Embed Size (px)
Citation preview

University of Jordan 1
Renal system
Faisal I. Mohammed, MD, PhD
Yanal Shafagoj, MD, PhD

University of Jordan 2
Tubular reabsorption and tubular secretion Reabsorption – return of most of the filtered
water and many solutes to the bloodstream About 99% of filtered water reabsorbed Proximal convoluted tubule cells make largest
contribution Both active and passive processes
Secretion – transfer of material from blood into tubular fluid Helps control blood pH Helps eliminate substances from the body (K+)

University of Jordan 3
Reabsorption routes and transport mechanisms Reabsorption routes
Paracellular reabsorption Between adjacent tubule cells Tight junction do not completely seal off interstitial fluid from tubule
fluid Passive
Transcellular reabsorption – through an individual cell Transport mechanisms
Reabsorption of Na+ especially important Primary active transport
Sodium-potassium pumps in basolateral membrane only Secondary active transport
Symporters, antiporters Transport maximum (Tm)
Upper limit to how fast it can work Obligatory vs. facultative water reabsorption

University of Jordan 4
Reabsorption routes: paracellular reabsorption and transcellular reabsorption

University of Jordan 5
Reabsorption and secretion in proximal convoluted tubule (PCT)
Largest amount of solute and water reabsorption Secretes variable amounts of H+, NH4
+ Most solute reabsorption involves Na+
Symporters with glucose, amino acids, lactic acid, water-soluble vitamins, phosphate and sulfate
Na+ / H+ antiporter causes Na+ to be reabsorbed and H+ to be secreted Solute reabsorption promotes osmosis – creates osmotic gradient
Aquaporin-1 in cells lining PCT and descending limb of loop of Henle As water leaves tubular fluid, solute concentration increases
Urea and ammonia in blood are filtered at glomerulus and secreted by proximal convoluted tubule cells

University of Jordan 6
Reabsorption and secretion in the proximal convoluted tubule

University of Jordan 7
Reabsorption in the loop of Henle
Chemical composition of tubular fluid quite different from filtrate Glucose, amino acids and other nutrients were already
reabsorbed in PT At the entranc of LH Osmolarity still close to that of blood
Reabsorption of water and solutes balanced In the descending: For the first time reabsorption of water is
NOT automatically coupled to reabsorption of solutes Independent regulation of both volume and osmolarity of
body fluids Ascending: Na+-K+-2Cl- symporters function in Na+ and Cl-
reabsorption – promotes reabsorption of cations No water is reabsorbed in ascending limb – osmolarity
decreases

University of Jordan 8
Na+–K+-2Cl- symporter in the thick ascending limb of the loop of Henle…Lasix

University of Jordan 9
Reabsorption and secretion in the late distale convoluted tubule and collecting duct Reabsorption on the early distal convoluted tubule
Na+-Cl- symporters reabsorb Na+ and Cl- (Thiazide) Major site where parathyroid hormone stimulates
reabsorption of Ca+ depending on body’s needs Reabsorption and secretion in the late distal
convoluted tubule and collecting duct 90-95% of filtered solutes and fluid have been returned by
now Principal cells reabsorb Na+ and secrete K+
Intercalated cells reabsorb K+ and HCO3- and secrete H+
Amount of water reabsorption and solute reabsorption and secretion depends on body’s needs

University of Jordan 10
Hormonal regulation of tubular reabsorption and secretion
Angiotensin II - when blood volume and blood pressure decrease Decreases GFR, enhances reabsorption of Na+, Cl- and water
in PCT Aldosterone - when blood volume and blood pressure
decrease Stimulates principal cells in collecting duct to reabsorb more
Na+ and Cl- and secrete more K+ (Aldactone) Parathyroid hormone
Stimulates cells in DCT to reabsorb more Ca2+

University of Jordan 11
Regulation of facultative water reabsorption by ADH
Antidiuretic hormone (ADH or vasopressin) Increases water
permeability of cells by inserting aquaporin-2 in last part of DCT and collecting duct
Atrial natriuretic peptide (ANP) Large increase in blood
volume promotes release of ANP
Decreases blood volume and pressure by inhibiting reabsorption of Na+ and water in PCT and collecting duct, suppress secretion of ADH and aldosterone

ANP
Produced by atria due to stretching of walls. Antagonist to aldosterone. Increases Na+ and H20 excretion. Acts as an endogenous diuretic.

