Embed Size (px)
Citation preview
University of Groningen
Oral health benefits of chewing gumWessel, Stefan
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2016
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Wessel, S. (2016). Oral health benefits of chewing gum [Groningen]: Rijksuniversiteit Groningen
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 23-07-2018
Effects of chewing gum with and
without active ingredients on oral
biofilm viability and composition
Chapter 3

CHAPTER 3
32
3
Abstract
Objectives
Chewing gum has developed into an oral care agent with multiple oral health benefits.
Active ingredients can be incorporated in chewing gum to improve the oral health benefits
of chewing gum. The aim of this study was to evaluate two chewing gums with widely
different active ingredients (Magnolia bark extract (MBE) and sodium hexametaphosphate
(SHMP)) for four weeks in vivo with respect to the total number of bacteria in oral biofilms
and their viability as well as with respect to the composition of the biofilm.
Methods
Ten healthy volunteers chewed gum with and without MBE or SHMP three times per day
for four weeks, during which oral biofilm was collected. Subsequently, the total number,
viability and composition of bacteria in the biofilm collected were determined.
Results
During four weeks of chewing gum use, both gums with and without active ingredients
yielded no significant decreases in the total numbers of bacteria and their viability in oral
biofilm. A trend of increasing diversity of the bacterial composition of the biofilms collected
was observed for all gums, including control gums without active ingredients added.
Conclusions
The chewing of sugar-free gum on a daily basis for a prolonged period of time can slowly
shift the bacterial composition of the oral biofilm in a more diverse and therewith healthy
direction, regardless of the addition of active ingredients such as MBE or SHMP.

EFFECTS OF CHEWING GUM ON ORAL BIOFILM VIABILITY AND COMPOSITION
33
3
Introduction
Oral health and disease centers around the formation and removal of oral biofilm as the
main cause of oral diseases such as caries, gingivitis or periodontitis. Planktonic bacteria
in saliva adhere to the salivary conditioning films on oral soft and hard surfaces and form a
matrix of extracellular polymeric substances which gives structure to the biofilm and shields
its inhabitants from environmental influences (1). During oral health, the bacterial
composition of the oral microbiome is diverse and in symbiosis with the host (2).
Pathogenicity arises when a unbalance in symbiosis occurs causing a shift in the
composition of the oral microbiome, in which pathogenic strains dominate (3). For instance,
strains that use environmental sugars to produce acids, lower the pH and demineralize the
enamel causing caries. Periodontopathogens cause an inflammatory response in the
gingiva, leading to gingivitis or in more severe cases periodontitis. In case of caries it has
been shown that as the disease progresses, the overall diversity of the oral microbiome
decreases (4). Maintaining oral health largely involves preventing a shift in oral microbiome
composition towards a pathogenic direction and is mainly achieved by regularly performing
mechanical procedures to remove the oral biofilm not targeted towards specific pathogenic
strains or species, such as toothbrushing, flossing and the use of toothpicks. Additionally
special dentifrice formulations, mouthrinses and chewing gums have been promoted to
enhance oral health (5,6). However, the majority of the studies on oral microbiome
composition focus on saliva and not on oral biofilm, despite the fact it is particularly the
biofilm and not the salivary microbiome that stimulates the development of diseases (7).
Chewing gum has developed in the past centuries from a candy into an oral
health care agent and functional food product. Sugar-free gum has multiple oral health
benefits mainly by increasing salivary flow (8), washing away food debris (9) and
neutralizing oral biofilm pH (10). Daily use of sugar-free chewing gum for one year or more,
especially when consumed after a meal, is effective in reducing the incidence of caries
(11,12).
The main component of chewing gum is the gum base, consisting of a mixture of
elastomers, like polyvinylacetate or polyisobutylene. The gum base is complemented with
softeners, texturizers, emulsifiers and plasticizers. Based on desired functionality,
formulation of the latter ingredients is adapted, for instance to generate a gradual release
profile of active ingredients from chewing gum into the oral cavity. Prolonged presence
and substantive action in the oral cavity make chewing gum a good vehicle to deliver active
ingredients that promote oral health (13,14). Highly diverse ingredients have been added to
chewing gum for various purposes. Magnolia bark extract (MBE) applied in chewing gum

CHAPTER 3
34
3
reduces the total number of salivary bacteria, including the number cariogenic
Streptococcus mutans (15,16). MBE is also advocated for a broad range of disorders such
as coughing, fever, pain relief and diarrhea (15,17). Its active components include
magnolol and honokiol which both possess antimicrobial properties (18). Another totally
different active ingredient applied in chewing gum is sodium hexametaphosphate (SHMP).
