2493 billion would be required over the next 10 years, which the Government will not be in a position to spend on its own and will have to buy health care services from private health care providers.
In addition, people also have a strong preference to avail of treatment in private health care facilities. Out of the 1.4 million hospital beds in the country, an estimated 45% are in the private sector, and ~65% of patients opt for private providers for in-patient treatment. Therefore,
going forward, purchase of health care services by the Government from private health care entities is expected to become a critical focus area.
• Collective dissatisfaction across stakeholder groups: There is general dissatisfaction across the stakeholder groups due to the way reimbursement tariffs are currently determined. Different schemes have followed varying methodologies to determine reimbursement tariffs, be they CGHS or government- sponsored health insurance schemes such as Rajiv Gandhi Aarogyasri or Rashtriya Swasthya Bima Yojna. However, unlike NLEM pricing of drugs, these methodologies have not been transparently documented and are not available in the public domain. Lack of clarity has prompted certain private health care providers to get themselves dis-empanelled, which has denied many potential beneficiaries access to health care services.
• Absence of uniform framework for determining reimbursement tariffs: The tariff-determination process is complex, since there are multiple purchasers (health being a state subject) of health care services and many providers with different capabilities as well as variations in costs structures by regions. Same providers may deliver services to patients under different schemes at different prices. Therefore, it is imperative to harmonize different schemes and develop a national tariff-determination framework that holistically focuses on economics, patients’ safety and their choice.
Challenges that will need to be addressedRedefining the reimbursement mechanism will require many challenges to be addressed. The key ones among them will be to:
• Define agendas for the reimbursement mechanism to address: Largely, government-sponsored health schemes have concentrated on the cost of purchase of health care services as a single agenda. While many additional aspects such as the quality of care are expected, these have not been built into current reimbursement mechanisms. Reimbursement can be a powerful tool to drive agendas the Government chooses, which could be to:
• Encourage the evolution of health care entities through provider differentiation based on enhanced quality of care, outcomes and patient experience
8. “Government Sponsored Health Insurance in India”, Gerard La Forgia and Somil Nagpal, World Bank, 2012.
14 Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
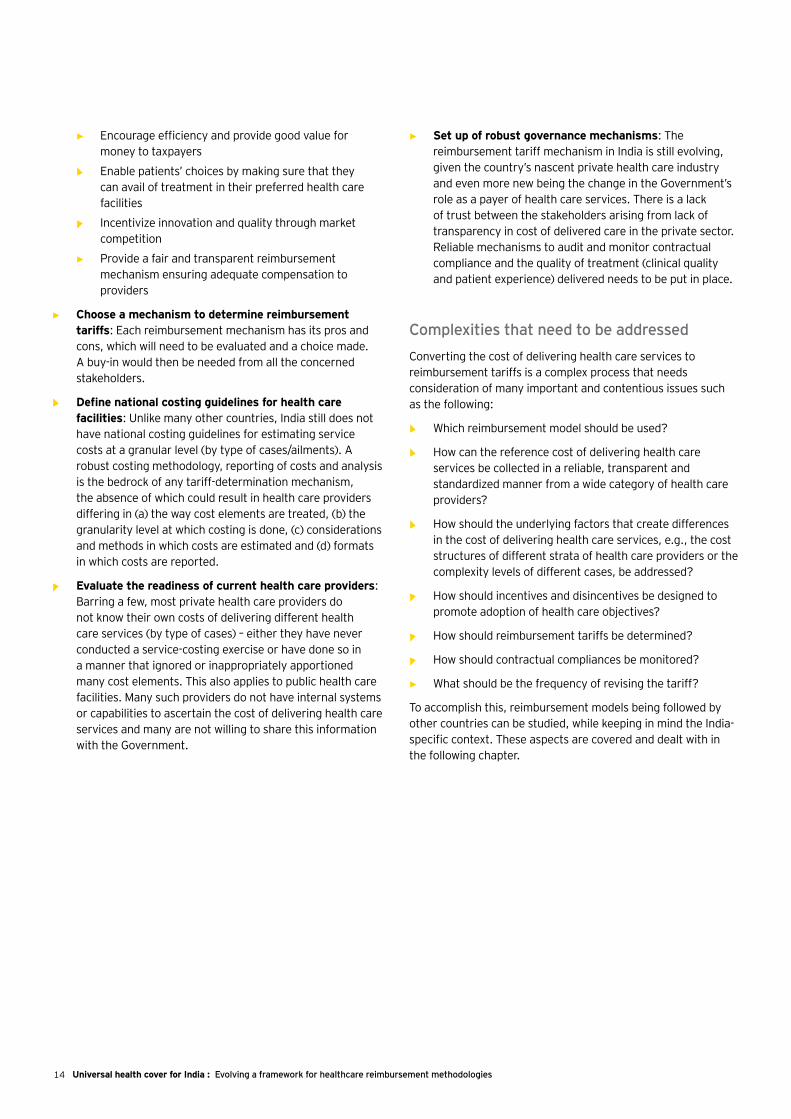
• Encourage efficiency and provide good value for money to taxpayers
• Enable patients’ choices by making sure that they can avail of treatment in their preferred health care facilities
• Incentivize innovation and quality through market competition
• Provide a fair and transparent reimbursement mechanism ensuring adequate compensation to providers
• Choose a mechanism to determine reimbursement tariffs: Each reimbursement mechanism has its pros and cons, which will need to be evaluated and a choice made. A buy-in would then be needed from all the concerned stakeholders.
• Define national costing guidelines for health care facilities: Unlike many other countries, India still does not have national costing guidelines for estimating service costs at a granular level (by type of cases/ailments). A robust costing methodology, reporting of costs and analysis is the bedrock of any tariff-determination mechanism, the absence of which could result in health care providers differing in (a) the way cost elements are treated, (b) the granularity level at which costing is done, (c) considerations and methods in which costs are estimated and (d) formats in which costs are reported.
• Evaluate the readiness of current health care providers: Barring a few, most private health care providers do not know their own costs of delivering different health care services (by type of cases) – either they have never conducted a service-costing exercise or have done so in a manner that ignored or inappropriately apportioned many cost elements. This also applies to public health care facilities. Many such providers do not have internal systems or capabilities to ascertain the cost of delivering health care services and many are not willing to share this information with the Government.
• Set up of robust governance mechanisms: The reimbursement tariff mechanism in India is still evolving, given the country’s nascent private health care industry and even more new being the change in the Government’s role as a payer of health care services. There is a lack of trust between the stakeholders arising from lack of transparency in cost of delivered care in the private sector. Reliable mechanisms to audit and monitor contractual compliance and the quality of treatment (clinical quality and patient experience) delivered needs to be put in place.
Complexities that need to be addressedConverting the cost of delivering health care services to reimbursement tariffs is a complex process that needs consideration of many important and contentious issues such as the following:
• Which reimbursement model should be used?
• How can the reference cost of delivering health care services be collected in a reliable, transparent and standardized manner from a wide category of health care providers?
• How should the underlying factors that create differences in the cost of delivering health care services, e.g., the cost structures of different strata of health care providers or the complexity levels of different cases, be addressed?
• How should incentives and disincentives be designed to promote adoption of health care objectives?
• How should reimbursement tariffs be determined?
• How should contractual compliances be monitored?
• What should be the frequency of revising the tariff?
To accomplish this, reimbursement models being followed by other countries can be studied, while keeping in mind the India-specific context. These aspects are covered and dealt with in the following chapter.

15Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
16 Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
Prevalent models of provider reimbursement mechanisms2

17Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
Across countries, frameworks for determination of reimbursement tariffs have been constantly evolving in response to changing contexts, revised priorities and experiences gained over years.
In this chapter, we have compared the key aspects of reimbursement methodologies being followed by different countries with models being followed in India. Accordingly, we have drawn certain learning that India can use to refine its future provider reimbursement framework.
18 Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
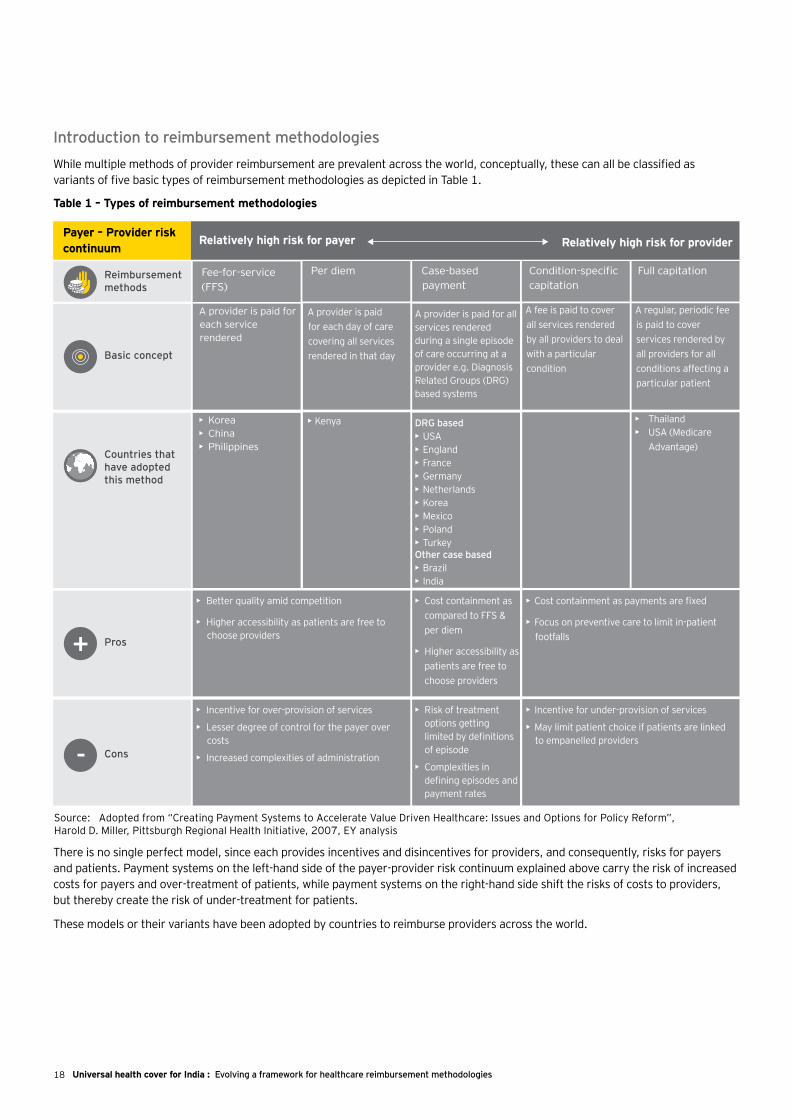
Introduction to reimbursement methodologiesWhile multiple methods of provider reimbursement are prevalent across the world, conceptually, these can all be classified as variants of five basic types of reimbursement methodologies as depicted in Table 1.
There is no single perfect model, since each provides incentives and disincentives for providers, and consequently, risks for payers and patients. Payment systems on the left-hand side of the payer-provider risk continuum explained above carry the risk of increased costs for payers and over-treatment of patients, while payment systems on the right-hand side shift the risks of costs to providers, but thereby create the risk of under-treatment for patients.
These models or their variants have been adopted by countries to reimburse providers across the world.
Payer – Provider risk continuum
Relatively high risk for payer
Reimbursement methods
Basic concept
Per diem Case-based payment
Condition-specific capitation
Full capitation
A provider is paid for each service rendered
A provider is paid for each day of care covering all services rendered in that day
A provider is paid for all services rendered during a single episode of care occurring at a provider �e.g. Diagnosis Related Groups (DRG) based systems
A fee is paid to cover all services rendered by all providers to deal with a particular condition
A regular, periodic fee is paid to cover services rendered by all providers for all conditions affecting a particular patient
Relatively high risk for provider
Pros
• Better quality amid competition
• Higher accessibility as patients are free to choose providers
• Cost containment as compared to FFS & per diem
• Higher accessibility as patients are free to choose providers
• Cost containment as payments are fixed
• Focus on preventive care to limit in-patient footfalls+
Cons
• Incentive for over-provision of services
• Lesser degree of control for the payer over costs
• Increased complexities of administration
• Risk of treatment options getting limited by definitions of episode
• Complexities in defining episodes and payment rates
• Incentive for under-provision of services
• May limit patient choice if patients are linked to empanelled providers
-
Countries that have adopted this method
• Korea• China• Philippines
• Kenya DRG based • USA• England• France• Germany• Netherlands• Korea• Mexico• Poland• TurkeyOther case based• Brazil• India
• Thailand• USA (Medicare
Advantage)
Fee-for-service (FFS)
Source: Adopted from “Creating Payment Systems to Accelerate Value Driven Healthcare: Issues and Options for Policy Reform”, Harold D. Miller, Pittsburgh Regional Health Initiative, 2007, EY analysis
Table 1 – Types of reimbursement methodologies
19Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
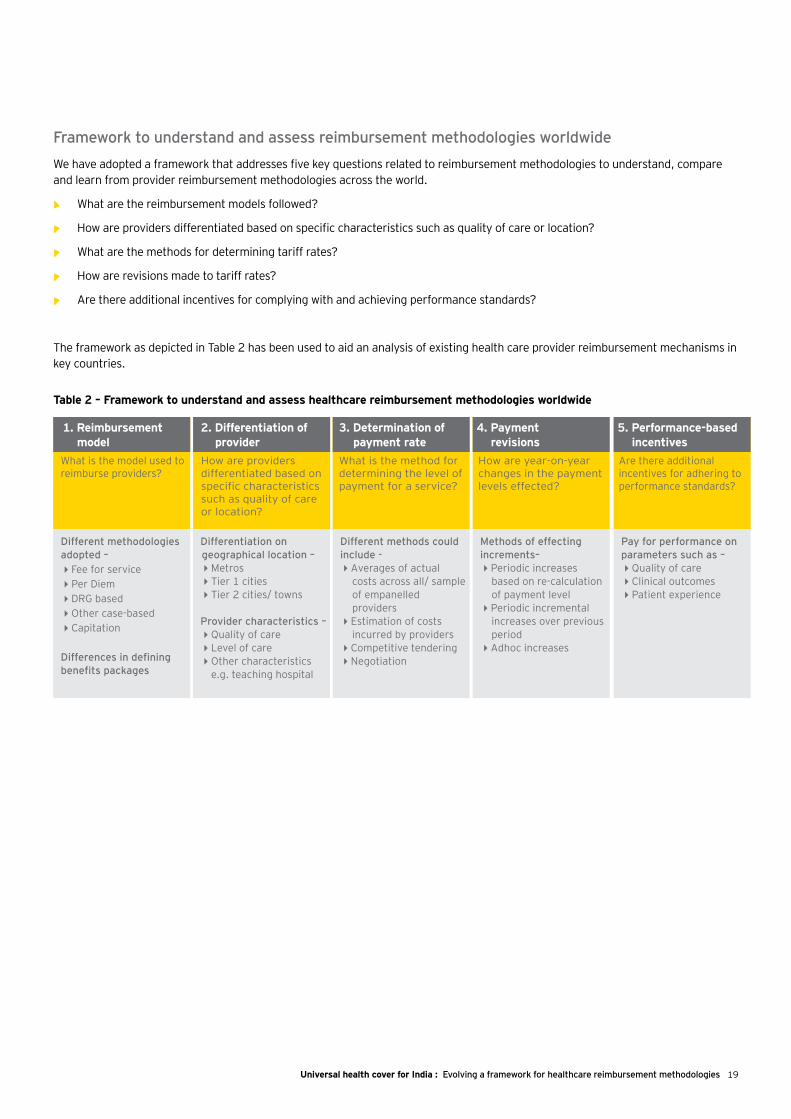
What is the model used to reimburse providers?
