Embed Size (px)
Citation preview

University of Groningen
New diagnostic and therapeutic options in early-stage vulvar cancerOonk, Maaike Henrike Marije
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2011
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Oonk, M. H. M. (2011). New diagnostic and therapeutic options in early-stage vulvar cancer Groningen: s.n.
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 29-08-2018

CHAPTER 5Sentinel node dissection is safe in the treatment of early-stage vulvar cancer
Ate G.J. van der Zee
Maaike H.M. Oonk
Joanne A. de Hullu
Anca C. Ansink
Ignace Vergote
René H. Verheijen
Angelo Maggioni
Katja N. Gaarenstroom
Peter J. Baldwin
Eleonora B. van Dorst
Jacobus van der Velden
Ralph H. Hermans
Hans van der Putten
Pierre Drouin
Achim Schneider
Wim J. Sluiter
Journal of Clinical Oncology 2008; 26: 884 – 889

62 | Chapter 5
Abstract
PurposeTo investigate the safety and clinical utility of the sentinel node procedure in early-stage vulvar
cancer patients.
Patients and MethodsA multicenter observational study on sentinel node detection using radioactive tracer and blue dye
was performed in patients with T1 / T2 (< 4cm) squamous cell cancer of the vulva. When the sentinel
node was found to be negative at pathologic ultrastaging, inguinofemoral lymphadenectomy was
omitted, and the patient was observed with follow-up for two years at intervals of every 2 months.
Stopping rules were defined for the occurrence of groin recurrences.
ResultsFrom March 2000 until June 2006, a sentinel node procedure was performed in 623 groins of
403 assessable patients. In 259 patients with unifocal vulvar disease and a negative sentinel node
(median follow-up time, 35 months), six groin recurrences were diagnosed (2.3%; 95% CI, 0.6% to
5%), and 3-year survival rate was 97% (95% CI, 91% to 99%). Short-term morbidity was decreased in
patients after sentinel node dissection only when compared with patients with a positive sentinel
node who underwent inguinofemoral lymphadenectomy (wound breakdown in groin: 11.7% v
34.0%, respectively; P < 0.0001; and cellulitis: 4.5 v 21.3%, respectively; P < 0.0001). Long-term
morbidity also was less frequently observed after removal of only the sentinel node compared with
sentinel node removal and inguinofemoral lymphadenectomy (recurrent erysipelas: 0.4 v 16.2 %,
respectively; P < 0.0001; and lymphedema of the legs: 1.9 v 25.2%, respectively; P < 0.0001).
ConclusionIn early-stage vulvar cancer patients with a negative sentinel node, the groin recurrence rate is low,
survival is excellent, and treatment-related morbidity is minimal. We suggest that sentinel node
dissection, performed by a quality-controlled multidisciplinary team, should be part of the standard
treatment in selected patients with early-stage vulvar cancer.

Sentinel node dissection early-stage vulvar cancer | 63
Introduction
Squamous cell cancer of the vulva is a rare disease with an annual incidence of two to three per
100,000 women.1-3 Current standard treatment for early-stage disease consists of radical excision of
the tumor with elective inguinofemoral lymphadenectomy. The efficacy of this treatment is good,
with reported groin recurrence rates varying between 1% and 10%.4-11 However, only 25% to 35% of
patients with early-stage disease will have lymph node metastases,5-9 and the remaining 65% to 75%
of patients are unlikely to benefit from elective inguinofemoral lymphadenectomy but will be at risk
of its significant morbidity. In the short term, wound healing in the groin is compromised by infection
and breakdown in 20% to 40% of patients. In the long term, lymphedema of the legs with increased
risk for erysipelas occurs in 30% to 70% of patients.10,12-14 Despite significant surgical morbidity and
a low frequency of lymph node metastases, an elective lymphadenectomy is regarded as standard
of care because unrecognized disease in the inguinofemoral lymph nodes is nearly always fatal. A
noninvasive or minimally invasive technique that allows the detection of inguinofemoral metastases
with a low false-negative rate is desirable. To date, noninvasive imaging techniques are neither
sensitive nor specific enough for the detection of (micro)metastases in inguinofemoral lymph
nodes.15,16
In a variety of malignancies, such as breast cancer and cutaneous melanoma, the false-negative
rate of the sentinel node procedure seems to be low (range, 0% to 29%; average, 7.3%).17,18
In breast cancer, not only was the nodal recurrence rate in the axilla exceptionally low (0.1% to
0.3%), but the sentinel node procedure was also associated with lower morbidity and improved
quality of life when compared with complete lymphadenectomy.19-23 Studies in vulvar cancer in
which sentinel node detection was followed by inguinofemoral lymphadenectomy suggest that the
sentinel node procedure is highly accurate in identifying lymph node metastases with a negative
predictive value approaching 100%.24-34 However, safety and clinical utility still need to be proven in
large clinical trials. The optimal design would be an equivalence randomized trial in which patients
with a negative sentinel node are randomly assigned to either observation alone or inguinofemoral
lymphadenectomy. However, because of the low incidence of the disease and the high number of
patients needed, several collaborative groups in gynecologic cancer deemed such a design as highly
unrealistic.
The aims of this observational study were to investigate the safety of omitting inguinofemoral
lymphadenectomy in patients with a negative sentinel node and to compare short- and long-term
morbidity between sentinel node removal only and inguinofemoral lymphadenectomy performed in
patients with a positive sentinel node. Groin recurrences were regarded as the most serious short-
term threat for participating patients with a negative sentinel node. Therefore, for safety reasons,
stopping rules were formulated, using continuous sequential analysis of the occurrence of groin
recurrences in the first 2 years of follow-up for each patient.
in

