Embed Size (px)
Citation preview

University of Groningen
Clinical studies with biological response modifiers in the treatment of solid tumorsButer, Jan
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:1994
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Buter, J. (1994). Clinical studies with biological response modifiers in the treatment of solid tumors.Groningen: s.n.
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 10-07-2020

1 Introduction
Biological therapy is referred to as the fourth modality in cancer treatment because it differs
conceptually from surgery, radiation and chemotherapy as it acts not only directly by
attacking the tumor cells but also by stimulating the immune system to mediate the regressionof cancer (1,2). Translating the expanding knowledge of the immune system into biological
therapies has been difficult because of the complexity of the immune system includingcytokines, growth factors, antibodies, oncogenes and their products, and the vast array of
effector and suppressor cells and their receptors. Furthermore, in patients with cancer
cytokines and cytokine receptors are often deregulated and cytokines produced by the tumormay contribute to the pathophysiology of cancer. Early biological treatments were performed
using crude preparations of immunostimulants mostly derived from bacterial products ortumor extracts with usually disappointing results (3). However, the development of recom-
binant DNA and hybridoma techniques has enabled the synthesis of purified proteins capable
of more selective interventions in the immune cascade (4). Since then, intensive research hasbeen devoted to define the therapeutic use of these proteins in the treatment of cancer. In this
review the current state of clinical application of the biological response modifiers Interleukin-2 (IL-2) and Interferon-α (IFN) in the treatment of solid tumors will be discussed.
2 Interleukin-2
The first observations of mitogenic factors in the supernatant of stimulated leucocytes datefrom 1963 (5) but it was not until more than 10 years later that a growth factor for bone
marrow derived T-cells was described by Morgan and coworkers (6). This T-cell growth
factor (TCGF) was renamed Interleukin-2 (IL-2) in 1979 after discovery of its pleiotropiceffects (7). IL-2 is a 15Kd glycoprotein produced by T-helper cells that plays a central role
in the immune response. The human IL-2 gene has been mapped to chromosome 4q (bands
26 to 28). It has been isolated, cloned and expressed inE. Coli (8). The IL-2 gene consistsof four exons separated by introns with strong similarity to the genes of interleukin-4 and the
growth factor granulocyte-macrophage-colony stimulating factor (9). Subsequent to itsproduction IL-2 undergoes a variety of different post-translational steps including cleavage
of a 20 amino acid signal peptide, the addition of a carbohydrate at position 3 (threonine) and
creation of a disulfide bond between cysteines located at positions 58 and 105. This bondguarantees the stability of the tertiary structure which is essential for its biological activity
(10). Although IL-2 is naturally sialylated and glycosylated, the carbohydrate component ap-pears to play no part in the activity of the peptide since non-glycosylated recombinant IL-2
is equally effective at stimulating T-cell proliferation as glycosylated IL-2 (11).
15

2.1 BiologyThe biological effects of IL-2 have been described in detail by Smith (12,13). IL-2 is
produced by T-helper cells upon activation by Interleukin-1 and an antigen. The regulationof IL-2 production is only partly understood. In many cells at least two signals are required
for induction that are mimicked by phorbol ester and calcium ionophore stimulation (14).Presumably this usually involves ligation of the T-cell receptor and co-signaling through a
second cytokine or a receptor pair (CD28-B7) (15,16). Biologic activities of IL-2 are mediated
through both direct interaction with specific receptors on T cells, B cells, natural killer (NK)cells, monocytes, macrophages, and oligodendrocytes and through secondary effects resulting
from the induction of a variety of cytokines.
2.1.1 IL-2 receptorThe IL-2 receptor consists of at least three transmembrane associated units, each with anexternal domain of approximately 215 amino acid residues: a 55kDα chain (IL-2Rα, Tac,
p55), a 70 to 75kDβ chain (IL-2Rß, p70), and a 64kDγ chain (IL-2Rγ, p64) that combinenoncovalently (17-20). Only NK-cells and possiblyγδ T cells constitutively express theβ-
chain (Kd of 10-9 mol/L) in the absence of antigenic stimulation, and these cells are therefore
the immediately IL-2 responsive cell population (21). The biological activity on unstimulatedNK cells is presumably due to interaction of the slow binding intermediate affinityβ/γ dimer
that rapidly leads to upregulation of the fast bindingα chain ( Kd of 10-8 mol/L) to create ahigh-affinity α/β/γ heterotrimer with a Kd of 10-12 mol/L. Interaction of IL-2 with the high-
affinity receptor results in internalization through receptor-mediated endocytosis. The 75 kD
β chain, with the largest cytoplasmic domain of 286 amino residues, and theγ chain areprobably responsible for triggering intracellular biochemical pathways (22). Signal transduc-
tion after receptor binding remains obscure. The IL-2 receptor itself has no known enzymaticactivity. Upon IL-2 interaction with its receptors a variety of intracellular events occur.
Hydrolysis of inositol phosphates and increases in intracellular calcium are coupled with
activation of calcineurin, a calcium/calmodulin-responsive protein phosphatase, activation oftyrosine kinase and ultimately induction of transcriptional regulatory molecules. NK-506 and
cyclosporine appear to block these early events (23).
2.1.2 Soluble IL-2 receptorSoluble forms of the IL-2Rα chain have been identified in the serum of patients withmalignant, autoimmune and allergic disorders, systemic parasitic infections and in patients
undergoing graft versus host disease. Theα chain is thought to be released from the cell-membrane of activated T cells by proteolytic cleavage. The presence of the soluble IL-2Rαis therefore thought to reflect the state of T cell activation in these patients (24). Soluble IL-
2Rα has been found to be increased during IL-2 therapy (25). Some investigators suggest an
16

inhibitory effect of sIL-2Rα, the soluble form competing with the signal transducingmembrane bound receptor for the IL-2 molecules (26). This is however debatable regarding
the different affinities of the receptors for the IL-2 molecule.
2.1.3 Biological effect on cellsThe phenotype of a variety of lymphoid cells proliferating in response to IL-2in vitro appear
to depend on the concentration of IL-2 and the duration of culture. At relative lowconcentrations IL-2 is able to induce cytolytic activity in MHC-restricted, antigen specific T
lymphocytes (CTL) after 6-7 days. These CTL express CD3, CD8, CD10 and CD16 surfaceantigens. Natural killer (NK) cells exhibit a broad range of MHC-nonrestricted cytotoxic
responses when exposed to IL-2 after 2 to 3 days. NK cells comprise 2-5% of the peripheral
blood mononuclear cells and these cells may express CD2, CD3, CD7, CD8, CD11, CD16,CD35 and CD56 surface antigens. When incubated with higher concentrations of IL-2, resting
peripheral blood large granular lymphocytes, T lymphocytes and possible even B lymphocytesbecome capable of non-specific lysis of fresh cancer cells but not normal cells after 5 to 10
days in short-term assays. This was named the Lymphokine Activated Killer (LAK) cell
phenomenon (27). Lymphocytes expressing LAK activity may express CD2, CD3, CD5, CD6,CD7, CD8, CD11, CD16, CD45 and CD57 surface antigens (28,29). Lymphocytes infiltrating
a tumor are frequently found in surgically removed tumors. These cells can be selectivelyexpanded to large numbers from tumor cell suspensions using IL-2. These tumor infiltrated
lymphocytes (TIL) are generally of the CD3 CD8 positive phenotype and have been reported
to show specific MHC-restricted killing (30). Upon stimulation by IL-2 several secondarycytokines are induced. NK-cells produce IFN-γ, GM-CSF and TNF-α and -β (31). Monocytes
release large amounts of IL-1, IL-6, and TNF-α when stimulated by cytokines in conjunctionwith bacterial agonists (32,33). In vivo IL-2 treatment induces the production of several
growth factors including IL-5, GM-CSF, M-CSF and IL-6 (34).
2.2 Preclinical studiesIn murine models, repeated systemic administration of high doses IL-2 induced LAK-cytotoxicity in vivo and resulted in significant antitumor responses in disseminated murine
leukemia, as well as in fibrosarcoma and melanoma metastases (35-37). The intravenous ad-
ministration of in vitro activated LAK-cells in combination with IL-2 induced also a sig-nificant reduction in the number and size of murine pulmonary and hepatic metastases
(38-40). These effects were dependent on the dose and schedule of IL-2 administered (41-45),the number of LAK-cells infused (36,38,40) and on the extend of the tumor burden (36,46).
Tumor inhibition has also been observed with low doses of IL-2 (43,47). Established 10-day
metastases but not 3-day metastases were sensitive to low dose IL-2 (43). Athymic nude micefailed the low dose IL-2 treatment while they were responsive to high dose IL-2, suggesting
that the antitumor activity of low dose IL-2 was T cell mediated (47). Local intratumoral
17

injections with low doses of IL-2 could cure mice bearing a large burden of metastatic tumor(48,49). How an effective antitumor response in vivo is orchestrated using these different
mechanisms is poorly understood. Despite the direct cytotoxicity of LAK cells against tumor
cells in vitro, in vivo studies have shown that LAK cells do not selectively localize to tumorsites. In a rat model, systemically infused labeled-LAK cells migrated first to the lung and
subsequently to the liver and spleen in a 2 to 6 hours period. No difference in the distributionpattern was observed between normal and tumor bearing animals (50). Adoptively
administered TIL cells have been shown to travel to metastatic sites in clinical imaging
studies (30,51,52). Lymphocytes infiltrating renal cell carcinoma or lung carcinoma, however,have been shown to be functionally impaired, possibly due to tumor-derived
immunosuppressive factors (53,54). Interestingly, lymphocytes of tumor bearing mice havebeen found to have structurally altered CD3-TCR complexes, including the loss of the signal-
transducing CD3-ζ chain (55). If these findings also apply to human lymphocytes, this may
have important consequences for future immunotherapy studies.
2.3 PharmacokineticsUnder physiological conditions IL-2 is thought to act in an autocrine and paracrine way in
localized areas of inflammation with no detectable levels in the circulation. Pharmacokinetics
of exogenous administered IL-2 have been studied in rodents and in humans. The differentmutated recombinant proteins of IL-2 do not differ significantly in their pharmacological
properties and they will not be discussed separately. After intravenous administration, IL-2is rapidly distributed to the extravascular, extracellular space. Approximately 30% of the
administered dose initially distributes over the plasma volume. After high peak levels, serum
concentrations decrease with an alfa and beta half-life of 13 minutes and 2 hours, respectively(56). With a clearance rate of approximately 120 ml/min, the kidneys appear to be the main
site of clearance where IL-2 is probably metabolized by the proximal renal tubules, asminimal levels of active IL-2 are found in the urine (56,57). During 24-hour infusion serum
IL-2 concentrations appear to reach a steady state after 2 to 6 hours (56,58). The hydrophobic
nature of IL-2 necessitates formulation with albumin or a detergent to maintain solubility (59).At slow infusion rates and low concentrations the bioavailabillity of some IL-2 muteins may
be reduced due to adherence to the infusion material (60). After subcutaneous bolus injectionIL-2 serum concentrations rise slowly, reaching a maximum concentration after 3 to 4 hours.
The serum levels decline slowly with prolonged mean half-lives of 4 to 5 hours (58).
Intraperitoneal infusion of IL-2 results in long half-life times with medians of 22 and 6.3hours in peritoneal fluid and serum respectively. The serum concentrations seem to reflect the
efflux from the peritoneal cavity (56). Other routes of administration of IL-2 includeinhalation (61) and regional injection of IL-2 (62). No pharmacological data on these routes
are available. Modifications of IL-2 with monomethoxy-polyethylene-glycol (PEG-IL-
2)(63,64) or a collagen matrix (65) alters its pharmacokinetics properties resulting in a
18

prolonged serum half life time.
2.4 Clinical spectrum of IL-2In contrast to the broad spectrum of activity in pre-clinical models, IL-2 has in clinicaloncology emerged as a treatment for renal cell cancer almost exclusively. The overall
response in this tumor is around 20% and this is not different from the remission rate inpatients with melanoma. Probably the acceptance of IL-2 as a treatment of renal cell cancer
is dictated also by the lack of active alternatives in that tumor (although as is discussed later,
activity of interferon is at least quantitatively not very different). In melanoma dacarbazine(DTIC) has the same response rate as IL-2 but since the introduction of 5-HT3-receptor
antagonistic anti-emetics this treatment is less toxic. Alternatives for IL-2, in the sense ofequally (in)effectivity exist in all tumors other than renal cell cancer. However occasional
responses have been described for IL-2 in a broad spectrum of tumors. Colorectal
adenocarcinoma for instance is relatively insensitive to IL-2 based immunotherapy. In theNational Cancer Institute trials 5 out of 30 patients responded to IL-2/LAK treatment while
no responses were observed in 12 patients treated with IL-2 alone (66). In a review of 15trials with IL-2 containing trials, the National Biotherapy Group reported only one partial
response among 76 patients treated (67). In patients with ovarian cancer with disease confined
to the abdomen, intraperitoneal administration of IL-2 or LAK cells have been used withreported response rates of 20%. Intraperitoneal fibrosis and abdominal pain were dose limiting
factors in this approach (68,69). In patients with bladder cancer, intravesical instillation ofhigh dose IL-2 produced almost no toxicity. One complete response lasting more than 6
months was observed in a small group of 5 patients (70). In patients with lung cancer, a
response rate of 16% was reported by the National Biotherapy Study Group, but most of theseresponses could be attributed to the concomitant treatment with etoposide or cisplatin (67).
Clamon et al. reported a response rate of 21% in a phase II trial with continuous infusion IL-2in patients with extensive small cell lung cancer who failed first line combination
chemotherapy with cisplatinum, doxorubicin, cyclophosphamide and etoposide. Complete
responses were observed in 17% of patients, but toxicity, especially pulmonary toxicity, wasconsiderable, requiring discontinuation of treatment in 46% of patients (71). In patients with
non-Hodgkin lymphoma, early trials showed promising results mainly with IL2/LAKtreatment with reported response rates up to 40% but this has not been confirmed by other
trials. Small patient numbers and conflicting results preclude any conclusions about the role
of IL-2 in the treatment of non-Hodgkin lymphoma (66).In conclusion, the actual activity spectrum of IL-2 in human tumors may not differ that
much from the earlier experience with this drug in model systems. Its clinical use isinfluenced primarily by the alternatives in therapy and especially by the IL-2 related toxicity
(and possibly economic considerations). The concept that there is a relation between
"immunogeneity" of tumors and IL-2 activity is challenging but needs substantiating. Despite
19

considerable clinical experience with the use of IL-2 in the treatment of patients with cancer,several important issues still remain unresolved. This review will address some of these key
questions; 1) Is there a relation between tumor response and route of administration? 2) Is
there a dose response relation for IL-2? 3) Does the addition of adoptively administered LAKor TIL cell increase response rate? 4) Does IL-2 based immunotherapy have an effect on
survival?
Effect of route of administration on responseMost patients are treated systemically by the intravenous or subcutaneous route. Intravenous
therapy, given either as bolus injections or as a continuous infusion is associated withconsiderable dose dependent toxicity which necessitates special care for patients treated.
Subcutaneous administration produces local toxicity at the injection sites that can be
inconvenient, but the systemic toxicity with the vascular leak syndrome is rarely observed.No randomized experiences concerning efficacy are available between subcutaneous and
intravenous IL-2 treatment. However, in view of the range of activity of IL-2 given eitherway, a difference in response rate, if present, will be limited to 5%. Also the incidence of
complete remissions after both administrations is limited to a narrow range. So differences
in effects of the two routes of administration if present will be found in the duration ofresponse and the quality of life of non-responders. If eventually comparative studies are going
to be done, these questions will have to be addressed.IL-2 has also been administered regionally by several other routes including
intraperitoneal (69,72,73), intravesical (70), intrapleural (74), intraspinal (75), intralymphatic
(76), extracorporal perfusion (77), arterial perfusion of the liver or spleen (78,79), local slowdelivery pellets into the tumor (65), and by inhalation (61). Toxicity of these regional
applications were mostly less than with intravenous administration, but patient numbers areto small to draw conclusions about the clinical efficacy of these routes of administration.
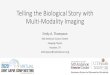
Legend to figure 1. Response rates with 95% confidence intervals of IL2 monotherapy studies inpatients with metastatic renal cell carcinoma. The dashed line expresses the mean, the box the 95%confidence interval of the cumulative response of all patients included.
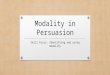
Legend to figure 2. Response rates with 95% confidence intervals of IL2 monotherapy studies inpatients with metastatic melanoma.The dashed line expresses the mean, the box the 95% confidenceinterval of the cumulative response of all patients included.
20


