Embed Size (px)
Citation preview

High-dose immunosuppression to prevent death after paraquat self-poisoning - a randomised controlled trial
Indika Gawarammana,1,2,3 Nick A Buckley,2,3,4 Fahim Mohamed,2,3 Kamal Naser,5 K Jeganathan,6,7 PL
Ariyananada,8 Klintean Wunnapuk,9,10 Timothy A Dobbins,3,11 John A Tomenson,12 Martin F Wilks,13
Michael Eddleston,2,14 and Andrew H Dawson.2,3,4
1 Department of Medicine, Faculty of Medicine, University of Peradeniya, Sri Lanka
2 South Asian Clinical Toxicology Research Collaboration, Faculty of Medicine, University of
Peradeniya, Sri Lanka
3 Department of Pharmacology, University of Sydney, Sydney, Australia
4 Royal Prince Alfred Hospital, Sydney Australia
5Peradeniya, 6Anuradhapura, and 7 Rathnapura Hospitals, Sri Lanka.
8 Faculty of Medicine, University of Ruhuna, Sri Lanka
9Therapeutics Research Centre, School of Medicine, University of Queensland, Australia
10 Department of Forensic Medicine, Faculty of Medicine, Chiang Mai University, Thailand
11 National Drug and Alcohol Research Centre, Sydney, Australia
12 Causation Limited, Macclesfield, United Kingdom
13Swiss Centre for Applied Human Toxicology, University of Basel, Switzerland
14 Pharmacology, Toxicology & Therapeutics, University/BHF Centre for Cardiovascular Science,
University of Edinburgh and National Poisons Information Service - Edinburgh Unit, Royal Infirmary
of Edinburgh, UK
Correspondence: Nick Buckley
1

Abstract
Context Intentional self-poisoning with the herbicide paraquat has a very high case-fatality
and is a major problem in rural Asia and Pacific.
Objectives We aimed to determine whether the addition of immunosuppression to supportive
care offers benefit in resource poor Asian district hospitals.
Materials and Methods We performed a randomised placebo-controlled trial comparing
immunosuppression (intravenous cyclophosphamide up to 1g/day for two days and
methylprednisolone 1g/day for 3 days, and then oral dexamethasone 8mg three-times-a-day
for 14 days) with saline and placebo tablets, in addition to standard care, in patients with
acute paraquat self-poisoning admitted to six Sri Lankan hospitals between 1st March 2007
and 15th November 2010. The primary outcome was in hospital mortality.
Results 299 patients were randomised to receive immunosuppression (147) or saline/placebo
(152). There was no significant difference in in-hospital mortality rates between the groups
(immunosuppression 78 [53%] vs. placebo 94 [62%] (Chi squared test 2.4, p=0.12). There
was no difference in mortality at 3 months between and immunosuppression (101/147 [69%])
and placebo groups (108/152 [71%]); (Mortality reduction 2%, 95% CI: -8 to +12%). A Cox
model did not support benefit from high-dose immunosuppression but suggested potential
benefit from the subsequent two weeks of dexamethasone.
Conclusions We found no evidence that high dose immunosuppression improves survival in
paraquat-poisoned patients. The continuing high mortality means further research on the use
of dexamethasone and other potential treatments is urgently needed.
Trial registration: ISRCTN85372848.Abstract word count: 231Key words: Paraquat, Acute self-poisoning, immunosuppression, randomised controlled trial
2

