Embed Size (px)
Citation preview

BIOCHEMICAL AND BIOPHYSICAL RESEARCH COMMUNICATIONS 240, 545–551 (1997)ARTICLE NO. RC977691
Universal Skew of T Cell Receptor (TCR) Vb Usagefor Crohn’s Disease (CrD)
Hiroyuki Ogawa,* Hiroaki Ito,*,1 Akira Takeda,* Sumie Kanazawa,* Mitsunari Yamamoto,*Hideji Nakamura,* Yoshihiro Kimura,* Kazuyuki Yoshizaki,† and Tadamitsu Kishimoto**Department of Medicine III, Osaka University Medical School and †Faculty of Health and Sport Sciences,Osaka University, 2-2, Yamada-oka, Suita City, Osaka 565, Japan
Received October 9, 1997
cell mediated. T cells in the lamina propria were shownIt would be of clear interest and importance to iden- to be activated with CD25 expression (3). The number
tify T cell populations which correlate with the initia- of ab/ T cells increased in the intestinal mucosa, whiletion of some T cell-mediated diseases; however, it is the number of gd/ T cells did not. Therefore, ab/ Tdifficult to observe the initial response of T cells in cells were thought to play an important role in thethese diseases because of modification due to immuno- pathogenesis of CrD (4). In addition, immunomodulat-suppressive treatment. We investigated T cell receptor
ing therapies that target T cells such as cyclosporine(TCR) Vb usage in both affected and unaffected mucosa(5) and anti-CD4 monoclonal antibody (6) were provedfrom 16 patients with active Crohn’s disease (CrD), un-to be effective. It was also reported that a patient withdergoing nutritional therapy without any immunomod-active CrD showed complete remission after sufferingulatory medications. Semiquantitative reverse tran-severe CD4/ T cell deficiency due to HIV infection (7).scriptase-polymerase chain reaction showed increasedThese findings suggest that CD4/ ab/ T cells may playexpression of Vb12 and 13 in the entire mucosa of CrDa crucial role in its pathogenesis.but not in the controls. This was confirmed by introduc-
Analysis of T cell repertoire is useful to investigateing a random cloning method. Such skewing was ob-the nature and the specificity of the responses mediatedserved primarily in CD4/ lamina propria lymphocytes.
DNA sequence analysis demonstrated a striking clonal by T cells. In fact, in human autoimmune diseases suchexpansion of Vb12 T cells, but the dominant clones were as multiple sclerosis (8), rheumatoid arthritis (9), andnot identical in the patients. These findings suggest the Sjogren’s disease (10), skewed TCR repertoire has beenimportance of superantigen as well as specific T cell demonstrated, which was considered to be relevant toresponse in the pathogenesis of CrD. q 1997 Academic Press their pathogenesis. Therefore, we examined the TCR
Vb usage in the intestinal mucosa of CrD, based on thehypothesis that CrD may be initiated by an antigen-driven T cell response.
CrD is a chronic granulomatous inflammatory dis-ease which can affect any portion of gastrointestinal
MATERIALS AND METHODStract. Discontinuous (skipping) ulceration, stricturing,and fistula formation are the morphological findings of
Patients and tissue samples. Following approval of the EthicalCrD. Its clinical course is characterized by repetitiveCommittee of Osaka University Medical School, mucosal samplesepisodes of remission and exacerbation. However, gran-were obtained from 16 patients with CrD by biopsy during colonos-ulomas are often seen also in normal-looking areas (1, copy or surgical resection for problems secondary to the complications
2). Increasing evidence suggests that CrD might be T of CrD. The diagnoses of CrD were based on clinical, endoscopic,radiologic and histopathologic criteria (11). All patients were Japa-nese; 8 females and 8 males with a mean age of 25.2 years (range16Ç48). Each patient had active disease diagnosed by IOIBD score1 Correspondence to Hiroaki Ito, M.D., Department of Medicine
III, Osaka University Medical School, 2-2, Yamada-oka, Suita City, (IOIBD stands for International Organization for the Study of In-flammatory Bowel Disease; mean score 3.1, range 2Ç7) (12). At theOsaka 565, Japan. Fax: (81) 6-879-3839. E-mail: hiroito@imed3.
med.osaka-u.ac.jp. time of sampling, none of the patients had received corticosteroidsor other immunosuppressive medications during the preceding 3Abbreviations used: CrD, Crohn’s disease; UC, ulcerative colitis;
TCR, T cell receptor; PBL, peripheral blood lymphocyte; LPL, lamina months. Of the 14 patients on whom serologic HLA-typing was avail-able, 7 expressed HLA-DR4. Mucosal samples were obtained frompropria lymphocyte; IEL, intraepithelial lymphocyte; RT-PCR, re-
verse transcriptase-polymerase chain reaction; HBSS, Hanks’ bal- both affected (longitudinal or aphthoid ulcers) and unaffected (mac-roscopically normal) areas of each patient. Peripheral blood lympho-anced salt solution.
0006-291X/97 $25.00Copyright q 1997 by Academic PressAll rights of reproduction in any form reserved.