SHMP is a surface active agent, inhibiting the formation of extrinsic tooth stain when
supplemented in chewing gum (19,20) and creating a more hydrophilic enamel surface in
vivo (21). The main hurdle in demonstrating efficacy of active ingredients applied in
chewing gum is the overriding effect of the chewing action itself, stimulating salivary flow.
Moreover, since all added ingredients released by the chewing of gum are swallowed, only
low concentrations of added ingredients can be applied and as a result effects of a single
chew are relatively small compared to effects of the single use of a toothbrush. Any effects
of the chewing of gum should therefore be evaluated over a period of at least several
weeks.
The aim of this study was to evaluate two chewing gums with widely different
active ingredients (MBE and SHMP) for a prolonged period of time in vivo with respect to
the viability and composition of the oral microbiome adhering to enamel surfaces. To this
end, ten healthy volunteers chewed gum with and without MBE and SHMP three times per
day for four weeks, during which oral biofilm was collected weekly for analysis.
Materials and methods
Subjects and inclusion criteria Ten healthy volunteers (5 females and 5 males, aged between 24 and 57 years)
participated in this study. The Medical Ethical Testing Committee of the University Medical
Center Groningen (METc 2011/330) approved this study and all subjects agreed to sign a
declaration of informed consent. All volunteers had a dentition with at least 16 natural
elements and considered themselves in good health. Use of antibiotics up to three months
prior to the study or use of a mouthrinse in the month preceding the study led to exclusion
from participation. During the study, use of mouthrinse, antibiotics, mints or other chewing
gum was not allowed.
Treatment and schedule Two weeks prior to the start of the study and continuing during the entire study, volunteers
brushed their teeth with a standard fluoridated toothpaste without antimicrobial claims

EFFECTS OF CHEWING GUM ON ORAL BIOFILM VIABILITY AND COMPOSITION
35
3
(Prodent Softmint, Sara Lee Household & Bodycare, The Hague, The Netherlands)
according to their habitual routine.
After two weeks of regular brushing, at the beginning of the third week volunteers
were asked to come to the laboratory after breakfast without their morning brushing for the
collection of oral biofilm. This marked the start of four weeks of chewing two pellets of gum
three times per day. Gums with and without the active ingredients were packaged with a
code only to be disclosed after full analysis of all data at the end of the evaluation period.
Gums were randomly assigned to each volunteer. Volunteers were instructed to chew the
gum for ten minutes, with the three chewing points in time evenly spread over the day but
preferably after breakfast, lunch and dinner. The laboratory visits were repeated after one,
two and four weeks of the start of the study. After finishing the four week period with one of
the gums received, a four week washout period was taken into account during which the
volunteers solely had to brush with the standard, fluoridated toothpaste provided.
Subsequently, volunteers were given another coded batch of chewing gum and the
schedule was repeated.
Chewing gum Chewing gums were provided by Wm. Wrigley Jr. Company (Chicago, IL, USA). Active
ingredients were added to 1.5 g pellet shaped gums. MBE (3 mg, Honsea Sunshine
Biotech Co., Ltd, Guangzhou, China) was added to the coating of a gum containing:
gumbase, sorbitol, flavors, sweeteners and coolants. SHMP (7.5 % w/w Sigma Aldrich, St.
Louis, MO, USA) was added to a gum containing: gumbase, sorbitol, xylitol, glycerol,
flavors, sweeteners and coolants. Respective gums without the active ingredient added
were used as control gums.
Biofilm collection After instructions, volunteers collected oral biofilm themselves from the left upper quadrant
of the dentition (buccal, palatal, occlusal and interproximal sides of the dentition) using a
sterile hook and a cotton swab. Biofilm was suspended in 1 ml sterile Reduced Transport
Fluid (RTF) (22) and stored on ice immediately after collection. Next, biofilm samples were
sonicated 10 sec at 30 W (Vibra Cell model 375, Sonics and Materials Inc., Danbury, CT,
USA) in RTF to suspend bacterial clumps. The bacterial suspension was partly used for
bacterial viability analysis. The remainder of the suspension was stored at -20 °C for later
bacterial composition analysis.