1. Reimbursementmodel
How are providers differentiated based on specific characteristics such as quality of care or location?
2. Differentiation ofprovider
What is the method for determining the level of payment for a service?
3. Determination of payment rate
How are year-on-year changes in the payment levels effected?
4. Payment revisions
Are there additional incentives for adhering to performance standards?
5. Performance-based incentives
Different methodologies adopted – Fee for servicePer DiemDRG basedOther case-basedCapitation
Differences in defining benefits packages
Differentiation on geographical location –MetrosTier 1 citiesTier 2 cities/ towns
Provider characteristics –Quality of careLevel of careOther characteristics
e.g. teaching hospital
Different methods could include - Averages of actual
costs across all/ sample of empanelled providers
Estimation of costs incurred by providers
Competitive tenderingNegotiation
Methods of effecting increments–Periodic increases
based on re-calculation of payment level
Periodic incremental increases over previous period
Adhoc increases
Pay for performance on parameters such as – Quality of careClinical outcomesPatient experience
Framework to understand and assess reimbursement methodologies worldwideWe have adopted a framework that addresses five key questions related to reimbursement methodologies to understand, compare and learn from provider reimbursement methodologies across the world.
• What are the reimbursement models followed?
• How are providers differentiated based on specific characteristics such as quality of care or location?
• What are the methods for determining tariff rates?
• How are revisions made to tariff rates?
• Are there additional incentives for complying with and achieving performance standards?
The framework as depicted in Table 2 has been used to aid an analysis of existing health care provider reimbursement mechanisms in key countries.
Table 2 – Framework to understand and assess healthcare reimbursement methodologies worldwide
20 Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
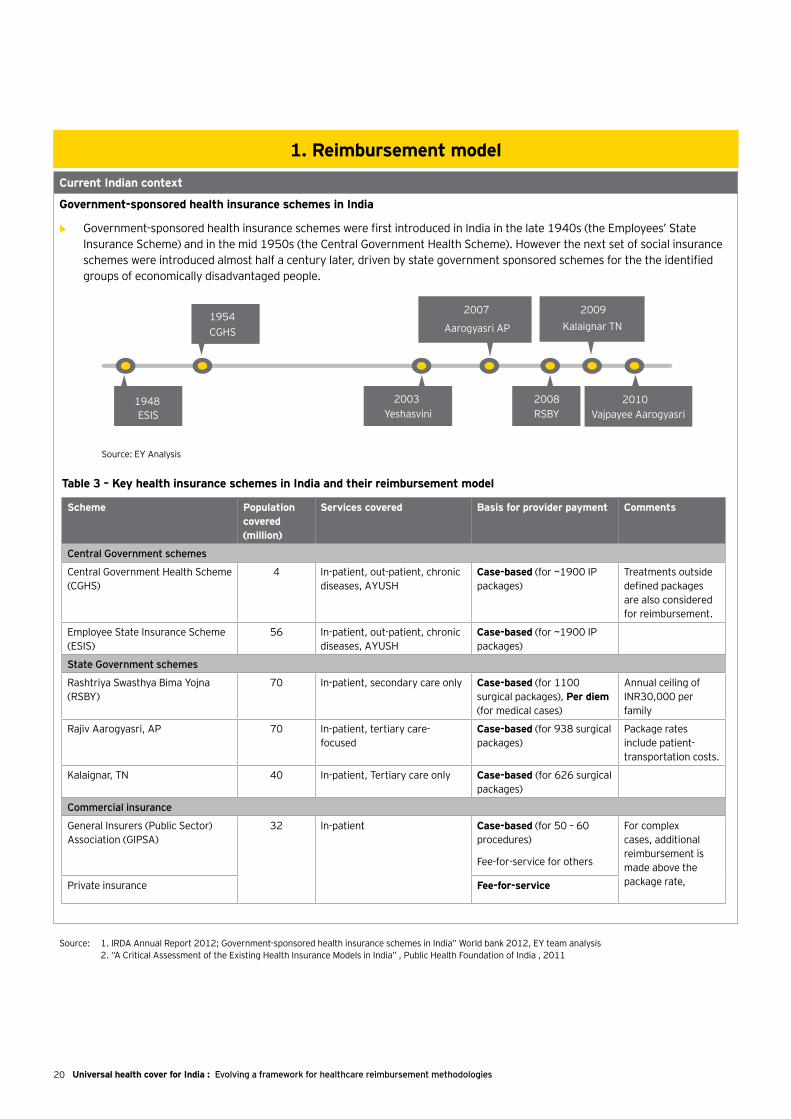
Current Indian context
Government-sponsored health insurance schemes in India
• Government-sponsored health insurance schemes were first introduced in India in the late 1940s (the Employees’ State Insurance Scheme) and in the mid 1950s (the Central Government Health Scheme). However the next set of social insurance schemes were introduced almost half a century later, driven by state government sponsored schemes for the the identified groups of economically disadvantaged people.
1. Reimbursement model
-
-
-2008 RSBY
1948 ESIS
1954 CGHS
2003 Yeshasvini
Aarogyasri AP
2007 2009 Kalaignar TN
2010 Vajpayee Aarogyasri
Source: EY Analysis
Scheme Population covered (million)
Services covered Basis for provider payment Comments
Central Government schemes
Central Government Health Scheme (CGHS)
4 In-patient, out-patient, chronic diseases, AYUSH
Case-based (for ~1900 IP packages)
Treatments outside defined packages are also considered for reimbursement.
Employee State Insurance Scheme (ESIS)
56 In-patient, out-patient, chronic diseases, AYUSH
Case-based (for ~1900 IP packages)
State Government schemes
Rashtriya Swasthya Bima Yojna (RSBY)
70 In-patient, secondary care only Case-based (for 1100 surgical packages), Per diem (for medical cases)
Annual ceiling of INR30,000 per family
Rajiv Aarogyasri, AP 70 In-patient, tertiary care- focused
Case-based (for 938 surgical packages)
Package rates include patient-transportation costs.
Kalaignar, TN 40 In-patient, Tertiary care only Case-based (for 626 surgical packages)
Commercial insurance
General Insurers (Public Sector) Association (GIPSA)
32 In-patient Case-based (for 50 – 60 procedures)
Fee-for-service for others
For complex cases, additional reimbursement is made above the package rate,Private insurance Fee-for-service
Table 3 – Key health insurance schemes in India and their reimbursement model
Source: 1. IRDA Annual Report 2012; Government-sponsored health insurance schemes in India” World bank 2012, EY team analysis 2. “A Critical Assessment of the Existing Health Insurance Models in India” , Public Health Foundation of India , 2011
21Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
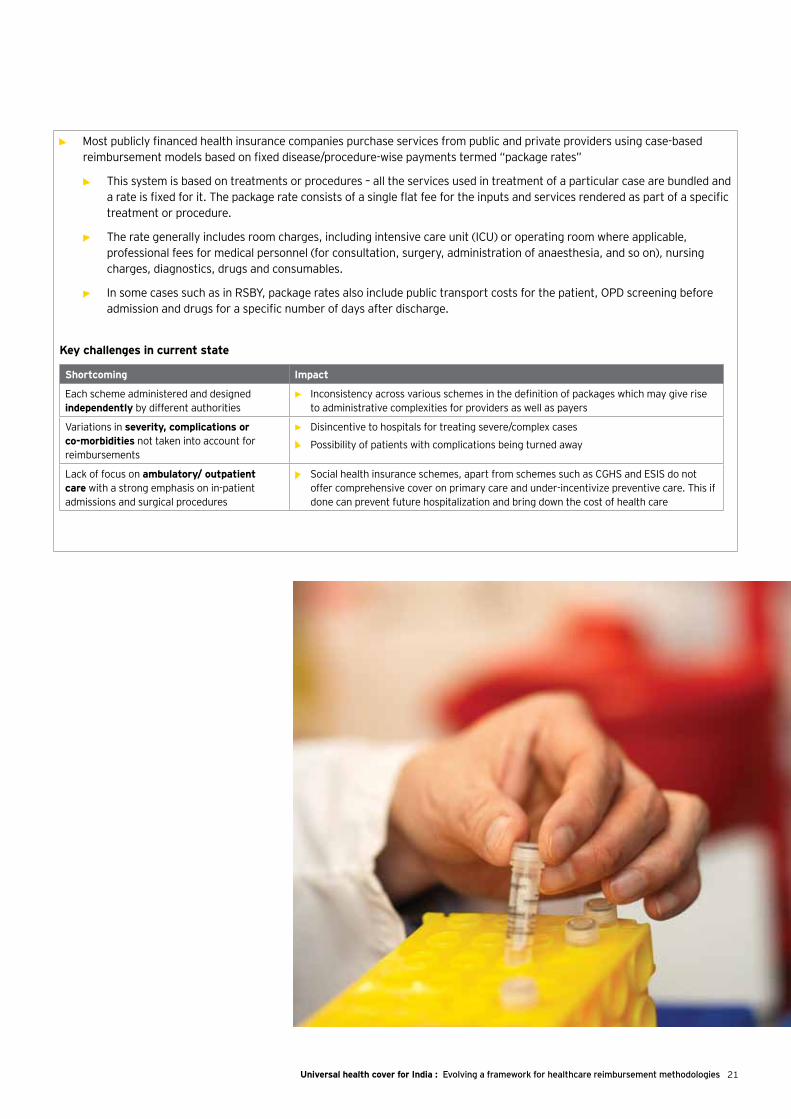
• ►Most publicly financed health insurance companies purchase services from public and private providers using case-based reimbursement models based on fixed disease/procedure-wise payments termed “package rates”
• This system is based on treatments or procedures – all the services used in treatment of a particular case are bundled and a rate is fixed for it. The package rate consists of a single flat fee for the inputs and services rendered as part of a specific treatment or procedure.
• The rate generally includes room charges, including intensive care unit (ICU) or operating room where applicable, professional fees for medical personnel (for consultation, surgery, administration of anaesthesia, and so on), nursing charges, diagnostics, drugs and consumables.
• In some cases such as in RSBY, package rates also include public transport costs for the patient, OPD screening before admission and drugs for a specific number of days after discharge.
Shortcoming Impact
Each scheme administered and designed independently by different authorities
• Inconsistency across various schemes in the definition of packages which may give rise to administrative complexities for providers as well as payers
Variations in severity, complications or co-morbidities not taken into account for reimbursements
• Disincentive to hospitals for treating severe/complex cases
• Possibility of patients with complications being turned away
Lack of focus on ambulatory/ outpatient care with a strong emphasis on in-patient admissions and surgical procedures
• Social health insurance schemes, apart from schemes such as CGHS and ESIS do not offer comprehensive cover on primary care and under-incentivize preventive care. This if done can prevent future hospitalization and bring down the cost of health care
Key challenges in current state

22 Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
9. ”DRG-based payment systems in low- and middle-income countries: Implementation experiences and challenges” ,Inke Mathaue and Friedrich Wittenecher,
WHO , Discussion Paper Number 1, 2012.
International experiences
1. Most countries are moving toward a DRG-based payment system, which is in principle a case-based model of reimbursement.
While the DRG based system was pioneered in USA, as depicted in Table 4 many countries including developing economies are adopting a DRG based payment system to reimburse providers.
Simply put, DRGs classify all human diseases according to the affected organ, diagnosis and other characteristics of patients, such as age, gender, complications, co-morbidities and procedures performed.
DRG-based payment systems comprise a patient case-classification system and a payment rate-setting mechanism that assigns cost weights to DRGs in relation to the intensity of resources used in treatment. Services that need to be offered to treat a patient in a particular DRG group are bundled and payment rates fixed for the bundle. DRGs are mainly applied to remuneration for acute in-patient care, but in principle, can also be used for non-acute in-patient care as well as out-patient case classification and payment9.
While the case-based system adopted in India also bundles services required for specific treatments/ procedures and fixes payment rates for these, DRGs are a more sophisticated and scientifically developed classification. The most commonly used classification is WHO’s International Statistical Classification of Diseases, 10th revision (ICD 10) for diagnosis9. Furthermore, a DRG- based system is in principle exhaustive and classifies all patient cases in its system, whereas a case-based system (adopted in India) focuses on a selected number of treatments/procedures.