University of Jordan 13
Production of dilute and concentrated urine Even though your fluid intake can be highly
variable, total fluid volume in your body remains stable
Depends in large part on the kidneys to regulate the rate of water loss in urine
ADH controls whether dilute or concentrated urine is formed Absent or low ADH = dilute urine Higher levels = more concentrated urine through
increased water reabsorption

University of Jordan 14
Formation of dilute urine
Glomerular filtrate has same osmolarity as blood 300 mOsm/liter
Fluid leaving PCT is isotonic to plasma When dilute urine is being formed, the osmolarity
of fluid increases as it goes down the descending loop of Henle, decreases as it goes up the ascending limb, and decreases still more as it flows through the rest of the nephron and collecting duct

University of Jordan 15
Formation of dilute urine
Osmolarity of interstitial fluid of renal medulla becomes greater, more water is reabsorbed from tubular fluid so fluid become more concentrated
Water cannot leave in thick portion of ascending limb but solutes leave making fluid more dilute than blood plasma
Additional solutes but not much water leaves in DCT
Low ADH makes late DCT and collecting duct have low water permeability

University of Jordan 16
Formation of concentrated urine
Urine can be up to 4 times more concentrated than blood plasma
Ability of ADH depends on presence of osmotic gradient in interstitial fluid of renal medulla
3 major solutes contribute – Na+, Cl-, and urea 2 main factors build and maintain gradient
Differences in solute and water permeability in different sections of loop of Henle and collecting ducts
Countercurrent flow of fluid though descending and ascending loop of Henle and blood through ascending and descending limbs of vasa recta

University of Jordan 17
Countercurrent multiplication
Process by which a progressively increasing osmotic gradient is formed as a result of countercurrent flow
Long loops of Henle of juxtamedullary nephrons function as countercurrent multiplier
Symporters in thick ascending limb of loop of Henle cause buildup of Na+ and Cl- in renal medulla, cells impermeable to water
Countercurrent flow establishes gradient as reabsorbed Na+ and Cl- become increasingly concentrated
Cells in collecting duct reabsorb more water and urea Urea recycling causes a buildup of urea in the renal medulla Long loop of Henle establishes gradient by countercurrent
multiplication

University of Jordan 18
Countercurrent exchange
Process by which solutes and water are passively exchanged between blood of the vasa recta and interstitial fluid of the renal medulla as a result of countercurrent flow
Vasa recta is a countercurrent exchanger Osmolarity of blood leaving vasa recta is only
slightly higher than blood entering Provides oxygen and nutrients to medulla without
washing out or diminishing gradient Vasa recta maintains gradient by countercurrent
exchange

University of Jordan 19
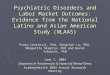
Mechanism of urine concentration in long-loop juxtamedullary nephrons