CHAPTER 3
36
3
Bacterial viability analysis The total number of bacteria in suspension was determined using a Bürker Türk counting
chamber and expressed as the total number of bacteria collected from a volunteer at each
time of collection. Bacterial viability was determined using 20 µL of sonicated biofilm
suspension. The suspension was spread on a glass microscope slide, stained with 15 µL
of LIVE/DEAD staining solution (BacLight™, Molecular Probes Europe BV) and covered by
a coverslip. Next, images were collected using a fluorescence microscope (Leica DM 4000
B, Leica Microsystems Heidelberg GmbH, Heidelberg, Germany). At least three images
per suspension were taken at random spots, with a minimum of 100 visible bacteria. Live,
green fluorescent and dead, red fluorescent bacteria were counted and results are
expressed as the percentage of the total number of bacteria counted. Subsequently, using
the total number of bacteria and the percentage of live/dead bacteria, the total number of
live and dead bacteria per suspension was calculated and averaged over all volunteers for
each time of collection.
Bacterial composition – Denaturing Gradient Gel Electrophoresis (DGGE) To determine bacterial composition, DGGE was performed. First, frozen bacterial
suspensions were thawed and centrifuged at 18000 g for 10 min, after which the pellet was
washed by resuspension in 200 µL tris-ethylenediaminetetraacetic-acid (TE) buffer (10 mM
Tris HCl, pH 7.5, 1 mM EDTA) and centrifuged again for 10 min. Isolation of chromosomal
DNA from the biofilm bacteria was done as has been described earlier (23). The DNA
concentration was measured using a NanoDrop® Spectrophotometer (ND-100, NanoDrop
Technologies Inc., Wilmington, DE, USA) at 230 nm. Polymerase Chain Reaction (PCR)
was performed with 100 ng of DNA on a T-gradient thermocycler (Bio-rad I-Cycler, GENO-
tronics BV, USA) to amplify the universal V3 region of the 16S rRNA gene in all samples
with the F357-GC forward primer and R-518 as the reverse primer (24). Products of the
PCR were applied on an 8% (w/v) polyacrylamide gel in 0.5 x TAE buffer (20 mM Tris
acetate, 10 mM sodium acetate, 0.5 mM EDTA, pH 8.3). The denaturing gradient gel
ranged from 30 – 80% urea made from a stock solution (100% denaturant equals 7 M urea
and 37% formamide). A stacking gel without denaturant was added on top. Electrophoresis
was started 200 V for the first 10 min, and adjusted for overnight electrophoresis to 120 V
at 60 °C. Gels were subsequently stained using a silver nitrate solution (0.2% AgNO3 (w/v))
until maximum staining intensity was observed.
Gelcompar II (v6.5 Applied Maths, Sint-Martens-Latem, Belgium) was used for gel
analysis. A reference lane with known bacterial species was used on every gel to align and
compare separate gels. The presence of a band was taken as indicative of the presence of

EFFECTS OF CHEWING GUM ON ORAL BIOFILM VIABILITY AND COMPOSITION
37
3
a bacterial strain or species in the sample, regardless of the staining intensity. Dice’s
similarity coefficient was calculated according to band-based matching with 0.5%
optimization and 0.5% band tolerance as accuracy settings.
Statistical analysis Data was tested for normality using probability plots, Kolmogorov-Smirnov and Shapiro-
Wilk tests (P<0.05). Subsequently, data was assessed for an effect within subjects during
four weeks of use. In case of normality, data was analyzed using a repeated measures
ANOVA followed by a Bonferroni test for pairwise comparison otherwise, when data was
not normally distributed, using the Friedman test (P < 0.05) followed by a Wilcoxon signed
rank test to identify pairwise differences. All statistical tests were performed using SPSS
v20.0 (IBM inc., Chicago, USA)
Results
On average, volunteers collected between 4 x 108 and 8 x 108 bacteria from their left upper
quadrants. Chewing of the MBE control gum yielded lower numbers of bacteria than
chewing of the SHMP control gum, although differences were small (Fig. 1). Unfortunately
due to experimental problems, one and two week data for the MBE and its control gum are
missing. Overall, no significant decrease in numbers of bacteria collected was seen over
the four weeks period of chewing MBE gum nor its control. This is similar to what is seen
for the SHMP gum and where the control gum yielded similar bacterial numbers over the
evaluation period, use of the SHMP gum gave a small downward trend over the first two
weeks, however going up again after four weeks of use of the gum. Whether or not this
trend would also have existed in the MBE gum group, cannot be concluded from the data
available. The trends in the total numbers of bacteria collected coincided fully with changes
in the number of live bacteria collected (see also Fig. 1).