► USA - Medicare (USA’s social health insurance for the aged) established in 1965 initially adopted a retrospective cost-based fee-for-service reimbursement system and then moved to a prospective ‘Case-based’ system in 1980s which has evolved into the MS-DRG system used today with over 750 DRGs which are based on patient’s diagnosis, clinical conditions and treatment strategies
► Europe – Most developed economies in Europe including England, France, Germany, Portugal, Spain, Sweden, Netherlands migrated from their traditional ‘fee-for-service’ systems or ‘global budget’ systems to DRG based systems between 1984 and 2005
► Developing economies in Asia – Thailand which relies on a capitation system of global budgets introduced reimbursements based on a DRG system for acute in-patient care since 2001. Indonesia initiated and implemented DRG based reimbursement in 2009-10
► Other developing economies – Developing economies such as Mexico, Turkey, Poland have all adopted DRG based systems in the period 1990 to 2010
Fee-for-service (FFS)
Illustrative
Per diem Case-based payment – using DRG or its variants
Full capitation – using global budgets
Reimbursementmethods
Sources : 1. ”DRG-based payment systems in low- and middle-income countries: Implementation experiences and challenges” ,Inke Mathaue and Friedrich Wittenecher , WHO , Discussion Paper Number 1, 2012.
2. “Diagnosis Related Groups in Europe : Moving towards transparency , efficiency and quality in Hospitals " , European Observatory on Health Systems and Policies Series , 2011.
3. “Medicare Hospital Prospective Payment System How DRG Rates Are Calculated and Updated” , Office of Inspector General ,Office of Evaluation and Inspections ,Region IX ,2001.
4. “Hospital Acute Inpatient Services Payment System” , Medpac , 2012.
Table 4 – Trends in reimbursement models
23Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
International experiences (cont’d.)
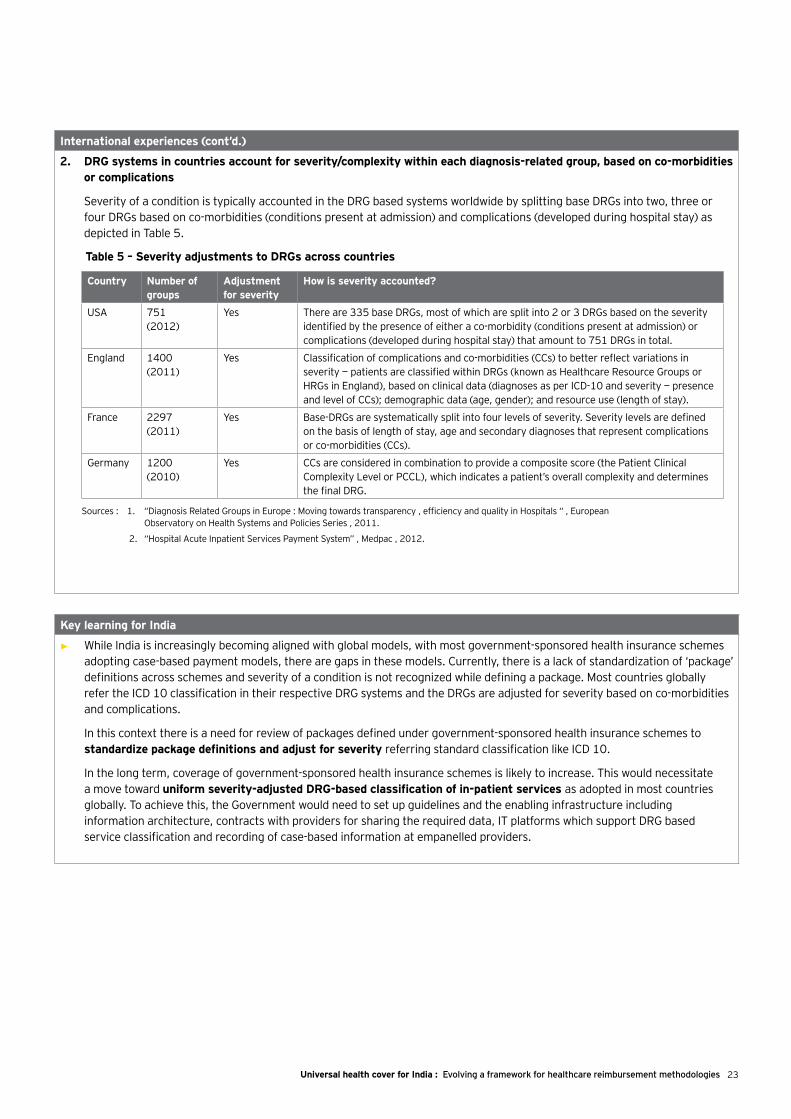
2. DRG systems in countries account for severity/complexity within each diagnosis-related group, based on co-morbidities or complications
Severity of a condition is typically accounted in the DRG based systems worldwide by splitting base DRGs into two, three or four DRGs based on co-morbidities (conditions present at admission) and complications (developed during hospital stay) as depicted in Table 5.
Country Number of groups
Adjustment for severity
How is severity accounted?
USA 751 (2012)
Yes There are 335 base DRGs, most of which are split into 2 or 3 DRGs based on the severity identified by the presence of either a co-morbidity (conditions present at admission) or complications (developed during hospital stay) that amount to 751 DRGs in total.
England 1400 (2011)
Yes Classification of complications and co-morbidities (CCs) to better reflect variations in severity — patients are classified within DRGs (known as Healthcare Resource Groups or HRGs in England), based on clinical data (diagnoses as per ICD-10 and severity — presence and level of CCs); demographic data (age, gender); and resource use (length of stay).
France 2297 (2011)
Yes Base-DRGs are systematically split into four levels of severity. Severity levels are defined on the basis of length of stay, age and secondary diagnoses that represent complications or co-morbidities (CCs).
Germany 1200 (2010)
Yes CCs are considered in combination to provide a composite score (the Patient Clinical Complexity Level or PCCL), which indicates a patient’s overall complexity and determines the final DRG.
Sources : 1. “Diagnosis Related Groups in Europe : Moving towards transparency , efficiency and quality in Hospitals “ , European Observatory on Health Systems and Policies Series , 2011.
2. “Hospital Acute Inpatient Services Payment System” , Medpac , 2012.
Table 5 – Severity adjustments to DRGs across countries
Key learning for India
• While India is increasingly becoming aligned with global models, with most government-sponsored health insurance schemes adopting case-based payment models, there are gaps in these models. Currently, there is a lack of standardization of ‘package’ definitions across schemes and severity of a condition is not recognized while defining a package. Most countries globally refer the ICD 10 classification in their respective DRG systems and the DRGs are adjusted for severity based on co-morbidities and complications.
In this context there is a need for review of packages defined under government-sponsored health insurance schemes to standardize package definitions and adjust for severity referring standard classification like ICD 10.
In the long term, coverage of government-sponsored health insurance schemes is likely to increase. This would necessitate a move toward uniform severity-adjusted DRG-based classification of in-patient services as adopted in most countries globally. To achieve this, the Government would need to set up guidelines and the enabling infrastructure including information architecture, contracts with providers for sharing the required data, IT platforms which support DRG based service classification and recording of case-based information at empanelled providers.
24 Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
Current Indian context
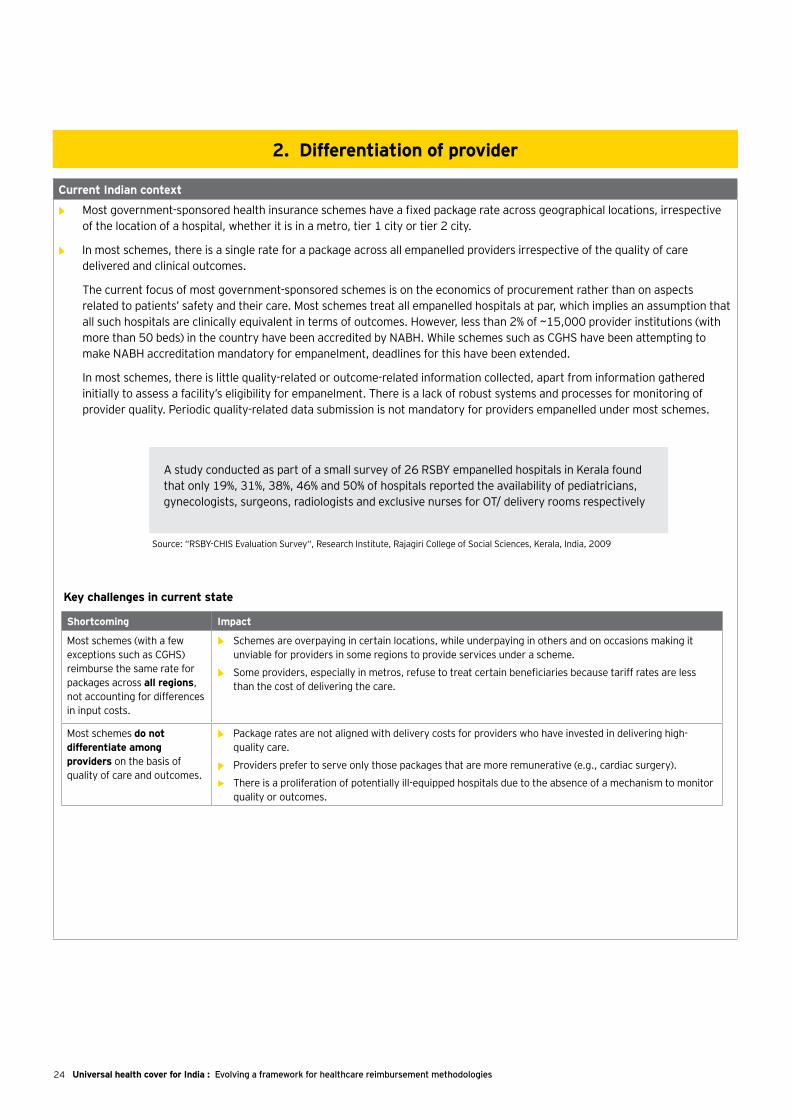
• Most government-sponsored health insurance schemes have a fixed package rate across geographical locations, irrespective of the location of a hospital, whether it is in a metro, tier 1 city or tier 2 city.
• ► In most schemes, there is a single rate for a package across all empanelled providers irrespective of the quality of care delivered and clinical outcomes.
The current focus of most government-sponsored schemes is on the economics of procurement rather than on aspects related to patients’ safety and their care. Most schemes treat all empanelled hospitals at par, which implies an assumption that all such hospitals are clinically equivalent in terms of outcomes. However, less than 2% of ~15,000 provider institutions (with more than 50 beds) in the country have been accredited by NABH. While schemes such as CGHS have been attempting to make NABH accreditation mandatory for empanelment, deadlines for this have been extended.
In most schemes, there is little quality-related or outcome-related information collected, apart from information gathered initially to assess a facility’s eligibility for empanelment. There is a lack of robust systems and processes for monitoring of provider quality. Periodic quality-related data submission is not mandatory for providers empanelled under most schemes.
2. Differentiation of provider
A study conducted as part of a small survey of 26 RSBY empanelled hospitals in Kerala found that only 19%, 31%, 38%, 46% and 50% of hospitals reported the availability of pediatricians, gynecologists, surgeons, radiologists and exclusive nurses for OT/ delivery rooms respectively
Source: “RSBY-CHIS Evaluation Survey“, Research Institute, Rajagiri College of Social Sciences, Kerala, India, 2009
Shortcoming Impact
Most schemes (with a few exceptions such as CGHS) reimburse the same rate for packages across all regions, not accounting for differences in input costs.
• Schemes are overpaying in certain locations, while underpaying in others and on occasions making it unviable for providers in some regions to provide services under a scheme.
• Some providers, especially in metros, refuse to treat certain beneficiaries because tariff rates are less than the cost of delivering the care.
Most schemes do not differentiate among providers on the basis of quality of care and outcomes.
• Package rates are not aligned with delivery costs for providers who have invested in delivering high-quality care.
• Providers prefer to serve only those packages that are more remunerative (e.g., cardiac surgery).
• There is a proliferation of potentially ill-equipped hospitals due to the absence of a mechanism to monitor quality or outcomes.
Key challenges in current state

25Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
International experiences
1. In most countries, regional variances in cost structures are accounted for by using a mechanism of regional weights.
Country Mechanism used to account for regional variances in cost structures
England Market Forces Factor (MFF)
• MFF is a top-up applied to England’s DRG-based payment tariff (PbR – Payment by Results) to reflect unavoidable cost variations driven by geographical/economic factors outside an organization’s control, e.g., high staff costs in cities such as London.
• The MFF index is based on four key input cost factors, as shown below:
USA Hospital wage index
• In Medicare’s DRG-based reimbursement system, a wage index is used to make adjustments to the labor charge part of the base payment amount to account for differences in wage rates in a region.
Labor charges adjusted based on wage rates
Local market factors adjustment
Hospital wage index
Non-labor charges
Adjusted base payment rate
Operating base payment rate per case
Staff index A%
B%
C%
D%
Sub-indices WeightsIllustrative
Doctor index
Buildings index
Land index
MFFindex
► Overall MFF is the weighted average of sub-indices
Weights are based on a national average split of costs
Sources : 1. EY knowledge base
2. “Hospital Acute Inpatient Services Payment System” , Medpac , 2012.
26 Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
International experiences (cont’d.)