545
AID BBRC 7691 / 693f$$$$81 10-30-97 22:35:42 bbrcg AP: BBRC

Vol. 240, No. 3, 1997 BIOCHEMICAL AND BIOPHYSICAL RESEARCH COMMUNICATIONS
cytes (PBLs) were also drawn to compare local with systemic change.In addition, inflamed colonic mucosa was collected from 8 patientswith ulcerative colitis (UC) as disease controls, and tissue was col-lected from the uninvolved portions of 8 patients with colon canceror polyps as normal controls. PBLs were isolated by Ficoll-Paque(Pharmacia Biotech.) density gradient.
Isolation of CD4/ and CD8/ T cells from the mucosal tissue. Intra-epithelial lymphocytes (IELs) and LPLs were isolated from the mucosaof CrD patients 13 and 14 as described previously (13). Briefly, dis-sected mucosa was incubated with CMF-HBSS containing dithiothrei-tol and 2% FCS. IELs were then released by three 40 minute washesin HBSS containing 2% FCS and 1 mM EDTA. The remaining mucosaltissue was incubated overnight at 377C in RPMI 1640 containing0.01% collagenase I (Sigma Chemical) and 0.01% deoxyribonucleaseI (Takara Biochemicals) to collect LPLs. Each IEL and LPL fractionwas passed through a 100 mm nylon membrane, and applied to subse-quent 44%/66% Percoll (Pharmacia) density gradient. CD4/ and CD8/
T cells were purified using magnetic beads conjugated with anti-hu-man CD4 (Leu-3a) or anti-human CD8 (Leu-2a) monoclonal antibody FIG. 1. Standard curves for quantitation of PCR amplified prod-(Miltenyi Biotec.) according to the manufacturer’s instructions. ucts. cDNA obtained from PBLs of a healthy person were titrated
and subjected to PCR as described in Materials and Methods. Autora-Semiquantitation of TCR Vb-specific RNA by RT-PCR. Totaldiographic intensities in arbitrary units were log-log plotted againstRNA was isolated from the mucosal tissue of CrD patients and con-the concentrations of RNA which was transcribed into cDNA. s, Cb;trols by acid guanidium thiocyanate-phenol-chloroform extraction ash, Vb2; j, Vb12; l, Vb13.previously described (14). The same method was applied to the isola-
tion of total RNA from the PBLs and fractionated mucosal lympho-cytes. Twenty Vb-specific primers were synthesized as previouslydescribed (10). Sense and antisense oligonucleotide, 5*-CCCGAG-
ucts amplified using each Vb primer and antisense Cb primer wereGTCGCTGTGTTTGAGCCATCAGAA-3 * and 5*-GGCAGACAGGAC-digested with Eco RI and Bgl II, and ligated into the pBluescript.CCCTTGCTGGTAGGACAC-3 * were used for amplification of 450 bpApproximately 30 white colonies were randomly picked up from LBfragment of Cb messenger RNA (mRNA). These synthesized primersplates containing X-Gal, and the inserts were sequenced on an auto-were exactly matched both Cb1 and Cb2 gene segments. Comple-mated DNA sequencer (Applied Biosystem).mentary DNA (cDNA) was synthesized by incubating 5 mg of total
RNA with 600 U of Moloney murine leukemia virus (MMLV) reversetranscriptase (GIBCO BRL Inc.) in the presence of 0.05 U of oligo- RESULTSdT primers (Pharmacia), 3 mg of acetylated bovine serum albumin(GIBCO BRL Inc.) and 40 U of RNase inhibitor (Promega) in a vol- Analysis of Vb expression by semiquantitative PCRume of 30 ml for 1 hour at 377C, then for 5 minutes at 967C to stop