CHAPTER 3
38
3
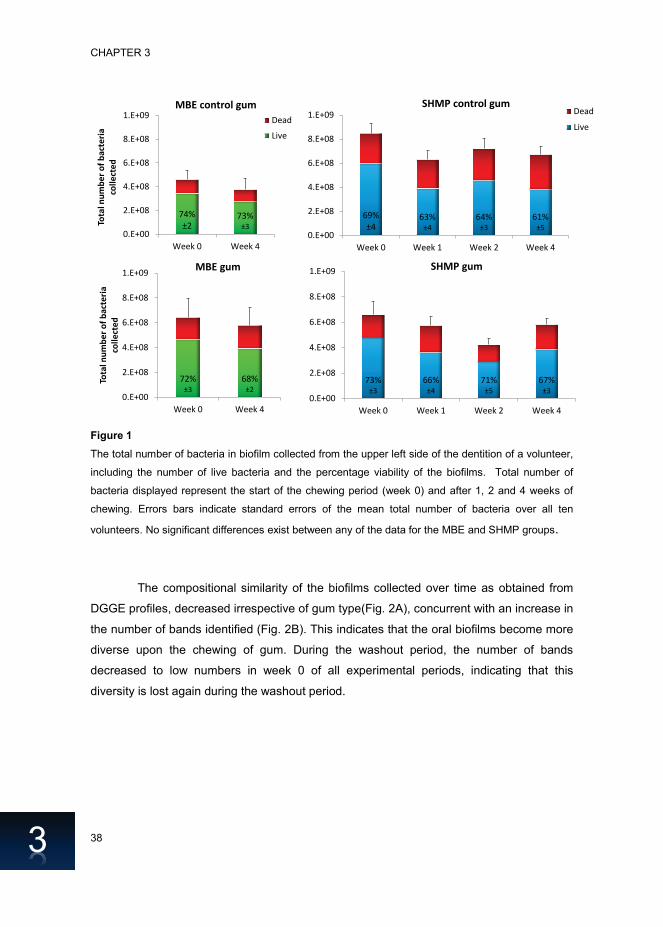
Figure 1
The total number of bacteria in biofilm collected from the upper left side of the dentition of a volunteer,
including the number of live bacteria and the percentage viability of the biofilms. Total number of
bacteria displayed represent the start of the chewing period (week 0) and after 1, 2 and 4 weeks of
chewing. Errors bars indicate standard errors of the mean total number of bacteria over all ten
volunteers. No significant differences exist between any of the data for the MBE and SHMP groups.
