Embed Size (px)
Citation preview
1285
to the treatment of bleeding varices. Vasopressin raisesL.E.S.P. and is already used in the treatment of bleedingvarices. Metoclopramide and bethanechol, which are
used in the treatment of gastro-oesophageal reflux, alsoraise L.E.S.P.; so do gastrin, motilin, prostaglandin, andcoffee. IS Falls in L.E.S.P. occur after alcohol, cigarettesmoking, chocolates, fatty meals, benzodiazepines, mor-phine, -glucagon, cholecystokinin, and secretin. IS Theuse of agents which raise L.E.s.P. and the avoidance of
agents which lower L.E.s.P. may be valuable in the treat-ment of oesophageal varices.
FURTHER RESEARCH
Further oesophagographic, endoscopic, or portagraphic stu-dies of the relation between L.E.s.P. and oesophageal varicesare necessary. When varices are seen on conventional oesopha-gography their size should be reduced after the use ofL.E.S.P.-increasing agents. Fibreoptic endoscopy may be in-accurate because inflation of the lumen may reduce the size ofthe varices. Portagraphy seems to be the best technique. Con-trast material can be injected through a transhepatically intro-duced catheter placed in the portal vein, and oesophageal var-ices visualised. After a rise in L.E.S.P. the flow of contrastmaterial into the varices should be smaller or absent.
I thank Prof. H. Baden and Dr B. Andersen for their help.
Methods and Devices
UNIVERSITY COLLEGE HOSPITALMUSCLE-BIOPSY NEEDLE
ARCHIE YOUNG* C. M. WILESR. H. T. EDWARDS
Department of Human Metabolism, University CollegeHospital Medical School, London
INTEREST in needle biopsy of muscle for the diagnosis ofneuromuscular disorders has steadily increased since we de-scribed the technique in this journal.l 2 At the IVth Inter-national Congress on Neuromuscular Diseases we reported ourexperience of 490 such biopsies;3 in discussion it became
apparent that some workers had found difficulty using theneedle originally introduced by Bergstrom.4 We describe amodification which overcomes the main problem experiencedwith Bergstrom’s needle-i.e., the small size of the sample.This modified needle is very satisfactory in clinical practicewhen muscle samples are required for chemical analysis, histo-chemistry, and electron miscroscopy. 5The main part of the modified needle (see accompanying
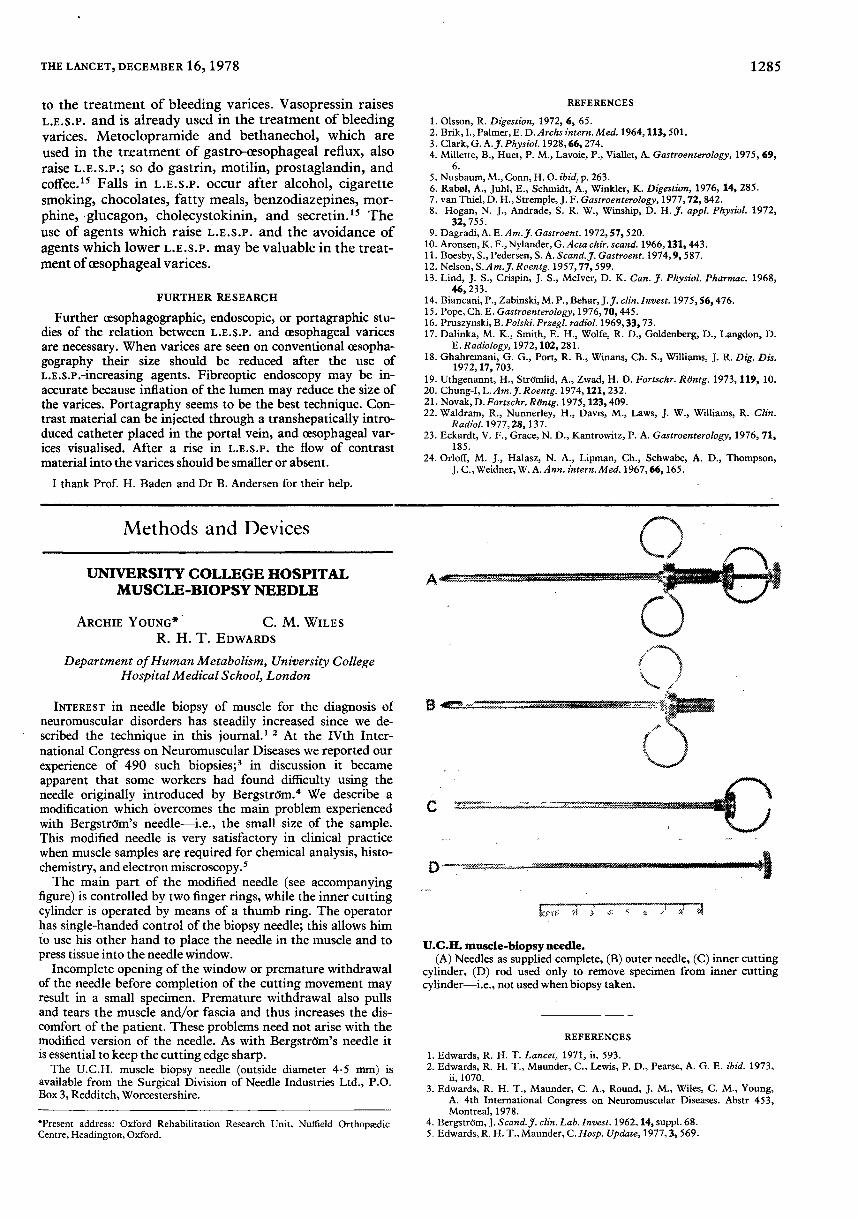
figure) is controlled by two finger rings, while the inner cuttingcylinder is operated by means of a thumb ring. The operatorhas single-handed control of the biopsy needle; this allows himto use his other hand to place the needle in the muscle and topress tissue into the needle window.