amplification. The fraction of mucosal lymphocytesreaction. Each cDNA sample was PCR-amplified using 10 pmol eachwhich utilized each Vb family was estimated by semi-of sense Vb specific primer or Cb primer (internal control) with anti-
sense Cb primer in a reaction mixture of 50 ml containing KCl, quantitative PCR amplification of cDNA from intesti-Tris, MgCl2, 200 mM of dNTP (TOYOBO) and 1.25 U of Taq DNA nal tissue. As can be seen in Table 1 and Fig.2, CrDpolymerase (Perkin Elmer Cetus). Each cycle was 947C for 90 sec- patients showed marked skewing toward Vb12 andonds, 607C for 60 seconds, and 727C for 60 seconds. Quantitation of
Vb13. Vb2 expression was also noticeable but less fre-the PCR products was made by Southern blot hybridization. Aliquotsof 10 ml after 30 cycles of PCR were separated on a 2% agarose gel, quent. None of the twenty Vb families were deficientblotted onto a nitrocellulose membrane, and hybridized with a-32P- in any patients. Such skewing was seen regardless oflabeled l Hb1 fragment of human Cb gene (15). The intensities of the location or presence of macroscopic inflammation.the autoradiographic bands were quantified with microcomputer im-
The frequency of Vb12 and Vb13 in inflamed area wasaging device (Imaging Research Inc.). For standard curves for quanti-13.1 { 2.9% and 14.4 { 3.9% (mean { SD), that intation of PCR amplified products, as shown in Fig.1, cDNA obtained
from PBLs of a healthy person were titrated and PCR-amplified, unaffected area was 11.9 { 5.2% and 13.1 { 3.6%, re-and their autoradiographic intensities were log-log plotted against spectively. In contrast, no particular difference wasoriginal RNA concentrations to confirm all samples were within the seen among the expression of Vb families in either UCrange of linear relationship as previously described (10). Every Vb
patients or healthy controls. Frequency of Vb12 andgene family expression was represented as Vb/Cb (%).Vb13 in UC patients was 5.5 { 1.9% and 5.4 { 2.0%,Random cloning of cDNA from PCR products. mRNA was ex-that in healthy controls was 5.1{ 1.8% and 6.4{ 1.7%,tracted from samples obtained from patients 12 and 17 using mRNA
Purification Kit (Pharmacia) and reverse-transcribed with Cb primer respectively. No particular trend towards increased us-(CATAGAGGATGGTGGCAG for downstream) to synthesize RNA: age of Vb12 or Vb13 was seen in the PBLs from CrDcDNA duplex using cDNA synthesis Kit (Pharmacia). Double strand patients (data not shown).DNA synthesized from the duplex was digested with Eco RI and NotI, ligated to the pBluescript (Stratagene) and cloned. Approximately Vb repertoire of isolated CD4/ and CD8/ T cells from60 white colonies were randomly picked up from LB plates containing CrD patients. To determine which mucosal T cell pop-X-Gal, and screened by PCR using sense and antisense Cb primers. ulation has such prominent skewing, IELs and LPLsCb positive clones were then PCR-amplified using sense Vb-specific
were isolated from CrD patients 13 and 14, and CD4/primers and antisense Cb primer to analyze the repertoire.and CD8/ T cells were then positively selected fromCloning and sequencing of PCR-amplified TCRs. Following puri-
fication with QIAquick PCR Purification Kit (QIAGEN), PCR prod- each population. As shown in Table 2, only CD4/ LPLs
546
AID BBRC 7691 / 693f$$$$81 10-30-97 22:35:42 bbrcg AP: BBRC