Effect of dose and treatment regimen on antitumor efficacyIn a randomized phase II trial comparing intravenous high-dose IL-2 bolus injections with
24-hour continuous infusion at equivalent toxic doses in the treatment of patients with renalcell carcinoma, no difference was shown in antitumor activity (80). No comparative studies
on the dose-response relationship of IL-2 among humans have been reported but numerousphase II studies have been performed using different doses and treatment regimens. Taking
into account the limitations of comparing results between different phase II trials, acomparison of the impact of dose on clinical results in patients with renal cell cancer and
melanoma is presented here (Fig. 1 to 4) To prevent the bias of small studies, a selection hasbeen made, including only those trials with more than 20 patients. In figures 1 and 2 the
response of several trials with the 95% confidence intervals is shown for patients with RCCand melanoma, respectively. In an attempt to compare different treatment schedules, the IL-2
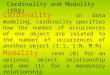
dose is expressed as dose intensity (DI), defined as the dose of IL-2 administered in the firstseven days of treatment. Figures 3 and 4 show the response rates in patients with renal cell
cancer (66,80-104) or melanoma (66,88,89,101a,105-111). We conclude that no dose responserelation is observed in either renal cell cancer or melanoma patients. IL-2 induces an objectiveresponse rate of 18% (14%-19%, 95% confidence interval) of the patients with renal cell
cancer; in approximately 6% these responses are complete. In melanoma response rates of15% (11%-19%, 95% confidence interval) are observed with complete responses in less than
5%. In both groups response duration in patients with a complete response can be durablewith some of the patients remaining free of disease for more than 2 years.
Adoptive immunotherapyWe conclude (Figs. 3 and 4) that the considerable logistic burden of LAK acquisition is nottranslated into improved results. In a overview on 15 different phase II protocols with
inpatient IL-2 treatment, the National Biotherapy Study Group reported a higher response ratein the protocols involving adoptive immunotherapy than in those without in vitro activated
cells (15% versus 7%, respectively, p=0.003), but without any effect on survival (67). Inanother analysis of 327 patients treated in 5 different protocols Palmer, using multivariant
analysis, could not observe any difference in objective response nor in survival when hecompared treatment with IL-2 alone or in conjunction with LAK-cells (97). In three
prospective randomized controlled trials, the addition of LAK-cell treatment to continuousinfusion or high-dose bolus injection IL-2 in melanoma and renal cell cancer patients had no
Legend to figure 3. Dose intensity/response relation of IL-2 with or without adoptive immunotherapyin patients with metastatic renal cell carcinoma. Open points ( ), IL2 monotherapy ; solid points ( ) IL2+ adoptive immunotherapy.Legend to figure 4. Dose intensity/response relation of IL-2 with or without adoptive immunotherapyin patients with metastatic melanoma. Open points ( ), IL2 monotherapy ; solid points ( ) IL2 +adoptive immunotherapy.
22


effect on response rate or on survival (80,101,112). One study among melanoma patientsreported a correlation between the number of TIL-cells infused and the clinical response, with
responding patients receiving significantly more TIL’s than non-responders (113).Rosenberg reported initially a response rate of 50% in patients with melanoma (114) but these
results could not be confirmed in other studies. Dillman could raise TIL’s in only 21 out of82 patients with melanoma, and he reported responses in 5 out 21 patients (24%, 10% - 49%,
95% confidence interval) (115). Bukowski was able to raise TIL’s in 18 of 25 eligible patientswith renal cell carcinoma, but no responses were observed (116). Baars et al also observed
no responses in 4 patients with melanoma (117). The treatment with TIL’s is possible in onlya minority of patients, it is technically difficult, costly, and the clinical results are not superior
to those with other IL-2 based regimens.
Effect on survivalThe effect of IL-2 treatment on survival remains unclear. Randomized trials comparing
patients treated with IL-2 with control patients that could answer this issue are not availableand ethical considerations limit the institution of these trials. Retrospective studies are limited
by the influence of patient selection and changes in diagnostic procedures over time
(118,119). In historical control groups the median survival of patients with metastatic renalcell carcinoma was 8 months (120). In an analysis of a cumulated single center experience
in 181 patients with RCC who were candidate for IL-2 therapy, median survival afteroccurrence of metastases was 16 months in all patients irrespective of treatment with IL-2
(intention to treat). Comparison of this survival with a historical control group from the same
institution was however impaired due to the lack of information on two important prognosticfactors being weight loss and performance status in the control group. The relative high
median survival of this group may reflect the difference in diagnostic procedures over timewith the availability of a new treatment modality (121). Given the small numbers of
responders in all series the effect of IL-2 therapy on survival is influenced by especially
patients with stable disease and possibly also by non-responders.
2.5 Markers of clinical responseOnly a minority of patients respond to IL-2 based immunotherapy, while toxicity occurs in
all. Therefore, several investigators have looked for markers that could predict or monitor
clinical response. Despite intensive research, no consistent relationship betweenimmunological changes and clinical response has been found (97,101). Several factors have
been partially related to treatment efficacy. These include the number of pretreatmentlymphocytes, the number of eosinocphils, the expression of CD56 on NK-cells, sustained
serum levels of TNF, high levels of soluble CD8 and low pretreatment C-reactive protein
(CRP) serum levels (122-128). Elevated levels of IL-6 before IL-2 treatment were associatedwith disease progression after therapy and shorter survival (129). Previous chemotherapeutic
24

treatments had a negative effect on clinical response in patients with renal cell carcinoma(130) but not in melanoma patients (113). Among melanoma patients HLA Class I phenotypes
were correlated with response to IL-2 based immunotherapy. Responding patients had a
significantly higher frequency of the alleles A11 and A19 than the overall melanoma patientpopulation (113). High numbers of CD8bright and CD56-cells that express the HLA-DR
activation marker were found to be prognostic for a good therapeutic response tosubcutaneous IL-2 treatment (123). As to the localization of responses, most responses are
observed in the lung or soft tissues, while few responses are observed in the primary tumor
or bone lesions.
2.6 TolerabillityBecause of a dose relationship observed in animal studies the initial clinical studies were
performed with high dose bolus injections of IL-2 (37,38,40,131,132). High dose treatmentis associated with severe toxicity for which intensive care support is necessary in an number
of patients. IL-2 therapy is accompanied by considerable side effects, including fever, chills,nausea, vomiting, skin toxicity, hepatic and renal dysfunction, mental status changes, and
respiratory failure. The most frequent dose limiting side effect of high dose intravenous IL-2
is hypotension. Frequency and severity of IL-2 toxicity is dose-related and schedule-dependent. High dose intravenous regimens require intensive treatment care monitoring and
patient selection. Most adverse reactions are self limiting and are usually reversible within 2to 3 days after discontinuation of therapy. The mechanisms of IL-2 induced toxicity are partly
understood. The release of secondary cytokines such as IFN-γ and TNF-α are thought to be
important mediators of toxicity (133,134). Passive immunization against TNF-α could indeedpartially abrogate IL-2 toxicity (135). More recently, the role of cytokine induced nitric oxide
has been proposed as a central factor in IL-2 induced hypotension (134). The L-alanine analogNG-methyl-L-arginine has been used in patients with renal cell cancer in order to reduce nitric
oxide production to suppress IL-2 toxicity (136). Since the effector mechanism of IL-2
therapy in vivo is not defined care has to be taken with these approaches not to suppress theantitumor effects of IL-2 as well.
2.6.1 Cardiovascular effectsSeveral cardiac side effects have been observed during IL-2 therapy including arrhythmias,
ischemia, myocarditis, hypocontractility and pericardial effusions (66,137-140).Supraventricular arrhythmias, particularly supraventricular tachycardia and atrial fibrillation,
occur in 10% or more of the patients treated with intensive regimes and generally resolveafter discontinuation of IL-2 (138). In patients over 65 years of age who were treated with
intravenous IL-2, cardiac side effects, especially arrhythmias were the most important dose
limiting toxicities (96). Angina and myocardial infarction have been observed by several
25

investigators in patients treated with IL-2. In large series ischemia occurred in 3% to 9% ofpatients and myocardial infarction in 1 to 4% (3,139,141). The frequency of these toxicities
depend on patient selection and treatment regimen. ECG changes, CPK-MB band elevations,
with or without chest pain have been described that may not represent infarction or ischemiabut rather an IL-2 induced, nonischaemic myocardial injury or myocarditis (142).
Hemodynamic changes after IL-2 administration resemble those observed in early septicshock. Shortly after IL-2 administration, a fall in mean arterial pressure resulting from the
decreased systemic vascular resistance induced by IL-2 is observed, which is countered by
an increase in heart rate and cardiac output (140,143). Subsequently, the development of a’vascular leak syndrome’ (VLS) leads to extravasation of fluid and albumin from the
intravascular space, resulting in edema and extravascular fluid accumulation which may leadto or exacerbate pleural effusions and ascites. These effects may be due to a variety of
lymphokines induced by IL-2 such as interferon-γ and tumor necrosis factor-α. Nitric oxide
produced by macrophages and endothelial cells might play a role in the induction ofhypotension during treatment with IL-2 (134,144).
2.6.2 Pulmonary effectsPulmonary congestion, interstitial oedema, dyspnoea and pleural effusions are common results
of the VLS (66,82,137,138). In high dose regimens, approximately 20% of the patientsdevelop respiratory distress and 5- 10% require intubation and mechanical ventilation
(66,137,138). Reversible bronchospasm has been observed in patients undergoing IL-2therapy.
2.6.3 Renal effectsRenal dysfunction is one of the major complications of IL-2 therapy. Azotemia, oliguria,
elevated plasma aldosterone and renin activity with low fractional sodium excretion andincreased serum creatinine levels are found in more than 60% of patients. Prerenal
mechanisms with impaired renal perfusion due to the reduced cardiac function, peripheral
vascular dilatation and intravascular volume depletion are thought to be the cause of theseabnormalities in renal function (145). An additional intrarenal defect has been postulated
(146). Most nephrotoxicities are transient and tend to resolve after cessation of treatment,although in some patients recovery may be prolonged or incomplete (147,148). Administration
of non-steroidal anti-inflammatory drugs can contribute to the impairment of renal function
(81).
2.6.4 Gastrointestinal and hepatic toxicityNausea and vomiting, stomatitis, peptic ulceration, anorexia and diarrhea are frequently
observed during IL-2 therapy. Rarely, bowel hemorrhage, perforation, infarction and
exacerbation of Crohn’s disease have been reported (149-151). Elevated values of liver
26

enzymes are frequently observed. Intravenous IL-2 treatment related reversible intrahepaticcholestase with elevated billirubin levels has been described in a number of patients (152).
2.6.5 Endocrine effectsThyroid dysfunction is reported by several investigators, with a frequency ranging from 20-90
percent of patients treated with IL-2. Initially LAK cells appeared to be essential for thedevelopment of hypothyroidism (153), but in later studies thyroid dysfunction has also been
reported after treatment with single agent IL-2 (154), IFN (155), or combinations of IL-2 and
IFN (156-159). Primary hypothyroidism, hyperthyroidism as well as biphasic dysfunction withhyperthyroidism followed by hypothyroidism have been reported. Thyroid dysfunction has
been found to correlate with treatment duration (160), cumulative dose of IL-2 (161) and afavorable tumor response to treatment (161,162). However, in another study no relation
between response and thyroid dysfunction was observed (160). The pathogenesis of
hypothyroidism is probably multifactorial. Because of elevated anti-thyroglobulin antibodyand anti-microsomal antibody titers, autoimmunity has been implicated as a mechanism for
thyroid dysfunction. However, in most studies the presence of auto-antibodies did notcorrelate with hypothyroidism.
Increased hormone levels of beta-endorphin, adrenocorticotropic hormone (ACTH),
and cortisol have been reported after intravenous IL-2 administration given as a bolus orconstant infusion. The effect of IL-2 was not altered by the concomitant administration of
LAK cells. Increased hormonal stimulation occurred upon re-exposure to IL-2 (163).Melatonin levels were found to be significantly decreased during IL-2 infusion. The IL-2-
induced effects on cortisol, beta-endorphin and melatonin levels resulted in a complete
abolition of their physiological circadian rhythm (164). Endocrine effects of subcutaneousIL-2 therapy were found to be similar to those observed with intravenous administration
(165).
2.6.6 Neurological effectsNeuropsychiatric changes are frequently observed during IL-2 therapy. On intensive treatmentregimens, patients become frequently agitated, combative, and disoriented, or somnolent and
occasionally comatose (66,82,137). These symptoms may progress even in the first days aftercessation of IL-2 therapy (166). Increased brain water content of both grey and white matter
in patients receiving intravenous IL-2 therapy have been observed using magnetic resonance
imaging (167). Perivascular demyelinization was observed on autopsy in a patient with amalignant melanoma who developed neurological symptoms (ataxia, visual disturbances) and
subsequently died after receiving IL-2 therapy (168). Hyperesthesia and paresthesia have beenobserved in patients on IL-2 therapy. Transient ischemic attacks and cerebrovascular accidents
have occurred during IL-2 administration (137).
27

2.6.7 Dermatological effectsCutaneous toxicities include macular erythema, pruritus, and general erythrodermia with dry
desquamation, especially of palms and soles, affecting almost all patients treated with the high
dose regimens and approximately half of the patients at the intermediate dose regimens. Theerythema resolves within 48 hours but the desquamation can last for several weeks. Sporadic
erythema nodosum, angioneurotic edema, lobular panniculitis, urticaria, fatal pemphigus andlife threatening bullous skin lesions have been observed (169-173). Subcutaneous
administration of IL-2 caused transient inflammation at the injection sites, and nodular lesions
resembling subcutaneous lipomas, that gradually disappeared within 6 months. Concomitantuse of anticoagulant therapy can cause sometimes local hemorrhage at the injection sites
(174). Exacerbations of pre-existing psoriasis and polymyositis/dermatomyositis have beenreported after intravenous IL-2 therapy (137,175).
2.6.8 Hematological effectsEosinophilia, probably due to an increase in IL-5 levels (176); early transient lymphopenia
and rebound lymphocytosis are observed in all patients. Thrombocytopenia is frequentlyreported as a clinical important toxic side effect of intravenous IL-2 therapy.
Thrombocytopenia was found to be directly related to IL-2 dose and indirectly to renal
function. A peripheral clearing mechanism triggered by the IL-2 dependent release of aleucocyte-produced eicosanoid that initiates platelet degranulation and clearing by the
reticuloendothelial system is hypothesized (177). Using a cDNA-polymerase chain reaction(PCR) with specific primer sets for the various colony stimulating factors, Schaafsma et al
showed that IL-2 treatment induced the expression of mRNA for M-CSF, GM-CSF, IL-3, and
IL-5, but not for G-CSF, in peripheral blood monocuclear cells. Furthermore no IFN-γ orTNF was detected in plasma (34).
2.6.9 Infectious complicationsIL-2 therapy is complicated by development of bacterial infections in approximately 23% of
the patients.Staphylococcus Aureusis the most commonly isolated organism (178-180).Bacterial sepsis is one of the major causes of death related to IL-2 therapy, and is frequently
catheter related. Prophylactic use of antibiotics before the placement of central venous
catheters markedly reduces the incidence of infection to approximately 7% (181).Subcutaneous administration may also limit the incidence of infection, although inflammation
at the injection site is frequently observed (174,182). Reversible impaired neutrophilchemotaxis during IL-2 therapy has been reported that may contribute to the development of
infection (183) These effects may be due to secondary release of TNF since concomitant use
of dexamethasone both decreases IL-2 induced release of TNF and almost completelyabrogates the chemotactic defect (184).
28