Incomplete opening of the window or premature withdrawalof the needle before completion of the cutting movement mayresult in a small specimen. Premature withdrawal also pullsand tears the muscle and/or fascia and thus increases the dis-comfort of the patient. These problems need not arise with themodified version of the needle. As with Bergstrom’s needle itis essential to keep the cutting edge sharp.The U.C.H. muscle biopsy needle (outside diameter 4.5 mm) is
available from the Surgical Division of Needle Industries Ltd., P.O.Box 3, Redditch, Worcestershire.
*Present address: Oxford Rehabilitation Research Unit, Nuffield OrthopædicCentre, Headington, Oxford.
REFERENCES
1. Olsson, R. Digestion, 1972, 6, 65.2. Brik, I., Palmer, E. D. Archs intern. Med. 1964, 113, 501.3. Clark, G. A.J. Physiol. 1928, 66, 274.4. Millette, B., Huet, P. M., Lavoie, P., Viallet, A. Gastroenterology, 1975, 69,
6.5. Nusbaum, M., Conn, H. O. ibid. p. 263.6. Rabøl, A., Juhl, E., Schmidt, A., Winkler, K. Digestion, 1976, 14, 285.7. van Thiel, D. H., Stremple, J. F. Gastroenterology, 1977, 72, 842.8. Hogan, N. J., Andrade, S. R. W., Winship, D. H. J. appl. Physiol. 1972,
32, 755.9. Dagradi, A. E. Am. J. Gastroent. 1972, 57, 520.
10. Aronsen, K. F., Nylander, G. Acta chir. scand. 1966, 131, 443.11. Boesby, S., Pedersen, S. A. Scand. J. Gastroent. 1974, 9, 587.12. Nelson, S. Am. J. Roentg. 1957, 77, 599.13. Lind, J. S., Crispin, J. S., Mclver, D. K. Can. J. Physiol. Pharmac. 1968,
46, 233.14. Biancani, P., Zabinski, M. P., Behar, J. J. clin. Invest. 1975, 56, 476.15. Pope, Ch. E. Gastroenterology, 1976, 70, 445.16. Pruszynski, B. Polski. Przegl. radiol. 1969, 33, 73.17. Dalinka, M. K., Smith, E. H., Wolfe, R. D., Goldenberg, D., Langdon, D.
E. Radiology, 1972, 102, 281.18. Ghahremani, G. G., Port, R. B., Winans, Ch. S., Williams, J. R. Dig. Dis.
1972, 17, 703.19. Uthgenannt, H., Strömlid, A., Zwad, H. D. Fortschr. Röntg. 1973, 119, 10.20. Chung-I, L. Am. J. Roentg. 1974, 121, 232.21. Novak, D. Fortschr. Röntg. 1975, 123, 409.22. Waldram, R., Nunnerley, H., Davis, M., Laws, J. W., Williams, R. Clin.
Radiol. 1977, 28, 137.23. Eckardt, V. F., Grace, N. D., Kantrowitz, P. A. Gastroenterology, 1976, 71,
185.24. Orloff, M. J., Halasz, N. A., Lipman, Ch., Schwabe, A. D., Thompson,
J. C., Weidner, W. A. Ann. intern. Med. 1967, 66, 165.
U.C.H. muscle-biopsy needle.(A) Needles as supplied complete, (B) outer needle, (C) inner cutting
cylinder, (D) rod used only to remove specimen from inner cuttingcylinder-i.e., not used when biopsy taken.
REFERENCES
1. Edwards, R. H. T. Lancet, 1971, ii, 593.2. Edwards, R. H. T., Maunder, C., Lewis, P. D., Pearse, A. G. E. ibid. 1973,
ii, 1070.3. Edwards, R. H. T., Maunder, C. A., Round, J. M., Wiles, C. M., Young,
A. 4th International Congress on Neuromuscular Diseases. Abstr 453,Montreal, 1978.
4. Bergström, J. Scand. J. clin. Lab. Invest. 1962, 14, suppl. 68.5. Edwards, R. H. T., Maunder, C. Hosp. Update, 1977, 3, 569.





