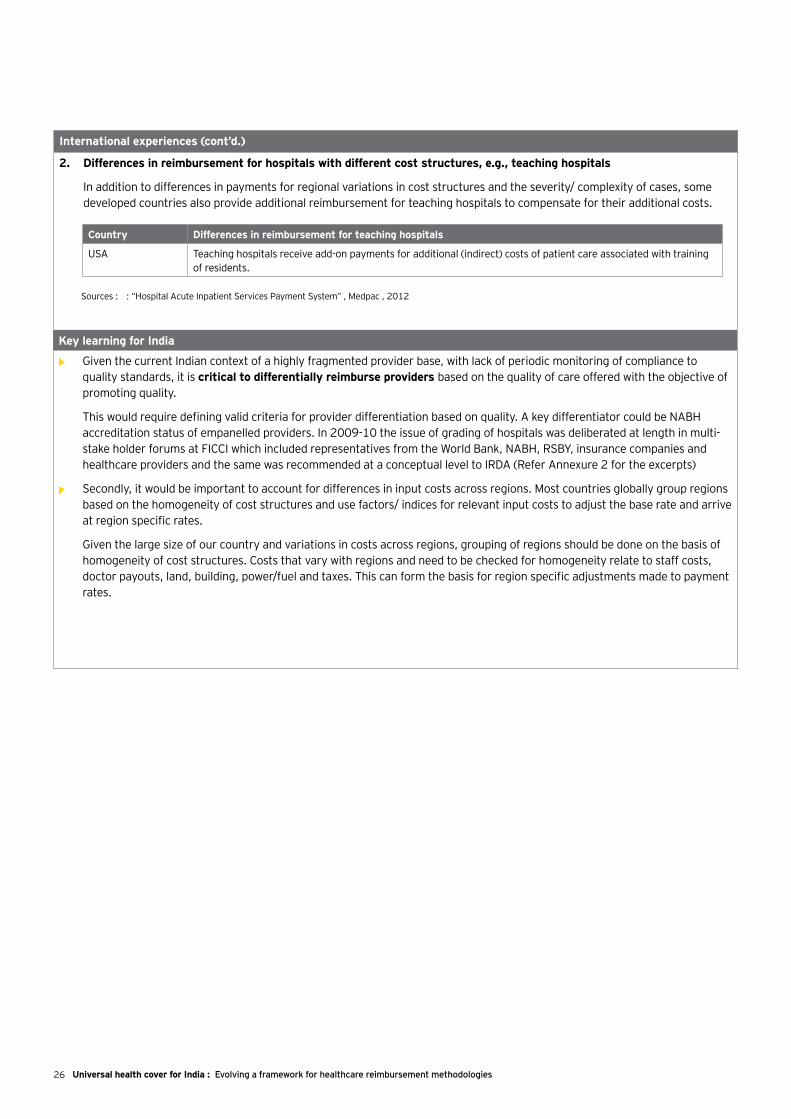
2. Differences in reimbursement for hospitals with different cost structures, e.g., teaching hospitals
In addition to differences in payments for regional variations in cost structures and the severity/ complexity of cases, some developed countries also provide additional reimbursement for teaching hospitals to compensate for their additional costs.
Key learning for India
• Given the current Indian context of a highly fragmented provider base, with lack of periodic monitoring of compliance to quality standards, it is critical to differentially reimburse providers based on the quality of care offered with the objective of promoting quality.
This would require defining valid criteria for provider differentiation based on quality. A key differentiator could be NABH accreditation status of empanelled providers. In 2009-10 the issue of grading of hospitals was deliberated at length in multi-stake holder forums at FICCI which included representatives from the World Bank, NABH, RSBY, insurance companies and healthcare providers and the same was recommended at a conceptual level to IRDA (Refer Annexure 2 for the excerpts)
• Secondly, it would be important to account for differences in input costs across regions. Most countries globally group regions based on the homogeneity of cost structures and use factors/ indices for relevant input costs to adjust the base rate and arrive at region specific rates.
Given the large size of our country and variations in costs across regions, grouping of regions should be done on the basis of homogeneity of cost structures. Costs that vary with regions and need to be checked for homogeneity relate to staff costs, doctor payouts, land, building, power/fuel and taxes. This can form the basis for region specific adjustments made to payment rates.
Country Differences in reimbursement for teaching hospitals
USA Teaching hospitals receive add-on payments for additional (indirect) costs of patient care associated with training of residents.
Sources : : “Hospital Acute Inpatient Services Payment System” , Medpac , 2012
27Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
Current Indian context
Fixing of tariffs by government-sponsored health insurance schemes in India is not aligned to costs incurred by providers.
• ►CGHS was the first to adopt the package rate system. Services that form part of a particular episode of care (treatment/procedure) are bundled as part of a package and the rate is agreed on and fixed for the package.
• Package rates were originally generated through a competitive tendering process according to which quotes were invited from empanelled hospitals on specified procedures and treatments.
• However, the methodology for arriving at final package rates has varied over the years. In 2001, package rates were based on a median of quoted rates. Subsequently, the scheme has moved to the lowest quotes received (L1).
• Many other health schemes, such as ESIS and the one used by the railways, refer to CGHS rates.
Key challenges in current state
3. Determination of payment rate
Shortcoming Impact
Package rates in many cases are not aligned to the cost of providing a service
Tariff determination is through economics focused methods such as L1 competitive tendering
• Providers who have invested in ensuring quality of care may be dis-incentivized.
• Providers selectively serve only those packages that are remunerative.
• In the absence of adequate controls, unscrupulous providers may resort to fraud by “upcoding.”
28 Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
International experiences
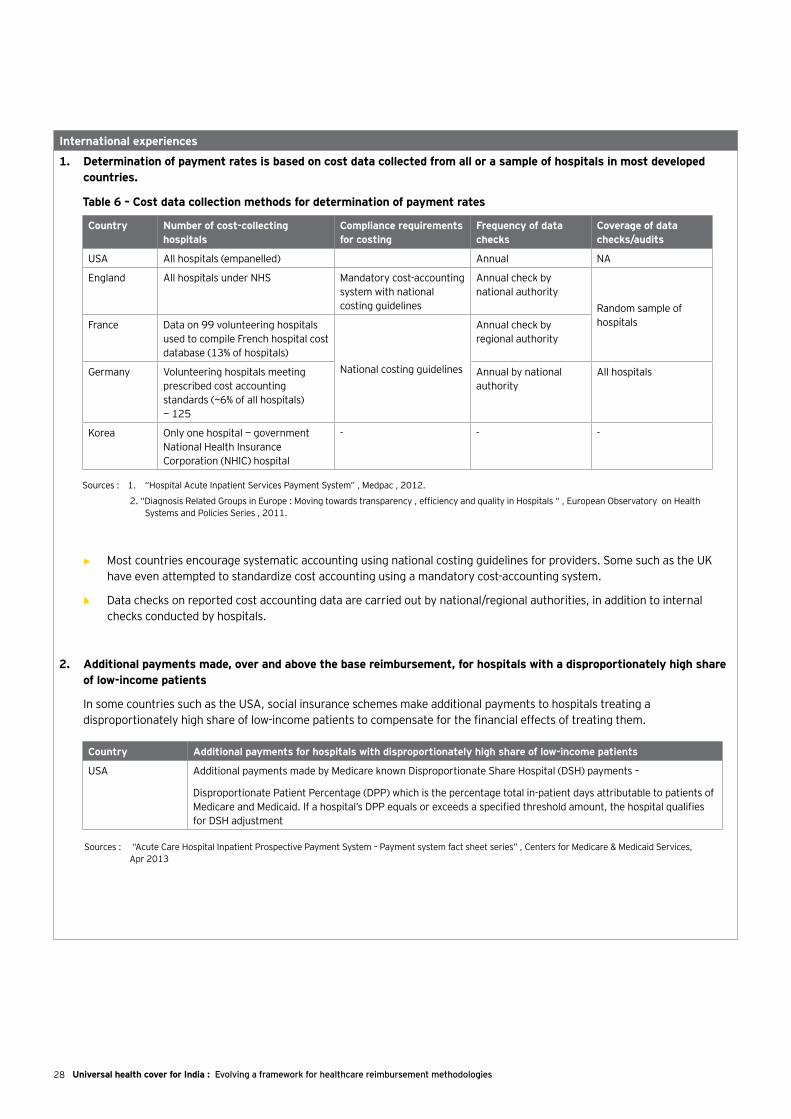
1. Determination of payment rates is based on cost data collected from all or a sample of hospitals in most developed countries.
• ► Most countries encourage systematic accounting using national costing guidelines for providers. Some such as the UK have even attempted to standardize cost accounting using a mandatory cost-accounting system.
• ► Data checks on reported cost accounting data are carried out by national/regional authorities, in addition to internal checks conducted by hospitals.
2. Additional payments made, over and above the base reimbursement, for hospitals with a disproportionately high share of low-income patients
In some countries such as the USA, social insurance schemes make additional payments to hospitals treating a disproportionately high share of low-income patients to compensate for the financial effects of treating them.
Country Number of cost-collecting hospitals
Compliance requirements for costing
Frequency of data checks
Coverage of data checks/audits
USA All hospitals (empanelled) Annual NA
England All hospitals under NHS Mandatory cost-accounting system with national costing guidelines
Annual check by national authority
Random sample of hospitalsFrance Data on 99 volunteering hospitals
used to compile French hospital cost database (13% of hospitals)
National costing guidelines
Annual check by regional authority
Germany Volunteering hospitals meeting prescribed cost accounting standards (~6% of all hospitals) — 125
Annual by national authority
All hospitals
Korea Only one hospital — government National Health Insurance Corporation (NHIC) hospital
- - -
Sources : 1. “Hospital Acute Inpatient Services Payment System” , Medpac , 2012.
2. “Diagnosis Related Groups in Europe : Moving towards transparency , efficiency and quality in Hospitals “ , European Observatory on Health Systems and Policies Series , 2011.
Table 6 – Cost data collection methods for determination of payment rates
Country Additional payments for hospitals with disproportionately high share of low-income patients
USA Additional payments made by Medicare known Disproportionate Share Hospital (DSH) payments –
Disproportionate Patient Percentage (DPP) which is the percentage total in-patient days attributable to patients of Medicare and Medicaid. If a hospital’s DPP equals or exceeds a specified threshold amount, the hospital qualifies for DSH adjustment
Sources : “Acute Care Hospital Inpatient Prospective Payment System – Payment system fact sheet series” , Centers for Medicare & Medicaid Services, Apr 2013
29Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
Sources : 1. “Hospital Acute Inpatient Services Payment System” , Medpac , 2012.
2. “Diagnosis Related Groups in Europe : Moving towards transparency , efficiency and quality in Hospitals “ , European Observatory on Health Systems and Policies Series , 2011.
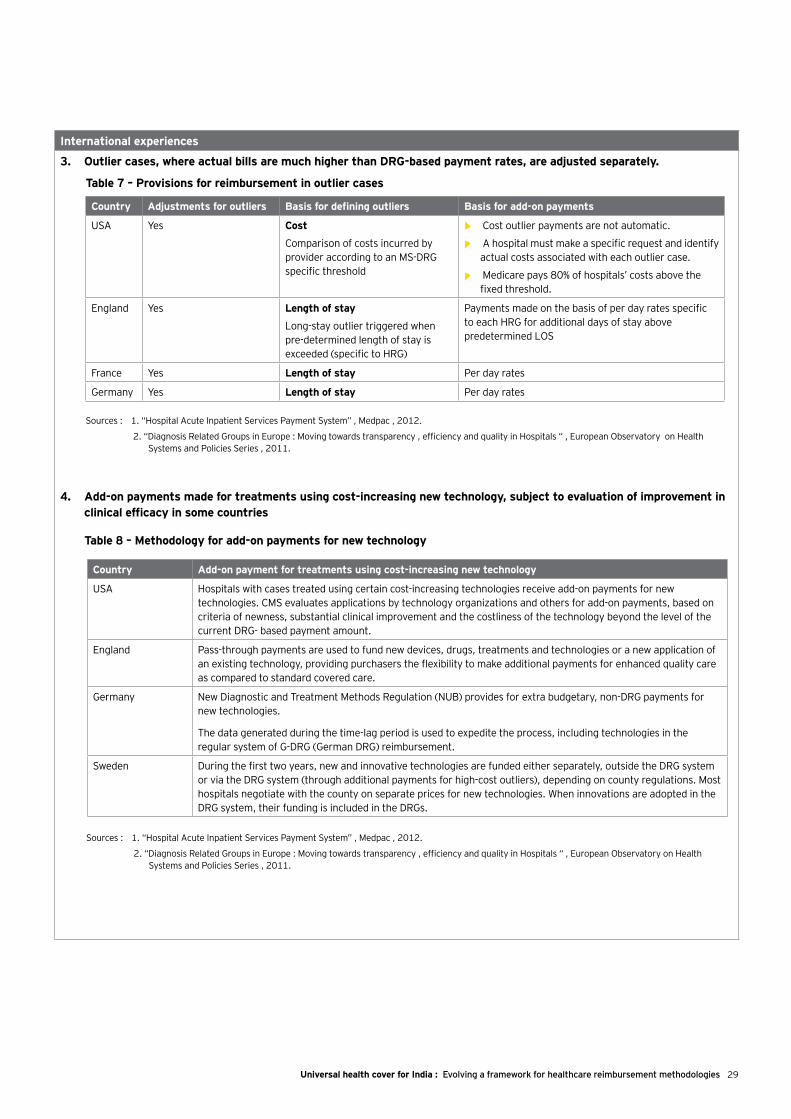
Country Adjustments for outliers Basis for defining outliers Basis for add-on payments
USA Yes Cost
Comparison of costs incurred by provider according to an MS-DRG specific threshold
• ► Cost outlier payments are not automatic.
• ► A hospital must make a specific request and identify actual costs associated with each outlier case.
• ► Medicare pays 80% of hospitals’ costs above the fixed threshold.