2.7 Combination treatmentIL-2 based immunotherapy has been investigated in combination with a number of other
molecules including interferons (156,185-187), TNF (188-190), cytokines (26,191) and
cytotoxic agents (192-196) to increase response rates or to reduce toxicity.
IL-2 and interferonSynergistic activity of IL-2 and IFN-α has been suggested in preclinical studies (197,198),
because interferon induces upregulation of MHC-molecules on tumor cells (199,200). In
several phase I/II studies the activity of this combination was shown (156,185-187). Howeverin 3 randomized controlled trials comparing IL-2 alone or combined with IFN-α no
differences in immune parameters, nor antitumor activity were observed (100,111,201). Inrenal cell cancer the IFN/IL- 2 combination induced response rates of 4 to 42%, with an
average response rate of all patients of 18% and complete responses occurring in 5%
(67,100,112,130,185,202-213) In melanoma response rates of 4 to 59% are reported with anaverage response rate of all included patients of 29% and CR occurring in 7%
(111,196,214-216).
IL-2 and other cytokinesCombination of IL-2 and TNF resulted in synergistic activity in generating LAK-cells (217),enhanced activation of peritoneal macrophages (218), and antitumor activity in murine models
against sarcoma cells (189). Clinical results were reported by Rosenberg and Dillman withresponses only in patients with melanoma and renal cell carcinoma. The response rates in
these trials were not different from that expected from the use of IL-2 alone (66,67). In a
phase I trial with low dose IL-2 and TNF in patients with non small cell lung cancer, TNFshowed a four fold lower MTD compared to the single-agent use of TNF with
thrombocytopenia as dose limiting factor. One partial response was observed in 12 evaluablepatients (188).
IL-3 and the pineal hormone melatonin (MLT) inhibited neopterin release and
significantly decreased IL-2 induced sIL-2R secretion when given in combination with IL-2(191). The increase in soluble IL-2 receptor (sIL-2R) and neopterin levels were related to the
generation of macrophage-mediated immunosuppression and these were associated with areduced clinical efficacy during IL-2 therapy. In a phase II study with combined s.c. IL-2 and
i.v. IL-3 treatment the increase in serum neopterin, serum sIL-2R and serum cortisol were
neutralized by IL-3. Toxicity was decreased in the IL-3/IL-2 combination compared withtreatment with IL-2 alone. One out of six patients treated with the IL-2/IL-3 combination had
a partial response of a lung adenocarcinoma with a response duration of 7+ months (26).
IL-2 and chemotherapyThe combination of IL-2 based immunotherapy with chemotherapy has been studied in several
29

trials. In early studies low doses of cyclophosphamide have been used in an attempt to reduceimmunosuppressive cell populations during IL-2 therapy without improving response rates
(192,193). Sequential combination of IL-2/LAK immunotherapy with DTIC in melanoma
patients resulted in a response rate of 26% (194). In two recent studies in melanoma patientspromising results have been reported with sequential combined chemoimmunotherapy
consisting of IL-2/IFN with CDDP(195) or CDDP, BCNU and DTIC resulting in responserates of 54 and 57%, respectively (196).
2.8 Conclusions and perspectivesClearly the early promise of IL-2 as a major breakthrough in cancer treatment has not beenfulfilled. Nevertheless IL-2 has permitted the conclusion that tumors in patients can regress
as a result of the immune response from that patient. This confirmation of the applicability
of the immune response in the setting of advanced cancer should form the basis for furtherstudies. What directions should these studies take? In our opinion not much is to be gained
by further analysis of modifications in dose or schedule. Also the impact of reducing toxicitywill be marginal. The addition of other drugs to IL-2 does not seem to be promising although
occasional observations such as the results of the combination IL-2, IFN and platinum in
patients with melanoma are provocative (195). If such observations are reproducible theymight lead to the direction of changes brought about by cytotoxic drugs, presumably
membrane changes, that makes these cells more easily recognizable for activated lymphocytes.A systematic approach into the problem of non-responders to IL-2 should start with analyzing
the mechanism for resistance. This could stem from a general lack of stimulation of the
immune system, however, this seems not likely as with present day techniques no differencescan be found between cell populations in responders and non-responders. If the relevant cells
are present in the circulation, the problem may be for them to reach the tumor. This is notunlikely as homing experiments fail to demonstrate selective penetration of LAK cells into
the tumor. The fact that TIL cells do home, suggests that these cells have some memory of
their past migration pattern. Analysis of this pattern might solve some of the problems.However in clinical practice, at least during subcutaneous treatment a pattern of mixed
response is often seen; some lesions grow, others remain stable or diminish. This suggestsclonal differences in the metastases with regard to recognition by LAK cells. Retargetting of
LAK cells to a more common antigen may deal with this problem. Another way would be to
trigger tumor cells to express recognizable antigens, this will probably require the applicationof gene transfer techniques into clinical oncology.
3 Interferon
The use of the interferons in solid tumors has been reviewed by several investigators
30

(4,219-222). Originally they were described as antiviral factors (223), but after discovery oftheir antiproliferative and immune modulatory activities, partly purified human leucocyte
derived interferon (IFN) was investigated as a potential anticancer agent. Numerous clinical
trials started after highly purified interferons produced by recombinant DNA-technologybecame available. Today, interferon is used in the treatment of several hematologic
malignancies as well as in patients with solid tumors. In this review the role of IFN-α in thetreatment of solid tumors will be discussed.
3.1 BiologyInterferons are a family of more than 20 proteins which are produced by different cell types
under specific activating conditions. Type I IFNs are synthesized in response to viralinfections or following exposure to B-cell mitogens, foreign cells or tumor cells. Lymphocytes
produce primarily IFN-α, whereas IFN-β is produced by fibroblasts. The originally termed
IFN-β2, now renamed interleukin-6, will not be discussed here. Type II IFN, IFN-γ isproduced by antigen- or mitogen-activated T lymphocytes. A new interferon family, IFN-ω,
has been distinguished from other interferons (224). The genes for IFN-α, IFN-β and IFN-ωhave been found on chromosome 9 and the one for IFN-γ on chromosome 12. There are 23
IFN-α genes (8 pseudogenes) encoding acid-stable peptides of 18-20 kD. Only one single
gene for IFN-β has been identified encoding 166 amino acids. IFN-β is an acid stableglycoprotein of 23 kD. For IFN-γ a single gene encoding for a protein of 144 amino acids
has been identified. There are two active forms of IFN-γ: glycosilated proteins of 20 kD and25 kD. The genes for theα, β andγ interferones have been cloned and expressed in bacterial
systems. Interferons bind specifically to receptors on the target cell membrane. IFN-α and
IFN-β share the same receptor, found on the surface of most cells. The gene for the receptorfor IFN-α and -β has been found on chromosome 21 while chromosome 6 encodes for the
IFN-γ receptor (225,226). The IFN-γ receptor is found on T-cells, B-cells, monocytes,neutrophils, fibroblasts and colony forming cells. Antineoplastic activity of IFN probably
results form a direct inhibitory effect on cell growth and proliferation, and from indirect
effects on the immune system, including increased NK-cell activity, enhanced expression ofMHC class I and II cell surface antigens (200, 227) and stimulatory or inhibitory effects on
certain B- and T-cell functions.
3.2 Preclinical studiesPharmacokineticsThe pharmacokinetics of IFN-α have been studied in healthy volunteers. After an intravenous
injection plasma levels of IFN-α decrease with an alfa and beta half life times of 5-10minutes and 4-5 hours, respectively. Intramuscular or subcutaneous injections results in peak
levels occurring after 4 to 7 hours. The area under the plasma concentration-time curve
(AUC) after subcutaneous or intramuscular injection is approximately 80 to 100% of that after
31

intravenous administration. The distribution volume at a steady state condition was 31.4 L.The clearance of IFN-α occurs mainly by catabolism in the renal tubulus, no active protein
is found in the urine (228,229).
3.3 Clinical spectrumThe clinical use for oncological purpose of IFN-β and IFN-γ has been investigated lessintensively than IFN-α. IFN-β has been studied mainly in patients with RCC (230,231). IFN-
γ has been studied alone (232-234), or in combination with IFN-α (235), or IL-2 (236-238)
or TNF (239). This review will focus on the clinical use of IFN-α in solid tumors. Mostquestions as to potential influence of dose and route of administration seem to have been
solved and the answers have been dictated by acceptability of toxicity. A narrow field ofindications seem to be emerging, although recently its limits may have been changed by
descriptions of influence of IFN-α on chemotherapeutic effects especially on 5FU. IFN-α is
approved for the treatment of patients with hairy cell leukemia, where response rates of 80%could be achieved. In chronic myeloid leukemia treatment with IFN-α has resulted in
therapeutic responses in up to 70% of the patients and occasional in the reversion to a normalchromosomal state (240). Responses to IFN-α are also reported in patients with Kaposi’s
sarcoma (30%), myeloma (10-20%), and carcinoid tumors (40%). Reproducible activity also
was found against tumors such as melanoma and renal cell carcinoma, which are unresponsiveto conventional chemotherapy.
3.3.1 Renal cell carcinomaThe use of the interferons in renal cell carcinoma has been reviewed by Muss (241).
Interferon induces responses in 13% of patients with renal cell carcinoma, with mostly partialresponses. Median response duration was 6 months. Routes of administration do not appear
to influence response rates or toxicity although intramuscular or subcutaneous administrationmay be preferable. Maximal response rates are obtained with both low and intermediate doses.
Randomized studies addressing the dose-response issue suggested in two trials that a high
dose regimen was superior, while a third study did not show any difference between the lowand high dose treatment. Toxicity was substantially enhanced using the high dose IFN in all
trials (242-244). A dose of 5-10 MU, given subcutaneous or intramuscular, at least three timesa week appears to result in the best therapeutic index. In one study, antibody formation,
occurring in up to 38% of the patients was associated with a loss of toxicity and a decrease
in median survival and remission duration (243).
3.3.2 Malignant melanomaThe use of IFN in the treatment of patients with malignant melanoma has recently been
reviewed by Kirkwood (245). In several clinical trials response rates of 12% - 22% were
reported with occasional complete responses. No dose response relationship has been found
32

in melanoma patients in the range of 10 to 100 MU IFN with daily or alternate-day dosing.Responses may be observed late during therapy after 3 - 6 month, with most of them being
partial, with a median response duration of 4 months. However, a small minority of patients
may achieve long term disease free remissions of several years following IFN-α therapy(246). IFN-α has been used in combination with cimetidine (247), zidovudine (248) and
cytotoxic agents with either no or small improvement in response rates. The combination ofDTIC with recombinant interferonα-2a has been shown to produce objective response rates
of 26%, with low toxicity and maintenance of quality of life. In some, but not all randomized
trials with DTIC as a single agent, the combination treatment showed improved response rates(249-252). The combination treatment of patients with melanoma using IFN, IL-2 and
cytotoxic agents is discussed in section 2.7.
3.3.3 Aids related Kaposi’s sarcomaKaposi’s sarcoma is a rare malignant disease that is associated with the acquiredimmunodeficiency syndrome (AIDS). Numerous controlled trials have demonstrated
reproducible response rates in the range of 20-40% with IFN-α therapy; a substantialproportion have been complete responses. Higher doses IFN (>=20 MIU/m2/day) have been
associated with better responses than lower doses. The total lymphocyte count, CD4
lymphocyte count, and CD4/CD8 ratio, as well as the beta-2- microglobulin level have beenassociated with better responses (253). Combination of IFN-α with chemotherapeutic agents
have not produced significant enhanced response rates compared with IFN alone. Howeverthe hematological and other organ related toxicity were enhanced and dose reductions of both
IFN and the cytotoxic drug were often necessary. Combination of IFN with zidovudine
produces good results, with reproducible response rates of approximately 40%, whilesuppressing HIV-infection (248,254). The clinical use of this combination is however
frequently complicated by the overlapping myelotoxicity, particularly neutropenia, of theseagents. Hematopoietic growth factors such as granulocyte (G-CSF) or granulocyte-macrophage
colony-stimulating factor (GM-CSF) can be useful in restoring neutrophil counts and
preventing of otherwise required dose modifications, but it did not have an effect on theresponse rate, the CD4-cell count, or the improvement in any other hematologic parameter.
The use of growth factors was not associated with an increased toxicity or a change in serumHIV p24 antigen (255).
3.3.4 Colorectal cancerIFN-α as a single agent has only little activity in the treatment of patients with colorectal
cancer, with response rates of approximately 10% (256,257). In vitro IFN-α synergisticallyaugments the cytotoxic effects of the antimetabolite fluorouracil (5-FU) against human colon
cancer cell lines (258). IFN-α can also improve 5-FU/Leucovorin mediated growth inhibition
in fluoropyrimidine sensitive colon cancer cells (259,260). In animal studies interferon
33

potentiates the effect of 5-FU in inhibiting liver metastases in nude mice (261). Themechanisms of the synergy between IFN and 5-FU are not clarified. IFN-α treatment of
HT-29 colon carcinoma cells induced a greater than two-fold increase in the intracellular
levels of the active metabolite of 5-FU, FdUMP. Using cell extracts from HT-29 cells and 5-FU as substrate, IFN-α produced a 1.9- and 8.7-fold increase, respectively, in the activities
of uridine phosphorylase and pyrimidine nucleoside phosphorylase (PyNP). The effect wasselective for the conversion of 5-FU to FdUMP, as IFN-α did not increase the cellular levels
of FUTP, nor did it change the extent of incorporation of 5-FU into RNA (or DNA). IFN-αalso had no effect on thymidine kinase activity, the second step in the activation of 5-FU.Hence the effect of IFN-α on PyNP-activity is likely a critical biochemical event that
modulates the cytotoxicity of 5-FU (258). IFN also alters the pharmacokinetics of 5-FU,inducing higher serum levels of 5-FU and increased drug exposure (262,263). In a clinical
trial, treatment of patients with advanced colorectal carcinoma with the combination of 5-FU
750 mg/m2/d for 5 days as a continuous infusion followed by weekly outpatient bolus therapyand IFN 9 MU subcutaneously starting day 1 and administered three times per week resulted
in objective tumor regression in 62% of patients (264). In a multi-institutional setting phaseII clinical trial by the Eastern Cooperative Oncology Group (ECOG) the addition of IFN to
5-FU enhanced the objective response rates achieved in patients with advanced colorectal
carcinoma with acceptable toxicities. IFN also enhances fluorouracil-induced toxicities,especially mucositis (265). The triple combination of 5-FU, IFN and Leucovorin was highly
active in patients with advanced colorectal cancer, at the cost of increased toxicity, mainlymucositis and diarrhea (262,266).
3.3.5 CarcinoidThe malignant carcinoid is a slowly growing tumor arising from cells of the neural crest that
are capable of amine precursor uptake and decarboxylation. Multiple small tumors in the gutor metastases in the liver may produce a variety of biological active peptides that can cause
the carcinoid syndrome, which includes severe diarrhea, cutaneous flushes, hypotension, and
cardiac valvular lesions. The primary form of treatment in this disease is surgery. When thetumor is unresectable or metastatic, chemotherapeutic approaches have been investigated, with
combination treatment of streptozocin and fluorouracil being the most effective regimenreported (267,268). Besides the symptomatic treatment with somatostatin analogues (269,270),
interferons have been investigated in the treatment of the malignant carcinoid. IFN-α, at doses
of 2.5 to 42 MU/week induced responses in 30% to 60% of the patients with reduction ofserum tumor marker levels and symptomatic improvement, rather than a reduction in tumor
size (271-278). Side effects, consisting of anorexia and fatigue, were observed inapproximately one third of the patients treated. These side effects were dose related and they
required dose reductions of IFN or discontinuation of treatment in a number of patients. Dose
escalation of IFN did not improve response rate (277). Low doses of 3 to 9 MU/d i.m. at least
34