64 | Chapter 5
Patients and Methods
PatientsEligible patients had T1 or T2, less than 4cm, squamous cell cancer of the vulva with a depth of
invasion more than 1mm and clinically nonsuspicious inguinofemoral lymph nodes. To ensure the
quality of the sentinel node procedure in the participating centers, it was determined that each
gynecologic oncology center needed to have documented successful experience of the sentinel node
procedure with subsequent inguinofemoral lymphadenectomy in at least 10 vulvar cancer patients
(see Appendix). Permission from all local ethics committees was obtained. All patients gave written
informed consent. Patients were only included when registered at the University Medical Center
Groningen (Groningen, the Netherlands) before the start of treatment of the patient. Central data
management was performed at the University Medical Center Groningen.
Sentinel Node Detection and Treatment ProtocolTreatment consisted of radical excision of the primary tumor in combination with the sentinel
node procedure. The sentinel node procedure was performed with the combined technique
(radioactive tracer and blue dye), as previously described.26 After removal, sentinel nodes were
sent to the pathologist as individual specimens. When the sentinel node was negative, no further
treatment followed. If metastatic disease was identified in the sentinel node, an inguinofemoral
lymphadenectomy was performed, either during the same operation when found at frozen sectioning
or during a subsequent operation when found at routine pathologic examination or ultrastaging.
When more than one intranodal metastasis and / or extranodal growth was detected, postoperative
external-beam radiotherapy (50 Gy) to the groin / pelvis was recommended (treatment protocol is
detailed in Appendix).
Morbidity and Follow-UpData on postoperative morbidity were collected in a prospective fashion. Short-term morbidity
was defined as the occurrence of wound breakdown or wound infection (requiring antibiotics).
Patients were seen at least every 2 months for the first 2 years after treatment. Assessment included
interview, gynecologic examination, and palpation of the groins. The presence of lymphedema
(objective findings and subjective symptoms) and / or erysipelas of the legs was documented.
Long-term morbidity, defined by either lymphedema (present at two consecutive follow-up visits
> 1 year after primary therapy) and / or recurrent erysipelas (> one episode of erysipelas requiring
antibiotics), was also documented.
| 65
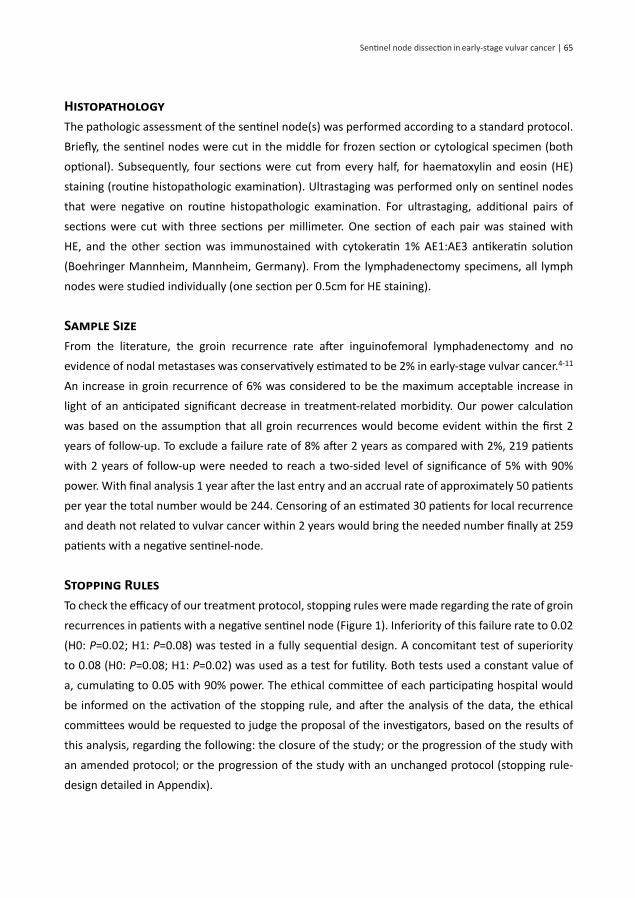
HistopathologyThe pathologic assessment of the sentinel node(s) was performed according to a standard protocol.
Briefly, the sentinel nodes were cut in the middle for frozen section or cytological specimen (both
optional). Subsequently, four sections were cut from every half, for haematoxylin and eosin (HE)
staining (routine histopathologic examination). Ultrastaging was performed only on sentinel nodes
that were negative on routine histopathologic examination. For ultrastaging, additional pairs of
sections were cut with three sections per millimeter. One section of each pair was stained with
HE, and the other section was immunostained with cytokeratin 1% AE1:AE3 antikeratin solution
(Boehringer Mannheim, Mannheim, Germany). From the lymphadenectomy specimens, all lymph
nodes were studied individually (one section per 0.5cm for HE staining).
Sample SizeFrom the literature, the groin recurrence rate after inguinofemoral lymphadenectomy and no
evidence of nodal metastases was conservatively estimated to be 2% in early-stage vulvar cancer.4-11
An increase in groin recurrence of 6% was considered to be the maximum acceptable increase in
light of an anticipated significant decrease in treatment-related morbidity. Our power calculation
was based on the assumption that all groin recurrences would become evident within the first 2
years of follow-up. To exclude a failure rate of 8% after 2 years as compared with 2%, 219 patients
with 2 years of follow-up were needed to reach a two-sided level of significance of 5% with 90%
power. With final analysis 1 year after the last entry and an accrual rate of approximately 50 patients
per year the total number would be 244. Censoring of an estimated 30 patients for local recurrence
and death not related to vulvar cancer within 2 years would bring the needed number finally at 259
patients with a negative sentinel-node.
Stopping RulesTo check the efficacy of our treatment protocol, stopping rules were made regarding the rate of groin
recurrences in patients with a negative sentinel node (Figure 1). Inferiority of this failure rate to 0.02
(H0: P=0.02; H1: P=0.08) was tested in a fully sequential design. A concomitant test of superiority
to 0.08 (H0: P=0.08; H1: P=0.02) was used as a test for futility. Both tests used a constant value of
a, cumulating to 0.05 with 90% power. The ethical committee of each participating hospital would
be informed on the activation of the stopping rule, and after the analysis of the data, the ethical
committees would be requested to judge the proposal of the investigators, based on the results of
this analysis, regarding the following: the closure of the study; or the progression of the study with
an amended protocol; or the progression of the study with an unchanged protocol (stopping rule-
design detailed in Appendix).
Sentinel node dissection early-stage vulvar cancer in