University of Jordan 20(b) Recycling of salts and urea in the vasa recta(a) Reabsorption of Na+CI– and water in a long-loop juxtamedullary nephron
Glomerular (Bowman’s) capsule
Afferentarteriole
Efferentarteriole
Glomerulus
Distal convoluted tubule
Proximalconvolutedtubule
Symporters in thickascending limb causebuildup of Na+ and Cl–
Interstitial fluidin renal medulla
300
1200
1000
800
Osmoticgradient
600
400
H2OH2O
H2O
200
1200
980
600780
400580
200380
300
100
Loop of Henle1200 Concentrated urine
300
300
320
400
600
800
1000
1200
800
H2O
Urea
Papillaryduct
Collectingduct
300
500
700
900
1100
1200
400
800
1000
600
Na+CI–
Blood flow
Flow of tubular fluid
Presense of Na+-K+-2CI–
symportersInterstitialfluid inrenal cortex
320
Juxtamedullary nephronand its blood supply together
Vasarecta
Loop ofHenle
H2O
H2O
H2O
H2O
H2O
H2O
H2O
1
H2O
H2O
Na+CI–
Na+CI–
H2O
Na+CI–
H2O
Na+CI–
(b) Recycling of salts and urea in the vasa recta(a) Reabsorption of Na+CI– and water in a long-loop juxtamedullary nephron
Glomerular (Bowman’s) capsule
Afferentarteriole
Efferentarteriole
Glomerulus
Distal convoluted tubule
Proximalconvolutedtubule
Symporters in thickascending limb causebuildup of Na+ and Cl–
Interstitial fluidin renal medulla
300
1200
1000
800
Osmoticgradient
600
400
H2OH2O
H2O
200
1200
980
600780
400580
200380
300
100
Loop of Henle1200 Concentrated urine
300
300
320
400
600
800
1000
1200
800
H2O
Urea
Papillaryduct
Collectingduct
Countercurrent flowthrough loop of Henleestablishes an osmoticgradient
300
500
700
900
1100
1200
400
800
1000
600
Na+CI–
Blood flow
Flow of tubular fluid
Presense of Na+-K+-2CI–
symportersInterstitialfluid inrenal cortex
320
Juxtamedullary nephronand its blood supply together
Vasarecta
Loop ofHenle
H2O
H2O
H2O
H2O
H2O
H2O
H2O
1
2
H2O
H2O
Na+CI–
Na+CI–
H2O
Na+CI–
H2O
Na+CI–
(b) Recycling of salts and urea in the vasa recta(a) Reabsorption of Na+CI– and water in a long-loop juxtamedullary nephron
Glomerular (Bowman’s) capsule
Afferentarteriole
Efferentarteriole
Glomerulus
Distal convoluted tubule
Proximalconvolutedtubule
Symporters in thickascending limb causebuildup of Na+ and Cl–
Interstitial fluidin renal medulla
300
1200
1000
800
Osmoticgradient
600
400
H2OH2O
H2O
200
1200
980
600780
400580
200380
300
100
Loop of Henle1200 Concentrated urine
300
300
320
400
600
800
1000
1200
800
H2O
Urea
Papillaryduct
Collectingduct
Countercurrent flowthrough loop of Henleestablishes an osmoticgradient
Principal cells incollecting ductreabsorb morewater when ADHis present
300
500
700
900
1100
1200
400
800
1000
600
Na+CI–
Blood flow
Flow of tubular fluid
Presense of Na+-K+-2CI–
symportersInterstitialfluid inrenal cortex
320
Juxtamedullary nephronand its blood supply together
Vasarecta
Loop ofHenle
H2O
H2O
H2O
H2O
H2O
H2O
H2O
1
2
3
H2O
H2O
Na+CI–
Na+CI–
H2O
Na+CI–
H2O
Na+CI–
(b) Recycling of salts and urea in the vasa recta(a) Reabsorption of Na+CI– and water in a long-loop juxtamedullary nephron
Glomerular (Bowman’s) capsule
Afferentarteriole
Efferentarteriole
Glomerulus
Distal convoluted tubule
Proximalconvolutedtubule
Symporters in thickascending limb causebuildup of Na+ and Cl–
Interstitial fluidin renal medulla
300
1200
1000
800
Osmoticgradient
600
400
H2OH2O
H2O
200
1200
980
600780
400580
200380
300
100
Loop of Henle1200 Concentrated urine
300
300
320
400
600
800
1000
1200
800
H2O
Urea
Papillaryduct
Urea recyclingcauses buildupof urea in therenal medulla
Collectingduct
Countercurrent flowthrough loop of Henleestablishes an osmoticgradient
Principal cells incollecting ductreabsorb morewater when ADHis present
300
500
700
900
1100
1200
400
800
1000
600
Na+CI–
Blood flow
Flow of tubular fluid
Presense of Na+-K+-2CI–
symportersInterstitialfluid inrenal cortex
320
Juxtamedullary nephronand its blood supply together
Vasarecta
Loop ofHenle
H2O
H2O
H2O
H2O
H2O
H2O
H2O
1
2
3
4
H2O
H2O
Na+CI–
Na+CI–
H2O
Na+CI–
H2O
Na+CI–

University of Jordan 21
Summary of filtration, reabsorption, and secretion in the nephron and collecting duct

Na+ Reabsorption
90% filtered Na+ reabsorbed in PCT.
In the absence of aldosterone, 80% of the remaining Na+ is reabsorbed in DCT.
Final [Na+] controlled in CD by aldosterone.
When aldosterone is secreted in maximal amounts, all Na+ in DCT is reabsorbed.
Insert fig. 17.26

K+ Secretion
90% filtered K+ is reabsorbed in early part of the nephron.
Secretion of K+ occurs in CD. Amount of K+ secreted depends upon:
Amount of Na+ delivered to the region. Amount of aldosterone secreted.
As Na+ is reabsorbed, lumen of tubule becomes –charged. Potential difference drives secretion of K+ into tubule.
Transport carriers for Na+ separate from transporters for K+.