Vol. 240, No. 3, 1997 BIOCHEMICAL AND BIOPHYSICAL RESEARCH COMMUNICATIONS
TABLE 1
Intestinal Vb Repertoire in CrD Patients and Controls
TCR V b/Cb (%)
Donor 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
Crohn’s disease
1 C-L 0 / 0 0 0 0 / / 0 0 0 /// /// 0 0 0 // 0 0 0C-N 0 / 0 0 0 0 / / 0 0 0 // // / 0 0 / / 0 0
2 C-L 0 / 0 0 0 0 0 / 0 0 0 /// /// 0 0 0 0 0 0 0C-N 0 // 0 0 / / / // 0 0 0 // // 0 / 0 / 0 0 0
3 C-L 0 // 0 0 0 / / 0 0 0 0 // / / 0 / / 0 0 0C-N 0 / 0 0 0 0 0 / 0 0 0 // // / 0 0 / / 0 0
4 C-L 0 // / / / 0 0 0 0 0 0 // /// 0 0 0 0 0 0 0C-N 0 /// // / / 0 / 0 0 0 0 / // / / 0 0 0 0 0
5 C-L 0 // 0 0 0 / // 0 0 0 0 // // / 0 0 / / 0 0C-N 0 / 0 0 0 0 / 0 0 0 0 / /// / / 0 0 // 0 /
6 I-L 0 // 0 0 0 0 / / 0 0 0 /// /// // 0 0 // 0 0 0I-N 0 / 0 0 / / / 0 0 0 0 /// // 0 0 / // / 0 0
7 I-L 0 // 0 0 0 0 0 // / 0 0 /// /// / 0 0 / 0 0 0I-N 0 / 0 0 0 0 / /// 0 0 0 // /// 0 0 0 0 0 0 0
8 I-L 0 // 0 0 0 0 / / 0 0 0 // /// / 0 0 // 0 0 0I-N 0 / 0 0 0 0 / / / 0 0 / // / 0 0 // 0 0 0
9 I-L 0 / 0 / / / / / / 0 0 // /// / 0 0 // 0 0 0I-N 0 / 0 0 / 0 / / 0 0 0 // // / 0 0 / / 0 0
10 I-L 0 / 0 / / 0 / / / 0 0 // // / 0 0 / 0 0 0I-N 0 0 0 / // 0 // / // 0 0 / / / 0 0 0 0 0 0
11 I-L 0 0 0 0 0 0 0 / 0 0 0 // // 0 0 0 0 / 0 0I-N 0 /// 0 0 0 0 / // / 0 0 // // 0 0 0 0 / 0 0
12 I-L 0 /// 0 0 / 0 0 / / 0 0 // // / 0 0 / 0 0 0I-N 0 / 0 0 0 0 0 / / 0 0 // // / 0 / / / 0 0C-L 0 // 0 / / 0 / / 0 0 0 / // 0 0 0 / 0 0 0
13 I-L 0 // 0 0 / 0 / / / 0 0 /// 0 / 0 0 / / 0 0I-N 0 // 0 0 0 0 0 / / 0 0 /// /// 0 0 0 / 0 0 0C-L 0 // 0 / 0 0 / 0 0 0 0 // /// 0 / 0 / 0 0 0
14 I-L 0 /// 0 0 0 0 // 0 0 0 0 / /// / 0 0 / 0 0 0I-N 0 /// 0 0 0 0 // / / 0 0 // // / 0 0 / 0 0 0
15 I-L 0 / 0 0 0 0 / / / 0 0 // // 0 0 0 / 0 0 0I-N 0 / 0 0 / / / / / 0 0 / // / 0 0 / 0 0 0
16 I-L 0 / / / 0 0 0 0 0 0 0 / // / / 0 0 0 0 0I-N 0 / / 0 0 / 0 / 0 0 0 // // / / 0 / 0 0 0
Healthy control
17 C 0 / / / 0 0 / / 0 0 0 0 0 0 0 0 0 / / 018 C 0 / 0 0 / / // // / 0 0 0 / 0 0 0 / 0 / 019 C 0 / 0 0 0 / / // 0 0 0 / / 0 0 0 / / 0 020 C 0 / 0 0 / / / / 0 0 0 / / / 0 / / 0 0 021 I 0 0 0 0 0 0 / // 0 0 0 0 0 0 0 0 0 0 0 022 I 0 / 0 0 0 / / / 0 0 0 0 / 0 0 0 0 0 0 023 I 0 / 0 / 0 0 / 0 0 0 0 0 / 0 0 0 // 0 0 024 I 0 / 0 / / 0 / / 0 0 0 / / / 0 0 / / 0 0
Ulcerative colitis
25 C 0 / 0 0 / / / / / 0 0 0 0 0 0 0 / / 0 026 C 0 / 0 / 0 / / / / 0 0 / / 0 0 0 0 0 0 027 C 0 0 0 0 0 / / // // 0 0 / 0 0 0 0 0 0 0 028 C 0 / 0 0 / / 0 / / 0 0 0 0 / / 0 // / 0 029 C 0 0 0 0 0 / // /// / 0 0 / / 0 0 0 / / 0 030 C 0 / / 0 0 0 / / 0 0 0 0 0 0 / / 0 / / 031 C 0 0 0 0 0 0 0 0 0 0 0 / / / 0 0 // // 0 032 C / / 0 0 / / // / / 0 0 / / 0 0 0 0 0 0 0
Note. Every Vb gene family expression assessed by PCR was represented as Vb/Cb (%). 0, 0-5%; /, 5-10%; //, 10-15%; ///, ú 15%.C, colon; I, ileum; L, longitudinal ulcers; N, unaffected (normal-looking) area.
547
AID BBRC 7691 / 693f$$7691 10-30-97 22:35:42 bbrcg AP: BBRC

Vol. 240, No. 3, 1997 BIOCHEMICAL AND BIOPHYSICAL RESEARCH COMMUNICATIONS
FIG. 2. Analysis of TCR Vb gene family expression. Panels A, B, C, and D show TCR Vb gene usage in the inflamed intestinal mucosaof 16 patients with CrD, the unaffected intestinal mucosa of 16 patients with CrD, the uninvolved intestinal mucosa of 8 normal controldonors and the inflamed intestinal mucosa of 8 patients with ulcerative colitis, respectively. Data are presented as Vb gene segmentexpression determined by quantitative PCR analysis expressed as a percentage of Cb gene expression, as described in Methods. Barsrepresent the means { SD of Vb densitometric values obtained for individuals.