66 | Chapter 5
Figure 1. The ‘unsafe’ line indicates inferiority to a groin recurrence rate of 0.02; the ‘safe’ line
indicates superiority to 0.08. The ‘safe’ boundary was passed by the ‘events’ line when 126 patients
with unifocal vulvar cancer and a negative sentinel lymph node had completed 2 years of follow-up
without groin recurrences. Patients were censored at time of death by other causes than vulvar
cancer or local recurrence.
StatisticsAll analyses were performed using SPSS soft ware, version 11 (SPSS Inc, Chicago, IL). Diff erences
in the distributi ons of pati ent characteristi cs were analyzed with the χ2 test. Diff erences between
characteristi cs such as tumor diameter were tested with the t test. We performed analyses of
survival using the Kaplan-Meier method. Diff erences associated with a P < 0.05 were considered
signifi cant. Follow-up and survival rates were calculated from the date of primary surgery to the data
of last examinati on or death.
Results
PatientsFrom March 2000 unti l June 2006, 457 pati ents from 15 centers were registered (see Appendix). All
centers had fulfi lled the quality criteria. The median number of registered pati ents per center was 21
(range, three to 113 pati ents). In 403 pati ents, a senti nel node procedure according to the protocol
was performed. The clinical characteristi cs of these pati ents are listed in Table 1. In 127 (31.5%) of

| 67
403 patients, pathology showed ≥ one metastatic sentinel node, and therefore, a total of 276 (68.5%)
of 403 patients were eligible for the observational study.
Table 1. Characteristics of 403 Patients Who Underwent the Sentinel Node Procedure According to
the Protocol
Characteristic No. of Patients %
Location of primary tumor * Lateral Midline
151252
37.562.5
Disease Unifocal Multifocal
377 26
93.56.5
Treatment of vulvar tumor Wide local excision Radical vulvectomy Radiotherapy §
358 41 4
88.810.2
1.0
* A lateral tumor is defined as a tumor that has a median margin located ≥ 1cm from the midline. A midline tumor is defined as a tumor that has a median margin located < 1cm from the midline.§ Because of localization close to the anal sphincter.
Sentinel Node CharacteristicsIn 623 groins of 403 patients, a sentinel node procedure was performed (183 patients only unilateral).
In 163 groins (26.2%), metastatic sentinel node(s) were found. Routine pathologic examination
detected 95 (58.3%) of 163 groins with metastatic sentinel nodes, and ultrastaging 68 (41.7%) of 163
groins with metastatic sentinel nodes.
Short-Term and Long-Term ComplicationsFor analyses of short-term morbidity, only patients who underwent a sentinel node procedure
and inguinofemoral lymphadenectomy within the same procedure were included (n=47). In the
observational study, 12 patients underwent inguinofemoral lymphadenectomy in the contralateral
groin. For morbidity analyses, they were included in the lymphadenectomy group. Fourteen patients
were excluded because they received radiotherapy instead of lymphadenectomy, three patients
refused, two patients died, and one patient had recurrent disease before start of adjuvant treatment.
Both short-term and long-term morbidity were less common in patients who underwent sentinel
node removal alone compared with patients with a metastatic sentinel node who subsequently
underwent inguinofemoral lymphadenectomy (Table 2). Patients who received postoperative
radiotherapy in addition to lymphadenectomy experienced recurrent erysipelas more frequently
Sentinel node dissection early-stage vulvar cancer in

68 | Chapter 5
than patients who underwent lymphadenectomy without postoperative radiotherapy (5.9% v 30.6%,
respectively; P < 0.0001). The median hospital stay for patients after sentinel node removal only was
8.4 days compared with 13.7 days for patients who underwent an inguinofemoral lymphadenectomy
immediately after a sentinel node was found positive at frozen section (P < 0.0001).
table 2. Short- and Long-term Morbidity After SLN Procedure Alone Compared with SLN with
Subsequent Inguinofemoral Lymphadenectomy
Morbidity SLN dissection only
SLN dissection plus lymphadenectomy
P
Short term Total No. of patients Wound breakdown, groin No. of patients % Cellulitis No. of patients % Hospital stay, days
264
3111.7
124.58.4
47*
1634.0
1021.313.7
< 0.0001
< 0.0001
<0.0001
Long term Total No. of patients Lymphedema No. of patients % Recurrent erysipelas No. of patients %
264
51.9
10.4
119†
3025.2
19‡
16.2
<0.0001
<0.0001
Abbreviation: SLN, sentinel lymph node.* For comparison of short-term morbidity, only patients who had a complete lymphadenectomy within the same pro-cedure as the SLN dissection procedure were included in the analysis (n=47).† Long-term morbidity was compared between 264 patients after SLN dissection only (276 patients in the observational study minus four patients who had unilateral lymphadenectomy because of an SLN dissection that was not found, and minus eight patients who had one positive node in one groin in the observational study and had a lymphadenectomy on the contralateral side) and 119 patients who had undergone full lymphadenectomy either in the same session as the SLN procedures or at a second procedure (n=119).‡ Out of a total of 117 patients.
Stopping RulesIn October 2003, of 139 patients with a negative sentinel node on study, two patients with multifocal
disease (two separate vulvar lesions that were injected separately) and a negative sentinel node
suffered from a groin recurrence within a short period of time. Despite the fact that the stopping
rules had not yet been activated, it was decided to amend the protocol and to further exclude
patients with multifocal disease. This amendment was approved by the ethics committees in all