3 times a week have been reported to have the best therapeutic index with prolongedsymptomatic improvement and tolerable toxicity.
3.3.6 Ovarian cancerDespite the improved results of platinum-based combination chemotherapy, local tumor
recurrence remains a major problem in the treatment of patients with ovarian cancer.Interferon has been used intraperitonally in patients with ascites from a local relapse. In three
studies, using high doses (50 MU) of IFN-α administered in 2 L dialysate, response rates up
to 52% were observed (279-281). When alternated with intraperitoneal cisplatin, a responserate of 50% was described in one study (282).
3.3.7 Bladder cancerTreatment of superficial bladder cancer with IFN administered intravesically has been
effective with complete responses against both carcinoma in situ and recurrent noninvasivelow-grade transitional cell carcinomas. In a phase II study intravesical instillations of
recombinant IFN-α, at a daily dose of 54 MU for 5 days for 2 consecutive weeks resulted ina response rate of 79% of patients. The median relapse time was 40 weeks, while clinical and
local tolerance were optimal (283).
3.3.8 Benign TumorsInterferon-α appears to induce the early regression of life-threatening corticosteroid-resistanthemangiomas including pulmonary hemangiomatosis of infancy (284,285).
3.4 TolerabillityThe clinical toxicity of interferon has been reviewed by Quesada (219) and Dorr (221). The
most common acute toxicity is a flu like syndrome with fever up to 38 to 40 C, startingwithin 6 hours after a parenteral dose and lasting for 4 to 8 hours, if untreated. Chills,
myalgias, arthralgias and headache may accompany the febrile reaction. These side effects can
be partially inhibited with acetaminophen. With repeated daily treatment the febrile reactionand accompanying symptoms usually decrease in intensity in seven to ten days. With
intermittent cyclic administration no such tachyphylaxis is observed, with symptomsfrequently reoccurring after re-exposure to IFN. Fatigue and anorexia are the most prominent
dose limiting toxicities of chronic interferon treatment. Alternate-day administration may be
better tolerated than daily administration in this setting. At high doses IFN can be neurotoxic,with symptoms of vertigo, confusion and decreased mental status. Severe IFN toxicities are
rare, but isolated reports of coma, cerebrovascular accidents have been reported.Hematological toxicity consists of mild leucopenia, and sometimes anemia and
thrombocytopenia. Few gastrointestinal symptoms are observed with low dose IFN (3-5
MU/day). With higher doses toxicity consisting of nausea, vomiting, and diarrhoea become
35

more prominent. Cardiovascular effects of IFN are uncommon and rarely serious. Elevationof serum transaminases may reflect hepatic toxicity. Renal toxicity is usually low, but severe
renal toxicities with reversible renal failure and nephrotic syndrome have been reported.
Interferon toxicity is dose related. In general, tolerance and compliance are excellent withdoses of 1-9 MU. At doses above 18 MU there is a significant increase in the incidence of
severe adverse effects particularly gastro-intestinal and neurological effects. Doses over 36MU are rarely tolerated for more than 8 weeks.
3.5 Conclusions and perspectivesThe clinical spectrum of IFN seems, as far as oncology is concerned to have almost
crystallized. It is an active agent in some hematological tumors, but usually alternatives areavailable. This is important considering its side effects and high costs. However in view of
the reversibility of these side effects, in contrast to those of many cytotoxic agents, doubtless
IFN-α will remain part of the armamentarium in the fight against cancer. In solid tumors itsplace is still uncertain, until now the only synergy that has reproducibly been found is that
with the cytostatic 5-FU. However, the possibilities to translate this into clinical practicedeserve further study.
References
1. Oldham R. Biotherapy: The 4th Modality of Cancer Treatment. J. Cell. Physiol. 1986; (Suppl),4: 91-99.2. Rosenberg SA. Karnofsky Memorial Lecture. The immunotherapy and gene therapy of cancer. J. Clin.
Oncol. 1992; 10: 180-199.3. Currie GA. Eighty years of immunotherapy: a review of immunological methods used for the treatment
of human cancer. Br. J. Cancer 1972; 26: 141-153.4. Wadler S. The role of interferons in the treatment of solid tumors. Cancer 1992; 70: 949-958.5. Hirschhorn K, Kolodny RL, Hashem N and Bach FH. Mitogen action of phytohaemagglutinin. Lancet
1963; i: 305-306.6. Morgan DA, Ruscetti FW and Gallo RC. Selective in vitro growth of T lymphocytes from normal
human bone marrows. Science 1976; 193: 1007-1008.7. Aarden LA, Brunner TK, Cerottini JC et al. Revised Nomenclature for Antigen-Nonspecific T Cell
Proliferation and Helper Factors. J. Immunol. 1979; 123: 2928-2929.8. Chanda PK, Chen GF, Baine Y, Leonard WJ, Greene WC, Chang TW and Chang NT. Expression of
human interleukin-2 receptor cDNA in E. coli. Biochem. Biophys. Res. Commun. 1986; 141: 804-811.9. Fujita T, Takaoka C, Matsui H and Taniguchi T. Structure of the human interleukin 2 gene. Proc. Natl.
Acad. Sci. U. S. A. 1983; 80: 7437-7441.10. Brandhuber BJ, Boone T, Kenney WC and McKay DB. Three-dimensional structure of interleukin-2.
Science 1987; 238: 1701-1709.11. Robb RJ, Kutny RM, Panico M, Morris HR and Chowdhry V. Amino acid sequence and
post-translational modification of human interleukin 2. Proc. Natl. Acad. Sci. U. S. A. 1984; 81:6486-6490.
12. Smith KA. Interleukin-2: inception, impact, and implications. Science 1988; 240: 1169-1176.13. Smith KA. Lowest dose interleukin-2 immunotherapy. Blood 1993; 81: 1414-1423.14. Vyth-Dreese FA, Van der Reijden HJ and De Vries JE. Phorbol-ester-mediated induction and
augmentation of mitogenesis and interleukin-2 production in human T-cell lymphoproliferative disease.
36

Blood 1982; 60: 1437-1446.15. Schwartz RH. Costimulation of T lymphocytes: The role of CD28, CTLA-4, and B7/BB1 in
interleukin-2 production and immunotherapy. Cell 1992; 71: 1065-1068.16. Townsend SE and Allison JP. Tumor rejection after direct costimulation of CD8+ T cells by B7-
transfected melanoma cells. Science 1993; 259: 368-370.17. Leonard WJ, Depper JM, Crabtree GR, Rudikoff S, Pumphrey J, Robb RJ, Kronke M, Svetlik PB,
Peffer NJ, Waldmann TA et al. Molecular cloning and expression of cDNAs for the human interleukin-2receptor. Nature 1984; 311: 626-631.
18. Nikaido T, Shimizu A, Ishida N, Sabe H, Teshigawara K, Maeda M, Uchiyama T, Yodoi J and HonjoT. Molecular cloning of cDNA encoding human interleukin-2 receptor. Nature 1984; 311: 631-635.
19. Hatakeyama M, Tsudo M, Minamoto S, Kono T, Doi T, Miyata T, Miyasaka M and Taniguchi T.Interleukin-2 receptorβ chain gene: Generation of three receptor forms by cloned humanα and βchain cDNA’s. Science 1992; 257: 379.
20. Takeshita T, Asao H, Ohtani K, Ishii N, Kumaki S, Tanaka N, Munakata H, Nakamura M andSugamura K. Cloning of theτ chain of the human IL-2 receptor. Science 1992; 257: 379.
21. Ritz J, Schmidt RE, Michon J, Hercend T and Schlossman SF. Characterization of functional surfacestructures on human natural killer cells. Adv. Immunol. 1988; 42: 181-211.
22. Wang HM and Smith KA. The interleukin-2 receptor: Functional consequenses of its bimolecularstructure. J. Exp. Med. 1981; 154: 1455-1474.
23. Hatfield SM. Cyclosporine and FK506 inhibition of murine mast cell cytokine production. J. Pharmacol.Exp. Ther. 1992; 260: 680-688.
24. Rubin LA and Nelson DL. The soluble interleukin-2 receptor: biology, function, and clinical application.Ann. Intern. Med. 1990; 113: 619-627.
25. Lissoni P, Tisi E, Brivio F, Barni S, Rovelli F, Perego M and Tancini G. Increase in solubleinterleukin-2 receptor and neopterin serum levels during immunotherapy of cancer with interleukin-2.Eur. J. Cancer 1991; 27: 1014-1016.
26. Lissoni P, Barni S, Tisi E, Rovelli F, Pittalis S, Rescaldani R, Vigore L, Biondi A, Ardizzoia A andTancini G. In vivo biological results of the association between interleukin-2 and interleukin-3 in theimmunotherapy of cancer. Eur. J. Cancer 1993; 29A: 1127-1132.
27. Grimm EA, Mazumder A, Zhang HZ and Rosenberg SA. Lymphokine-activated killer cell phenomenon.Lysis of natural killer-resistant fresh solid tumor cells by interleukin 2- activated autologous humanperipheral blood lymphocytes. J. Exp. Med. 1982; 155: 1823-1841.
28. Pfizenmaier K, Scheurich P, Daubener W, Kronke M, Rollinghoff M and Wagner H. Quantitativerepresentation of all T cells committed to develop into cytotoxic effector cells and/or interleukin 2activity- producing helper cells within murine T lymphocyte subsets. Eur. J. Immunol. 1984; 14: 33-39.
29. Lotze MT, Grimm EA, Mazumder A, Strausser JL and Rosenberg SA. Lysis of fresh and culturedautologous tumor by lymphocytes cultured in T-cell growth factor. Cancer Res. 1981; 41: 4420-4425.
30. Rosenberg SA, Spiess PJ and Lafreniere R. A new approach to the adoptive immunotherapy of cancerwith tumor infiltrating lymphocytes. Science 1986; 233: 1318-1321.
31. Ortaldo JR, Mason AT, Gerard JP, Henderson LE, Farrar W, Hopkins RF, Herberman RB and RabinH. Effects of natural and recombinant IL 2 on regulation of IFN gamma production and natural killeractivity: lack of involvement of the Tac antigen for these immunoregulatory effects. J. Immunol. 1984;133: 779-783.
32. Saraya KA and Balkwill FR. Temporal sequence and cellular origin of interleukin-2 stimulated cytokinegene expression. Br. J. Cancer 1993; 67: 514-521.
33. Kovacs EJ, Becker SK, Longo DL, Versio L and Young HA. Cytokine gene expression during thegenration of lymphokine activated killer cells: early induction of IL-1β by IL-2. Cancer Res. 1989; 49:940-944.
34. Schaafsma MR, Falkenburg JH, Landegent JE, Duinkerken N, Osanto S, Ralph P, Kaushansky K,Wagemaker G, Van Damme J, Willemze R and Fibbe WE. In vivo production of interleukin-5,granulocyte-macrophage colony-stimulating factor, macrophages colony-stimulating factor, andinterleukin-6 during intravenous administration of high-dose interleukin-2 in cancer patients seecomments. Blood 1991; 78: 1981-1987.
35. Donohue JH, Rosenstein M, Chang AE, Lotze MT, Robb RJ and Rosenberg SA. The systemicadministration of purified interleukin 2 enhances the ability of sensitized murine lymphocytes to cure
37

a disseminated syngeneic lymphoma. J. Immunol. 1984; 132: 2123-2128.36. Thompson JA, Peace DJ, Klarnet JP, Kern DE, Greenberg PD and Cheever MA. Eradication of
disseminated murine leukemia by treatment with high-dose interleukin 2. J. Immunol. 1986; 137:3675-3680.
37. Rosenberg SA, Mule JJ, Spiess PJ, Reichert CM and Schwarz SL. Regression of established pulmonarymetastases and subcutaneous tumour mediated by the systemic administration of high-dose recombinantinterleukin 2. J. Exp. Med. 1985; 161: 1169-1188.
38. Mule JJ, Shu S, Schwarz SL and Rosenberg SA. Adoptive immunotherapy of established pulmonarymetastases with LAK cells and recombinant interleukin-2. Science 1984; 225: 1487-1489.
39. Mazumder A and Rosenberg SA. Successful immunotherapy of natural killer-resistant establishedpulmonary melanoma metastases by the intravenous adoptive transfer of syngeneic lymphocytesactivated in vitro by interleukin 2. J. Exp. Med. 1984; 159: 495-507.
40. Lafreniere R and Rosenberg SA. Succesful immunotherapy of murine experimental hepatic metastaseswith lymphokine-activated killer cells and recombinant interleukin-2. Cancer Res. 1985; 45: 3735-3741.
41. Donohue JH, Lotze MT, Robb RJ, Rosenstein M, Braziel RM, Jaffe ES and Rosenberg SA. In vivoadministration of purified Jurkat-derived interleukin 2 in mice. Cancer Res. 1984; 44: 1380-1386.
42. Chang AE, Hyatt CL and Rosenberg SA. Systemic administration of recombinant human interleukin2 in mice. J. Biol. Resp. Mod. 1984; 3: 561-572.
43. Cheever MA, Thompson JA, Kern DE and Greenberg PD. Interleukin-2 (IL-2) administered in vivo:influence of IL-2 route and timing on T cell growth. J. Immunol. 1985; 134: 3895-3899.
44. Mule JJ, Shu S and Rosenberg SA. The anti-tumor efficacy of lymphokine-activated killer cells andrecombinant interleukin 2 in vivo. J. Immunol. 1985; 135: 646-652.
45. Ettinghausen SE and Rosenberg SA. Immunotherapy of murine sarcomas using lymphokine activatedkiller cells: optimization of the schedue and route of administration of recombinant interleukin 2. CancerRes. 1986; 46: 2784-2792.
46. Mule JJ, Yang JC, Lafreniere R, Shu S and Rosenberg SA. Identification of cellular mechanismsoperational in vivo during the regression of esthablished pulmonary metastases by the systemicadministration of high dose recombinant interleukin 2. J. Immunol. 1987; 139: 285-294.
47. Talmadge JE, Phillips H, Schindler J, Tribble H and Pennington R. Systemic Preclinical Study of theTherapeutic Properties of Recombinant Human Interleukin 2 for the Treatment of Metastatic Disease.Cancer Res. 1987; 47: 5725-5732.
48. Maas RA, Dullens HF, De Jong WH and Den Otter W. Immunotherapy of mice with a large burdenof disseminated lymphoma with low-dose interleukin 2. Cancer Res. 1989; 49: 7037-7040.
49. Forni G, Giovarelli M, Santoni A, Modesti A and Forni M. Tumour inhibition by interleukin-2 at thetumour/host interface. Biochim. Biophys. Acta 1986; 865: 307-327.
50. Felgar RE and Hiserodt JC. In vivo migration and tissue localization of highly purifiedlymphokine-activated killer cells (A-LAK cells) in tumor-bearing rats. Cell. Immunol. 1990; 129:288-298.
51. Griffith KD, Read EJ, Carrasquillo JA, Carter CS, Yang JC, Fisher B, Aebersold P, Packard BS, YuMY and Rosenberg SA. In vivo distribution of adoptively transferred indium-111- labeled tumorinfiltrating lymphocytes and peripheral blood lymphocytes in patients with metastatic melanoma. J. Natl.Cancer Inst. 1989; 81: 1709-1717.
52. Fisher B, Packard BS, Carrasquillo JA, Carter CS, Topalian SL, Yang JC, Yolles P, Larson SM andRosenberg SA. Tumor localization of adoptively transferred indium-111 labeled tumor infiltratinglymphocytes in patients with metastatic melanoma. J. Clin. Oncol. 1989; 7: 250-261.
53. Yoshino I, Yano T, Murata M, Ishida T, Sugimachi K, Kimura G and Nomoto K. Tumor-reactiveT-cells accumulate in lung cancer tissues but fail to respond due to tumor cell-derived factor. CancerRes. 1992; 52: 775-781.
54. Alexander JP, Kudoh S, Melsop KA, Hamilton TA, Edinger MG, Tubbs RR, Sica D, Tuason L, KleinE, Bukowski RM and Finke JH. T cells infiltrating renal cell carcinoma display a poor proliferativeresponse even though they can produce interleukin 2 and express interleukin 2 receptors. Cancer Res.1993; 53: 1380-1387.
55. Miescher S, Whiteside TL, Carrel S and Von Fliedner V. Functional properties of tumor-infiltrating andblood lymphocytes in patients with solid tumors: effects of tumor cells and their supernatants onproliferative responses of lymphocytes. J. Immunol. 1986; 136: 1899-1907.
38