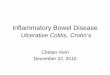
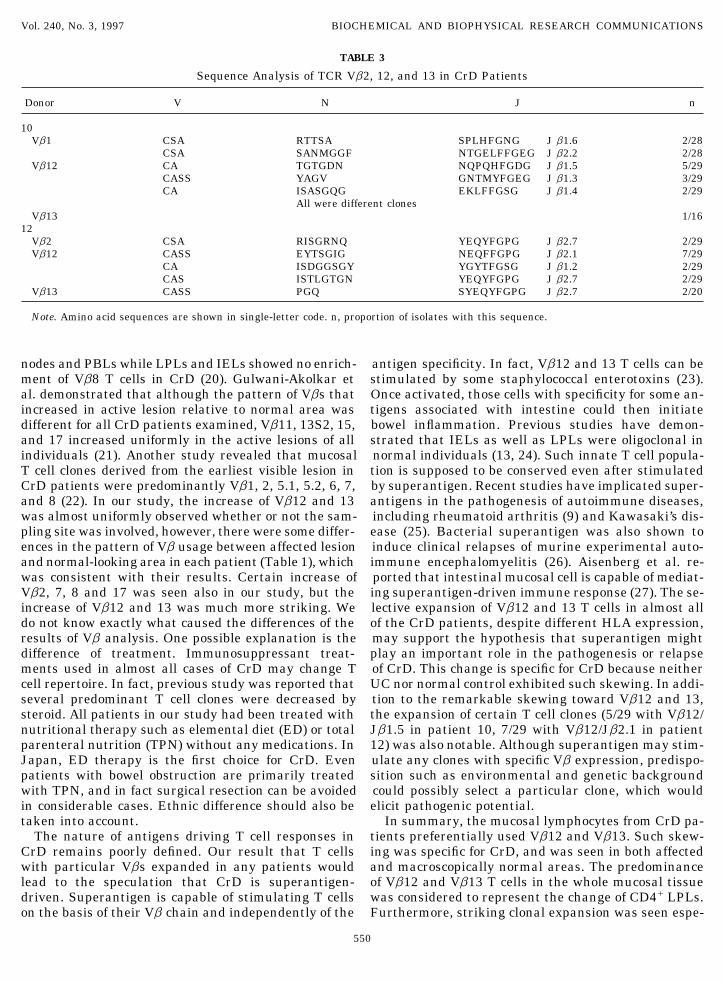
showed high expression of Vb12 and Vb13. Therefore DNA sequences of Vb2, 12 and 13 were analyzed forCrD patients 10 and 12. Table 3 shows the CDR3 regionthe skewing of Vb repertoire seen in the whole mucosal
lymphocytes from CrD patients was considered to rep- amino acid sequences as deduced from the nucleotidesequence. Reiterative sequences, identified more thanresent the characteristics of CD4/ LPLs.once, were observed in most of the Vbs examined inConfirmation of the PCR results by random cloning.both patients. Among those, clonal expansion wasApproximately 60 colonies were randomly selectedstriking especially in Vb12 in both patients but thefrom the plasmids containing cDNAs obtained from thedominant clones were not identical (5 of 29 clones withinflamed mucosa of CrD patient 12 and the normalVb12/Jb1.5 in patient 10 and 7 of 29 clones with Vb12/mucosa of control 17. Following PCR amplification withJb2.1 in patient 12).sense and antisense Cb primer, the frequency of each
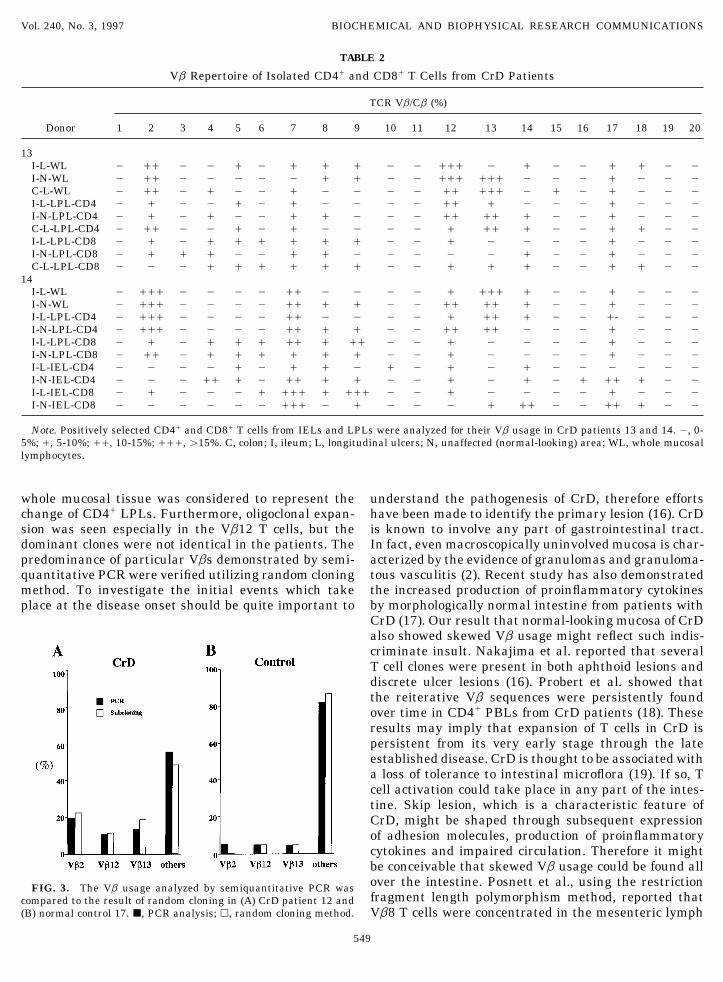
Vb was analyzed by PCR using each Vb and Cb prim-ers. As depicted in Fig. 3, the fractions of Vb2, Vb12 DISCUSSIONand Vb13 were 22.2%, 11.1% and 18.5% in the CrDpatient, 4.5%, 4.5% and 4.5% in the healthy control, The results presented here demonstrated that the mu-respectively. No significant difference was seen be- cosal lymphocytes from CrD patients preferentially usedtween the result of semiquantitative PCR analysis and Vb12 and Vb13. Such skewing was specific for CrD, andthat obtained by random cloning. was seen in both affected and macroscopically normal
areas, but was not found in the PBLs from CrD patients.Sequence analysis of samples from CrD patients. Todetermine whether there are dominant clones present, The predominance of Vb12 and Vb13 T cells in the
548
AID BBRC 7691 / 693f$$$$81 10-30-97 22:35:42 bbrcg AP: BBRC
Vol. 240, No. 3, 1997 BIOCHEMICAL AND BIOPHYSICAL RESEARCH COMMUNICATIONS
TABLE 2
Vb Repertoire of Isolated CD4/ and CD8/ T Cells from CrD Patients
TCR Vb/Cb (%)
Donor 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
13I-L-WL 0 // 0 0 / 0 / / / 0 0 /// 0 / 0 0 / / 0 0I-N-WL 0 // 0 0 0 0 0 / / 0 0 /// /// 0 0 0 / 0 0 0C-L-WL 0 // 0 / 0 0 / 0 0 0 0 // /// 0 / 0 / 0 0 0I-L-LPL-CD4 0 / 0 0 / 0 / 0 0 0 0 // / 0 0 0 / 0 0 0I-N-LPL-CD4 0 / 0 / 0 0 / / 0 0 0 // // / 0 0 / 0 0 0C-L-LPL-CD4 0 // 0 0 / 0 / 0 0 0 0 / // / 0 0 / / 0 0I-L-LPL-CD8 0 / 0 / / / / / / 0 0 / 0 0 0 0 / 0 0 0I-N-LPL-CD8 0 / / / 0 0 / / 0 0 0 0 0 / 0 0 / 0 0 0C-L-LPL-CD8 0 0 0 / / / / / / 0 0 / / / 0 0 / / 0 0
14I-L-WL 0 /// 0 0 0 0 // 0 0 0 0 / /// / 0 0 / 0 0 0I-N-WL 0 /// 0 0 0 0 // / / 0 0 // // / 0 0 / 0 0 0I-L-LPL-CD4 0 /// 0 0 0 0 // 0 0 0 0 / // / 0 0 /- 0 0 0I-N-LPL-CD4 0 /// 0 0 0 0 // / / 0 0 // // 0 0 0 / 0 0 0I-L-LPL-CD8 0 / 0 / / / // / // 0 0 / 0 0 0 0 / 0 0 0I-N-LPL-CD8 0 // 0 / / / / / / 0 0 / 0 0 0 0 / 0 0 0I-L-IEL-CD4 0 0 0 0 / 0 / / 0 / 0 / 0 / 0 0 0 0 0 0I-N-IEL-CD4 0 0 0 // / 0 // / / 0 0 / 0 / 0 / // / 0 0I-L-IEL-CD8 0 / 0 0 0 / /// / /// 0 0 / 0 0 0 0 / 0 0 0I-N-IEL-CD8 0 0 0 0 0 0 /// 0 / 0 0 0 / // 0 0 // / 0 0