| 69
participating centers. Figure 1 shows the performance of the stopping rule for the observational
study in unifocal patients at the time of activation because of passing the safety border. At that
time, the groin recurrence rate for patients who had completed 2 years of follow-up (n=126) was
4.0% (95% CI, 1.6% to 8.0%). After reaching the number of 259 patients with unifocal disease and a
negative sentinel node, the study was closed in June 2006.
Follow-Up in Sentinel Node-Negative PatientsGroin recurrences
The median follow-up time of 276 patients in the observational study (17 with multifocal disease)
was 35 months (range, 2 to 87 months; date of final analysis: July 1, 2007). Four patients without
recurrence were lost to follow-up and did not complete the minimum of 24 months of follow-up.
Currently, 202 of 276 patients have completed at least 24 months of follow-up. In eight of 276
patients, groin recurrences were observed after a negative sentinel node procedure (two with
multifocal disease). The actuarial groin recurrence rate after two years was 3% (95% CI, 1% to 6%)
for all patients and 2.3% (95% CI, 1.0% to 5.0%) for patients with unifocal disease. Median time
to groin recurrence was 12 months (range, 5 to 16 months; Figure 2A). All patients with a groin
recurrence underwent a bilateral inguinofemoral lymphadenectomy and adjuvant (chemo)radiation.
Locoregional control was achieved in four of eight patients. Six patients died of disease, whereas two
are alive without evidence of disease (50 and 6 months after treatment of recurrence). Two patients
had only one sentinel node removed, whereas the lymphoscintigram showed two sentinel nodes.
Two patients had micrometastases at ultrastaging that were only detected at pathology review. In
the remaining four patients, no obvious explanation for failure was found, but two of the patients
had multifocal disease.
Local recurrences and disease-specific and overall survival
During follow-up, 16 (5.8%) of 276 patients died of intercurrent disease, and 10 patients (3.6%) died
of vulvar cancer. In 34 patients (12.3%), a local recurrence occurred (median time to recurrence, 16
months; range, 2 to 67 months). Treatment in these patients was at the discretion of the individual
center. Five patients with local recurrence eventually died of distant metastases (15, 18, 22, 41, and
41 months after primary treatment). Figure 2B shows the disease-specific survival curve for patients
with negative sentinel nodes. The 3-year disease-specific survival rate for patients with unifocal
vulvar disease and negative sentinel nodes was 97.0%.
Sentinel node dissection early-stage vulvar cancer in

70 | Chapter 5
Figure 2: (A) Cumulative Proportion of Groin Recurrences in Patients with Unifocal Vulvar Cancer
and Negative Sentinel Node (Dark Blue Line); 95% CIs Are Also Given (Light Blue Lines). (B) Disease-
Specific Survival Curve for Early-stage, Unifocal Vulvar Cancer Patients with a Negative Sentinel
Node.