Introduction
Deaths from pesticide self-poisoning is a major clinical and public health problem in rural
Asia (1-3). The herbicide paraquat is a leading cause of death (4) from pesticide self-
poisoning (3-8). In a prospective observational cohort of 9300 patients with pesticide self-
poisoning, paraquat had a case fatality of 42% and accounting for 25% of pesticide poisoning
deaths (4).
Ingestion of paraquat results in rapid multi-organ failure or more drawn out lethal pulmonary
fibrosis. Paraquat’s very high case-fatality is due both to its inherent toxicity and the lack of
any effective treatment. There are no widely accepted guidelines on treatment of patients with
paraquat self-poisoning; treatment regimens vary from supportive care alone to combinations
of immunomodulation, anti-oxidant therapy, haemoperfusion and haemodialysis (9).
Since paraquat leads to an acute inflammatory response (9), immunosuppression with
cyclophosphamide, methylprednisolone and dexamethasone has become a frequent method of
treatment for paraquat self-poisoning. The regimen was first suggested in 1986 in a report of
an uncontrolled study (10). A series of small clinical studies using immunosuppression
reported a marked improvement in survival (11-13). However, a systematic review found
insufficient evidence from high quality randomised controlled trials (RCT) to recommend its
use (14). We established an RCT in 2007 to determine the effectiveness of
immunosuppression versus placebo in preventing deaths from paraquat self-poisoning.
Materials and Methods
The RCT (ISRCTN85372848) was conducted in six Sri Lankan district hospital sites. Ethics
approval was received from the Ethics committees of Peradeniya, Colombo and Ruhuna
3

Faculties of Medicine, Sri Lanka, and the Australian National University. Written informed
consent was taken from each patient in their own language.
Participants
We approached all patients aged 14 years and over with paraquat pesticide self-poisoning
admitted to adult wards with systemic exposure to paraquat as indicated by a positive urine
dithionite test, a marker of poor prognosis (15). Patients were initially approached if they
presented within 24 h of ingestion; following consultation with the DMEC in May 2009, all
patients who presented within 48 h of ingestion were approached to improve recruitment.
None of the patients received other specific treatments such as haemodialysis or
haemoperfusion.
Exclusion criteria included: age <14 years, known pregnancy, and known allergy to, or prior
therapy with, trial medication. In addition, patients with a systolic blood pressure less than
70mmHg that did not respond to 1L of intravenous fluid or a Glasgow Coma score less than
8/15 were excluded; these criteria were intended to exclude severely poisoned patients who
were expected to die imminently without any chance of responding to therapy.
Outcomes, objectives and hypotheses
The primary aim was to determine whether, in addition to standard care (intravenous fluid,
activated charcoal and pain relief), high dose immunosuppression with cyclophosphamide,
methylprednisolone and dexamethasone reduced in-hospital death from all causes in paraquat
self-poisoning compared with no immunosuppression. Secondary outcomes were all-cause
mortality at three months post-ingestion and lung function in survivors at 3 months.
4

At trial registration, we specified in-hospital deaths as the primary outcome. As people may
die over 1-2 months after discharge (16) we planned a secondary outcome of 3 month
survival. The other pre-specified secondary outcome of lung function [formal lung functions
and a High Resolution CT scan (HRCT) to be performed in tertiary referral hospitals at long-
term follow-up] did not prove possible to obtain from a meaningful number of patients.
Randomisation
Randomisation was done using purpose-designed computer software. The random sequence
and allocation were concealed prior to randomisation. The program randomised eligible
patients in a 1:1 ratio to the placebo and immunosuppression arms (without block-allocation).
The allocation sequences were generated and encrypted independently by an IT consultant
who had no role in patient recruitment, treatment and assessment.
The randomisation was performed by study pharmacists at a central location in each hospital.
Upon recruiting a patient, the pharmacist was provided with the name, hospital number and
weight of the patient. The pharmacist randomised the patient and subsequently prepared
treatment packs. The allocation was only known to the pharmacists who had no other role in
patient management and data collection. The other members of the team could neither predict
allocation nor alter randomisation.
Intervention
Patients randomised to the intervention arm were treated as described in supplemental Box 1
(Treatment Protocol). We visited patients 3 months after discharge to record if they were still
alive or dead. Deaths were confirmed by observation of death certificates issued by the
5