Note. Positively selected CD4/ and CD8/ T cells from IELs and LPLs were analyzed for their Vb usage in CrD patients 13 and 14. 0, 0-5%; /, 5-10%; //, 10-15%; ///, ú15%. C, colon; I, ileum; L, longitudinal ulcers; N, unaffected (normal-looking) area; WL, whole mucosallymphocytes.
whole mucosal tissue was considered to represent the understand the pathogenesis of CrD, therefore effortshave been made to identify the primary lesion (16). CrDchange of CD4/ LPLs. Furthermore, oligoclonal expan-
sion was seen especially in the Vb12 T cells, but the is known to involve any part of gastrointestinal tract.In fact, even macroscopically uninvolved mucosa is char-dominant clones were not identical in the patients. The
predominance of particular Vbs demonstrated by semi- acterized by the evidence of granulomas and granuloma-tous vasculitis (2). Recent study has also demonstratedquantitative PCR were verified utilizing random cloning
method. To investigate the initial events which take the increased production of proinflammatory cytokinesby morphologically normal intestine from patients withplace at the disease onset should be quite important toCrD (17). Our result that normal-looking mucosa of CrDalso showed skewed Vb usage might reflect such indis-criminate insult. Nakajima et al. reported that severalT cell clones were present in both aphthoid lesions anddiscrete ulcer lesions (16). Probert et al. showed thatthe reiterative Vb sequences were persistently foundover time in CD4/ PBLs from CrD patients (18). Theseresults may imply that expansion of T cells in CrD ispersistent from its very early stage through the lateestablished disease. CrD is thought to be associated witha loss of tolerance to intestinal microflora (19). If so, Tcell activation could take place in any part of the intes-tine. Skip lesion, which is a characteristic feature ofCrD, might be shaped through subsequent expressionof adhesion molecules, production of proinflammatorycytokines and impaired circulation. Therefore it mightbe conceivable that skewed Vb usage could be found allover the intestine. Posnett et al., using the restrictionFIG. 3. The Vb usage analyzed by semiquantitative PCR wasfragment length polymorphism method, reported thatcompared to the result of random cloning in (A) CrD patient 12 and
(B) normal control 17. j, PCR analysis; h, random cloning method. Vb8 T cells were concentrated in the mesenteric lymph
549
AID BBRC 7691 / 693f$$$$81 10-30-97 22:35:42 bbrcg AP: BBRC
Vol. 240, No. 3, 1997 BIOCHEMICAL AND BIOPHYSICAL RESEARCH COMMUNICATIONS
TABLE 3
Sequence Analysis of TCR Vb2, 12, and 13 in CrD Patients
Donor V N J n
10Vb1 CSA RTTSA SPLHFGNG J b1.6 2/28
CSA SANMGGF NTGELFFGEG J b2.2 2/28Vb12 CA TGTGDN NQPQHFGDG J b1.5 5/29
CASS YAGV GNTMYFGEG J b1.3 3/29CA ISASGQG EKLFFGSG J b1.4 2/29
All were different clonesVb13 1/16
12Vb2 CSA RISGRNQ YEQYFGPG J b2.7 2/29Vb12 CASS EYTSGIG NEQFFGPG J b2.1 7/29
CA ISDGGSGY YGYTFGSG J b1.2 2/29CAS ISTLGTGN YEQYFGPG J b2.7 2/29
Vb13 CASS PGQ SYEQYFGPG J b2.7 2/20
Note. Amino acid sequences are shown in single-letter code. n, proportion of isolates with this sequence.