56. Konrad MW, Hemstreet G, Hersh EM, Mansell PWA, Mertelsmann R, Kolitz JE and Bradley EC.Pharmacokinetics of recombinant interleukin 2 in humans. Cancer Res. 1990; 50: 2009-2017.
57. Donohue JH and Rosenberg SA. The fate of interleukin 2 after in vivo administration. J. Immunol.1983; 130: 2203-2208.
58. Gustavson LE, Nadeau RW and Oldfield NF. Pharmacokinetics of Teceleukin (recombinantinterleukin-2) after intravenous or subcutaneous administration to patients with cancer. J. Biol. Resp.Mod. 1989; 8: 440-449.
59. Lamers CHJ, Stoter G, Goey SH, Oosterom R and Bolhuis RLH. Bioavailabillity of interleukin-2 afterreconstitution with albumin. Correspondence. Lancet 1992; 340: 241.
60. Vlasveld LT, Beijnen JH, Sein JJ, Rankin EM, Melief CJM and Hekman A. Reconstitution ofrecombinant interleukin-2 (rIL-2): a comparative study of various rIL-2 Muteins. Eur. J. Cancer 1993;29A: 1977-1979.
61. Huland E, Huland H and Heinzer H. Interleukin-2 by inhalation: Local therapy for metastatic renal cellcarcinoma. J. Urol. 1992; 147: 344-348.
62. Pizza G, Severini G, Menniti D, De Vinci C and Corrado F. Tumour regression after intralesionalinjection of interleukin 2 (IL-2) in bladder cancer. Preliminary report. Int. J. Cancer 1984; 34: 359-367.
63. Zimmerman RJ. Schedule dependency of the antitumor activity and toxicity of polyethyleneglycol-modified interleukin 2 in murine tumor models. Cancer Res. 1989; 49: 6521-6528.
64. Feruglio C, Zambello R, Trentin L, Bulian P, Franceschi T, Cetto GL and Semenzato G. Cytotoxic invitro function in patients with metastatic renal cell carcinoma before and after alpha-2b-interferontherapy. Effects of activation with recombinant interleukin-2. Cancer 1992; 69: 2525-2531.
65. Matsuoka J, Sakagami K, Higaki K, Idani H, Fujiwara T, Kaneshige T and Orita K. Site directedimmunotherapy by intratumoral administrations of slow delivery system of interleukin 2: A pilot studyin 14 breast cancer patients. Proc. Am. Assoc. Cancer Res. 1993; 12: 934. (Abstract)
66. Rosenberg SA, Lotze MT, Yang JC, Aebersold PM, Linehan WM, Seipp CA and White DE. Experiencewith the use of high-dose interleukin-2 in the treatment of 652 cancer patients. Ann. Surg. 1989; 210:474-485.
67. Dillman RO, Church C, Oldham RK, West WH, Schwartzberg L and Birch R. Inpatientcontinuous-infusion interleukin-2 in 788 patients with cancer. The National Biotherapy Study Groupexperience. Cancer 1993; 71: 2358-2370.
68. Stewart JA, Belinson JL, Moore AL, Dorighi JA, Grant BW, Haugh LD, Roberts JD, Albertini RJ andBranda RF. Phase I trial of intraperitoneal recombinant interleukin- 2/lymphokine-activated killer cellsin patients with ovarian cancer. Cancer Res. 1990; 50: 6302-6310.
69. Steis RG, Urba WJ, VanderMolen LA, Bookman MA, Smith JW, Clark JW, Miller RL, Crum ED,Beckner SK, McKnight JE, Ozols RF, Stevenson HC, Young RC and Longo DL. Intraperitoneallymphokine-activated killer-cell and interleukin- 2 therapy for malignancies limited to the peritonealcavity. J. Clin. Oncol. 1990; 8: 1618-1629.
70. Huland E and Huland H. Local continuous high dose interleukin 2: a new therapeutic model for thetreatment of advanced bladder carcinoma. Cancer Res. 1989; 49: 5469-5474.
71. Clamon G, Herndon J, Perry MC, Ozer H, Kreisman H, Maher T, Ellerton J and Green MR.Interleukin-2 activity in patients with extensive small-cell lung cancer: A phase II trial of caner andleukemia group B. J. Natl. Cancer Inst. 1993; 85: 316-320.
72. Lotze MT, Custer MC and Rosenberg SA. Intraperitoneal administration of interleukin-2 in patients withcancer. Arch. Surg. 1986; 121: 1373-1379.
73. Berek JS. Intraperitoneal adoptive immunotherapy for peritoneal cancer. editorial. J. Clin. Oncol. 1990;8: 1610-1612.
74. Viallat JR, Boutin C, Rey F, Astoul Ph, Farisse P and Brandely M. Intrapleural immunotherapy withescalating doses of interleukin-2 in metastatic pleural effusions. Cancer 1993; 71: 4067-4071.
75. List J, Moser RP, Steuer M, Loudon WG, Blacklock JB and Grimm EA. Cytokine responses tointraventricular injection of interleukin 2 into patients with leptomeningeal carcinomatosis: rapidinduction of tumor necrosis factor alpha, interleukin 1 beta, interleukin 6, gamma-interferon, and solubleinterleukin 2 receptor (Mr 55,000 protein). Cancer Res. 1992; 52: 1123-1128.
76. Galvani DW, Walton S, Davies JM, Owen RR, Carr R et al. Endolymphatic delivery of IL2 in patientswith melanoma and lymphoma. Biotherapy 1992; 4: 251-255.
77. Belli F, Arienti F, Rivoltini L, Santinamini M, Mascheroni L et al. Treatment of recurrent in transit
39

metastases from cutaneous melanoma by isolation perfusion in extracorporal circulation withinterleukin-2 and lymphokine activated killer cells. A pilot study. Melanoma. Res 1992; 2: 263-271.
78. Keilholz U, Schlag P, Tilgen W, Brado B, Galm F, Görich J, Kauffmann GW, Möller P, Schneider Sand Hunstein W. Regional administration of lymphokine-activated killer cells can be superior tointravenous application. Cancer 1992; 69: 2172-2175.
79. Klasa RJ, Silver HKB and Kong S. In vivo induction of lymphokine activated killer cells byinterleukin-2 splenic artery perfusion in advanced malignancy. Cancer Res. 1990; 50: 4906-4910.
80. Weiss GR, Margolin KA, Aronson FR, Sznol M, Atkins MB, Dutcher JP, Gaynor ER, Boldt DH,Doroshow JH, Bar MH, Hawkins MJ, Demchak PA, Gucalp R and Fisher RI. A randomized phase IItrial of continuous infusion interleukin-2 or bolus injection interleukin-2 plus lymphokine-activated killercells for advanced renal cell carcinoma. J. Clin. Oncol. 1992; 10: 275-281.
81. Sosman JA, Kohler PC, Hank JA, Moore KH, Bechhofer R, Storer B and Sondel PM. Repetitive weeklycycles of interleukin-2. II. clinical and immunologic effects of dose, schedule, and addition ofindomethacin. J. Natl. Cancer Inst. 1988; 80: 1451-1461.
82. Fisher RI, Coltman CA, Doroshow JH, Rayner AA, Hawkins MJ, Mier JW, Wiernik P, McMannis JD,Weiss GR, Margolin KA, Gemlo BT, Hoth DF, Parkinson DR and Paietta E. Metastatic renal cancertreated with interleukin-2 and lymphokine activated killer cells. Ann. Intern. Med. 1988; 108: 518-523.
83. Negrier S, Philip T, Stoter G, Fossa SD, Janssen S, Iacone A, Cleton FS, Eremin O, Israel L, JasminC, Rugarli C, Masse HVD, Thatcher N, Symann M, Bartsch HH, et al. Interleukin-2 with or withoutLAK cells in metastatic renal cell carcinoma: A report of a European multicenter study. Eur. J. Cancerand Clin. Oncol. 1989; 25(suppl. 3): S21-S28.
84. West WH. Continuous infusion recombinant interleukin-2 (rIL-2) and adoptive cellular therapy of renalcell carcinoma and other molignancies. Cancer Treat. Rev. 1989; 16(supp. A): 83-89.
85. Dillman RO, Barth NM, Oldham RK et al. Continuous interleukin-2 and lymphokine activated killercells in advanced cancer. Proc. Am. Soc. Clin. Oncol. 1989; 8: 188. (Abstract)
86. Bajorin DF, Sell K, Richards JM et al. A randomized trial of interleukin-2 plus lymphokine activatedkiller cells versus interleukin-2 alone in renal cell carcinoma. Proc. Am. Assoc. Cancer Res. 1990; 31:186. (Abstract)
87. Bukowski RM, Goodman P, Crawford ED, Sergi JS, Redman BG and Whitehead RP. Phase II trial ofhigh-dose intermittent interleukin-2 in metastatic renal cell carcinoma: A Southwest Oncology GroupStudy. J. Natl. Cancer Inst. 1990; 82: 143-146.
88. Parkinson DR, Fisher RI, Rayner AA, Paietta E, Margolin KA, Weiss GR, Mier JW, Sznol M, GaynorER, Bar MH, Gucalp R, Boldt DH, Mills B and Hawkins MJ. Therapy of renal cell carcinoma withinterleukin-2 and lymphokine-activated killer cells: Phase II experience with a hybrid bolus andcontinuous infusion interleukin-2 regimen. J. Clin. Oncol. 1990; 8: 1630-1636.
89. Gaynor ER, Weiss GR, Margolin KA et al. Phase I study of high-dose recombinant interleukin-2 andautologous lymphokine activated killer cells in patients with metastatic or unresectable malignantmelanoma and renal cell carcinoma. J. Natl. Cancer Inst. 1990; 82: 1397-1402.
90. Von der Maase H, Geertsen PF, Thatcher N, Jasmin C, Marcatello A, Fosså SD, Symann M, Stoter G,Nagel G, Israel L, Oskam R, Palmer P and Franks CR. Recombinant interleukin-2 in metastatic renalcell carcinoma. A European multicenter phase II study. Eur. J. Cancer 1991; 27: 1583-1589.
91. Douillard JY, Chevreau C, Perrocheau G, Mignot L, Tueni E, Lanson Y, Namer M, Mangin P, SuretJY, Burki F and Brandely M. Phase II trial of interleukin II (rIL2) for metastatic renal cell carcinoma.Eur. J. Cancer 1991; 27 (suppl. 2): S99. (Abstract)
92. Sorio R, Galligioni E, Sacco C, Errante D, Freschi A, Quaia M, Spada A, Santarosa M, Franchini M,Morassut S, Monfardini S and Aviano CRO. Recombinant interleukin-2 (rIL-2) by continuous infusion(CI) in 20 patients with advanced renal cell cancer (RCC). Eur. J. Cancer 1991; 27 (suppl. 2): S98.(Abstract)
93. Koretz MJ, Lawson DH, York RM, Graham SD, Murray DR, Gillespie TM, Levitt D and Sell KM.Randomized study of interleukin 2 (IL-2) alone vs IL-2 plus lymphokine-activated killer cells fortreatment of melanoma and renal cell cancer. Arch. Surg. 1991; 126: 898-903.
94. Escudier B, Rossi JF, Ravaud A, Douillard JY, Negrier S, Baume D, Dorval T, Chevreau C, MignotL, Pein F, Fargeot P, Lesimple T and Brandely M. French expirience of high dose IL2 on a two-daysa week schedule in metastatic renal cell carcinoma: a multicenter study. Proc. Am. Soc. Clin. Oncol.1992; 11: 651. (Abstract)
40

95. Sleijfer DTh, Janssen RAJ, Willemse PHB, Martens A, Leij de L, De Vries EGE and Mulder NH.Low-dose regimen of interleukin-2 for metastatic renal carcinoma. Lancet 1990; 335: 1522-1523.
96. Negrier S, Mercatello A, Bret M, Thiesse P, Blay JY, Coronel B, Merrouche Y, Oskam R, Franks CR,Clavel M, Moskovtchenko JF and Philip T. Intravenous interleukin-2 in patients over 65 with metastaticrenal carcinoma. Br. J. Cancer 1992; 65: 723-726.
97. Palmer PA, Vinke J, Evers P, Pourreau C, Oskam R and Roest G. Continuous infusion of recombinantinterleukin-2 with or without autologous lymphokine activated killer cells for the treatment of advancedrenal cell carcinoma. Eur. J. Cancer 1992; 67: 1038-1044.
98. Geertsen PF, Hermann GG, Von der Maase H and Steven K. Treatment of metastatic renal cellcarcinoma by continuous intravenous infusion of recombinant interleukin-2: a single- center phase IIstudy. J. Clin. Oncol. 1992; 10: 753-759.
99. Thompson JA, Shulman KL, Benyunes MC, Lindgren CG, Collins C, Lange PH, Bush WH,Jr., BenzLA and Fefer A. Prolonged continuous intravenous infusion interleukin-2 and lymphokine-activatedkiller-cell therapy for metastatic renal cell carcinoma. J. Clin. Oncol. 1992; 10: 960-968.
100. Atkins MB, Sparano JA, Fisher RI, Weiss GR, Margolin KA, Fink KI, Rubinstein L, Louie A, MierJW, Gucalp R, Sosman JA, Boldt DH, Doroshow JH, Aronson FR and Sznol M. Randomized phaseII trial of high-dose interleukin-2 either alone or in combination with interferon alfa-2b in advancedrenal cell carcinoma. J. Clin. Oncol. 1993; 11: 661-670.
101. Rosenberg SA, Lotze MT, Yang JC, Topalian SL, Chang AE, Schwartzentruber DJ, Aebersold P,Leitman S, Linehan WM, Seipp CA, White DE and Steinberg SM. Prospective randomized trial ofhigh-dose interleukin-2 alone or in conjunction with lymphokine-activated killer cells for the treatmentof patients with advanced cancer. J. Natl. Cancer Inst. 1993; 85: 622-632.
101a. Rosenberg SA, Yang JC, Topalian SL, Schwartzentruber DJ, Weber JS, Parkinson DR, Seipp CA,Einhorn JH and White DE. Treatment of 283 consecutive patients with metastatic melanoma or renalcell cancer using high-dose-bolus interleukin-2. JAMA 1994; 271: 907-913.
102. Kuebler JP, Whitehead RP, Ward DL, Hemstreet GPIII and Bradley EC. Treatment of metastatic renalcell carcinoma with recombinant interleukin-2 in combination with vinblastine or lyphokine-activatedkiller cells. J. Urol. 1993; 150: 814-820.
103. Lopez M, Carpano S, Cancrini A, Marcellini M, Del Medico P, Rinaldi M and Vici P. Interleukin-2(IL-2) by cintinuous intravenous infusion (CIV) in advanced renal cell carcinoma (RCC). Proc. Am.Soc. Clin. Oncol. 1993; 12: 251. (Abstract)
104. Whitehead RP, Wilf MK, Solanki DL, Benedetto P, Flanigan RC and Craword ED. A phase II trial ofcontinuous infusion recombinant interleukin-2 (rIL-2) in patients with advanced renal cell carcinoma:A Southwest oncology group study. Proc. Am. Soc. Clin. Oncol. 1993; 12: 253. (Abstract)
105. Thatcher N, Dazzi H, Gosh A and Johnson RJ. Recombinant IL-2 given intra-splenically andintravenously in advanced malignant melanoma: a phase I/II study. Cancer Treat. Rev. 1989; 16 (Suppl.A): 49-52.
106. Dutcher JP, Creekmore SP, Weiss GR, Margolin K, Markowitz AB, Roper M, Parkinson D, CiobanuN, Fisher RI, Boldt DH, Doroshow JH, Rayner AA, Hawkins MJ and Atkins M. A phase II study ofinterleukin-2 and lymphokine-activated killer cells in patients with metastatic malignant melanoma. J.Clin. Oncol. 1989; 7: 477-485.
107. Bar MH, Sznol M, Atkins MB, Ciobanu N, Micetich KC et al. Metastatic malignant melanoma treatedwith combined bolus and continuous infusion interleukin-2 and lymphokine-activated killer cells. J. Clin.Oncol. 1990; 8: 1138-1147.
108. Whitehead RP, Kopecky KJ, Samson MK, Constanzi JJ, Natale RB, Feun LG, Hersh EM and RinehartJJ. Phase II study of intravenous bolus recombinant interleukin-2 in advanced malignant melanoma:Southwest Oncology Group study. J. Natl. Cancer Inst. 1991; 83: 1250-1251.
109. Dutcher JP, Gaynor ER, Boldt DH, Doroshow JH, Bar MH, Sznol M, Mier J, Sparano J, Fisher RI,Weiss G et al. A phase II study of high-dose continuous infusion interleukin-2 withlymphokine-activated killer cells in patients with metastatic melanoma. J. Clin. Oncol. 1991; 9: 641-648.
110. Dorval T, Fridman WH, Mathiot C and Pouillart P. Interleukin-2 therapy for metastatic uvealmelanoma. Eur. J. Cancer 1992; 28A: 2087.
111. Sparano JA, Micetich KC, Sunderland M, Margolin K, Aronson F, Sznol M and Rubinstein LV. Arandomized Phase III trial of treatment with high-dose interleukin-2 (IL-2) either alone or in
41