registrar of deaths. Survivors were interviewed to see if they were engaged in their daily
routines and basic cardiovascular and respiratory clinical examinations were performed.
Blood and urine sampling
A urine sample and a 10 mL blood sample were obtained on admission after clinical
stabilisation. A dithionite test was immediately performed on the admission urine sample
(17). Five ml of blood was sampled at 8 hourly intervals up to 3 days and daily thereafter
until death or discharge from hospital. These blood samples were used to measure plasma
paraquat (as described elsewhere (18)), creatinine, liver enzymes and full blood count. The
treating physicians performed daily blood sugars using venous blood.
Sample size
In the second Taiwanese study, overall survival in the control group was 18% (12/65)
compared with 32% (18/56) in the treatment arm (11). An absolute increase in survival of
10%, to 28%, would be clinically important. In order to be able to detect whether either
regimen increases survival from 18% to 28%, with a significance level (alpha) of 5% and a
power of 80%, a minimum of 295 patients must be recruited to each arm of the trial (i.e., 590
patients in total). (See Supplementary Table 1 in the online data supplement)
Independent Data Monitoring & Ethics Committee
An independent Data Monitoring and Ethics Committee (DMEC) was established. The
DMEC met each year and reviewed data supplied by the trial statistician applying the
O'Brien-Fleming stopping rule (which has minimal effect on the power of the final analysis).
In the light of interim data, and emerging evidence from other studies, the DMEC was tasked
with advising the trial investigators to terminate the study if a treatment effect was clearly
6

demonstrated, or if continuation would be detrimental to future enrolled patients’ health, or it
was evident that no clear outcome would be obtained. The DMEC was also consulted when a
paraquat import ban resulted in a collapse in recruitment, endorsed the decision to terminate
the trial and reviewed the final manuscript.
Statistical analysis
All analyses were conducted using Stata Version 13. We compared demographic factors and
clinical characteristics between treatment groups to assess randomisation.
The primary analysis was conducted using an unadjusted chi-squared test to compare in-
hospital death between placebo and immunosuppression groups. We also did an intention to
treat analysis of 3 month survival (for this analysis we assumed that the 6 patients discharged
alive and lost to follow up survived.) We use and present this superior outcome in all
subsequent analyses; but conducted a sensitivity analysis restricted to in-hospital deaths
whenever statistical tests were applied.
The best estimates of prognosis come from a timed plasma paraquat concentration on
admission plotted on the Proudfoot nomogram (19) or converted to the Severity Index of
Paraquat Poisoning (SIPP = plasma paraquat concentration in mg/L multiplied by time in
hours since ingestion) score(20), the dose ingested and the serum creatinine (9). Eight values
of zero for SIPP were replaced with 0.05 (half the lowest measured value). The two
prediction methods are equally accurate but SIPP score has an advantage over the Proudfoot
(and other) nomograms as it can be applied to any timed sample (21). A SIPP could not be
calculated for 47 patients mostly due to a sample not having been analysed for paraquat. We
carried out adjusted regression analyses to assess whether controlling for age, gender, volume
7

of ingestion, or SIPP score altered the estimate of treatment effect. We used Cox proportional
hazards for survival time.
Post-hoc analysis
Lin et al in a post hoc analysis of patients who survived for 7 days and reported a
significantly lower case fatality of 18.2% (2/22) in the immunosuppression group compared
with 57% (16/28) case fatality in the control group (11). We performed the same analysis of
case fatality of patients who survive 7 days or longer.
Results
Patients were enrolled from 1st March 2007 until 15th November 2010. As a result of
regulatory decisions, the use of paraquat was phased out from Sri Lankan agricultural
practice through 2008 and 2009 and finally banned in August 2010. The trial was stopped in
November 2010 after consultation with the DMEC due to a collapse in recruitment.
Participants
604 patients with paraquat poisoning were assessed on admission; 305 patients were excluded
from the trial [negative urine test (149), refused consent (42), died before randomisation (46),
late admission (>48h post ingestion) (39), GCS< 8 (2), pregnancy (3), age less than 14 (3),
other reasons (21)]. 299 urine positive patients were eligible, consented, and randomised into
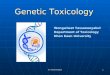
the trial: 152 received placebo and 147 received immunosuppression (Figure 1).
Baseline characteristics
Baseline demographic and clinical characteristics are presented in Table 1, and dose ingested
in Supplementary Figure 1. Admission plasma paraquat concentrations were available in 127
8