England Yes Length of stay
Long-stay outlier triggered when pre-determined length of stay is exceeded (specific to HRG)
Payments made on the basis of per day rates specific to each HRG for additional days of stay above predetermined LOS
France Yes Length of stay Per day rates
Germany Yes Length of stay Per day rates
Table 7 – Provisions for reimbursement in outlier cases
Country Add-on payment for treatments using cost-increasing new technology
USA Hospitals with cases treated using certain cost-increasing technologies receive add-on payments for new technologies. CMS evaluates applications by technology organizations and others for add-on payments, based on criteria of newness, substantial clinical improvement and the costliness of the technology beyond the level of the current DRG- based payment amount.
England Pass-through payments are used to fund new devices, drugs, treatments and technologies or a new application of an existing technology, providing purchasers the flexibility to make additional payments for enhanced quality care as compared to standard covered care.
Germany New Diagnostic and Treatment Methods Regulation (NUB) provides for extra budgetary, non-DRG payments for new technologies.
The data generated during the time-lag period is used to expedite the process, including technologies in the regular system of G-DRG (German DRG) reimbursement.
Sweden During the first two years, new and innovative technologies are funded either separately, outside the DRG system or via the DRG system (through additional payments for high-cost outliers), depending on county regulations. Most hospitals negotiate with the county on separate prices for new technologies. When innovations are adopted in the DRG system, their funding is included in the DRGs.
Sources : 1. “Hospital Acute Inpatient Services Payment System” , Medpac , 2012.
2. “Diagnosis Related Groups in Europe : Moving towards transparency , efficiency and quality in Hospitals “ , European Observatory on Health Systems and Policies Series , 2011.
Table 8 – Methodology for add-on payments for new technology
International experiences
3. Outlier cases, where actual bills are much higher than DRG-based payment rates, are adjusted separately.
4. Add-on payments made for treatments using cost-increasing new technology, subject to evaluation of improvement in clinical efficacy in some countries
30 Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
Key learning for India
• In the current state, each government-sponsored scheme is independently administered by different authorities leading to large variances in reimbursement rates even for the same procedure (CABG rates vary by 100%, hysterectomy rates by 150% across schemes). In this context, there is a need for a national administrative body for governance and oversight of reimbursement mechanisms. One of the key objectives of this body would be to provide reference rates for all government sponsored schemes irrespective of whether they are state or centre driven.
• The reimbursement mechanism should aim to employ true cost as basis for tariff determination with the following objectives
• Capture of cost data from a representative sample of providers for each provider grade based on quality and region group
• Determination of base tariff based on choice of appropriate method. E.g. average of full cost, average of full costs weighted by volumes of patients served under government-sponsored schemes
• Provisions for selective additional reimbursements for outlier cases
The formation of a national administrative body also becomes relevant given the fact that tariff determination based on true costs is an administratively complex process requiring technical and economic expertise apart from requisite infrastructure to collect costs from a large sample of providers.
• Hospitals treating a disproportionately high share of low income patients may be at a disadvantage as they may have low margins and low returns on investment. Social insurance schemes globally (such as Medicare in USA) make add-on payments to such hospitals based on the percentage of low-income patients treated. In Indian context, to promote private healthcare providers to focus on government sponsored patients, reimbursement tariffs can be appropriately adjusted to ensure reasonable returns
• To incentivize adoption of new technologies which can possibly advance quality of care, adjustments to reimbursement tariffs should be considered, subject to evaluation of improvement of efficacy. Globally such incentives are offered in countries such as USA, England, Sweden, Germany
• In the long term, the national administrative body should aim to achieve the following:
• Drive implementation of costing systems in all empanelled hospitals.
• Implement mechanism of data checks/audits to ensure authenticity of data collected.
• Deploy IT systems to assist in converting costs to reimbursement tariffs in a short period of time.

31Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
Current Indian context
• Most government-sponsored health insurance schemes do not have a defined periodicity for revisions made in payment rates.
• CGHS has no fixed interval for revisions made in its payment rate, but this typically takes place once in around three years. It uses the competitive tender route to invite quotations from empanelled hospitals for all procedures/treatments in its benefits package and the lowest bid is fixed as the payment rate for each procedure.
• ESIS follows CGHS rates and therefore revisions are made once CGHS rates are revised.
• Rajiv Aarogyasri has no fixed interval for making revisions in its payment rate. These take place once in more than four years. While its process for fixing tariffs or revising them is not clearly defined, this involves deliberations between government and provider representatives.
International experiences
1. Annual tariff revision in most countries using cost data received from hospitals
Most developed countries annually revise their classification system of procedures/treatments, re-calculate payment rates for each procedure and update the index, which enables calibration of location-specific costs for different locations
4. Payment revisions
Modification to DRG (Diagnosis Related Groups) classification based on actual data of patient & case wise data (with a 2 year lag) to account for –
► New technologies and treatment patterns
► Cases within a DRG with similar pattern of resource intensity and common clinical characteristics
Recalibration of payment rates by adjustments made to DRG weights by following the below-mentioned steps –
► Collection of data of all bills from all empanelled hospitals for each DRG
► Statistical removal of variations in location and provider specific costs (such as wage levels in the area, add-on payments for type of provider) to get standardized charges for each case
► National average standardized charges for a DRG considered as the payment rate
The standardized average charges for a DRG are typically adjusted by a factor that reflects the relative hospital wage level in a given geographic area to account for region specific cost variations. This wage index is also updated annually based on -
► A survey of wages and wage related costs of hospitals
Re-classification of groups
Re-calibrationof rates
Processperiodicity -
annual
Updation oflocal market
index
Source : “Medicare Hospital Prospective Payment System How DRG Rates Are Calculated and Updated” , Office of Inspector General ,Office of Evaluation and Inspections ,Region IX ,2001.
Table 9 - Revisions in payment rates in the US (Medicare payment system for acute in-patient care)
Key learnings
• There should be a reasonable time period for effecting payment revisions to the reimbursement tariffs. To begin with the periodicity could be once in 2 years. Collecting costs and converting them to reimbursement tariffs can be an enormous task and there could be time gaps between these two activities. Hence it will also be important to adjust for cost changes in the interim period through identification of appropriate cost drivers and indices. Also, going forward, like in most countries, tariffs may be revised annually supported by adequate IT and other infrastructure.
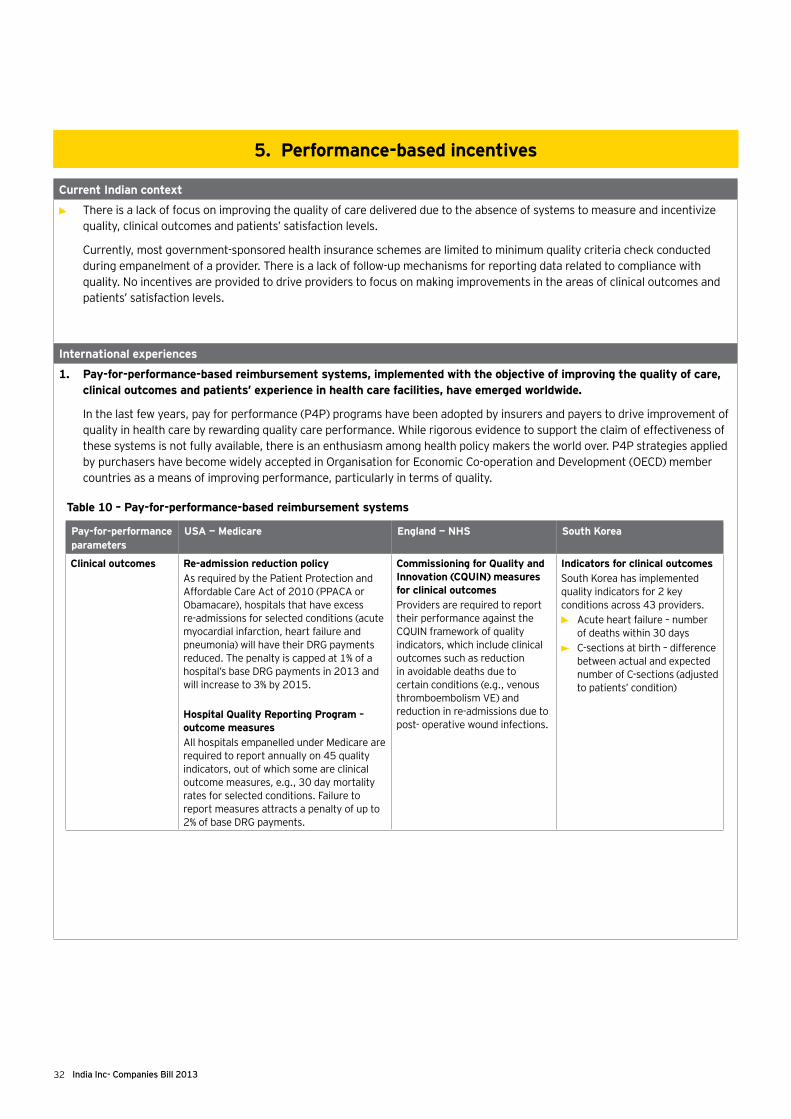
32 India Inc- Companies Bill 2013
Current Indian context
• There is a lack of focus on improving the quality of care delivered due to the absence of systems to measure and incentivize quality, clinical outcomes and patients’ satisfaction levels.
Currently, most government-sponsored health insurance schemes are limited to minimum quality criteria check conducted during empanelment of a provider. There is a lack of follow-up mechanisms for reporting data related to compliance with quality. No incentives are provided to drive providers to focus on making improvements in the areas of clinical outcomes and patients’ satisfaction levels.
International experiences
1. Pay-for-performance-based reimbursement systems, implemented with the objective of improving the quality of care, clinical outcomes and patients’ experience in health care facilities, have emerged worldwide.
In the last few years, pay for performance (P4P) programs have been adopted by insurers and payers to drive improvement of quality in health care by rewarding quality care performance. While rigorous evidence to support the claim of effectiveness of these systems is not fully available, there is an enthusiasm among health policy makers the world over. P4P strategies applied by purchasers have become widely accepted in Organisation for Economic Co-operation and Development (OECD) member countries as a means of improving performance, particularly in terms of quality.
5. Performance-based incentives
Pay-for-performance parameters
USA — Medicare England — NHS South Korea
Clinical outcomes Re-admission reduction policyAs required by the Patient Protection and Affordable Care Act of 2010 (PPACA or Obamacare), hospitals that have excess re-admissions for selected conditions (acute myocardial infarction, heart failure and pneumonia) will have their DRG payments reduced. The penalty is capped at 1% of a hospital’s base DRG payments in 2013 and will increase to 3% by 2015.
Hospital Quality Reporting Program – outcome measuresAll hospitals empanelled under Medicare are required to report annually on 45 quality indicators, out of which some are clinical outcome measures, e.g., 30 day mortality rates for selected conditions. Failure to report measures attracts a penalty of up to 2% of base DRG payments.
Commissioning for Quality and Innovation (CQUIN) measures for clinical outcomesProviders are required to report their performance against the CQUIN framework of quality indicators, which include clinical outcomes such as reduction in avoidable deaths due to certain conditions (e.g., venous thromboembolism VE) and reduction in re-admissions due to post- operative wound infections.
Indicators for clinical outcomes South Korea has implemented quality indicators for 2 key conditions across 43 providers.• Acute heart failure – number
of deaths within 30 days• C-sections at birth – difference
between actual and expected number of C-sections (adjusted to patients’ condition)
Table 10 – Pay-for-performance-based reimbursement systems

33Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
Key learning for India
• ► The reimbursement mechanism should address additional agendas such as clinical performance and patient experience. Please refer annexure 3 for illustrative list of parameters
• ► In the longer term, the reimbursement methodology should strive to create a mechanism to promote patient choice with data on comparable performance of hospitals to be made publicly available like in most other countries
International experiences
Pay-for-performance parameters
USA — Medicare England — NHS South Korea
Process quality indicators
Value-based purchasing – clinical process of care measuresAs mandated by PPACA, the value-based incentive program will be implemented in FY 2013. Out of the 45 quality indicators that hospitals report 13 have been selected for disbursement of value-based incentives. CMS will redistribute 1% of base DRG payments to hospitals, based on their overall performance in 2013, increasing this to 2% by 2015.
CQUIN measures for safety and effectivenessThe CQUIN framework of quality indicators includes safety and effectiveness parameters related to clinical processes, e.g., identification of and counseling of smokers and alcohol users and screening for premature retinopathy in neonates.Incentives of up to 1.5% of total contract income are offered to providers for their demonstrated performance.
Indicators for qualityFor the same conditions, there are process quality indicators such as treatment of acute heart failure within 120 minutes, administration of aspirin on arrival, prescription of aspirin and beta-blocker on discharge, etc.Hospitals are classified into five groups, based on their performance. The group with the best performers receives an incentive of 1% of total payments of that year.
Patient satisfaction Value-based purchasing – consumer survey measuresMedicare’s value-based incentive program, based on quality indicators, includes a survey of consumers on health care providers. This provides a measure of patients’ satisfaction levels.
CQUIN measures to gauge patients’ satisfaction levelsPatients’ satisfaction levels are measured on parameters such as health care providers’ responsiveness to the personal needs of patients.
Source: 1. “Diagnosis Related Groups in Europe: Moving towards transparency , efficiency and quality in Hospitals “ , European Observatory on Health Systems and Policies Series , 2011
2. “Medicare Hospital Prospective Payment System How DRG Rates Are Calculated and Updated” , Office of Inspector General ,Office of Evaluation and Inspections ,Region IX ,2001
3. EY knowledge base

34 Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
Recommendations3
35Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
The current focus of most government schemes (for hospitalization cases) is on the economics of procurement rather than on aspects related to patients’ safety and care. A fundamental shift is required in which the Government, while determining the provider reimbursement system, first evaluates health care providers on their standards of patient safety and quality of care. Reimbursement system should consider the following principles:
1. Follow ‘case-based’ reimbursement model as is the current practice, making it more robust through standardization and refinement of case definitions
2. Employ ‘true’ cost as a basis for tariff and recognize cost structure differences on account of quality and geography
3. Centrally determine reference tariff rates based on a formula that recognizes relevant costs, quantum of government-sponsored patients served and clinical advancement
4. Additionally, reward performance to drive chosen objectives
5. Define provisions for adequate and timely revision of tariffs

36 Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
Given the current state, there is a need to strengthen the current provider reimbursement system and create a robust framework to facilitate a smooth, effective and sustainable engagement between government payers and private health care providers with the objective of meeting the agenda of Universal Health Cover. Key recommendations include:
Aspect of framework Recommendations – Horizon 1 (near term) Recommendations – Horizon 2 (long term)
Reimbursement model 1. Review of packages defined under government-sponsored health insurance schemes:
• Standardize package definitions across different government-sponsored health schemes referring standard classification like ICD-10
• Incorporate variations in the severity of procedures and treatments on the basis of co-morbidities and complications in the definition of “packages”.