nodes and PBLs while LPLs and IELs showed no enrich- antigen specificity. In fact, Vb12 and 13 T cells can bestimulated by some staphylococcal enterotoxins (23).ment of Vb8 T cells in CrD (20). Gulwani-Akolkar et
al. demonstrated that although the pattern of Vbs that Once activated, those cells with specificity for some an-tigens associated with intestine could then initiateincreased in active lesion relative to normal area was
different for all CrD patients examined, Vb11, 13S2, 15, bowel inflammation. Previous studies have demon-strated that IELs as well as LPLs were oligoclonal inand 17 increased uniformly in the active lesions of all
individuals (21). Another study revealed that mucosal normal individuals (13, 24). Such innate T cell popula-tion is supposed to be conserved even after stimulatedT cell clones derived from the earliest visible lesion in
CrD patients were predominantly Vb1, 2, 5.1, 5.2, 6, 7, by superantigen. Recent studies have implicated super-antigens in the pathogenesis of autoimmune diseases,and 8 (22). In our study, the increase of Vb12 and 13
was almost uniformly observed whether or not the sam- including rheumatoid arthritis (9) and Kawasaki’s dis-ease (25). Bacterial superantigen was also shown topling site was involved, however, there were some differ-
ences in the pattern of Vb usage between affected lesion induce clinical relapses of murine experimental auto-immune encephalomyelitis (26). Aisenberg et al. re-and normal-looking area in each patient (Table 1), which
was consistent with their results. Certain increase of ported that intestinal mucosal cell is capable of mediat-ing superantigen-driven immune response (27). The se-Vb2, 7, 8 and 17 was seen also in our study, but the
increase of Vb12 and 13 was much more striking. We lective expansion of Vb12 and 13 T cells in almost allof the CrD patients, despite different HLA expression,do not know exactly what caused the differences of the
results of Vb analysis. One possible explanation is the may support the hypothesis that superantigen mightplay an important role in the pathogenesis or relapsedifference of treatment. Immunosuppressant treat-
ments used in almost all cases of CrD may change T of CrD. This change is specific for CrD because neitherUC nor normal control exhibited such skewing. In addi-cell repertoire. In fact, previous study was reported that
several predominant T cell clones were decreased by tion to the remarkable skewing toward Vb12 and 13,the expansion of certain T cell clones (5/29 with Vb12/steroid. All patients in our study had been treated with
nutritional therapy such as elemental diet (ED) or total Jb1.5 in patient 10, 7/29 with Vb12/Jb2.1 in patient12) was also notable. Although superantigen may stim-parenteral nutrition (TPN) without any medications. In
Japan, ED therapy is the first choice for CrD. Even ulate any clones with specific Vb expression, predispo-sition such as environmental and genetic backgroundpatients with bowel obstruction are primarily treated
with TPN, and in fact surgical resection can be avoided could possibly select a particular clone, which wouldelicit pathogenic potential.in considerable cases. Ethnic difference should also be
taken into account. In summary, the mucosal lymphocytes from CrD pa-tients preferentially used Vb12 and Vb13. Such skew-The nature of antigens driving T cell responses in
CrD remains poorly defined. Our result that T cells ing was specific for CrD, and was seen in both affectedand macroscopically normal areas. The predominancewith particular Vbs expanded in any patients would
lead to the speculation that CrD is superantigen- of Vb12 and Vb13 T cells in the whole mucosal tissuewas considered to represent the change of CD4/ LPLs.driven. Superantigen is capable of stimulating T cells
on the basis of their Vb chain and independently of the Furthermore, striking clonal expansion was seen espe-
550
AID BBRC 7691 / 693f$$$$81 10-30-97 22:35:42 bbrcg AP: BBRC

Vol. 240, No. 3, 1997 BIOCHEMICAL AND BIOPHYSICAL RESEARCH COMMUNICATIONS
10. Sumida, T., Yonahara, F., Maeda, T., Tanabe, E., Koike, T., Tom-cially in the Vb12 T cells, but the dominant clones wereioka, H., and Yoshida, S. (1992) J. Clin. Invest. 89, 681–685.not identical in the patients. These observations
11. Kirsner, J. B., and Shorter, R. G. (1982) N. Engl. J. Med. 306,strongly suggest an important role for superantigen775–785.