(84%) of the placebo group and 125 (85%) of the immunosuppression group. The
immunosuppression group had a slightly higher median paraquat concentration and SIPP
score but there were no other substantial differences.
Primary outcome - mortality
In-hospital mortality was 172/299 (58%). There was no significant difference in in-hospital
mortality between the placebo (61.8%) and immunosuppression (53.1%) groups (mortality
reduction 8.8%, 95% CI -2.4% to 20.0%, p=0.1). There was also no evidence of a difference
in case fatality at three months post ingestion between patients in placebo (71.1%) and
immunosuppression (68.7%) groups (mortality reduction 2.3%, 95% CI: -8.1% to 12.7%,
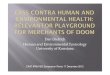
p=0.7). The paraquat concentrations of survivors and non-survivors from both groups plotted
against two risk prediction nomograms in Figure 2, indicate that death was predictable from
exposure in most individuals, with few individuals below the lines dying and few above
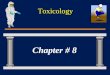
surviving, and no obvious difference with treatment. On an intention to treat basis, there was
no evidence of a difference in survival between the two groups (Figure 3, log rank p=0.6).
We were able to follow up all but 6 patients post discharge. HRCT and lung function became
available during the second year in one centre and the third year in another centre. However,
patients were unwilling to travel long distances for HRCT and formal lung functions, mostly
because for many this opportunity came 1-2 years after their poisoning. These outcomes were
only obtained on 17 patients (<20%), were mostly normal, and provide no insight into
treatment effectiveness.
9

Pre-specified multivariable analysis:
The Cox proportional hazards model suggests a small, albeit non-statistically-significant,
beneficial effect from immunosuppression (adjusted HR for death 0.74 (95%CI: 0.54 to 1.01)
– Table 2). Looking at this more closely, introducing a time dependent treatment effect into
the model showed that the favourable effect was not observed during the high-dose
immunosuppression but was restricted to the time of the dexamethasone administration
(Table 2), (See Supplementary Table 2 in the online data supplement).
Post-hoc analysis of patients surviving 7 days or longer
We compared the case fatality of the 124 patients who survived 7 days or longer. Death
occurred in 17/59 (28%) patients in the placebo group and 22/65 (34%) in the
immunosuppression group (mortality increase 5%, 95% CI: -11% to +21%).
Adverse events
Each patient was assessed twice daily for two specific adverse effects (haematuria, bladder
pain) attributable to cyclophosphamide, but these were not observed.
Discussion
This trial, the largest RCT in paraquat poisoning to date, showed no benefit of high dose
immunosuppression with cyclophosphamide, methylprednisolone and dexamethasone in
acute self-poisoning with paraquat. Previous reports have claimed large benefits from
immunosuppression but not provided convincing evidence (22). The original report claimed
improved survival on the basis that 6 of the 18 patients who had plasma paraquat
concentrations over 2mg/L survived and that the mortality in this group should be 100% (10).
This was followed by a negative observational study (23), and more recently by a series of
10