With coverage of government-sponsored health insurance schemes likely to expand in the future, encourage adoption of ICD-10 or equivalent system of classification at all empanelled hospitals and move towards a uniform system of severity-adjusted DRG-based classification of inpatient services. To achieve this, the Government should take the following steps:
• Define an appropriate classification system for India.
• Delineate standard information architecture, specifying information to be collected by empanelled hospitals and shared with payer-appointed body.
• Define contracts with empanelled providers, mandating them to share required data on hospital-based and claim-based statistics (including costs and quality).
• Incentivize health care providers to implement appropriate information technology platforms, which support DRG-based service classification, service costing and data interchange with government-appointed body, within a defined time-frame.
• Develop infrastructure and systems to obtain and record case information, including primary and secondary diagnoses and treatment strategy, from empanelled hospitals.
• Deploy robust governance systems that achieve the following:
• Validate DRG classification, based on clinical conditions, e.g., Medicare’s Grouper.
• Support rule-based identification of potential fraudulent cases.
• Promote compliance with treatment protocols and contractual norms.
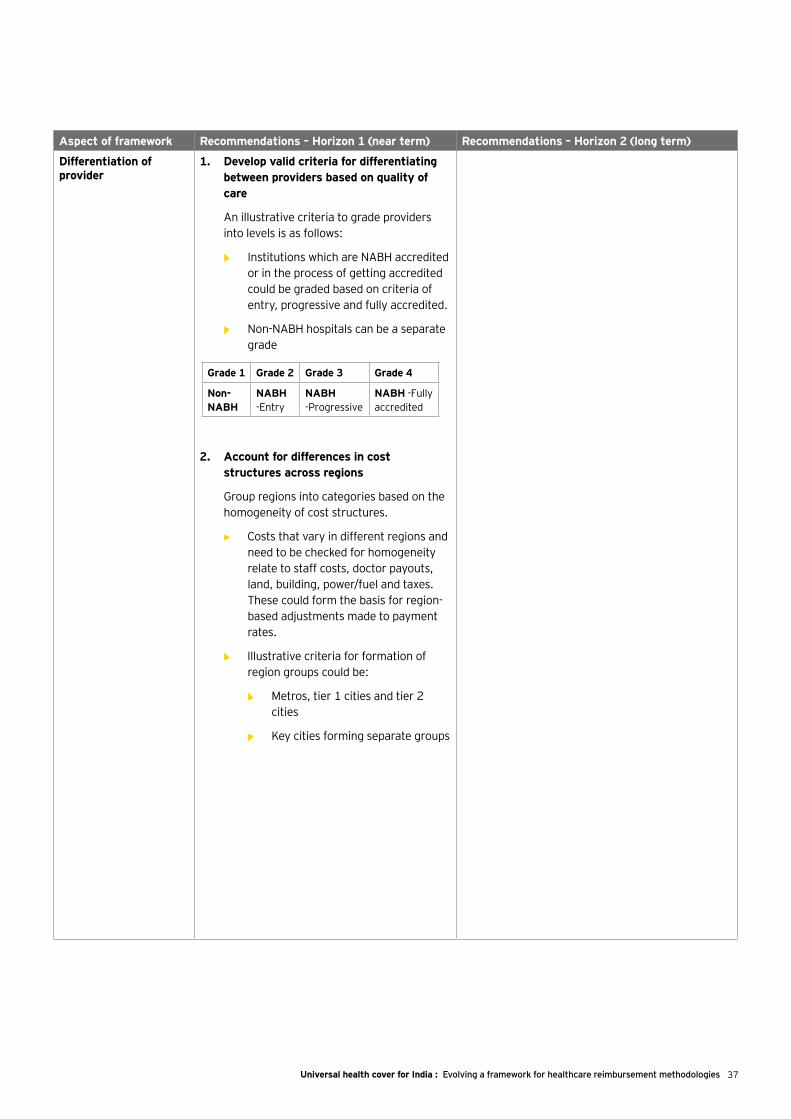
37Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
Grade 1 Grade 2 Grade 3 Grade 4
Non-NABH
NABH -Entry
NABH -Progressive
NABH -Fully accredited
Aspect of framework Recommendations – Horizon 1 (near term) Recommendations – Horizon 2 (long term)
Differentiation of provider
1. Develop valid criteria for differentiating between providers based on quality of care
An illustrative criteria to grade providers into levels is as follows:
• Institutions which are NABH accredited or in the process of getting accredited could be graded based on criteria of entry, progressive and fully accredited.
• Non-NABH hospitals can be a separate grade
2. Account for differences in cost structures across regions
Group regions into categories based on the homogeneity of cost structures.
• ► Costs that vary in different regions and need to be checked for homogeneity relate to staff costs, doctor payouts, land, building, power/fuel and taxes. These could form the basis for region- based adjustments made to payment rates.
• ► Illustrative criteria for formation of region groups could be:
• Metros, tier 1 cities and tier 2 cities
• Key cities forming separate groups

38 Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
Aspect of framework Recommendations – Horizon 1 (near term) Recommendations – Horizon 2 (long term)
Determination of payment rate
1. Set up a national administrative body for governance and oversight of reimbursement mechanisms and for reference tariff fixation, with adequate representation from centre, state and industry backed by requisite technical support. One of the key objectives of this body would be to fix provider reimbursement rates which may act as a reference point for all government- sponsored health insurance schemes irrespective of whether they are state or centre driven
2. Define national costing framework for costing of health care services (up to case type – bed type combination level) which includes definition of cost elements and guidelines to standardize their treatment for the purpose of costing
3. Determine cost of delivering health care services based on actual cost collected from a representative sample of providers:
• Collect procedure/treatment-wise detailed cost data from a sample of hospitals (refer to Annexure 1 for the illustrative cost sheet template)
• Use a stratified sample to ensure adequate representation of different grades of providers in different regions (At least 10% of empanelled providers in each grade)
• In cases where the cost structures in particular regions are inordinately high relative to other regions, evaluate reasons for the same. Apply an adjustment factor for such regions to bring down costs to a rational level with clear directional input to providers in these regions to improve efficiencies
In the long term, an organizational body should aim to:
Drive implementation of costing systems in all empanelled hospitals.
• Implement mechanism of data checks/ audits to ensure authenticity of data collected.
Deploy IT systems to assist in converting costs to reimbursement tariffs in a short period of time.
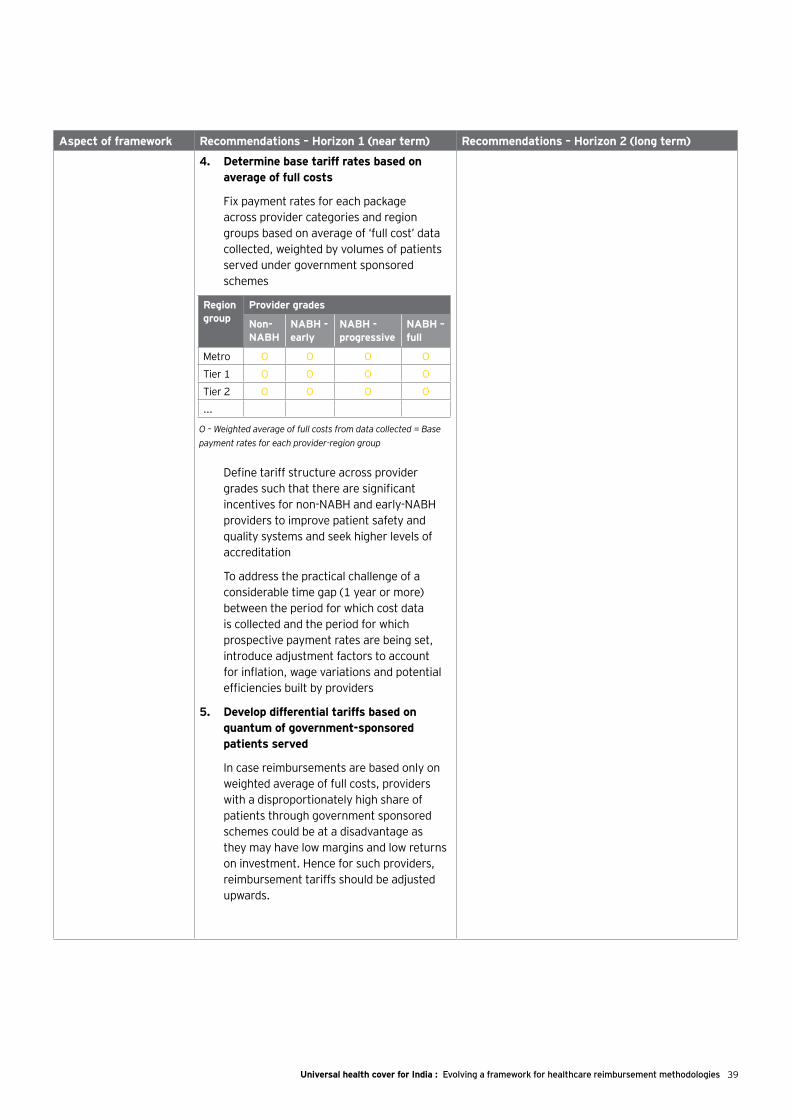
39Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
Region group
Provider grades
Non-NABH
NABH - early
NABH - progressive
NABH – full
Metro O O O O
Tier 1 O O O O
Tier 2 O O O O
...
O – Weighted average of full costs from data collected = Base payment rates for each provider-region group
Aspect of framework Recommendations – Horizon 1 (near term) Recommendations – Horizon 2 (long term)
4. Determine base tariff rates based on average of full costs
Fix payment rates for each package across provider categories and region groups based on average of ‘full cost’ data collected, weighted by volumes of patients served under government sponsored schemes
Define tariff structure across provider grades such that there are significant incentives for non-NABH and early-NABH providers to improve patient safety and quality systems and seek higher levels of accreditation
To address the practical challenge of a considerable time gap (1 year or more) between the period for which cost data is collected and the period for which prospective payment rates are being set, introduce adjustment factors to account for inflation, wage variations and potential efficiencies built by providers
5. Develop differential tariffs based on quantum of government-sponsored patients served
In case reimbursements are based only on weighted average of full costs, providers with a disproportionately high share of patients through government sponsored schemes could be at a disadvantage as they may have low margins and low returns on investment. Hence for such providers, reimbursement tariffs should be adjusted upwards.
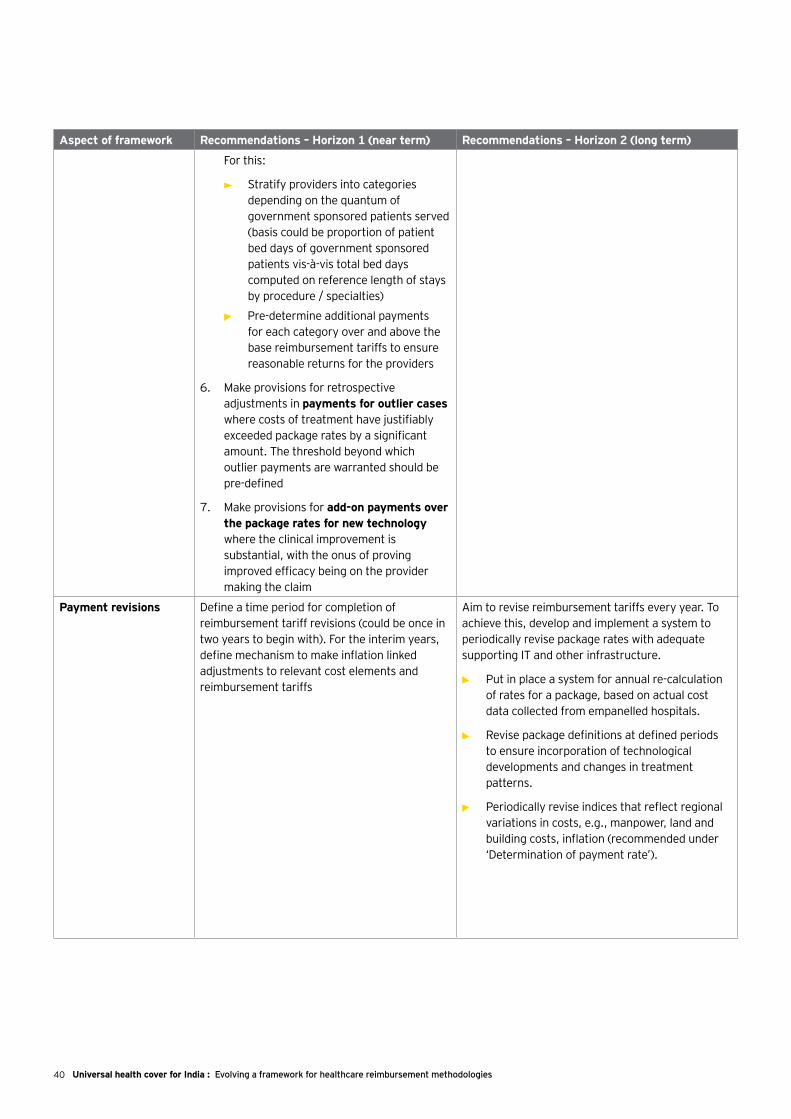
40 Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
Aspect of framework Recommendations – Horizon 1 (near term) Recommendations – Horizon 2 (long term)
For this:
• Stratify providers into categories depending on the quantum of government sponsored patients served (basis could be proportion of patient bed days of government sponsored patients vis-à-vis total bed days computed on reference length of stays by procedure / specialties)
• ► Pre-determine additional payments for each category over and above the base reimbursement tariffs to ensure reasonable returns for the providers
6. Make provisions for retrospective adjustments in payments for outlier cases where costs of treatment have justifiably exceeded package rates by a significant amount. The threshold beyond which outlier payments are warranted should be pre-defined
7. Make provisions for add-on payments over the package rates for new technology where the clinical improvement is substantial, with the onus of proving improved efficacy being on the provider making the claim
Payment revisions Define a time period for completion of reimbursement tariff revisions (could be once in two years to begin with). For the interim years, define mechanism to make inflation linked adjustments to relevant cost elements and reimbursement tariffs
Aim to revise reimbursement tariffs every year. To achieve this, develop and implement a system to periodically revise package rates with adequate supporting IT and other infrastructure.