along with genetic and environmental predisposition 12. Dombal, F. T., and Softley, A. (1987) Gut 28, 474–481.in the pathogenesis of CrD. 13. Chott, A., Probert, C. S., Gross, G. G., Blumberg, R. S., and Balk,
S. P. (1996) J. Immunol. 156, 3024–3035.14. Chomczynski, P., and Sacchi, N. (1987) Anal. Biochem. 162, 156–ACKNOWLEDGMENTS
159.15. Ikuta, K., Ogura, T., Shimizu, A., and Honjo, T. (1985) Proc.This work was supported by a Grant-in-Aid for Scientific Research
Natl. Acad. Sci. USA 88, 7701–7705.from the Japanese Ministry of Education, Science and Culture ofJapan. The authors thank Drs.Riichiro Nezu, Takushi Monden, and 16. Nakajima, A., Kodama, T., Yazaki, Y., Takazoe, M., Saito, N.,
Suzuki, R., Nishino, H., Yamamoto, K., Silver, J., and Matsu-Naohiro Tomita for surgical samples.hashi, N. (1996) J. Immunol. 157, 5683–5688.
17. Reimund, J-M., Wittersheim, C., Dumont, S., Muller, C. D., Ken-REFERENCES ney, J. S., Baumann, R., Poindron, P., and Duclos, B. (1996) Gut39, 684–689.
1. Burton, I. K., and Sommers, S. C. (1977) JAMA 237, 2742–2744. 18. Probert, C. S., Chott, A., Turner, J. R., Saubermann, L. J., Ste-2. Wakefield, A. J., Sankey, E. A., Dhillon, A. P., Sawyerr, A. M., vens, A. C., Bodinaku, K., Elson, C. O., Balk, S. P., and Blumb-
More, L., Sim, R., Pittilo, R. M., Rowles, P. M., Hudson, M., erg, R. S. (1996) J. Immunol. 157, 3183–3191.Lewis, A. A. M., and Pounder, R. E. (1991) Gastroenterology 100, 19. Pirzer, U., Schasanhaar, A., Fleischer, B., Hermann, E., and1279–1287. Meyer zum Buschenfelde, K. H. (1991) Lancet 338, 1238–1239.
3. Choy, M. Y., Walker-Smith, J. A., Williams, C. B., and MacDon- 20. Posnett, D. N., Schmelkin, I., Burton, D. A., August, A.,ald, T. T. (1990) Gut 31, 1365–1370. McGrath, H., and Mayer, L. F. (1990) J. Clin. Invest. 85, 1770–
4. Cuvelier, C. A., De Wever, N., Mielants, H., De Vos, M., Veys, 1776.E. M., and Roels, H. (1992) Clin. Exp. Immunol. 90, 275–279. 21. Gulwani-Akolkar, B., Akolkar, P. N., Minassian, A., Pergolizzi,
R., McKinley, M., Mullin, G., Fisher, S., and Silver, J. (1996) J.5. Brynskov, J., Freund, L., Rasmussen, S. N., Lauritsen, K., DeClin. Invest. 98, 1344–1354.Muckadell, O. S., Williams, N., MacDonald, A. S., Tanton, R.,
Molina, F., Campanini, M. C., Bianchi, P., Ranzi, T., De Palo, 22. Prindiville, T. P., Cantrell, M. C., Matsumoto, T., Brown, W. R.,F. Q., Malchow-Møller, A., Thomsen, O. Ø., Tage-Jensen, U., Ansari, A. A., Kotzin, B. L., and Gershwin, M. E. (1996) J. Auto-Binder, V., and Riis, P. (1989) N. Engl. J. Med. 321, 845–850. immunity 9, 193–204.
6. Stronkhorst, A. G., Tytgat, N. J., and Van Deventer, S. J. H. 23. Choi, Y., Kotzin, B., Herron, L., Callahan, J., Marrack, P., and(1992) Scand. J. Gastroenterol. 27, Suppl. 194:61–65. Kappler, J. (1989) Proc. Natl. Acad. Sci. USA 86, 8941–8949.
24. Blumberg, R. S., Yockey, C. E., Gross, G. G., Ebert, E. C., and7. James, S. P. (1988) Gastroenterology 95, 1667–1669.Balk, S. P. (1993) J. Immunol. 150, 5144–5153.8. Oksenberg, J. R., Panzara, M. A., Begovich, A. B., Mitchell, D.,
25. Donald, Y. M. L., Giorno, R. C., Kazemi, L. V., Flynn, P. A., andErlich, H. A., Murray, R. S. , Shimonkevitz, R., Sherritt, M.,Busse, J. B. (1995) J. Immunol. 155, 5018–5021.Rothbard, J., Bernard, C. C. A., and Steinman, L. (1993) Nature
362, 68–70. 26. Brocke, S,. Gaur, A., Piercy, C., Gautam, A., Gijbels, K., Fath-man, C. G., and Steinman, L. (1993) Nature 365, 642–644.9. Paliard, X., West, S. G., Lafferty, J. A., Clements, J. R., Kappler,
J. W., Marrack, P., and Kotzin, B. L. (1991) Science 253, 325– 27. Aisenberg, J., Ebert, E. C., and Mayer, L. (1993) Gastroenterol-ogy 105, 1421–1430.329.
551
AID BBRC 7691 / 693f$$$$81 10-30-97 22:35:42 bbrcg AP: BBRC