| 71
Discussion
This prospective study is the largest study on surgical techniques ever performed in vulvar cancer.
The low groin recurrence rate (3% including multifocal disease; 2.3% in unifocal vulvar disease) and
excellent disease-specific survival rate of 97% at 3 years in sentinel node-negative patients suggest
that the sentinel node procedure is a safe alternative to elective inguinofemoral lymphadenectomy
for selected vulvar cancer patients. Apart from two small, single-institution series from which no
conclusions with respect to efficacy and safety could be drawn, comparable data in vulvar cancer do
no exist.32,33 The primary end point in our study was groin recurrence rate because groin recurrences
are often fatal9 and of major concern when considering a less radical approach of the groin in vulvar
cancer. Groin recurrence rates in often small, retrospective studies vary from 0% to 5.8% for lymph
node-negative patients8,10,11 (see Appendix). The groin recurrence rate in sentinel node-negative
patients in the current study seems to be at least comparable to that reported for patients with
early-stage vulvar cancer treated with formal lymphadenectomy of any type.
The nodal recurrence risk may seem less favorable when compared with that seen after the
sentinel node procedure in the treatment of breast cancer (0.1 to 0.3%).35 This might be partly
explained by the fact that the majority of breast cancer patients will receive adjuvant treatment after
surgery, whereas vulvar cancer patients with a negative sentinel node do not receive any adjuvant
treatment. However, from studies where the sentinel node procedure was followed by formal
lymphadenectomy, the variation in false-negative rates (range, 0% to 27%; average, 6.7%)17 seems to
be higher in breast cancer than the variation found for the sentinel node procedure in vulvar cancer
(typically 0% to 2%).
The excellent performance of the sentinel node technique in vulvar cancer is perhaps surprising
given that the accuracy of the sentinel node procedure is strongly associated with the experience
of the surgeon. In the Axillary Lymphatic Mapping Against Nodal Axillary Clearance trial in breast
cancer, centers were only allowed to participate after at least 40 successful sentinel node procedures
followed by full axillary lymphadenectomy.21 Even in countries where treatment of vulvar cancer
is centralized, such figures are not realistic because of the rarity of the disease. It may be that
the more superficial location of the inguinofemoral region compared with the axillary region
facilitates easier and thus more accurate detection, even by less experienced surgeons such as in
our multicenter study. However, in depth analysis of our eight patients with false-negative results
revealed surgeon- and procedure-related factors in four of eight patients, stressing the necessity of
strict adherence to the sentinel node protocol by the entire multidisciplinary team to prevent false-
negative results. Therefore, implementation of the sentinel node procedure in routine treatment of
early-stage vulvar requires quality control at each step of this multidisciplinary procedure, including
injection of radioactive tracer by either the surgeon or a nuclear medicine physician familiar with
vulvar anatomy, careful interpretation of lymphoscintigram, a surgeon with successful experience
Sentinel node dissection early-stage vulvar cancer in
72 | Chapter 5
(sentinel node procedure followed by full lymphadenectomy) in at least 10 patients, and a pathology
department experienced in ultrastaging of the sentinel nodes. All sentinel nodes that are negative at
routine HE examination need to be further analyzed by ultrastaging. Finally, to keep the experience
at a high level, an exposure of at least five to 10 patients per year per surgeon should be regarded as
a minimum figure. In a rare tumor such as vulvar cancer, this will require centralization of early-stage
vulvar cancer treatment in oncology centers.
Two years after activation of the study, a protocol amendment was made when two groin
recurrences occurred in 19 patients with multifocal disease. Analysis revealed that peritumoral
injection of the tracer in multifocal disease seemed likely to not be representative of the extent of
the tumors. Fortunately, no further recurrences were observed in the additional 19 patients with
negative sentinel nodes already registered on the study. If all patients with multifocal disease are
excluded, only six groin recurrences occurred, pointing to an even lower groin recurrence rate (six of
259 patients; 2.3%; 95% CI, 1% to 5%). Apart from multifocal disease, we also excluded patients with
tumors greater than 4cm from our study. Although this figure was arbitrarily chosen, representative
injection of tracer around larger tumors is less likely. Furthermore, nodal involvement increases with
lesion size, and alterations in lymphatic flow that may occur with large involved nodes could further
increase the likelihood of false-negative results.35
The main purpose of the introduction of the sentinel node technique in early-stage vulvar cancer
is reduction of treatment-related morbidity in patients without metastatic nodes. We have shown
that sentinel node removal alone resulted in less short- and long-term morbidity compared with
inguinofemoral lymphadenectomy. The rates of short- and long-term morbidity after inguinofemoral
lymphadenectomy in this study were comparable to those reported in the literature.10,12-14 Long-
term morbidity was especially high in patients who underwent inguinofemoral lymphadenectomy
followed by radiotherapy. In the ongoing Groningen International Study on Sentinel Nodes in
Vulvar Cancer-II study, patients with a metastatic sentinel node will receive radiotherapy instead of
inguinofemoral lymphadenectomy to reduce morbidity caused by double-modality treatment.
In conclusion, our study demonstrates that the introduction of the sentinel node procedure in
the management of early-stage vulvar cancer performed by a quality-controlled multidisciplinary
team results in decreased morbidity without compromising groin recurrence or survival rates.
Sentinel node detection should be discussed as a safe treatment option when counseling a patient
with unifocal, early-stage vulvar cancer.
| 73
References
1. Booth H, Cooper N, Quinn M (eds): Cancer statistics registration: Registration of cancer diagnosed in 2000, England. http://www.statistics.gov.uk/downloads/theme_healthy/ Mb1_31/Mb1_31.pdf
2. U.S. Cancer Statistics Working Group. United States Cancer Statistics: 2003 Incidence and Mortality. Atlanta: US Department of Health and Human Services, Centers for Disease Control and Prevention, and National Cancer Institute, 2006.
3. Hemminki K, Li X, Vaittinen P. Time trends in the incidence of cervical and other genital squamous cell carcinomas and adenocarcinomas in Sweden, 1958-1996. Eur J Obstet Gynecol Reprod Biol 2002;101:64-69.
4. Homesley HD, Bundy BN, Sedlis A, et al. Assessment of current International Federation of Gynecology and Obstetrics staging of vulvar carcinoma relative to prognostic factors for survival (A Gynecologic Oncology Group study). Am J Obstet Gynecol 1991;164:997-1004.
5. Burger MP, Hollema H, Emanuels AG, et al. The importance of the groin node status for the survival of T1 and T2 vulval carcinoma patients. Gynecol Oncol 1995;57:327-334.
6. Hacker NF, Leuchter RS, Berek JS, et al. Radical vulvectomy and bilateral inguinal lymphadenectomy through separate groin incisions. Obstet Gynecol 1981;58:574-579.
7. De Hullu JA, Hollema H, Lolkema S, et al. Vulvar carcinoma: The price of less radical surgery. Cancer 2002;95:2331-2338.
8. Bell JG, Lea JS, Reid GC. Complete groin lymphadenectomy with preservation of the fascia lata in the treatment of vulvar carcinoma. Gynecol Oncol 2000;77:314-318.
9. Katz A, Eifel PJ, Jhingran A, et al. The role of radiation therapy in preventing regional recurrences of invasive squamous cell carcinoma of the vulva. Int J Radiat Oncol Biol Phys 2003;57:409-418.
10. Stehman FB, Bundy BN, Dvoretsky PM, et al. Early stage I carcinoma of the vulva treated with ipsilateral superficial inguinal lymphadenectomy and modified radical hemivulvectomy: a prospective study of the Gynecologic Oncology Group, Obstet Gynecol 1992;79:490-497.
11. Kirby TO, Rocconi RP, Numnum TM, et al. Outcomes of stage I/II vulvar cancer patients after negative superficial inguinal lymphadenectomy. Gynecol Oncol 2005;98:309-312.
12. De Hullu JA, Ansink AC, Tymstra T, et al. What doctors and patients think about false-negative sentinel lymph nodes in vulvar cancer. J Psychosom Obstet Gynaecol 2001;22:199-203.
13. Rouzier R, Haddad B, Dubernard G, et al. Inguinofemoral dissection for carcinoma of the vulva: effect of modifications of extent and technique on morbidity and survival. J Am Coll Surg 2003;196:4442-4450.
14. Gaarenstroom KN, Kenter GG, Trimbos JB, et al. Postoperative complications after vulvectomy and inguinofemoral lymphadenectomy using separate groin incisions. Int J Gynecol Cancer 2003;13:522-527.
15. Oonk MH, Hollema H, de Hullu JA, et al. Prediction of lymph node metastases in vulvar cancer: a review. Int J Gynecol Cancer 2006;16:963-971.
16. Selman TJ, Luesley DM, Acheson N, et al. A systematic review of the accuracy of diagnostic tests for inguinal lymph node status in vulvar cancer. Gynecol Oncol 2005;99:206-214.
17. Kim T, Giuliano AE, Lyman GH. Lymphatic mapping and sentinel lymph node biopsy in early-stage breast carcinoma: a metaanalysis. Cancer 2006;106:4-16.
18. Thompson JF, Shaw HM. Sentinel node mapping for melanoma: results of trials and current applications. Surg Oncol Clin N Am 2007;16:35-54.
19. Purushotham AD, Upponi S, Klevesath MB, et al. Morbidity after sentinel lymph node biopsy in primary breast cancer: results from a randomized controlled trial. J Clin Oncol 2005;23:4312-4321.
Sentinel node dissection early-stage vulvar cancer in