• Put in place a system for annual re-calculation of rates for a package, based on actual cost data collected from empanelled hospitals.
• Revise package definitions at defined periods to ensure incorporation of technological developments and changes in treatment patterns.
• Periodically revise indices that reflect regional variations in costs, e.g., manpower, land and building costs, inflation (recommended under ‘Determination of payment rate’).
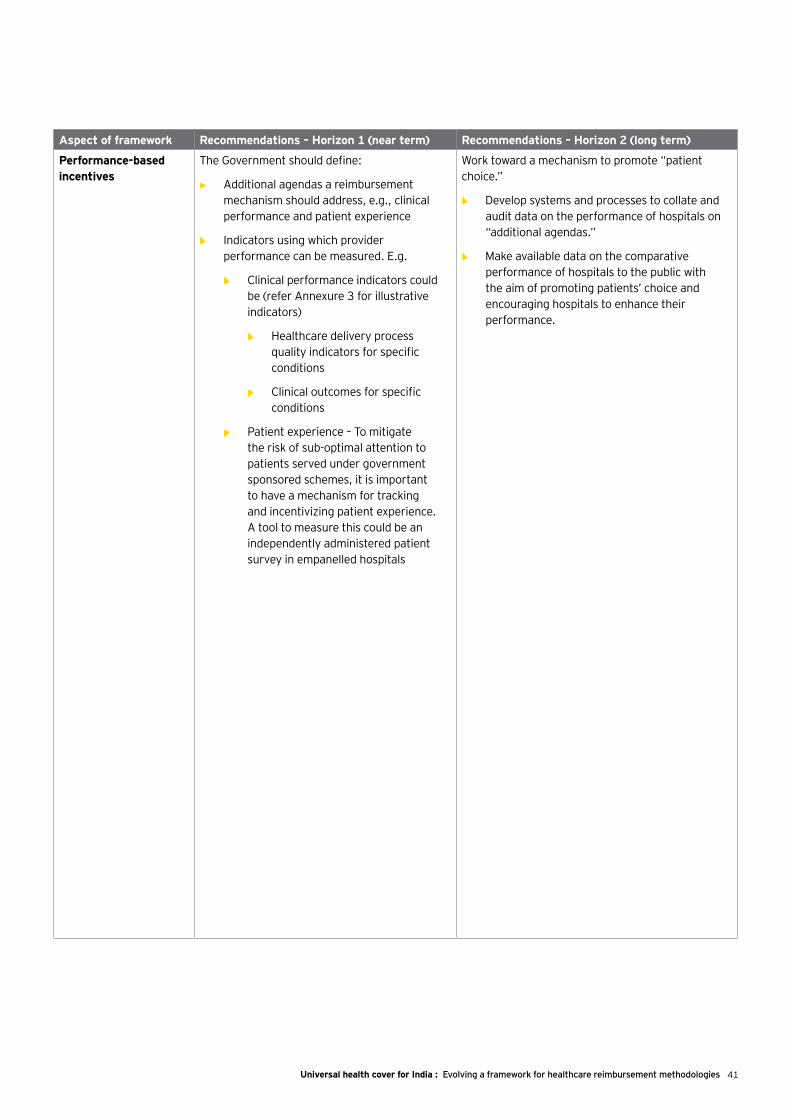
41Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
Aspect of framework Recommendations – Horizon 1 (near term) Recommendations – Horizon 2 (long term)
Performance-based incentives
The Government should define:
• Additional agendas a reimbursement mechanism should address, e.g., clinical performance and patient experience
• Indicators using which provider performance can be measured. E.g.
• Clinical performance indicators could be (refer Annexure 3 for illustrative indicators)
• Healthcare delivery process quality indicators for specific conditions
• Clinical outcomes for specific conditions
• Patient experience – To mitigate the risk of sub-optimal attention to patients served under government sponsored schemes, it is important to have a mechanism for tracking and incentivizing patient experience. A tool to measure this could be an independently administered patient survey in empanelled hospitals
Work toward a mechanism to promote “patient choice.”
• ► Develop systems and processes to collate and audit data on the performance of hospitals on “additional agendas.”
• ► Make available data on the comparative performance of hospitals to the public with the aim of promoting patients’ choice and encouraging hospitals to enhance their performance.
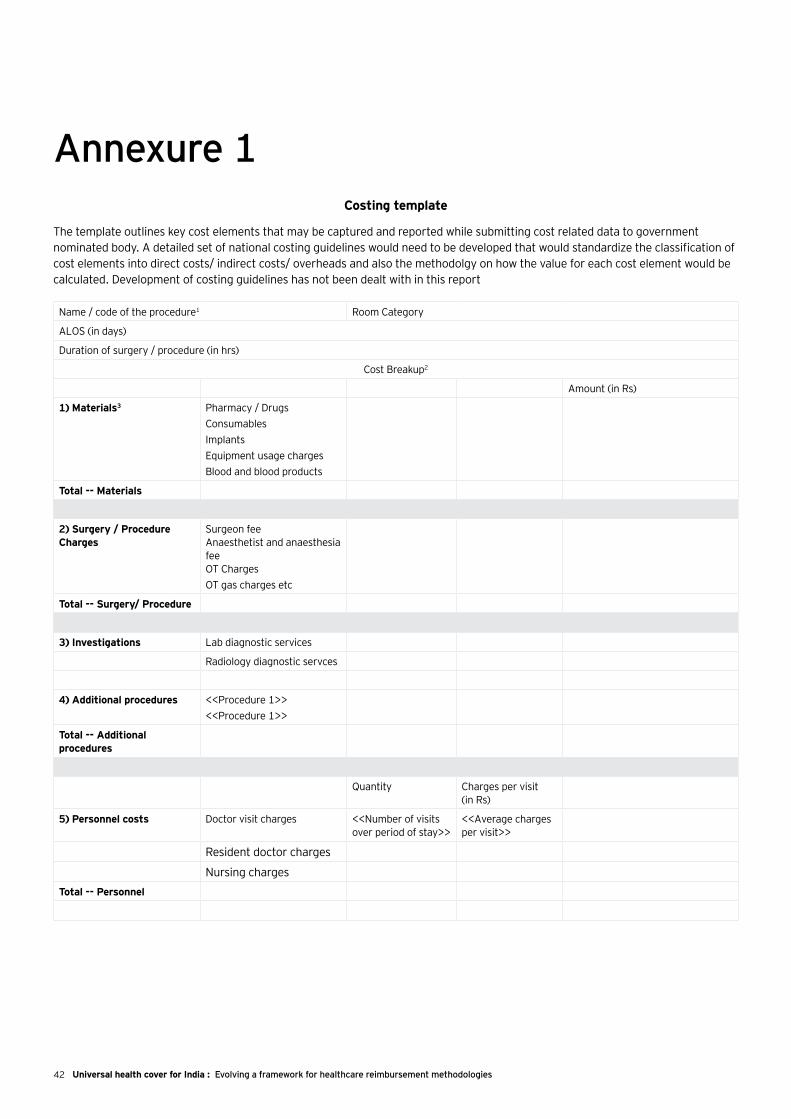
42 Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
Annexure 1Costing template
The template outlines key cost elements that may be captured and reported while submitting cost related data to government nominated body. A detailed set of national costing guidelines would need to be developed that would standardize the classification of cost elements into direct costs/ indirect costs/ overheads and also the methodolgy on how the value for each cost element would be calculated. Development of costing guidelines has not been dealt with in this report
Name / code of the procedure1 Room Category
ALOS (in days)
Duration of surgery / procedure (in hrs)
Cost Breakup2
Amount (in Rs)
1) Materials3 Pharmacy / DrugsConsumablesImplantsEquipment usage chargesBlood and blood products
Total -- Materials
2) Surgery / Procedure Charges
Surgeon feeAnaesthetist and anaesthesia feeOT ChargesOT gas charges etc
Total -- Surgery/ Procedure
3) Investigations Lab diagnostic services
Radiology diagnostic servces
4) Additional procedures <<Procedure 1>><<Procedure 1>>
Total -- Additional procedures
Quantity Charges per visit (in Rs)
5) Personnel costs Doctor visit charges <<Number of visits over period of stay>>
<<Average charges per visit>>
Resident doctor charges
Nursing chargesTotal -- Personnel

43Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
Quantity (number of days)
Rate per day (in Rs)
Amount(in Rs)
6) Stay charges Room charges
ICU charges
ER charges (if applicable)
Total -- Stay charges
7) Other charges Admission charges
Service charges
Total -- Other charges
8) Other overheads Overheads
Total cost (Rs)
1 Procedure code should be at a level that differentiates based on complexities and co-morbities involved
2 Should include all drugs, consumables and implants used for the patient. Since these are average amounts, patients wise variations in usage of material costs whould get accounted for
3 Amount to be filled in is the cost and not billing price (e.g. in case of drugs, it should be based on cost of purchase and not MRP of drugs; similarly for surgeon fee, the amount should be actual payout to doctor net of amount retained by the hospital as association fee)
44 Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
Promoting quality in Healthcare through Health Insurance
“Health Insurance as a lever to promote quality: the incentive/disincentive mechanism”
(Excerpt from the FICCI Knowledge Paper titled Health Insurance Report, 2011)
A multi-stakeholder group- “Promoting Quality in Healthcare through Health Insurance” was created by FICCI in 2011, supported by IRDA and the World Bank with representatives from NABH, RSBY, insurance companies and healthcare providers to develop a pay for quality framework through consultation and consensus. The objective of the group was to develop an incentive and disincentive mechanism which could be used by the insurance industry to promote quality in health services which shall include include healthcare providers i.e. small, medium and large into a uniform quality process encompassing and leading towards accreditation and beyond.
For the Social Insurance Schemes, the first step to trigger adoption of quality by Providers would be for the social insurance schemes to mandate reporting on quality to their Provider base. The second step would be for the NABH / IRDA / World Bank / Ministry of Health to contribute to a fund. This fund would provide a small cash incentive for providers who are part of the hospital network for social insurance and Govt insurance to pre-register for quality.
In the context of the private sector insurers, there is a need to run a quantitative pilot which details and quantifies levers within the quality framework (e.g. standard treatment protocols/reporting / documentation / audit processes) which actually contribute to lower overall claims cost.
The objective is to “reward” Providers who demonstrate intent to adopt quality by entering pre-registration process for accreditation of the NABH. Non monetary incentives include the following:
1. Shorter credit cycles for hospitals who demonstrate intent to adopt a quality framework.
2. A fast track dispute resolution mechanism
3. Quality certification as a qualifying step for a rate negotiation. In other words, Insurers would not agree to any rate changes unless the Providers adopt and demonstrate progress through the quality framework.
Implementing the above incentive schemes would automatically create a Preferred Provider Network.
In addition, the following “disincentives” shall further strengthen the quality movement:
1. Providing a deadline for pre-registering for quality as an entry criteria for empanelled insurance network hospitals
2. In the interim period – implementing a system of copays and deductibles – i.e. for hospitals which are currently on the network but not registered for pre-assessment of their quality frameworks – the level of copays / deductibles would be higher
The implementation of a system as proposed above shall undoubtedly promote quality in healthcare organizations across the country. States like Karnataka, Gujarat and Andhra Pradesh have already initiated the implementation of the Incentive Mechanism for fully accredited hospitals.