combination with interferonα-2a (IFN) in patients with advanced melanoma. Proc. Am. Soc. Clin.Oncol. 1993; 12: 1332. (Abstract)
112. Sznol M, Clark JW, Smith JW, Steis RG, Urba WJ, Rubinstein LV, VanderMolen LA, Janik J,Sharfman WH, Fenton RG, Creekmore SP, Kremers P, Conlon K, Hursey J, Beveridge J, et al. Pilotstudy of interleukin-2 and lymphokine-activated killer cells combined with immunomodulatory dosesof chemotherapy and sequenced with interferon alfa-2a in patients with metastatic melanoma and renalcell carcinoma. J. Natl. Cancer Inst. 1992; 84: 929-937.
113. Marincola FM, Venzon D, White D, Rubin JT, Lotze MT, Simonis TB, Balkissoon J, Rosenberg SAand Parkinson DR. HLA association with response and toxicity in melanoma patients treated withInterleukin-2 based immunotherapy. Cancer Res. 1992; 52: 6561-6566.
114. Rosenberg SA, Packard BS, Aebersold PM, Solomon D, Topalian SL, Toy ST, Simon P, Lotze MT,Yang JC, Seipp CA, Simpson C, Carter C, Bock S, Schwartzentruber D, Wei JP, et al. Use oftumor-infiltrating lymphocytes and interleukin-2 in the immunotherapy of patients with metastaticmelanoma: A preliminary report. N. Engl. J. Med. 1988; 319: 1676-1680.
115. Dillman RO, Oldham RK, Barth NM, Cohen RJ, Minor DR, Birch R, Yanelli JR, Maleckar JR,Sferruzza A, Arnold J and West WH. Continuous interleukin-2 and tumor-infiltrating lymphocytes astreatment of advanced melanoma. Cancer 1991; 68: 1-8.
116. Bukowski RM, Sharfman W, Murthy S, Rayman P, Tubbs R, Alexander J, Budd GT, Sergi JS, BauerL, Gibson V, Stanley J, Boyett J, Pontes E and Finke J. Clinical results and characterization oftumor-infiltrating lymphocytes with or without recombinant interleukin 2 in human metastatic renal cellcarcinoma. Cancer Res. 1991; 51: 4199-4205.
117. Baars JW, Fonk JC, Scheper RJ, Von Blomberg-Van der Flier ME, Bril H, Van der Valk P, Pinedo HMand Wagstaff J. Treatment with tumour infiltrating lymphocytes and interleukin-2 in patient withmetastatic melanoma: A pilot study. Biotherapy 1992; 4: 289-297.
118. Peto R, Pike MC, Armitage J, Breslow NE, Cox DR, Howard SV, Mantel N, McPherson K, Peto J andSmith PG. Design and analysis of randomized clinical trials requiring prolongued observation of eachpatient. I. Introduction and design. Br. J. Cancer 1976; 34: 585-612.
119. Peto R, Pike MC, Armitage J, Breslow NE, Cox DR, Howard SV, Mantel N, McPherson K, Peto J andSmith PG. Design and analysis of randomized clinical trials requiring prolongued observation of eachpatient. II. Analysis and examples. Br. J. Cancer 1977; 35: 1-39.
120. deKernion JB, Ramming KP and Smith RB. The natural history of metastatic renal cell carcinoma: acomputer analysis. J. Urol. 1978; 120: 148-152.
121. Philip T, Negrier S, Lasset C, Coronel B, Bret M, Blay JY, Merrouche Y, Carrie C, Kaemmerlen P,Chauvin F, Favrot M, Oskam R, Tabah I, Clavel M, Moskovtchenko JF, et al. Patients with metastaticrenal carcinoma candidate for immunotherapy with cytokines. Alanysis of a single institution study on181 patients. Br. J. Cancer 1993; 68: 1036-1042.
122. West WH, Tauer KW, Yanelli JR, Marshall GD, Orr DW, Thurman GD and Oldham RK. Constantinfusion recombinant interleukin-2 in adoptive immunotherapy of advanced cancer. N. Engl. J. Med.1987; 316: 898-905.
123. Janssen RAJ, Sleijfer DTh, Heijn AA, Mulder NH, The TH and Leij de L. Peripheral blood lymphocytenumber and phenotype prior to therapy correlate with response in subcutaneously applied rIL-2 therapyof renal cell carcinoma. Br. J. Cancer 1992; 66: 1177-1179.
124. Arinaga S, Karimine N, Takamuku K, Nanbara S, Inoue H, Abe R, Watanabe D, Matsuoka H, Ueo Hand Akiyoshi T. Correlation of eosinophilia with clinical response in patients with advanced carcinomatreated with low-dose recombinant interleukin-2 and mitomycin C. Cancer Immunol. Immunother. 1992;35: 246-250.
125. Hanninen EL, Korfer A, Hadam M, Schneekloth C, Dallmann I, Menzel T, Kirchner H, Poliwoda Hand Atzpodien J. Biological monitoring of low-dose interleukin 2 in humans: soluble interleukin 2receptors, cytokines, and cell surface phenotypes. Cancer Res. 1991; 51: 6312-6316.
126. Blay JY, Favrot MC, Negrier S, Combaret V, Chouaib S, Mercatello A, Kaemmerlen P, Franks CR andPhilip T. Correlation between clinical response to IL-2 therapy and sustained production of TNF. CancerRes. 1990; 50: 2371-2374.
127. Martens A, Janssen RAJ, Sleijfer DTh, Heijn AA, Mulder NH, The TH and De Leij L. Early sCD8plasma levels during subcutaneous rIL-2 therapy in patients with renal cell carcinoma correlate withresponse. Br. J. Cancer 1993; 67: 1118-1121.
42

128. Broom J, Heys SD, Whiting PH, Park KGM, Strachan A, Rothnie I, Franks CR and Eremin O.Interleukin 2 therapy in cancer: identification of responders. Br. J. Cancer 1992; 66: 1185-1187.
129. Blay JY, Negrier S, Combaret V, Attali S, Goillot E, Merrouche Y, Mercatello A, Ravault A, TouraniJM, Moskovtchenko JF and Philip T. Serum level of interleukin 6 as a prognosis factor in metastaticrenal cell carcinoma. Cancer Res. 1992; 52: 3317-3322.
130. Atzpodien J and Kirchner H. The out-patient use of recombinant human interleukin-2 and interferonalfa-2b in advanced malignancies. Eur. J. Cancer 1991; 27 Suppl 4P S88-91;:
131. Lotze MT, Chang AE, Seipp CA, Simpson C, Vetto JT and Rosenberg SA. High-dose recombinantinterleukin 2 in the treatment of patients with disseminated cancer. Responses, treatment-relatedmorbidity, and histologic findings. JAMA 1986; 256: 3117-3124.
132. Rosenberg SA, Lotze MT, Muul LM, Chang AE, Avis FP, Leitman S, Lineham WM, Robertson CN,Lee RE, Rubin JT, Seipp CA, Simpson CG and White DE. A progress report on the treatment of 157patients with advanced cancer using lymphokine-activated killer cells and interleukin-2 or high-doseinterleukin-2 alone. N. Engl. J. Med. 1987; 316: 889-897.
133. Economou JS, Hoban M, Lee JD, Essner R, Swisher S, McBride W, Hoon DB and Morton DL.Production of tumor necrosis factor alpha and interferon gamma in interleukin-2-treated melanomapatients: correlation with clinical toxicity. Cancer Immunol. Immunother. 1991; 34: 49-52.
134. Ochoa JB, Curti B, Peitzman AB, Simmons RL, Billiar TR, Hoffman R, Rault R, Longo DL, Urba WJand Ochoa AC. Increased circulating nitrogen oxides after human tumor immunotherapy: correlationwith toxic hemodynamic changes published erratum appears in J Natl Cancer Inst 1992 Aug 19;84(16):1291. J. Natl. Cancer Inst. 1992; 84: 864-867.
135. Fraker DL, Langstein HN and Norton JA. Passive immunization against tumor necrosis factor partiallyabrogates interleukin-2 toxicity. J. Exp. Med. 1989; 170: 1015-1020.
136. Kilbourn RG, Logothesis CJ, Striegel A and Griffith OW. Interleukin-2 (IL-2) mediated hypotensionin humans is reversed by NG-monomethyl-L-arginine (NMA) an inhibitor of nitric oxide (NO-)production. Proc. Am. Soc. Clin. Oncol. 1993; 12: 759. (Abstract)
137. Siegel JP and Puri RK. Interleukin-2 toxicity. J. Clin. Oncol. 1991; 9: 694-704.138. Margolin KA, Rayner AA, Hawkins MJ, Atkins MB, Dutcher JP, Fisher RI, Weiss GR, Doroshow JH,
Jaffe HS, Roper M, Parkinson DR, Wiernik PH, Creekmore SP and Boldt DH. Interleukin-2 andlymphokine-activated killer cell therapy of solid tumors: analysis of toxicity and management guidelines.J. Clin. Oncol. 1989; 7: 486-498.
139. Lee RE, Lotze MT, skibber JM, Tucker E, Bonow RO et al. Cardiorespiratory efects of immunotherapywith interleukin-2. J. Clin. Oncol. 1989; 7: 7-20.
140. Ognibene FP, Rosenberg SA, Lotze MT et al. Interleukin-2 administration causes reversiblehemodynamic changes and left ventricular dysfunction similar to those seen in septic shock. Chest 1988;94: 750-754.
141. Nora R, Abrams JS, Tait NS, Hiponia DJ and Silverman HI. Myocardial toxic effects duringrecombinant interleukin-2 therapy. J. Natl. Cancer Inst. 1989; 81: 59-63.
142. Osanto S, Cluitmans FH, Franks CR, Bosker HA and Cleton FJ. Myocardial injury after interleukin-2therappy. Lancet 1988; 11: 48-49.
143. Gaynor ER, Vitek L and Sticklin L. The haemodynamic effects of treatment with interleukin-2 andLymphokine Activated Killer cells. Ann. Intern. Med. 1988; 109: 953-958.
144. Hibbs JB,Jr., Westenfelder C, Taintor R, Vavrin Z, Kablitz C, Baranowski RL, Ward JH, Menlove RL,McMurry MP, Kushner JP and Samlowski WE. Evidence for cytokine-inducible nitric oxide synthesisfrom L- arginine in patients receiving interleukin-2 therapy. J. Clin. Invest. 1992; 89: 867-877.
145. Belldegrun A, Webb DE, Austin III HA, Steinberg SM, White DE, Linehan WM and Rosenberg SA.Effects of interleukin-2 on renal function in patients receiving immunotherapy for advanced cancer.Ann. Intern. Med. 1987; 106: 817-822.
146. Shalmi CL, Dutcher JP, Feinfeld DA, Chun KJ, Saleemi KR, Freeman LM, Lynn RI and Wiernik PH.Acute renal dysfunction during interleukin-2 treatment: suggestion of an intrinsic renal lesion. J. Clin.Oncol. 1990; 8: 1839-1846.
147. Webb DE, Austin III HA, Belldegrun A et al. Metabolic and renal effects of interleukin-2immunotherapy for metastatic cancer. Clin. Nephr. 1988; 30: 141-145.
148. Belldegrun A, Webb DE, Austin III HA, Steinberg SM, Lineham WM and Rosenberg SA. Renaltoxicity of interleukin-2 administration in patients with metastatic renal cell cancer: effect of pre-therapy
43

nephrectomy. J. Urol. 1989; 141: 499-503.149. Schwartzentruber D, Lotze MT and Rosenberg SA. Colonic perforation. An unusual complication of
therapy with high dose interleukin-2. Cancer 1988; 11: 2350-2353.150. Sparano JA, Dutcher JP, Kaleya R, Caliendo G, Fiorito J, Mitsudo S, Shechner R, Boley SJ, Gucalp
R, Ciobanu N, Grima K, Wiernik PH and Brandt LJ. Colonic ischemia complicating immunotherapywith interleukin-2 and interferon-alpha. Cancer 1991; 68: 1538-1544.
151. Sparano JA, Brandt LJ, Dutcher JP, DuBois JS and Atkins MB. Symptomatic exacerbation of Crohndisease after treatment with high-dose interleukin-2. Ann. Intern. Med. 1993; 118: 617-618.
152. Fisher B, Keenan AM, Garra BS, Steinberg SM, White DE, DiBisceglie AM, Hoofnagle JH, Yolles P,Rosenberg SA and Lotze MT. Interleukin-2 induces profound reversible cholestasis: a detailed analysisin treated cancer patients. J. Clin. Oncol. 1989; 7: 1852-1862.
153. Atkins MB, Mier JW, Parkinson DR, Gould JA, Berkman EM and Kaplan MM. Hypothyroidism aftertreatment with interleukin-2 and lymphokine-activated killer cells. N. Engl. J. Med. 1988; 318:1557-1563.
154. Mattijssen VJM, Mulder de PHM, Liessum van PA, Corstens FHM, Franks CR and Wagener DTW.Hypothyroidism and goiter in a patient during treatment with interleukin-2. Cancer 1990; 65: 2686-2688.
155. Conlon KC, Urba WJ, Smith JW, Steis RG, Longo DL and Clark JW. Exacerbation of symptoms ofautoimmune disease in patients receiving alpha-interferon therapy. Cancer 1990; 65: 2237-2242.
156. Kirchner H, Korfer A, Palmer PA, Evers P, De Riese W, Knuver-Hopf J, Hadam M, Goldman U,Franks CR, Poliwoda H et al. Subcutaneous interleukin-2 and interferon-alpha 2b in patients withmetastatic renal cell cancer: the German outpatient experience. Mol. Biother. 1990; 2: 145-154.
157. Pichert G, Jost LM, Zobeli L, Odermatt B, Pedia G and Stahel RA. Thyroiditis after treatment withinterleukin-2 and interferon alpha-2a. Br. J. Cancer 1990; 62: 100-104.
158. Scalzo S, Gengaro A, Boccoli G, Masciulli R, Giannella G, Salvo G, Marolla P, Carlini P, MassiminiG, Holdener EE et al. Primary hypothyroidism associated with interleukin-2 and interferon alpha-2therapy of melanoma and renal carcinoma. Eur. J. Cancer 1990; 26: 1152-1156.
159. Pichert G, Jost LM, Fierz W and Stahel RA. Clinical and immune modulatory effects of alternativeweekly interleukin-2 and interferon alfa-2a in patients with advanced renal cell carcinoma andmelanoma. Br. J. Cancer 1991; 63: 287-292.
160. Kruit WH, Bolhuis RL, Goey SH, Jansen RL, Eggermont AM, Batchelor D, Schmitz PI and Stoter G.Interleukin-2-induced thyroid dysfunction is correlated with treatment duration but not with tumorresponse. J. Clin. Oncol. 1993; 11: 921-924.
161. Weijl NI, Van der Horst D, Brand A, Kooy Y, Van Luxemburg S, Schroder J, Eentjes E, Van RoodJJ, Cleton FJ and Osanto S. Hypothyroidism during immunotherapy with interleukin-2 is associated withantithyroid antibodies and response to treatment. J. Clin. Oncol. 1993; 11: 1376-1383.
162. Reid I, Sharpe I, McDevitt J, Maxwell W, Emmons R, Tanner WA and Monson JR. Thyroiddysfunction can predict response to immunotherapy with interleukin-2 and interferon-2 alpha. Br. J.Cancer 1991; 64: 915-918.
163. Denicoff KD, Durkin TM, Lotze MT, Quinlan PE, Davis CL, Listwak SJ, Rosenberg SA and RubinowDR. The neuroendocrine effects of interleukin-2 treatment. J. Clin. Endocrinol. Metab. 1989; 69:402-410.
164. Lissoni P, Barni S, Archili C, Cattaneo G, Rovelli F, Conti A, Maestroni GJ and Tancini G. Endocrineeffects of a 24-hour intravenous infusion of interleukin-2 in the immunotherapy of cancer. AnticancerRes. 1990; 10: 753-757.
165. Lissoni P, Barni S, Rovelli F, Crispino S, Fumagalli G, Pescia S, Vaghi M, Camesasca G and TanciniG. Neuroendocrine effects of subcutaneous interleukin-2 injection in cancer. Tumori. 1991; 77: 212-215.
166. Denicoff KD, Rubinow DR, Papa MZ and Seipp CA. The neuropsychiatric effects of treatment withinterleukin-2 and lymphokine activated killer cells. Ann. Intern. Med. 1987; 107: 293-300.
167. Saris SC, Patronas NJ, Rosenberg SA, Alexander JT and Frank J. The effect of intravenousinterleukin-2 on brain water content. J. Neurosurg. 1989; 71: 169-174.
168. Vecht CJ, Keohane C, Menon RS, Punt CJA and Stoter G. Acute fatal leukoencephalopathy afterinterleukin-2 therapy. N. Engl. J. Med. 1990; 323: 1146-1147.
169. Gaspari G, Lotze MT, Rosenberg SA, Stern JB and Katz SI. Dermatological changes associated withinterleukin-2 administration. JAMA 1987; 258: 1624-1629.
44