very small RCTs (11-13;24). The trials have all been unregistered and no power calculations
would have supported trials this small. Hence, it seems likely that most or all of these studies
were prematurely stopped based on unplanned interim analyses with no adjustment to the
statistical plan to avoid inflated type I error. A forest plot of the various RCTs shows a very
strong inverse relationship between study and effect size (Supplementary Figure 3),
suggesting there may also be publication bias and that any pooled analysis suggesting a larger
overall benefit should be interpreted cautiously. We believe our trial (which has more than
half the total randomised patients) provides a more accurate estimate of the likely treatment
effect. In the next largest RCT, on intention to treat analysis 12/65 control patients and 18/56
patients receiving immunosuppression survived (P=0.09). The authors presented a post-hoc
analysis in which only patients who survived the first week after randomisation were
compared and claimed they had demonstrated benefit from immunosuppression in this sub-
group. Their study reported deaths (in those surviving more than a week) in 4/28 patients
with immunosuppression compared with 16/28 controls. Our post hoc analysis of more than
twice this number does not provide any evidence that supports survival benefit from
immunosuppression in this sub group. This illustrates (if any further illustrations are needed)
the pitfalls of conclusions based on post-hoc sub-group comparisons in clinical trials.
Despite that caveat, our own secondary analysis does suggest a potentially important
favourable effect of the two week dexamethasone course that followed the high dose
immunosuppression (Table 2B, Supplementary Figure 2). There is also a separation of the
survival curves between the 5th and the 14th day. From around that time onwards, the survival
curves come back together (Figure 3). Dexamethasone was the only active treatment during
this time and was stopped on the 17th day. While this effect was non-significant on the
intention to treat analysis, was not sustained after treatment stopped, and also quite modest,
11

any future studies using steroids should consider continuing this treatment for the 5 to 6 week
period in which deaths occur. It is possible, although less likely that this time course reflected
a delayed response to immunosuppression. However, in contrast to high-dose
immunosuppression dexamethasone is inexpensive, of low toxicity and easily administered.
A large nation-wide study of 1811 patients from Taiwan concluded that patients receiving
immunosuppression had modestly better outcomes (29% vs 24% survival). Intriguingly, the
only immunosuppressive regimens demonstrating improved outcomes were the 4 out of 7
which contained dexamethasone (25). Further, animal studies have shown dexamethasone
may be effective, and also that it has two mechanisms of action. As well as an anti-
inflammatory effect, it induces P-glycoprotein which may increase efflux of paraquat from
pulmonary tissue (26).
In contrast, a recent review of pathophysiological mechanisms in paraquat poisoning found
neither animal models nor plausible pathophysiological explanation for why high dose
immunosuppression would be effective in paraquat poisoning in humans(9). Paraquat rapidly
generates reactive oxygen species which causes cellular damage via lipid peroxidation,
activation of nuclear factor kappa B, mitochondrial damage and apoptosis in many organs.
This leads to rapid deterioration of renal and liver function and development of acute
alveolitis. Cyclophosphamide and methylprednisolone have not been shown to have
beneficial effects in scavenging free radicals during the acute stage. Nor were these
treatments alone (without dexamethasone) associated with better outcomes in the large
nationwide study from Taiwan (25).
Limitations
12

The most important limitation of our study was that, while it is much larger than the
preceding trials, we were unable to recruit the planned number of patients into the study as
the sale of paraquat was banned in Sri Lanka. However, as the difference in case fatality with
298 patients is minimal, it seems unlikely that continuation of the trial would have led to a
trial result that supported immunosuppression improving overall survival (the primary
outcome).. To achieve a 9% difference in survival with statistical significance, the survival in
the immunosuppression arm would need to increase to 50% in the remaining 150 patients
with the placebo group continuing at the current survival of 29%. This is a 19% increase in
survival from the current level of 31%. This is extremely unlikely to occur. Other limitations
largely relate to the resource poor setting of rural Asian hospitals; typical of paraquat
poisoning but not clinical trials. In a Western country such severely ill patients would be in
intensive care; in rural Asia they are on crowded open wards with few staff. There was very
limited laboratory testing and infrequent clinical monitoring of many patients. Thus we
cannot report on any disease modifying effects of treatment (e.g. less or more kidney failure)
that did not affect mortality, although such information would not alter our overall
conclusions. Further, we did not exclude patients based on pre-existing medical conditions,
however, there were very few in this predominately young healthy population and none that
were regarded as having directly contributed to death.
Conclusions
Intentional self-poisoning with paraquat continues to kill many people throughout rural Asia.
We have little evidence that supports any active medical treatment. Clinical trials to identify
more effective therapy are urgently needed in places where paraquat has not been banned.
Our study and observational studies suggest any possible benefit is due to the dexamethasone
component rather than high-dose immunosuppression. We believe clinical research efforts
13