Annexure 2
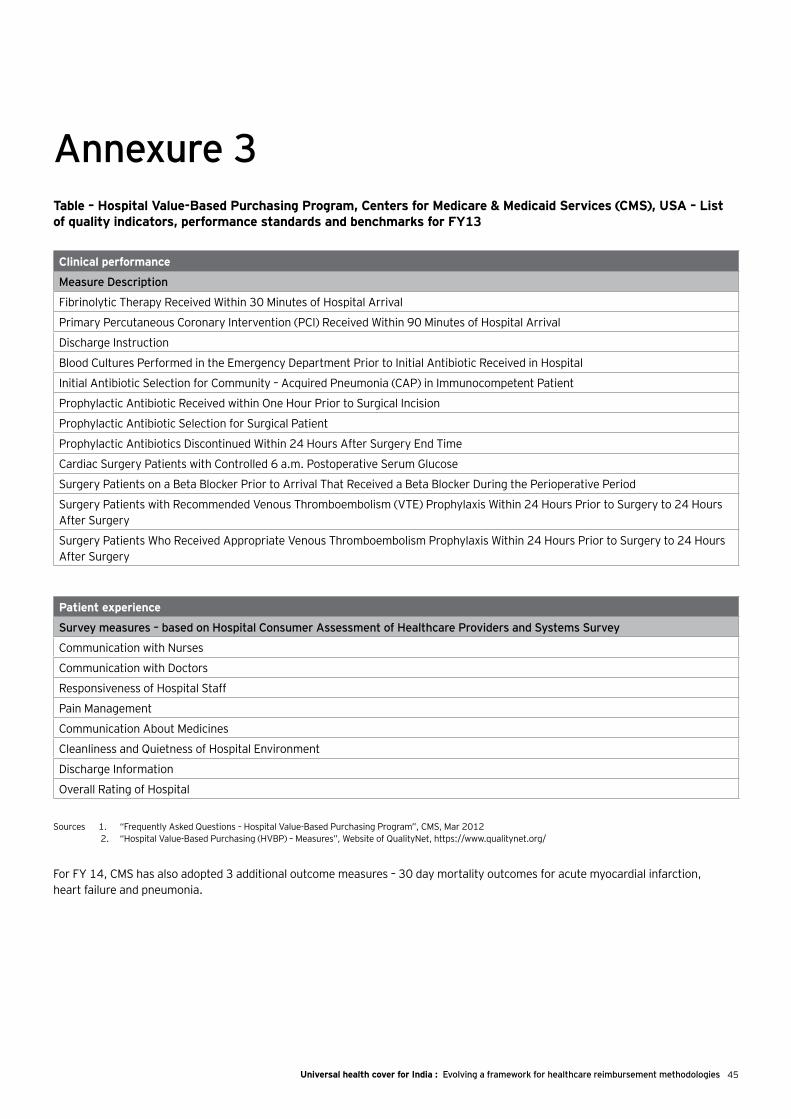
45Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
Annexure 3Table – Hospital Value-Based Purchasing Program, Centers for Medicare & Medicaid Services (CMS), USA – List of quality indicators, performance standards and benchmarks for FY13
Clinical performance
Measure Description
Fibrinolytic Therapy Received Within 30 Minutes of Hospital Arrival
Primary Percutaneous Coronary Intervention (PCI) Received Within 90 Minutes of Hospital Arrival
Discharge Instruction
Blood Cultures Performed in the Emergency Department Prior to Initial Antibiotic Received in Hospital
Initial Antibiotic Selection for Community – Acquired Pneumonia (CAP) in Immunocompetent Patient
Prophylactic Antibiotic Received within One Hour Prior to Surgical Incision
Prophylactic Antibiotic Selection for Surgical Patient
Prophylactic Antibiotics Discontinued Within 24 Hours After Surgery End Time
Cardiac Surgery Patients with Controlled 6 a.m. Postoperative Serum Glucose
Surgery Patients on a Beta Blocker Prior to Arrival That Received a Beta Blocker During the Perioperative Period
Surgery Patients with Recommended Venous Thromboembolism (VTE) Prophylaxis Within 24 Hours Prior to Surgery to 24 Hours After Surgery
Surgery Patients Who Received Appropriate Venous Thromboembolism Prophylaxis Within 24 Hours Prior to Surgery to 24 Hours After Surgery
Patient experience
Survey measures – based on Hospital Consumer Assessment of Healthcare Providers and Systems Survey
Communication with Nurses
Communication with Doctors
Responsiveness of Hospital Staff
Pain Management
Communication About Medicines
Cleanliness and Quietness of Hospital Environment
Discharge Information
Overall Rating of Hospital
Sources 1. “Frequently Asked Questions – Hospital Value-Based Purchasing Program”, CMS, Mar 2012 2. “Hospital Value-Based Purchasing (HVBP) – Measures”, Website of QualityNet, https://www.qualitynet.org/
For FY 14, CMS has also adopted 3 additional outcome measures – 30 day mortality outcomes for acute myocardial infarction, heart failure and pneumonia.

46 Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies46
List of abbreviations
Countries and states
AP Andhra Pradesh
TN Tamil Nadu
USA United States of America
UK United Kingdom
AYUSH Ayurveda , Unani , Siddha & Homeopathy
BPL Below Poverty Line
CC Complications and Co-morbidities
CGHS Central Government Health Scheme
CMS Centres for Medicare and Medicaid Services , USA
CoEs Centres of Excellence
CABG Coronary Artery Bypass Graft
CQUIN Commissioning for Quality and Innovation , England
DPP Disproportionate Patient Percentage, Medicare USA
DRG Diagnosis Related Groups
DSH Disproportionate Share Hospitals, Medicare USA
ESIS Employees’ State Insurance Scheme
FFS Fee for Service
GDP Gross Domestic Product
G-DRG German Diagnosis Related Groups
GIPSA General Insurers (Public Sector) Association
GP General Practitioner
HRG Healthcare Resource Group, England
ICD 10 International Statistical Classification of Diseases , 10th revision
ICU Intensive Care Unit
IP In-Patient
IPD In-Patient Department
LOS Length of Stay
MFF Market Forces Factor , England
MPCE Monthly Per Capita Expenditure
MS-DRG Medicare Severity Diagnosis Related Groups , USA
NABH National Accreditation Board for Hospitals & Healthcare Providers
NHIC National Health Insurance Corporation , Korea
NHS National Health Service , England
NLEM National List of Essential Medicines
NUB New Diagnostic and Treatment Methods Regulations, Germany
OECD Organization for Economic Co-operation and Development
OoP Out of Pocket
OP Out-Patient
OPD Out-Patient Department
P4P Pay for Performance
PbR Payment by Results
PCCL Patient Clinical Complexity Level, Germany
PPACA Patient Protection and Affordable Care Act , USA
PPP Public Private Partnership
RSBY Rashtriya Swasthya Bima Yojna
SME Small and Medium Enterprises
UHC Universal Health Coverage
47Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
AcknowledgementsRahul ChadhaCEO, Religare Wellness Ltd.
CG MuthanaV P Operations,Manipal Health Enterprises Pvt. Ltd.
Dr. Sanjeev ChaudhryManaging Director,SRL
Dr. Dharmindra NagarMD & CEO, Paras Hospital
Ravi DuggalIndependent Health Researcher
Dr. Somil NagpalHealth Specialist, Health Nutrition and Population,South Asia Region, The World Bank
Dr. Ravi Gaur Vice President-Operations,Oncquest
Dr. Rajeev NayyarMedical Superintendent, Fortis Hospitals
Shobha Mishra GhoshSenior Director,FICCI
Dr. Narottam PuriChairman – NABH, Advisor Health Services – FICCI and Advisor Medical, Fortis Healthcare
Dr. Shakti GuptaHOD Hospital Administration, AIIMS
Krishnan RamachandranCOO, Apollo Munich Health Insurance
R. K. JainAS & DG (CGHS),Ministry of Health & Family Welfare, GoI
Dr. Krishna ReddyCEO and Director,Care Hospitals
Manish JainDirector - Health Policy, J&J Medical
Chandra SekharExecutive Director – Marketing and StrategyGlobal Hospitals Group
Dr. Ravindra V. KaranjekarChairman – NABH accreditation committee,Exec Director & CEO, Medical Services and Quality Global Hospitals
Dr. (Capt) Sandeep Sharma Director, Axis Dental
Hon Brig Dr. Arvind LalChairman & Managing Director, Dr Lal Pathlabs
Shivkumar Tukaram Senior Manager- Government Affairs, Abbott Healthcare
Dr. Harsh MahajanHonorary Radiologist to the President of India, Mahajan Imaging Centre
Dr. Vijay VemuriAssociate Vice President,Global Hospitals, Hyderabad
Dr. S C MarwahCEO, HCV, Panacea Biotec Ltd.
Dr. Mahesh VermaDirector – Principal, Maulana Azad Institute of Dental Sciences
48 Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
EY team FICCI team
• Murali Nair
• Sumit Goel
• Kaivaan Movdawalla
• Shriharsha Sarkar
• Parth Patel
• Akash Chaudhary
• Poorvaja Sekaran
• Chandana Chandra
• Jayanta Ghosh
• Aloha McBride, USA
• Paul Dolan, Australia
• Frank Kumli, Switzerland
• Jo Smith, UK
• George Agathangelou, UK
• Dra Adriana Bassi Gasparian, Brazil
• Dr. Leandro Müller, Brazil
• Shraddha Arora, India
• Martha J. Nagy, USA
Core team
Writing and editing assistance
Design and layout
Knowledge and research assistance
FICCI Health services team:
• Shobha Mishra Ghosh
• Shilpa Sharma
• Sarita Chandra
• Siddharth Sonawat
• Sudhiranjan Banerjee
49Universal health cover for India : Evolving a framework for healthcare reimbursement methodologies
EY offices
Ahmedabad2nd floor, Shivalik Ishaan Near C.N. VidhyalayaAmbawadiAhmedabad - 380 015Tel: + 91 79 6608 3800Fax: + 91 79 6608 3900
Bengaluru12th & 13th floor“UB City”, Canberra BlockNo.24 Vittal Mallya RoadBengaluru - 560 001Tel: + 91 80 4027 5000 + 91 80 6727 5000 Fax: + 91 80 2210 6000 (12th floor)Fax: + 91 80 2224 0695 (13th floor)
1st Floor, Prestige Emerald No. 4, Madras Bank RoadLavelle Road JunctionBengaluru - 560 001Tel: + 91 80 6727 5000 Fax: + 91 80 2222 4112
Chandigarh1st Floor, SCO: 166-167Sector 9-C, Madhya MargChandigarh - 160 009 Tel: + 91 172 671 7800Fax: + 91 172 671 7888
ChennaiTidel Park, 6th & 7th Floor A Block (Module 601,701-702)No.4, Rajiv Gandhi Salai, Taramani Chennai - 600113Tel: + 91 44 6654 8100 Fax: + 91 44 2254 0120
HyderabadOval Office, 18, iLabs CentreHitech City, MadhapurHyderabad - 500081Tel: + 91 40 6736 2000Fax: + 91 40 6736 2200
Kochi9th Floor, ABAD NucleusNH-49, Maradu POKochi - 682304Tel: + 91 484 304 4000 Fax: + 91 484 270 5393
Kolkata22 Camac Street3rd floor, Block ‘C’Kolkata - 700 016Tel: + 91 33 6615 3400Fax: + 91 33 2281 7750
Mumbai14th Floor, The Ruby29 Senapati Bapat MargDadar (W), Mumbai - 400028Tel: + 91 022 6192 0000Fax: + 91 022 6192 1000
5th Floor, Block B-2Nirlon Knowledge ParkOff. Western Express HighwayGoregaon (E)Mumbai - 400 063Tel: + 91 22 6192 0000Fax: + 91 22 6192 3000
NCRGolf View Corporate Tower BNear DLF Golf CourseSector 42Gurgaon - 122002Tel: + 91 124 464 4000Fax: + 91 124 464 4050
6th floor, HT House18-20 Kasturba Gandhi Marg New Delhi - 110 001Tel: + 91 11 4363 3000 Fax: + 91 11 4363 3200
4th & 5th Floor, Plot No 2B, Tower 2, Sector 126, NOIDA 201 304 Gautam Budh Nagar, U.P. IndiaTel: + 91 120 671 7000 Fax: + 91 120 671 7171
PuneC-401, 4th floor Panchshil Tech ParkYerwada (Near Don Bosco School)Pune - 411 006Tel: + 91 20 6603 6000Fax: + 91 20 6601 5900
FICCI team

Scan this QR Code for more or visit www.ey.com/in
To download your free QR code scanner, visit your smartphone’s app-store
Available on
Ernst & Young LLPEY | Assurance | Tax | Transactions | Advisory
About EYEY is a global leader in assurance, tax, transaction and advisory services. The insights and quality services we deliver help build trust and confidence in the capital markets and in economies the world over. We develop outstanding leaders who team to deliver on our promises to all of our stakeholders. In so doing, we play a critical role in building a better working world for our people, for our clients and for our communities.
EY refers to the global organization, and may refer to one or more, of the member firms of Ernst & Young Global Limited, each of which is a separate legal entity. Ernst & Young Global Limited, a UK company limited by guarantee, does not provide services to clients. For more information about our organization, please visit ey.com.
Ernst & Young LLP is one of the Indian client serving member firms of EYGM Limited. For more information about our organization, please visit www.ey.com/in.
Ernst & Young LLP is a Limited Liability Partnership, registered under the Limited Liability Partnership Act, 2008 in India, having its registered office at 22 Camac Street, 3rd Floor, Block C, Kolkata - 700016
© 2013 Ernst & Young LLP. Published in India. All Rights Reserved.
EYIN1308-063 ED None
This publication contains information in summary form and is therefore intended for general guidance only. It is not intended to be a substitute for detailed research or the exercise of professional judgment. Neither Ernst & Young LLP nor any other member of the global Ernst & Young organization can accept any responsibility for loss occasioned to any person acting or refraining from action as a result of any material in this publication. On any specific matter, reference should be made to the appropriate advisor.
Established in 1927, FICCI is the largest and oldest apex business organisation in India. Its history is closely interwoven with India’s struggle for independence, its industrialization, and its emergence as one of the most rapidly growing global economies. FICCI has contributed to this historical process by encouraging debate, articulating the private sector’s views and influencing policy.
A non-government, not-for-profit organisation, FICCI is the voice of India’s business and industry.
FICCI draws its membership from the corporate sector, both private and public, including SMEs and MNCs; FICCI enjoys an indirect membership of over 2, 50,000 companies from various regional chambers of commerce.
FICCI provides a platform for sector specific consensus building and networking and as the first port of call for Indian industry and the international business community.
Our Vision
To be the thought leader for industry, its voice for policy change and its guardian for effective implementation.
Our Mission
To carry forward our initiatives in support of rapid, inclusive and sustainable growth that encompasses health, education, livelihood, governance and skill development.
To enhance efficiency and global competitiveness of Indian industry and to expand business opportunities both in domestic and foreign markets through a range of specialised services and global linkages.
Contact us:
FICCI, Federation HouseTansen Marg, New Delhi - 110 001Tel: 011 23357246 (D), 011 2373 8760 - 70 (Ext. 220/ 438/ 246)Fax: 011 2332 0714, 011 2372 1504Email: [email protected]
Visit us at: www.ficci-heal.com
About FICCI