170. Weinstein A, Brijak D, Mittelman A et al. Erythema nodosum in a patient with renal celll carcinomatreated with interleukin-2 and lymphokine activated killer cells. JAMA 1987; 258: 3120-3121.
171. Baars JW, Wagstaff J, Hack CE, Wolbink GJ, Eerenberg-Belmer AJM and Pinedo HM. Angioneuroticoedema and urticaria during therapy with interleukin-2. Br. J. Cancer 1992; 3: 243-244.
172. Baars JW, Coenen JL, Wagstaff J, Van der Valk P and Pinedo HM. Lobular panniculitis aftersubcutaneous administration of interleukin-2 (IL-2), and its exacerbation during intravenous therapy withIL-2. Br. J. Cancer 1992; 66: 698-699.
173. Ramseur WL, Richards F,II. and Duggan DB. A case of fatal pemphigus vulgaris in association withbeta interferon and interleukin-2 therapy. Cancer 1989; 63: 2005-2007.
174. Sleijfer DT, Janssen RA, Buter J, De Vries EGE, Willemse PHB and Mulder NH. Phase II study ofsubcutaneous interleukin-2 in unselected patients with advanced renal cell cancer on an outpatient basis.J. Clin. Oncol. 1992; 10: 1119-1123.
175. Lee RE, Gaspari AA, Lotze MT et al. Interleukin-2 and psoriasis. Arch. Dermatol. 1988; 124:1811-1815.
176. Van Haelst Pisani C, Kovach JS, Kita H, Leiferman KM, Gleich GJ, Silver JE, Dennin R and AbramsJS. Administration of interleukin-2 (IL-2) results in increased plasma concentrations of IL-5 andeosinophilia in patients with cancer. Blood 1991; 78: 1538-1544.
177. Paciucci PA, Mandeli J, Oleksowicz L, Ameglio F and Holland JF. Thrombocytopenia duringimmunotherapy with interleukin-2 by constant infusion. JAMA 1990; 89: 308-312.
178. Richards JM, Gilewski TA and Vogelzang NJ. Association of interleukin-2 therapy with staphylococcalbacteriemia. Cancer 1991; 67: 1570-1575.
179. Snydman DR, Sullivan B, Gill M, Gould JA, Parkinson DR and Atkins MB. Nosocomial sepsisassociated with interleukin-2 see comments. Ann. Intern. Med. 1990; 112: 102-107.
180. Lim SH, Giles FJ, Smith MP and Goldstone AH. Bacterial infections in lymphoma patients treated withrecombinant interleukin-2 infusion. Acta Haematol. 1991; 85: 135-138.
181. Pockaj BA, Topalian SL, Steinberg SM, White DE and Rosenberg SA. Infectious complicationsassociated with interleukin-2 administration: A retrospective review of 935 treatment courses. J. Clin.Oncol. 1993; 11: 136-147.
182. Buter J, De Vries EGE, Sleijfer DT, Willemse PHB and Mulder NH. Infection after subcutaneousinterleukin-2. Lancet 1992; 339: 552.
183. Klempner MS, Noring R, Mier JW and Atkins MB. An acquired chemotactic defect in neutrophils frompatients receiving interleukin-2 immunotherapy see comments. N. Engl. J. Med. 1990; 322: 959-965.
184. Mier JW, Vachino G, Klempner MS, Aronson FR, Noring R, Smith S, Brandon EP, Laird W andAtkins MB. Inhibition of interleukin-2-induced tumor necrosis factor release by dexamethasone:prevention of an acquired neutrophil chemotaxis defect and differential suppression of interleukin-2associated side effects. Blood 1990; 76: 1933-1940.
185. Rosenberg SA, Lotze MT, Yang JC, Linehan WM, Seipp C, Calabro S, Karp SE, Sherry RM, SteinbergS and White DE. Combination therapy with interleukin-2 and alpha-interferon for the treatment ofpatients with advanced cancer. J. Clin. Oncol. 1989; 7: 1863-1874.
186. Figlin RA, Abi-Aad AS, Belldegrun A and deKernion JB. The role of interferon and interleukin-2 inthe immunotherapeutic approach to renal cell carcinoma. Semin. Oncol. 1991; 18: 102-107.
187. Von Rohr A, Ghosh AK, Thatcher N and Stern PL. Immunomodulation during prolonged treatment withcombined interleukin-2 and interferon-alpha in patients with advanced malignancy. Br. J. Cancer 1993;67: 163-171.
188. Yang SC, Grimm EA, Parkinson DR, Carinhas J, Fry KD, Mendiguren-Rodriguez A, Licciardello J,Owen-Schaub LB, Hong WK and Roth JA. Clinical and immunomodulatory effects of combinationimmunotherapy with low-dose interleukin 2 and tumor necrosis factor alpha in patients with advancednon-small cell lung cancer: a phase I trial. Cancer Res. 1991; 51: 3669-3676.
189. McIntosh JK, Mule JJ, Merino MJ and Rosenberg SA. Synergistic anti-tumor effects of immunotherapywith recombinant interleukin-2 and recombinant tumor necrosis factor-alfa. Cancer Res. 1988; 48:4011-4017.
190. Zimmerman RJ, Gauny S, Chan A, Landre P and Winkelhake JL. Sequence dependence ofadministration of human tumor necrosis factor and interleukin-2 in murine tumor therapy. J. Natl.Cancer Inst. 1989; 81: 227-231.
191. Lissoni P, Pittalis S, Brivio F, Tisi E, Rovelli F, Ardizzoia A, Barni S, Tancini G, Giudici G, Biondi
45

A, Conti A and Maestroni G. In vitro modulatory effects of interleukin-3 on macrophage activationinduced by interleukin-2. Cancer 1993; 71: 2076-2081.
192. Mitchell MS, Kempf RA, Harel W, Shau H, Boswell WD, Lind S and Bradley EC. Effectiveness andtolerability of low dose cyclophosphamide and low-dose intravenous interleukin-2 disseminatedmelanoma. J. Clin. Oncol. 1988; 6: 409-424.
193. Mitchell MS. Chemotherapy in combination with biomodulation: a 5-year experience withcyclophosphamide and interleukin-2. Semin. Oncol. 1992; 19: 80-87.
194. Dillman RO, Oldham RK, Barth NM, Birch R, Arnold J and West WH. Recombinant interleukin-2 andadoptive immunotherapy alternated with dacarbazine therapy in melanoma: a National Biotherapy StudyGroup trial. J. Natl. Cancer Inst. 1990; 82: 1345-1349.
195. Khayat D, Borel C, Tourani JM, Benhammouda A, Antoine E, Rixe O, Vuillemin E, Bazex PA, ThillL, Franks R, Auclerc G, Soubrane C, Banzet P and Weil M. Sequential chemoimmunotherapy withcisplatin, interleukin-2, and interferon alfa-2a for metastatic melanoma. J. Clin. Oncol. 1993; 11:2173-2180.
196. Richards JM, Mehta N, Ramming K and Skosey P. Sequential chemoimmunotherapy in the treatmentof metastatic melanoma. J. Clin. Oncol. 1992; 10: 1338-1343.
197. Cameron RB, McIntosh JK and Rosenberg SA. Synergistic antitumor efects of combinationimmunotherapy with interleukin-2 and an recombinant hybrid interferon-alpha in the treatment ofestablished murine hepatic metastases. Cancer Res. 1988; 48: 5810-5817.
198. Chikkala NF, Lewis I, Ulchaker J, Stanley J, Tubbs R and Finke JH. Interactive effects ofalpha-interferon A/D and interleukin 2 on murine lymphokine-activated killer activity: analysis at theeffector and precursor level. Cancer Res. 1990; 50: 1176-1182.
199. Weber JS and Rosenberg SA. Effects of murine tumor class I major histocompatibility complexexpression on antitumor activity of tumor-infiltrating lymphocytes. J. Natl. Cancer Inst. 1990; 82:755-761.
200. Tanaka K, Yoshioka T, Bieberich C and Jay G. Role of the major histocompatibility complex class Iantigens in tumor growth and metastasis. Ann. Rev. Immunol. 1988; 6: 359-380.
201. Schiller JH, Hank J, Storer B, Borchert AA, Moore KH, Albertini M, Bechhofer R, Wesley O, BrownRR, Bastin AM and Sondel PM. A direct comparison of immunological and clinical effects ofinterleukin 2 with and without interferon-α in humans. Cancer Res. 1993; 53: 1286-1292.
202. West W, Schwartzberg L, Blumenchein G et al. Continuous infusion interleukin-2 plus subcutaneousinterferon alpha in advanced malignancy. Proc. Am. Soc. Clin. Oncol. 1990; 9: 191. (Abstract)
203. Demchak P, Atkins M, Sell K et al. Phase II study of interleukin-2 (IL-2) and interferon alpha-2a(IFN-α) outpatient therapy for metastatic renal cancer. Proc. Am. Assoc. Cancer Res. 1991; 32: 191.(Abstract)
204. Figlin RA, Belldegrun A, Moldawer N, Zeffren J and deKernion JB. Concomitant administration ofrecombinant human interleukin-2 and recombinant interferon alfa-2A: an active outpatient regimen inmetastatic renal cell carcinoma. J. Clin. Oncol. 1992; 10: 414-421.
205. Budd GT, Murthy S, Finke J, Sergi J, Gibson V, Medendorp S, Barna B, Boyett J and Bukowski RM.Phase I trial of high-dose bolus interleukin-2 and interferon alfa-2a in patients with metastaticmalignancy. J. Clin. Oncol. 1992; 10: 804-809.
206. Thomas H, Barton C, Saini A, Dalgleish A and Waxman J. Sequential interleukin-2 and alpha interferonfor renal cell carcinoma and melanoma. Eur. J. Cancer 1992; 28A: 1047-1049.
207. Ilson DH, Motzer RJ, Kradin RL, Vogelzang NJ, Bajorin DF, Scher HI, Nanus D, O’Moore P,Marathias K and Bosl GJ. A phase II trial of interleukin-2 and interferon alfa-2a in patients withadvanced renal cell carcinoma. J. Clin. Oncol. 1992; 10: 1124-1130.
208. Wang JCL, Walle A, Novogrodsky A, Suthanthiran M, Silver RT, Bander NH, Rubin AL and StenzelKH. A phase II clinical trial of adoptive immunotherapy for advanced renal cell carcinoma usingmitogen-activated autologous leucocytes and continous infusion interleukin-2. J. Clin. Oncol. 1989; 7:1885-1891.
209. Krigel RL, Radavic-Shaller KA, Rudolph AR, Konrad M, Bradley ED and Comis RL. Renal cellcarcinoma: treatment with recombinant interleukin-2 plus beta-interferon. J. Clin. Oncol. 1990; 8:460-467.
210. Negrier S, Ravaud A, Bui BN, Rebattu P, Lakdja F, Merrouche Y, Clavel M and Philip T.Subcutaneous interleukin-2 (IL-2) and interferon alpha (IFN) in metastatic renal cell cancer (MRCC):
46

a double institution study on 37 patients. Eur. J. Cancer 1991; suppl. 2: S233-A1365. (Abstract)211. Dutcher JP, Fisher RI, Weiss G, Aronson FR, Margolin K, Caliendo G, Louie A and Atkins M. An
outpatient (OPT) regimen of subcutaneous (SC) interleukin-2 (IL2) plus alpha-interferon (IFN) inmetastatic renal cell cancer (RCC). Proc. Am. Soc. Clin. Oncol. 1993; 12: 248. (Abstract)
212. Enzinger HM, Bergmann L, Fenchel K, Neugebauer T, Jahn B et al. Daily alternating schedules ofinterferon-α and interleukin-2 in advanced cancer - clinical results and biological effects. Onkologie1992; 24 (Suppl. 1): P-10. (Abstract)
213. Lipton A, Harvey H, Givant E, Hopper K, Lawler J et al. Interleukin-2 and interferon-α-2a outpatienttherapy for metastatic renal cell carcinoma. J. Immunother. 1993; 13: 122-129.
214. Keilholz U, Scheibenbogen C, Bergmann L, Tilgen W and Hunstein W. IFN-α and IL-2 in metastaticmelanoma: comparizon of two phase II trials. Onkologie 1992; 15 (Suppl. 1): 17. (Abstract)
215. Kirchner H, Lopez Haenninen E, Volkenandt M and Atzpodien J. Chemoimmunotherapy of advancedmalignant melanoma with carboplatin and DTIC followed by subcutaneous interleukin-2 andinterpheron-alpha. Proc. Am. Soc. Clin. Oncol. 1993; 12: 1356. (Abstract)
216. Kruit WH, Goey SH, Monson JR, Stahel RA, Calabresi F, Mertelsmann R, Holdener EE, EggermontAM, Bolhuis RL, De Mulder PHM et al. Clinical experience with the combined use of recombinantinterleukin-2 (IL2) and interferon alfa-2a (IFN alpha) in metastatic melanoma. Br. J. Haematol. 1991;79 Suppl 1P 84-6. XX:
217. Chouaib S, Bertoglio J, Blay J, Marchiol-Fournigault C and Fradelizi D. Generation oflymphokine-activated killer cells: synergy between tumor necrosis factor and interleukin-2. Proc. Natl.Acad. Sci. U. S. A. 1988; 85: 6875-6879.
218. Verstovsek S, Maccubbin D, Ehrke MJ and Mihich E. Tumoricidal activation of murine residentperitoneal macrophages by interleukin 2 and tumor necrosis factor alpha. Cancer Res. 1992; 52:3880-3885.
219. Quesada JR, Talpaz M, Rios A, Kurzrock R and Gutterman JU. Clinical toxicity of interferons in cancerpatients. J. Clin. Oncol. 1986; 4: 234-243.
220. Goldstein D and laszlo J. Interferon therapy in cancer: from imaginon to interferon. Cancer Res. 1986;46: 4315.
221. Dorr RT. Interferon-α in malignant and viral diseases. A review. Drugs 1993; 45(2): 177-211.222. Hansen RM and Borden EC. Current status of interferons in the treatment of cancer. Oncology
(Huntingt). 1992; 6: 19-24; discus.223. Isaacs H and Lindemann J. Virus interference: 1. The interferon. Proc. R. Soc. Lond. [Biol]. 1957; 147:
257-262.224. Adolf GR. Antigenic structure of human interferonΩ1 (interferon aplha II1): comparison with other
human interferons. J. Gen. Virol. 1987; 68: 1669-1676.225. Tan YH. Chromosome 21 and the cell growth inhibitory effect of humaninterferon prepartations. Nature
1976; 260: 141-143.226. Rashidbaigi A, Langer JA, Jung V et al. The gene for the human immune interferon receptor is located
on chromosome 6. Proc. Natl. Acad. Sci. U. S. A. 1986; 83: 384-388.227. Becker S. Interferon-τ accelerates immune proliferation via its effect on monocyte HLA-DR expression.
Cell. Immunol. 1985; 91: 301-307.228. Wills RJ, Dennis S, Spiegel HE, Gibson DM, Nadler PI et al. Interferon kinetics and adverse reactions
after intravenous, intramuscular, and subcutaneous injection. Clin. Pharm. Ther. 1984; 35: 755-757.229. Radwanski E, Perentesis G, Oden E, Jacobs S, Affrime M et al. Pharmakokinetics of IFN-α-2b in
healthy volunteers. J. Clin. Pharmacol. 1987; 27: 432-435.230. Tamura T, Sasaki Y, Shinkai T, Eguchi K, Sakurai M, Fujiwara Y, Nakagawa K, Minato K and Saijo
N. Phase I study of combination therapy with interleukin 2 andβ-interferon in patients with advancedmalignancy. Cancer Res. 1989; 49: 730-735.
231. Kinney P, Triozzi P and Young D. Phase II trial of interferon-beta-serine in metastatic renal cellcarcinoma. J. Clin. Oncol. 1990; 8: 881-885.
232. Greiner JW, Guadagni F, Hand PH, Pestka S, Noguchi P, Fisher PB and Schlom J. Augmentation oftumor antigen expression by recombinant human interferons: enhanced targeting of monoclonalantibodies to carcinomas. Cancer Treat. Res. 1990; 51P 413-32. XX:
233. Aulitzky W, Gastl G, Aulitzky WE et al. Successful treatment of metastatic renal cell carcinoma witha biological active dose of recombinant interferon-gamma. J. Clin. Oncol. 1989; 7(12): 1875-1884.
47