would be best spent on exploring the optimal dose of dexamethasone and other inexpensive
and low toxicity antidotes with favourable effects in animal studies (for example
acetylcysteine) (9, 27).
14

Reference List
(1) Jeyaratnam J. Acute pesticide poisoning: a major global health problem. World
Health Stat Q 1990;43:139-44.
(2) Eddleston M, Phillips MR. Self poisoning with pesticides. Br Med J 2004 January
3;328(7430):42-4.
(3) Gunnell D, Eddleston M, Phillips MR, et al: The global distribution of fatal pesticide
self-poisoning: systematic review. BMC Public Health 2007 December 21;7:357.
(4) Dawson AH, Eddleston M, Senarathna L, et al: Acute human lethal toxicity of
agricultural pesticides: a prospective cohort study. PLoS Med 2010 October
26;7(10):e1000357.
(5) Patel V, Ramasundarahettige C, Vijayakumar L, G et al: Suicide mortality in India: a
nationally representative survey. Lancet 2012 June 3;379(9834):2343-51.
(6) Eddleston M. Patterns and problems of deliberate self-poisoning in the developing
world. QJM 2000 November;93(11):715-31.
(7) Yin Y, Guo X, Zhang SL, et al: Analysis of paraquat intoxication epidemic (2002-
2011) within China. Biomed Environ Sci 2013 June;26(6):509-12.
(8) Chang SS, Lu TH, Eddleston M, et al: Factors associated with the decline in suicide
by pesticide poisoning in Taiwan: a time trend analysis, 1987-2010. Clin Toxicol
(Phila) 2012 July;50(6):471-80.
(9) Gawarammana IB, Buckley NA. Medical management of paraquat ingestion. Br J
Clin Pharmacol 2011 November;72(5):745-57.
15

(10) Addo E, Poon-King T. Leucocyte suppression in treatment of 72 patients with
paraquat poisoning. Lancet 1986 May 17;1(8490):1117-20.
(11) Lin JL, Leu ML, Liu YC, et al: A prospective clinical trial of pulse therapy with
glucocorticoid and cyclophosphamide in moderate to severe paraquat-poisoned
patients. Am J Respir Crit Care Med 1999 February;159(2):357-60.
(12) Lin JL, Wei MC, Liu YC. Pulse therapy with cyclophosphamide and
methylprednisolone in patients with moderate to severe paraquat poisoning: a
preliminary report. Thorax 1996 July;51(7):661-3.
(13) Lin JL, Lin-Tan DT, Chen KH, et al: Repeated pulse of methylprednisolone and
cyclophosphamide with continuous dexamethasone therapy for patients with severe
paraquat poisoning. Crit Care Med 2006 February;34(2):368-73.
(14) Eddleston M, Wilks MF, Buckley NA. Prospects for treatment of paraquat-induced
lung fibrosis with immunosuppressive drugs and the need for better prediction of
outcome: a systematic review. QJM 2003 November;96(11):809-24.
(15) Scherrmann JM, Houze P, Bismuth C, et al: Prognostic value of plasma and urine
paraquat concentration. Hum Toxicol 1987 January;6(1):91-3.
(16) Wilks MF, Fernando R, Ariyananda PL, et al: Improvement in survival after paraquat
ingestion following introduction of a new formulation in Sri Lanka. PLoS Med 2008
February;5(2):e49.
(17) Knepil J. Measurement of plasma-paraquat concentration. Lancet 1979 September
29;2(8144):699.
16