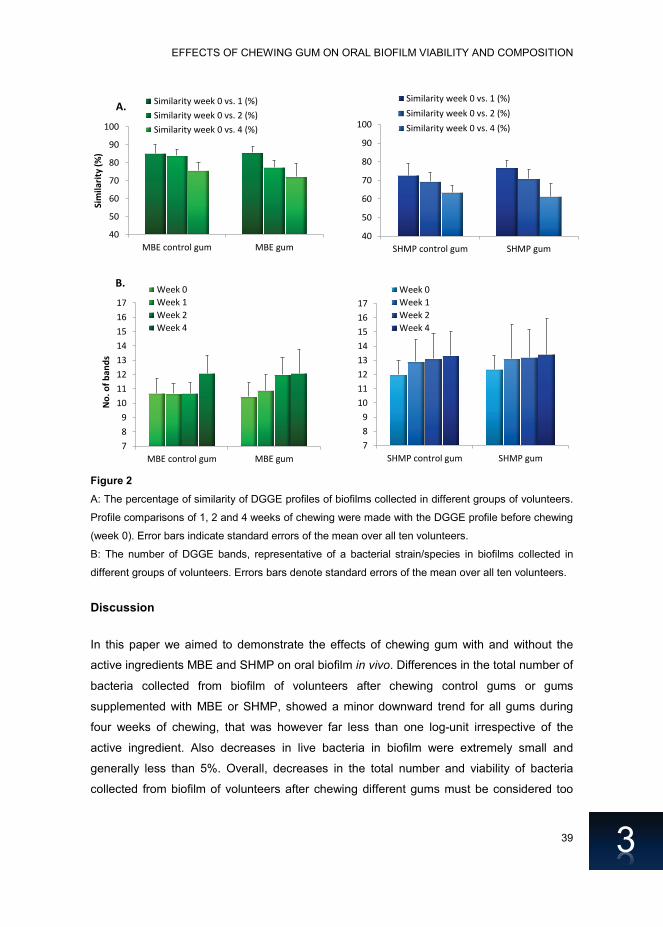
The compositional similarity of the biofilms collected over time as obtained from
DGGE profiles, decreased irrespective of gum type(Fig. 2A), concurrent with an increase in
the number of bands identified (Fig. 2B). This indicates that the oral biofilms become more
diverse upon the chewing of gum. During the washout period, the number of bands
decreased to low numbers in week 0 of all experimental periods, indicating that this
diversity is lost again during the washout period.
74%±2
73%±3
0.E+00
2.E+08
4.E+08
6.E+08
8.E+08
1.E+09
Week 0 Week 4
Tota
l num
ber o
f bac
teria
co
llect
edMBE control gum
Dead
Live
72%±3
68%±2
0.E+00
2.E+08
4.E+08
6.E+08
8.E+08
1.E+09
Week 0 Week 4
Tota
l num
ber o
f bac
teria
co
llect
ed
MBE gum
69% ±4
63% ±4
64% ±3
61% ±5
0.E+00
2.E+08
4.E+08
6.E+08
8.E+08
1.E+09
Week 0 Week 1 Week 2 Week 4
SHMP control gumDead
Live
73%±3
66%±4
71%±5
67%±3
0.E+00
2.E+08
4.E+08
6.E+08
8.E+08
1.E+09
Week 0 Week 1 Week 2 Week 4
SHMP gum
EFFECTS OF CHEWING GUM ON ORAL BIOFILM VIABILITY AND COMPOSITION
39
3
Figure 2
A: The percentage of similarity of DGGE profiles of biofilms collected in different groups of volunteers.
Profile comparisons of 1, 2 and 4 weeks of chewing were made with the DGGE profile before chewing
(week 0). Error bars indicate standard errors of the mean over all ten volunteers.
B: The number of DGGE bands, representative of a bacterial strain/species in biofilms collected in
different groups of volunteers. Errors bars denote standard errors of the mean over all ten volunteers.
Discussion
In this paper we aimed to demonstrate the effects of chewing gum with and without the
active ingredients MBE and SHMP on oral biofilm in vivo. Differences in the total number of
bacteria collected from biofilm of volunteers after chewing control gums or gums
supplemented with MBE or SHMP, showed a minor downward trend for all gums during
four weeks of chewing, that was however far less than one log-unit irrespective of the
active ingredient. Also decreases in live bacteria in biofilm were extremely small and
generally less than 5%. Overall, decreases in the total number and viability of bacteria
collected from biofilm of volunteers after chewing different gums must be considered too
789
1011121314151617
SHMP control gum SHMP gum
Week 0Week 1Week 2Week 4
789
1011121314151617
MBE control gum MBE gum
No.
of b
ands
B. Week 0Week 1Week 2Week 4
40
50
60
70
80
90
100
SHMP control gum SHMP gum
Similarity week 0 vs. 1 (%)Similarity week 0 vs. 2 (%)Similarity week 0 vs. 4 (%)
40
50
60
70
80
90
100
MBE control gum MBE gum
Sim
ilarit
y (%
)A. Similarity week 0 vs. 1 (%)
Similarity week 0 vs. 2 (%)Similarity week 0 vs. 4 (%)

CHAPTER 3
40
3
small to be clinically relevant. This conclusion coincides with previous reports stating that
the chewing of regular sugar-free gum is not effective in reducing oral biofilm (25,26).