74 | Chapter 5
20. Veronesi U, Paganelli G, Viale G, et al. Sentinel-lymph-node biopsy as a staging procedure in breast cancer: update of a randomised controlled study. Lancet Oncol 2006;7:883-890.
21. Mansel RE, Fallowfield L, Kissin M, et al. Randomized multicenter trial of sentinel node biopsy versus standard axillary treatment in operable breast cancer: the ALMANAC Trial. J Natl Cancer Inst 2006;98:599-609.
22. Wilke LG, McCall LM, Posther KE, et al. Surgical complications associated with sentinel lymph node biopsy: results from a prospective international cooperative group trial. Ann Surg Oncol 2006;13:491-500.
23. Lucci A, McCall LM, Beitsch PD, et al. Surgical complications associated with sentinel lymph node dissection (SLND) plus axillary lymph node dissection compared with SLND alone in the American College of Surgeons Oncology Group Trial Z0011. J Clin Oncol 2007;25:3657-3663.
24. Ansink AC, Sie-Go DMDS, van der Velden J, et al. Identification of sentinel lymph nodes in vulvar carcinoma patients with the aid of a patent blue V injection. Cancer 1999;86:652-656.
25. De Cicco C, Sideri M, Bartolomei M, et al. Sentinel node biopsy in early vulvar cancer. Brit J Cancer 2000;82:295-299.
26. De Hullu JA, Hollema H, Piers DA, et al. Sentinel lymph node procedure is highly accurate in squamous cell carcinoma of the vulva. J Clin Oncol 2000;18:2811-2816.
27. Levenback C, Coleman RL, Burke TW, et al. Intraoperative lymphatic mapping and sentinel node identification with blue dye in patients with vulvar cancer. Gynecol Oncol 2001;83:276-281.
28. Sliutz G, Reinthaller A, Lantzsch T, et al. Lymphatic mapping of sentinel nodes in early vulvar cancer. Gynecol Oncol 2002;84:449-452.
29. Moore RG, DePasquale SE, Steinhoff MM, et al. Sentinel node identification and the ability to detect metastatic tumor to inguinal lymph nodes in squamous cell cancer of the vulva. Gynecol Oncol 2003;89:475-479.
30. Puig-Tintoré LM, Ordi J, Vidal-Sicart S, et al. Further data on the usefulness of sentinel lymph node identification and ultrastaging in vulvar squamous cell carcinoma. Gynecol Oncol 2003;88:29-34.
31. De Hullu JA, Doting E, Piers DA, et al. Sentinel lymph node identification with Technetium-99m- labeled nanocolloid in squamous cell cancer of the vulva. J Nucl Med 1998;39:1381-1385.
32. Vidal-Sicart S, Puig-Tintoré LM, Lejárcegui JA, et al. Validation and application of the sentinel lymph node concept in malignant vulvar tumours. Eur J Nucl Mol Imaging 2007;34:384-391.
33. Nyberg RH, Iivonen M, Parkkinen J, et al. Sentinel node and vulvar cancer: a series of 47 patients. Acta Obstet Gynecol Scand 2007;86:615-619.
34. Terada KY, Shimizu DM, Jiang CS, et al. Outcomes for patients with T1 squamous cell cancer of the vulva undergoing sentinel node biopsy. Gynecol Oncol 2006;102:200-203.
35. de Hullu JA, Oonk MH, Ansink AC, et al. Pitfalls in the sentinel lymph node procedure in vulvar cancer. Gynecol Oncol 2004;94:10-15.

| 75
Appendix
Quality Control of the Sentinel Node Procedure Before Start of Participation in the StudySuccessful experience with the sentinel node procedure and subsequent inguinofemoral
lymphadenectomy needed to be documented in at least 10 patients. Successful was defined
as identification of the sentinel node(s) and no false-negative results. When false-negative
results occurred, another five patients needed to have procedure performed with subsequent
inguinofemoral lymphadenectomy before patients could be included in the Groningen International
Study on Sentinel Nodes in Vulvar Cancer (GROINSS-V).
Detailed Treatment Protocol of GROINSS-VSentinel node detection protocol
The day before the operation, 0.5 mL of 100 MBq technetium-99m (99mTc) -labeled nanocolloid (Solco
Nuclear, Birsfelden, Switzerland) with a particle size of less than 80 nm was injected circumferentially
intradermally on four locations (each 0.05 mL of 15 MBq 99mTc-labeled nanocolloid) around the
primary tumor. A half an hour before the injections, lidocaine-prilocaine 5% cream (EMLA; Astra
Pharmaceuticals, LP, Westborough, MA) was applied on the vulva for pain relief. Anterior images
were obtained using a single-head gamma camera with a low-energy, high-resolution collimator.
Within 5 minutes after injection, dynamic imaging was started within 30-second frames during 30
minutes. An anterior and lateral static image was obtained after 2.5 hours. To facilitate interpretation,
transmission scanning was performed simultaneously using the 120-KeV gamma rays of a cobalt-57
flood source. The first appearing persistent focal accumulation was considered to be a sentinel node,
especially when a direct connection from the injection site to the sentinel inguinofemoral lymph
node was visible. The site of the sentinel node was marked with a pencil on the overlying skin.
Before the operation, the gynecologic oncologist and the nuclear medicine physician looked at the
lymphoscintigram to see how many sentinel nodes must be removed. The next day, after induction of
anesthesia, approximately 2.0 mL of patent blue-V (2.5% in aqueous solution containing 0.6% sodium
chloride and 0.05% disodium hydrogen phosphate; Laboratoire Guerbet, Aulney-Sous-Bois, France)
was injected intradermally in the same four locations around the primary tumor approximately
5 to 10 minutes before the surgical procedure. The surgical procedure started with identification
and removal of the sentinel nodes. During operation, a handheld gamma-ray detection probe
(Neoprobe, Dublin, OH) was used to confirm the lymphoscintigraphy marked area of greatest activity
in the groin. A small skin incision was made at the marked spot, and a sentinel node excision biopsy
was performed using the handheld gamma-ray detector and by dissection of blue-stained lymph
vessels. The sentinel nodes were sent for frozen section to the pathologist (optional). Subsequently,
Sentinel node dissection early-stage vulvar cancer in