(18) Wunnapuk K, Medley GA, Liu X, et al: Simple and sensitive liquid chromatography-
tandem mass spectrometry methods for quantification of paraquat in plasma and
urine: application to experimental and clinical toxicological studies. J Chromatogr B
Analyt Technol Biomed Life Sci 2011 October 15;879(28):3047-52.
(19) Proudfoot AT, Stewart MS, Levitt T, et al: Paraquat poisoning: significance of
plasma-paraquat concentrations. Lancet 1979 August 18;2(8138):330-2.
(20) Sawada Y, Yamamoto I, Hirokane T, et al: Severity index of paraquat poisoning.
Lancet 1988 June 11;1(8598):1333.
(21) Senarathna L, Eddleston M, Wilks MF, et al: Prediction of outcome after paraquat
poisoning by measurement of the plasma paraquat concentration. QJM 2009
April;102(4):251-9.
(22) Li LR, Sydenham E, Chaudhary B, et al: Glucocorticoid with cyclophosphamide for
paraquat-induced lung fibrosis. Cochrane Database Syst Rev 2014 August
7;8:CD008084. doi: 10.1002/14651858.CD008084.pub4.:CD008084.
(23) Perriens JH, Benimadho S, Kiauw IL, et al: High-dose cyclophosphamide and
dexamethasone in paraquat poisoning: a prospective study. Hum Exp Toxicol 1992
March;11(2):129-34.
(24) Ghorbani A, Masoumi K, Forouzan A, et al: Effect of pulse therapy with
glucocorticoids and cyclophosphamide in patients with paraquat poisoning . Hong
Kong Journal of Emergency Medicine 22[4], 235-240. 2015. 1-7-2015.
(25) Wu WP, Lai MN, Lin CH, et al: Addition of immunosuppressive treatment to
hemoperfusion is associated with improved survival after paraquat poisoning: a
nationwide study. PLoS ONE 2014 January 27;9(1):e87568.
17

(26) Dinis-Oliveira RJ, Duarte JA, Remiao F, et al: Single high dose dexamethasone
treatment decreases the pathological score and increases the survival rate of paraquat-
intoxicated rats. Toxicology 2006 October 3;227(1-2):73-85.
(27) Yeh ST, Guo HR, Su YS, Lin HJ et al: Protective effects of N-acetylcysteine treatment
post-acute paraquat intoxication in rats and in human lung epithelial cells.
Toxicology. 2006 Jun 15;223(3):181-90.
18

Table 1: Baseline demographics, clinical parameters, and prognostic markers
Baseline characteristics Placebo group
(n=152)
Immunosuppression
group
(n=147)
Age – median (IQR) 27 (21 to 36) 27 (21 to 38)
Male – n (%) 113 (74%) 100 (68%)
Hours since ingestion (N=150, 144) – median (IQR) 6.0 (4.0 to 11.0) 6.6 (4.5 to 11.9)
Systolic blood pressure (mmHg, N=152, 143) – mean (SD) 119 (17) 117 (19)
Diastolic blood pressure (mmHg, N=152, 141) – mean (SD) 77 (10) 77 (10)
Pulse rate (per minute, N=152, 143)) – mean (SD) 82 (13) 83 (11)
Respiratory rate (per minute, N=150, 139) – median (IQR) 20 (20 to 26) 22 (20 to 28)
Creatinine (mg/dL, N=92, 88) 1.6 (0.9 to 2.5) 1.4 (0.9 to 2.8)
Paraquat concentration (mg/L, N=127, 125) – median (IQR) 1.7 (0.5 to 9.2) 2.6 (0.3 to 8.5)
Paraquat concentration above Proudfoot line (N = 93, 103) – n (%) 71 (76%) 76 (73%)
SIPP score (N=127, 125) – median (IQR) 13.1 (3.1 to 58.4) 18.4 (2.7 to 56.2)
19