234. Ernstoff MS, Gooding W, Nair S, Bahnson RR, Miketic LM, Banner B, Day R, Whiteside T,Titus-Ernstoff L and Kirkwood JM. Immunological effects of treatment with sequential administrationof recombinant interferon gamma and alpha in patients with metastatic renal cell carcinoma during aphase I trial. Cancer Res. 1992; 52: 851-856.
235. Ernstoff MS, Nair S, Bahnson RR, Miketic LM, Banner B, Gooding W, Day R, Whiteside T, HakalaT and Kirkwood JM. A phase IA trial of sequential administration recombinant DNA- producedinterferons: combination recombinant interferon gamma and recombinant interferon alfa in patients withmetastatic renal cell carcinoma. J. Clin. Oncol. 1990; 8: 1637-1649.
236. Weiner LM, Padavic-Shaller K, Kitson J, Watts P, Krigel RL and Litwin S. Phase I evaluation ofcombination therapy with interleukin 2 and gamma-interferon. Cancer Res. 1991; 51: 3910-3918.
237. Escudier B, Farace F, Angevin E, Triebel F, Antoun S, Leclerc B, Brandely M, Aboudaram A,Nitenberg G and Hercend T. Combination of interleukin-2 and gamma interferon in metastatic renal cellcarcinoma. Eur. J. Cancer 1993; 29A: 724-728.
238. Baars JW, Wagstaff J, Van Groeningen CJ, Vermorken JB, Bijvank EM, Pinedo HM and Nauta JJ.Phase II study of interferon-gamma and interleukin-2: tachyphylaxis of toxicity to the liver duringincreasing immune enhancement letter. J. Natl. Cancer Inst. 1993; 85: 410-411.
239. Urba WJ, Kopp WC, Clark JW, Smith II JW, Steis RG, Huber C, Coggin D and Longo DL. The invivo immunomodulatory effects of recombinant interferon gamma plus recombinant tumor necrosisfactor-alfa. J. Clin. Oncol. 1991; 10: 1831-1839.
240. Talpaz M, Kantarjian H, Kurzrock R, Trujillo JM and Gutterman JU. Interferon-alpha producessustained cytogenetic responses in chronic myelogenous leukemia. Philadelphia chromosome-positivepatients. Ann. Intern. Med. 1991; 114: 532-538.
241. Muss HB. Interferon therapy for renal cell carcinoma. Semin. Oncol. 1987; 14 (suppl 2): 36-42.242. Kirkwood JM, Harris JE, Vera R, Sandler S, Fischer DS, Khandekar J, Ernstoffo MS, Gordon L, Lutes
R, Boninie P, Lytton B, Gobleigh M and Taylor SJ. A randomized study of low and high doses ofleucocyte-α-interferon in metastatic renal cell carcinoma: the American Cancer Society collaborativetrial. Cancer Res. 1985; 45: 863-871.
243. Quesada JR, Rios A, Swanson DA, Trown P and Gutterman JU. Antitumor activity ofrecombinant-derived interferon alpha in metastatic renal cell carcinoma. J. Clin. Oncol. 1985; 3:1522-1528.
244. Muss HB, Constanzi JJ, Leavit R, Williams RD and Kempf RA. Recombinant alfa interferon in renalcell carcinoma: A randomized trial of two routes of administration. J. Clin. Oncol. 1987; 5: 286-291.
245. Kirkwood JM. Studies of interferons in the therapy of melanoma. Semin. Oncol. 1991; 18: 83-90.246. Creagan ET, Ahmann DL, Frytak S, Long HJ and Itri M. Recombinant leucocyte A interferon
(rIFN-alpha A) in the treatment of disseminated malignant melanoma: analysis of complete and longterm responding patients. Cancer 1986; 58: 2576.
247. Creagan ET, Ahmann DL, Green SJ, Long HJ, Frytak S and Itri LM. Phase II study of recombinantleukocyte A interferon (IFN-rA) plus cimetidine in disseminated malignant melanoma. J. Clin. Oncol.1985; 3: 977.
248. De Wit R, Danner SA, Bakker PJ, Lange JM, Eeftinck Schattenkerk JK and Veenhof CH. Combinedzidovudine and interferon-alpha treatment in patients with AIDS-associated Kaposi’s sarcoma. J. Intern.Med. 1991; 229: 35-40.
249. Falkson CI, Falkson G and Falkson HC. Improved results with the addition of interferon alfa-2b todacarbazine in the treatment of patients with metastatic malignant melanoma. J. Clin. Oncol. 1991; 9:1403-1408.
250. Sertoli MR, Queirolo P, Bajetta E, Negretti E, Calabresi F, Barduagni L, Giannotti B, Brogelli L,Bernengo MG, Sofra MC, Maifredi G, Zumiani G, Comella G, Bruzzoni R, DiLeo A, et al. Dacarbazine(DTIC) with or without recombinant interferon alpha-2a at different dosages in the treatment of stageIV melanoma patients. Prilimary results of a randomized trial. Proc. Am. Soc. Clin. Oncol. 1992; 11:1185. (Abstract)
251. Kirkwood JM, Ernstoff MS, Giuliano A, Gams R, Robinson WA, Costanzi J, Pouillart P, Speyer J,Grimm M and Spiegel R. Interferon alpha-2a and dacarbazine in melanoma. J. Natl. Cancer Inst. 1990;82: 1062-1063.
252. Thomson D, Adena M, McLeod GRC, Hersey P, Gill P, Coates A, Olver I, Kefford R, Lowenthal R,Beadle G, Walpole E, Boland K and Kingston D. Interferonα-2a (IFN) does not improve response or
48

survival when added to dacarbazine(DTIC) in metastatic melanoma: results of a multi-institutionalaustralian randomised trial QMP8704. Proc. Am. Soc. Clin. Oncol. 1992; 11: 1177. (Abstract)
253. Rozenbaum W, Gharakhanian S, Navarette MS, De Sahb R, Cardon B and Rouzioux C. Long-termfollow-up of 120 patients with AIDS-related Kaposi’s sarcoma treated with interferon alpha-2a. J.Invest. Dermatol. 1990; 95: 161S-165S.
254. Krown SE, Gold JW, Niedzwiecki D, Bundow D, Flomenberg N, Gansbacher B and Brew BJ.Interferon-alpha with zidovudine: safety, tolerance, and clinical and virologic effects in patients withKaposi sarcoma associated with the acquired immunodeficiency syndrome (AIDS) published erratumappears in Ann Intern Med 1990 Aug 15;113(4):334. Ann. Intern. Med. 1990; 112: 812-821.
255. Scadden DT, Bering HA, Levine JD, Bresnahan J, Evans L, Epstein C and Groopman JE.Granulocyte-macrophage colony-stimulating factor mitigates the neutropenia of combined interferon alfaand zidovudine treatment of acquired immune deficiency syndrome-associated Kaposi’s sarcoma. J.Clin. Oncol. 1991; 9: 802-808.
256. Silgals RM, Ahlgren JD and Neefe JR. A phase II trial of high-dose intravenous interferon alpha-2 inadvanced colorectal cancer. Cancer 1984; 54: 2257-2261.
257. Neefe JR, Sullivan JE, Ayoob M, Phillips E and Smith FP. Augmented immunity in cancer patientstreated withα-interferon. Cancer Res. 1985; 45: 874-878.
258. Schwartz EL, Hoffman M, O’Connor CJ and Wadler S. Stimulation of 5-fluorouracil metabolicactivation by interferon- alpha in human colon carcinoma cells. Biochem. Biophys. Res. Commun. 1992;182: 1232-1239.
259. Houghton JA, Adkins DA, Rahman A and Houghton PJ. Interaction between 5-fluorouracil,[6RS]leucovorin, and recombinant human interferon-α2a in cultured colon adenocarcinoma cells. CancerComm. 1991; 3: 225-231.
260. Sinnige HAM, Timmer-Bosscha H, Peters GF, De Vries EGE and Mulder NH. Combined modulationof leucovorin andα-2a interferon of fluoropyrimidine mediated growth inhibition. Anticancer Res.1993; 13: 1335-1340.
261. McBee P, Petraiuolo W and Katoh A. Inhibition of liver metastases in nude mice by the combinedaction of 5-fluorouracil and interferon. Anticancer Drugs 1990; 1: 165-170.
262. Grem JL, McAtee N, Murphy RF, Balis FM, Steinberg SM, Hamilton JM, Sorensen JM, Sartor O,Kramer BS, Goldstein LJ et al. A pilot study of interferon alfa-2a in combination with fluorouracil plushigh-dose leucovorin in metastatic gastrointestinal carcinoma. J. Clin. Oncol. 1991; 9: 1811-1820.
263. Grem JL, Chu E, Boarman D, Balis FM, Murphy RF, McAtee N and Allegra CJ. Biochemicalmodulation of fluorouracil with leucovorin and interferon: preclinical and clinical investigations. Semin.Oncol. 1992; 19: 36-44.
264. Wadler S and Wiernik PH. Clinical update on the role of fluorouracil and recombinant interferon alfa-2ain the treatment of colorectal carcinoma. Semin. Oncol. 1990; 17: 16-21; discus.
265. Wadler S, Lembersky B, Atkins M, Kirkwood J and Petrelli N. Phase II trial of fluorouracil andrecombinant interferon alfa- 2a in patients with advanced colorectal carcinoma: an Eastern CooperativeOncology Group study. J. Clin. Oncol. 1991; 9: 1806-1810.
266. Sinnige HAM, Buter J, De Vries EGE, Uges DRA, Roenhorst HW, Verschueren RCJ, Sleijfer DTh,Willemse PHB and Mulder NH. Phase I-II study of the addition ofα-2a interferon to5-fluorouracil/leucovorin. Pharmacokinetic interaction ofα-2a interferon and leucovorin. Eur. J. Cancer1993; 29A(12): 1715-1720.
267. Kvols LA. Metastatic carcinoid tumors and the carcinoid syndrome. A selective review of chemotherapyand hormonal therapy. Am. J. Med. 1986; 81,(Suppl 6B): 49-55.
268. Moertel CG. An Odyssey in the land of small tumors. J. Clin. Oncol. 1987; 5: 1503-1522.269. Kvols LK, Moertel CG, O’Connel MJ, Schutt AJ, Rubin J and Hahn RG. Treatment of the malignant
carcinoid syndrome. Evaluation of a long-acting somatostatin analogue. N. Engl. J. Med. 1986; 315:663-666.
270. Vinik AJ, Thompson N, Eckhauser F and Moatarri AR. Clinical features of the carcinoid syndrome andthe use of somatostatin analogue in its management. Acta Oncol. 1989; 28: 389-402.
271. Öberg K, Funa K and Alm G. Effects of leucocyte interferon on clinical symptoms and hormone levelsin patients with mid-gut carcinoid tumors and carcinoid syndrome. N. Engl. J. Med. 1983; 309: 129-133.
272. Öberg K, Norheim I, Lind E, Alm G, Lundqvist G, Wide L, Jonsdotter B, Magnusson A and WilanderE. Treatment of malignant carcinoid tumors with human leucocyte interferon: long term results. Cancer
49

Treat. Rep. 1986; 70: 1297-1304.273. Smith DB, Scarfee JH, Wagstaff J and Johnston RJ. Phase II trial of rDNA alfa 2b interferon in patients
with malignant carcinoid tumor. Cancer Treat. Rep. 1987; 71: 1265-1266.274. Öberg K, Alm G, Magnusson A, Lundqvist G, Theodorsson E, Wide L and Wilander E. Treatment of
malignant carcinoid tumors with recombinant interferon alfa-2b: development of neutralizing antibodiesand possible loss of antitumor activity. J. Natl. Cancer Inst. 1989; 81: 531-535.
275. Hanssen LE, Schrumpf E, Kolbenstved AN, Tausjo J and Dolva LO. Treatment of malignant metastaticmidgut carcinoid tumours with recombinant humanα2b interferon with or without prior hepatic arteryembolization. Scand. J. Gastroenterol. 1989; 24: 787-795.
276. Moertel CG, Rubin J and Kvols LK. Therapy of metastatic carcinoid tumor an the malignant carcinoidsyndrome with recombinant leucocyte A interferon. J. Clin. Oncol. 1989; 7: 865-868.
277. Veenhof CHN, De Wit R, Taal BG, Dirix LY, Wagstaff J, Hensen A, Huldij AC and Bakker PJM. Adose escalation study of recombinant interferon-alpha in patients with a metastatic carcinoid tumour.Eur. J. Cancer 1992; 28: 75-78.
278. Biesma B, Willemse PHB, Mulder NH, Verschueren RCJ, Kema IP, De Bruijn HWA, Postmus PE,Sleijfer DTh and De Vries EGE. Recombinant interferon alpha-2b in patients with metastatic apudomas:effect on tumours and tumour markers. Br. J. Cancer 1992; 66: 850-855.
279. Berek JS, Hacker NF, Lichtenstein A, Jung T, Spina C, Knox RM, Brady J, Greene T, Ettinger LM,Lagasse LD, Bonnem EM, Spiegel RJ and Zighelboim J. Intraperitoneal recombinant interferon for‘salvage‘ immunotherapy in stage III epithelian ovarian cancer: a gynaecologic oncology group study.Cancer Res. 1985; 45: 4447-4453.
280. Willemse PHB, De Vries EGE, Mulder NH, Aalders JG, Bouma J and Sleijfer DTh. Intraperitonealhuman recombinant interferon alpha-2b in minimal residual ovarian cancer. Eur. J. Cancer 1990; 26:353-358.
281. Bezwoda WR, Golombick T, Dansey R and Keeping J. Treatment of malignant ascites due torecurrent/refractory ovarian cancer: the use of interferon-alpha or interferon-alpha plus chemotherapyin vivo and in vitro. Eur. J. Cancer 1991; 27: 1423-1429.
282. Nardi M, Cognetti F, Giulia MD, Sternberg C, Lombardi A et al. Intraperitoneal rα2-interferon (IFN)alternating with cisplatin (DDP) as salvage therapy for minimal residual disease ovarian cancer. Proc.Am. Soc. Clin. Oncol. 1989; 8: 157. (Abstract)
283. Bartoletti R, Massimini G, Criscuolo D and Rizzo M. Interferon alfa 2a in superficial bladder cancerprophylaxis: toleration and long-term follow-up. A phase I-II study. Anticancer Res. 1991; 11:2167-2170.
284. Ezekowitz RA, Mulliken JB and Folkman J. Interferon alfa-2a therapy for life-threatening hemangiomasof infancy see comments. N. Engl. J. Med. 1992; 326: 1456-1463.
285. White CW, Wolf SJ, Korones DN, Sondheimer HM, Tosi MF and Yu A. Treatment of childhoodangiomatous diseases with recombinant interferon alfa-2a. J. Pediatr. 1991; 118: 59-66.
50