76 | Chapter 5
resection of the vulvar lesion was performed. When identification of the sentinel nodes was not
successful because of low radioactivity, the primary tumor was removed first. By resection of the
primary tumor together with the primary nanocolloid injection sites, the radiation background is
greatly reduced, allowing easier identification of the sentinel nodes, especially when the primary
tumor is near the groins. After removal of the sentinel nodes, the biopsy bed was re-examined for
radioactivity, and if higher than 10% of the first excised lymph node, the dissection was continued in
search of additional sentinel nodes. These were also sent to the pathologist for frozen section. The
pathologist had to report not only the absence or presence of a lymph node metastasis, but also the
total number of removed sentinel nodes from each groin.
Surgical treatment protocol
Treatment consisted of excision of the primary tumor in combination with the sentinel node
procedure. Only when sentinel nodes were positive was unilateral or bilateral inguinofemoral
lymphadenectomy by separate incisions performed. The lymphadenectomy was performed
immediately after the sentinel node procedure when frozen section showed lymph node metastases.
When the frozen section was negative but definitive histopathologic examination (including
multiple sectioning and immunohistochemistry) showed metastatic disease, lymphadenectomy
was performed in a second operation. In case of a positive sentinel node on one side and negative
sentinel node on the other side, full lymphadenectomy was only performed on the side with the
positive sentinel node. However, in case of a real midline tumor, unilateral flow was considered as a
technical failure, and complete inguinofemoral lymphadenectomy was performed in the side without
sentinel node identification. When the tumor did not cross the midline but the medial margin of the
tumor was within 1cm from the midline, in the majority of the patients, bilateral lymph drainage was
visualized on the lymphoscintigram. However, in case of unilateral lymph flow, a unilateral sentinel
lymph node procedure was sufficient if the sentinel node procedure was performed according to the
protocol. Separate incisions for the lymphadenectomy were made parallel to the inguinal ligament,
and then the node-bearing fat pad was removed. The extent of the dissection was the inguinal
ligament cephalad, the adductor longus muscle medially, and the sartorius muscle inferolaterally.
After opening of the cribiform fascia, all node-bearing fatty tissue medially from the femoral vein
was removed as well. The vulvar excision varied with the location of the lesion. The standard local
treatment was radical local excision with tumor-free margins of at least 1cm.
Histopathology
The pathologist received the sentinel node(s) and, if applicable, the lymphadenectomy specimens
separately. Initially, the sentinel nodes were cut in the middle for frozen section and cytologic
specimen. Later on, from every half, four sections were cut for haematoxylin and eosin staining
(routine histopathologic examination). Of all sentinel nodes that were negative on routine