Table 2: Cox model of hazard of death (n=252) without including time dependent
treatment effects (†) and incorporating an analysis of treatment effect based on
the time in which high-dose immunosuppression (days 0-3), dexamethasone
(days 3-17) and no treatment (>day 17) were given (††).
Factor Hazard ratio (95% CI) PImmunosuppression (†) Age (per 10 years) Male Log 2 SIPP
0.74 (0.54, 1.01)1.14 (1.01, 1.28)0.83 (0.57, 1.21)1.75 (1.62, 1.89)
0.060.040.3<0.001
Immunosuppression (††) (0, 3) days (3, 17) days (17+ ) days
Age (per 10 years) Male Log 2 SIPP
0.91 (0.62, 1.32)0.45 (0.25, 0.81)0.85 (0.25, 2.91)
1.13 (1.01, 1.28)0.82 (0.56, 1.19)1.75 (1.62, 1.89)
0.60.0080.8
0.040.3<0.001
Footnote: In the 252 patients with a SIPP score- 82/125 in the immunosuppression group
and 91/127 in the control group died during the 3 month follow up period.
†The unadjusted Hazard ratio in this sub group (n=252) of 0.87 (95% CI: 0.64, 1.17) is
similar to the unadjusted HR in the total cohort (n=299) of 0.93 (0.71, 1.22).
†† The unadjusted HRs in this subgroup are similar to the unadjusted HRs in the total cohort
[0 to <=3 days HR 1.02 (0.70, 1.49) vs HR 1.05 (0.73, 1.52); >3 to <= 17 days: HR 0.53
(0.30, 0.94) vs HR 0.69 (0.44, 1.06); >17 days: HR 1.56 (0.46, 5.32) vs HR 2.15 (0.66,
6.99)].
20

Figure legends
Figure 1: CONSORT statement flow diagram of patient progress through the RCT.
Footnotes
** 3 patients died and one withdrew consent after randomisation but before allocated treatment was given.1 patient randomised to placebo was given immunosuppressive treatment.
## 3 patients died and one left against medical advice after randomisation but before allocated treatment was given.
*** 18 patients left hospital against medical advice after starting allocated treatment (median of 1.9 days (IQR 0.7 to 3.7, range 0.16 to 5.1)
*** 26 patients left hospital against medical advice after starting allocated treatment (median of 2.1 days (IQR 1.1 to 3.0, range 0.20 to 9.7)
Figure 2: Admission plasma paraquat concentrations plotted against Proudfoot (with Schermann’s extension) and SIPP score =10 lines [concentrations above these shown to be highly predictive of a fatal outcome].
Footnote: patients lost to follow up before 3 months but assumed to have survived shown with green highlight. Lines on Proudfoot nomogram appear curved due to log transformed y-axis.
Figure 3: Timing of deaths in the two study arms.
Footnote: Percentage of patients still alive shown. The clock has been started at randomisation and stops either at death or last follow up or 3 months. The days on which cyclophosphamide were given and dexamethasone are shown in light purple and orange respectively in the top panel. Censored patients (lost to follow up) are tagged.
21

Figure 1
22

Figure 2
23

Figure 3
24



![TOXICOLOGY CENTRE SELF-ASSESSMENT DOCUMENT Assessment_Report... · toxicopathology, inorganic biogeochemistry [later changed to analytical toxicology], and contaminant fate ... Toxicology](https://img.pdfslide.net/doc/110x75/5b42ffd97f8b9ab15f8b94bd/toxicology-centre-self-assessment-document-assessmentreport-toxicopathology.jpg)



















![[Toxicology] toxicology introduction](https://img.pdfslide.net/doc/110x75/55c46616bb61ebb3478b4643/toxicology-toxicology-introduction.jpg)