Nevertheless, DGGE profile analysis did reveal a trend that biofilm composition
became more diverse during four weeks of chewing, irrespective of the gum type. This
effect was observed to be only temporal, since the biofilm composition returned to a less
diverse state during the washout period, which does not necessarily mean that bacterial
composition is the same as before four weeks of chewing. An increase in bacterial diversity
in oral biofilm is considered to be important in the maintenance of a healthy oral biofilm and
various studies have shown that progression of disease is related to the diversity of the
oral microbiome (3,4,27). For instance, the oral biofilm composition of children who did not
experience caries was more diverse than that of children who suffered from severe early
childhood caries (28). Bacterial diversity is similarly related to the occurrence of symptoms
in root canal infections and halitosis (3,27,29).
No differences were observed between the two widely different active ingredients
in the gums studied, which may reflect that the concentration of active ingredients in the
gums evaluated was too low or the length of the evaluation period too short. Alternatively, it
is likely that the effects observed in this study are solely related to the basic effects of
chewing sugar-free gum; mastication and stimulation of salivary flow. As food debris is
washed away during chewing (9), it also takes away sources of nutrients for bacteria, likely
affecting the composition of the oral biofilm.
In summary we have demonstrated that chewing two pieces of gum, three times
per day for four weeks does not significantly affect the total number and viability of bacteria
in oral biofilm, but that it creates a trend of increasing bacterial diversity in oral biofilm.
Since no differences between two widely different active ingredients were observed, this is
likely caused by the basic effects of chewing: mastication and stimulation of saliva. Disclosure statement This work was funded by Wm. Wrigley Jr. Co, Chicago, USA and SASA BV, Thesinge, NL.
Authors were employed by their own organizations. HJB is also director-owner of a
consulting company SASA BV, AM, MWJD are employees of Wm. Wrigley Jr. Company.
Opinions and assertions contained herein are those of the authors and are not meant to be
construed as the representing views of the organizations to which the authors are affiliated.
Acknowledgements We would like to thank all volunteers for their participation in the study.
EFFECTS OF CHEWING GUM ON ORAL BIOFILM VIABILITY AND COMPOSITION
41
3
References
1. Marsh PD, Moter A, Devine DA. Dental plaque biofilms: communities, conflict and control. Periodontol 2000. 2011; 55(1):16–35.
2. Marsh PD, Head DA, Devine DA. Ecological approaches to oral biofilms: Control without killing. Caries Res. 2015; 49(Suppl 1):46–54.
3. Zarco MF, Vess TJ, Ginsburg GS. The oral microbiome in health and disease and the potential impact on personalized dental medicine. Oral Dis. 2012; 18(2):109–20.
4. Gross EL, Leys EJ, Gasparovich SR, Firestone ND, Schwartzbaum JA., Janies DA., et al. Bacterial 16S sequence analysis of severe caries in young permanent teeth. J Clin Microbiol. 2010; 48(11):4121–8.
5. Reynolds EC, Cai F, Shen P, Walker GD. Retention in plaque and remineralization of enamel lesions by various forms of calcium in a mouthrinse or sugar-free chewing gum. J Dent Res. 2003; 82(3):206–11.
6. Otten MPT, Busscher HJ, Van der Mei HC, Abbas F, Van Hoogmoed CG. Retention of antimicrobial activity in plaque and saliva following mouthrinse use in vivo. Caries Res. 2010; 44(5):459–64.
7. Marsh PD. Dental plaque as a biofilm and a microbial community - implications for health and disease. BMC Oral Health. 2006; 6(Suppl 1):S14.
8. Bots CP, Brand HS, Veerman ECI, Van Amerongen BM, Nieuw Amerongen AV. Preferences and saliva stimulation of eight different chewing gums. Int Dent J. 2004; 54(3):143–8.
9. Fu Y, Li X, Ma H, Yin W, Que K.
Assessment of chewing sugar-free gums for oral debris reduction: a
randomized controlled crossover clinical trial. Am J Dent. 2012; 25(2):118–22.
10. Dodds MWJ, Chidichimo D, Haas MS.
Delivery of active agents from chewing gum for improved remineralization. Adv Dent Res. 2012; 24(2):58–62.