| 77
histopathologic examination, additional pairs of sections were subsequently cut, with three
sections per millimeter. One section of each pair was stained with haematoxylin and eosin, and
the other section was immunostained with cytokeratin 1% AE1:AE3 antikeratin solution (Boehringer
Mannheim, Mannheim, Germany). From the lymphadenectomy specimens, all lymph nodes were
studied individually. One section per 0.5cm diameter of the nodes was cut for haematoxylin and
eosin staining.
Detailed Statistical DesignTo check the efficacy of our treatment protocol, stopping rules were defined. These rules regard the
occurrence of groin recurrences. The rules were based on sequential analysis, with α and β spending
properties. The boundaries of the rules were derived from a higher incidence I0 and a lower incidence
I1, assuming binomial distribution. The upper unsafe boundary was approximated by the maximal
number of events UB to be accepted after n consecutive patients: UB(n) = integer(n x I1 + (Z(alpha) +
CTC) x SD(I1) + 0.5). The maximal number of patients needed was: N(ub) = (((Z(alpha) + CTC) x (I1 x (1
–I1))^0.5 + Z(beta) x (I0 x (1–I0))^0.5)/(I0 –I1))^2. In these equations, CTC was the so-called Christmas
Tree Correction (Whitehead J. The Design and Analysis of Sequential Clinical Trials [ed 2]. Chichester,
United Kingdom, Wiley, 1997). Z(alpha) and Z(beta) were constant and chosen in such a way that the
cumulative probabilities to pass the boundary did meet the preset Cum(alpha) for I1 and Cum(beta)
for I0. In analogy, the approximation for the minimal number of events LB was: LB(n) = integer(n x
I0 –(Z(alpha) + CTC) x SD(I0) + 0.5). The minimal number of patients needed was: N(lb) = (((Z(alpha)
+ CTC) x (I0 x (1 –I0))^0.5 + Z(beta) x (I1 x (1 –I1))^0.5)/(I0 –I1))^2. Because the boundaries were
only rough approximations in case of low values of I0 and I1 and because the probability to pass one
boundary was influenced by the probability to pass the other one, all probabilities were computed
exactly. The rule for patients with a negative sentinel node, with I0=0.08, I1=0.02, Cum(alpha)=0.05,
and Cum(beta)=0.90 was used. For the unsafe boundary (Z(alpha) + CTC)=1.978 (corresponding to a
nominal value of α =0.024), and Z(beta)=1.345, with N(ub)=115. For the safe boundary, these values
were 1.611 (0.054), 1.669, and 125. The cumulative probabilities to pass the boundaries of the rules
were used. Monitoring of the data, entered in a spreadsheet, was continuous. The individual follow-
up times were adjusted automatically on a daily basis. Events were also entered. The stopping rule
was activated when the upper (unsafe) boundary was passed after k patients, irrespective of the
individual follow-up intervals of the k patients; or when the lower (safe) boundary was passed after k
patients, provided that all k patients had completed their follow-up; or when neither boundary was
passed after the maximum number of patients had all completed their follow-up.
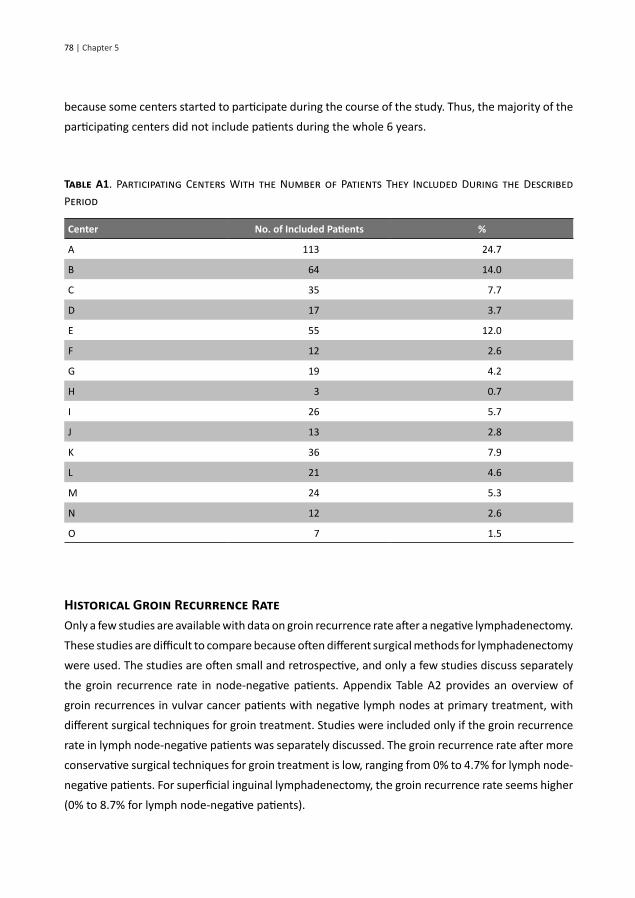
Participating CentersAppendix Table A1 lists the number of included patients per center. The number of included patients
per center cannot be interpreted as the number of patients included per center during 6 years
Sentinel node dissection early-stage vulvar cancer in
78 | Chapter 5
because some centers started to participate during the course of the study. Thus, the majority of the
participating centers did not include patients during the whole 6 years.
Table A1. Participating Centers With the Number of Patients They Included During the Described
Period
Center No. of Included Patients %
A 113 24.7
B 64 14.0
C 35 7.7
D 17 3.7
E 55 12.0
F 12 2.6
G 19 4.2
H 3 0.7
I 26 5.7
J 13 2.8
K 36 7.9
L 21 4.6
M 24 5.3
N 12 2.6
O 7 1.5
Historical Groin Recurrence RateOnly a few studies are available with data on groin recurrence rate after a negative lymphadenectomy.
These studies are difficult to compare because often different surgical methods for lymphadenectomy
were used. The studies are often small and retrospective, and only a few studies discuss separately
the groin recurrence rate in node-negative patients. Appendix Table A2 provides an overview of
groin recurrences in vulvar cancer patients with negative lymph nodes at primary treatment, with
different surgical techniques for groin treatment. Studies were included only if the groin recurrence
rate in lymph node-negative patients was separately discussed. The groin recurrence rate after more
conservative surgical techniques for groin treatment is low, ranging from 0% to 4.7% for lymph node-
negative patients. For superficial inguinal lymphadenectomy, the groin recurrence rate seems higher
(0% to 8.7% for lymph node-negative patients).

| 79
Table A2. Overview of Literature: Groin Recurrences After Negative Lymph Nodes at Primary
Treatment
Study* No. of Lymph Node-Negative Patients
Treatment of the Groins
Groin Recurrences (%)
Hacker et al 75 IL 0
Berman et al 49 SIL 0
Stehman et al 121 SIL 5.8
Burke et al 76 SIL 5
Burger et al 119 IL en bloc 0
Bell et al 39 IL† 0
Rodolakis et al 211 105 IL en bloc; 106 IL 1.6
Maggino et al 296 IL en bloc / IL / SIL 4.7‡
Gordinier et al 104 SIL 8.7
Kirby et al 65 SIL 4.6
Gonzalez Bosquet et al 217 IL en bloc / IL / SIL 0.5§
Woolderink et al 91 SIL 5
Abbreviations: IL, inguinofemoral lymphadenectomy (through separate incisions); IL en bloc, inguinofemoral lymphad-enectomy en bloc; SIL, superficial inguinal lymphadenectomy.* References for studies are as follows: Hacker NF, Leuchter RS, Berek JS, et al. Obstet Gynecol 58:574-579, 1981; Ber-man ML, Soper JT, Creasman WT, et al. Gynecol Oncol 35:352-357, 1989; Stehman FB, Bundy BN, Dvoretsky PM, et al. Obstet Gynecol 79:490-497, 1992; Burke TW, Levenback C, Coleman RL, et al. Gynecol Oncol 57:215-220, 1995; Burger MP, Hollema H, Emanuels AG, et al. Gynecol Oncol 57:327-334, 1995; Bell JG, Lea JS, Reid GC. Gynecol Oncol 77:314-318, 2000; Rodolakis A, Diakomanolis E, Voulgaris Z, et al. Gynecol Oncol 78:346-351, 2000; Maggino T, Landoni F, Sar-tori E, et al. Cancer 89:116-122, 2000; Gordinier ME, Malpica A, Burke TW, et al. Gynecol Oncol 90:625-628, 2003; Kirby TO, Rocconi RP, Numnum TM, et al. Gynecol Oncol 98:309-312, 2005; Gonzalez-Bosquet J, Magrina JF, Gaffey TA, et al. Gynecol Oncol 97:828-833, 2005; Woolderink JM, de Bock GH, de Hullu JA, et al. Gynecol Oncol 103:293-299, 2006.† With preservation of the fascia lata.‡ Not specified by type of groin surgery.§ One patient with a groin recurrence after superficial inguinal lymphadenectomy.
Sentinel node dissection early-stage vulvar cancer in