11. Mickenautsch S, Leal SC, Yengopal V, Bezerra AC, Cruvinel V. Sugar-free chewing gum and dental caries: a systematic review. J Appl Oral Sci. 2007; 15(2):83–8.
12. EFSA Panel on Dietetic Products Nutrition and Allergies (NDA). Scientific opinion on the substantiation of a health claim related to sugar free chewing gum and reduction of tooth demineralisation which reduces the risk of dental caries pursuant to Article 14 of Regulation (EC) No 1924/2006. EFSA J. 2010; 8(10):1775.
13. Chaudhary SA, Shahiwala AF.
Medicated chewing gum - a potential drug delivery system. Expert Opin Drug Deliv. 2010; 7(7):871–85.
14. Imfeld T. Chlorhexidine-containing chewing gum. Schweiz Monatssch Zahnmed. 2006; 116:476–83.
15. Greenberg M, Urnezis P, Tian M. Compressed mints and chewing gum containing magnolia bark extract are effective against bacteria responsible for oral malodor. J Agric Food Chem. 2007; 55(23):9465–9.
16. Campus G, Cagetti MG, Cocco F, Sale S, Sacco G, Strohmenger L, et al. Effect of a sugar-free chewing gum containing magnolia bark extract on different variables related to caries and gingivitis: a randomized controlled intervention trial. Caries Res. 2011; 45(4):393–9.
17. Hu Y, Qiao J, Zhang X, Ge C. Antimicrobial effect of Magnolia officinalis extract against Staphylococcus aureus. J Sci Food Agric. 2011; 91(6):1050–6.
CHAPTER 3
42
3
18. Ho K, Tsai C, Chen C. Antimicrobial activity of honokiol and magnolol isolated from Magnolia officinalis. Phyther Res. 2001; 141:139–41.
19. Walters P. Benefits of sodium hexametaphosphate-containing chewing gum for extrinsic stain inhibition. J Dent Hyg. 2004; 78(4):1–9.
20. Porciani P, Grandini S. Whitening effect by stain inhibition from a chewing gum with sodium hexametaphosphate in a controlled twelve-week single-blind trial. J Clin Dent. 2006; 17(1):14–6.
21. Van der Mei HC, Kamminga-Rasker HJ,De Vries J, Busscher HJ. The influence of a hexametaphosphate-containing chewing gum on the wetting ability of salivary conditioning films in vitro and in vivo. J Clin Dent. 2003; 14(1):14–8.
22. Syed SA, Loesche WJ. Survival of human dental plaque flora in various transport media. Appl Microbiol. 1972; 24(4):638–44.
23. Ferreira AVB, Glass NL. PCR from fungal spores after microwave treatment. Fungal Genet Newsl. 1996; 43:25–6.
24. Muyzer G, De Waal EC, Uitterlinden AG. Profiling of complex microbial populations by denaturing gradient gel electrophoresis analysis of polymerase chain reaction-amplified genes coding for 16S rRNA. Appl Env Microb. 1993; 59(3):695–700.
25. EFSA Panel on Dietetic Products Nutrition and Allergies (NDA). Scientific opinion on the substantiation of health claims related to sugar free chewing gum and reduction of dental plaque (ID 3084) pursuant to Article 13 (1) of Regulation (EC) No 1924/2006. EFSA J. 2010; 8(2):1480.
26. Mouton C, Scheinin A, Mäkinen K.
Effect on plaque of a xylitol-containing chewing-gum: A clinical and biochemical study. Acta Odontol Scand. 1975; 33:33–40.
27. He J, Li Y, Cao Y, Xue J, Zhou X. The
oral microbiome diversity and its relation to human diseases. Folia Microbiol (Praha). 2014; 60:69–80.
28. Li Y, Ge Y, Saxena D, Caufield PW. Genetic profiling of the oral microbiota associated with severe early-childhood caries. J Clin Microbiol. 2007; 45(1):81–7.
29. Kazor CE, Mitchell PM, Lee AM, Stokes LN, Dewhirst FE, Paster BJ, et al. Diversity of bacterial populations on the tongue dorsa of patients with halitosis and healthy patients. J Clin Microbiol. 2003; 41(2):558–63.





