K+ Secretion (continued)
Final [K+] controlled in CD by aldosterone. When
aldosterone is absent, no K+ is excreted in the urine.
High [K+] or low [Na+] stimulates the secretion of aldosterone.
Only means by which K+ is secreted.
Insert fig. 17.24

Renal Acid-Base Regulation
Kidneys help regulate blood pH by excreting H+ and reabsorbing HC03
-. Most of the H+ secretion occurs across the
walls of the PCT in exchange for Na+. Antiport mechanism.
Moves Na+ and H+ in opposite directions.
Normal urine normally is slightly acidic because the kidneys reabsorb almost all HC03
- and excrete H+. Returns blood pH back to normal range.

Reabsorption of HCO3-
Apical membranes of tubule cells are impermeable to HCO3
-. Reabsorption is indirect.
When urine is acidic, HCO3- combines with H+
to form H2C03-, which is catalyzed by ca
located in the apical cell membrane of PCT. As [C02] increases in the filtrate, C02 diffuses into
tubule cell and forms H2C03. H2C03 dissociates to HCO3
- and H+. HCO3
- generated within tubule cell diffuses into peritubular capillary.

Acidification of Urine
Insert fig. 17.28

Urinary Buffers
Nephron cannot produce a urine pH < 4.5. In order to excrete more H+, the acid must be
buffered. H+ secreted into the urine tubule and
combines with HPO4-2 or NH3.
HPO4-2 + H+ H2PO4
-
NH3 + H+ NH4+

Diuretics
Increase urine volume excreted. Increase the proportion of glomerular filtrate that is excreted as
urine.
Loop diuretics: Inhibit NaCl transport out of the ascending limb of the LH.
Thiazide diuretics: Inhibit NaCl reabsorption in the 1st segment of the DCT.
Ca inhibitors: Prevent H20 reabsorption in PCT when HC0s
- is reabsorbed.
Osmotic diuretics: Increase osmotic pressure of filtrate.

Clinical Diuretics Sites of Action
Insert fig. 17.29

University of Jordan 31
Evaluation of kidney function
Urinalysis Analysis of the volume and physical, chemical
and microscopic properties of urine Water accounts for 95% of total urine volume Typical solutes are filtered and secreted
substances that are not reabsorbed If disease alters metabolism or kidney function,
traces if substances normally not present or normal constituents in abnormal amounts may appear

University of Jordan 32
Evaluation of kidney function
Blood tests Blood urea nitrogen (BUN) – measures blood nitrogen that
is part of the urea resulting from catabolism and deamination of amino acids
Plasma creatinine results from catabolism of creatine phosphate in skeletal muscle – measure of renal function
Renal plasma clearance More useful in diagnosis of kidney problems than above Volume of blood cleared of a substance per unit time High renal plasma clearance indicates efficient excretion of
a substance into urine PAH administered to measure renal plasma flow

University of Jordan 33
Urine transportation, storage, and elimination Ureters
Each of 2 ureters transports urine from renal pelvis of one kidney to the bladder
Peristaltic waves, hydrostatic pressure and gravity move urine
No anatomical valve at the opening of the ureter into bladder – when bladder fills it compresses the opening and prevents backflow

University of Jordan 34
Ireters, urinary bladder, and urethra in a female

University of Jordan 35
Urinary bladder and urethra
Urinary bladder Hollow, distensible muscular organ Capacity averages 700-800mL Micturition – discharge of urine from bladder
Combination of voluntary and involuntary muscle contractions When volume increases stretch receptors send signals to
micturition center in spinal cord triggering spinal reflex – micturition reflex
In early childhood we learn to initiate and stop it voluntarily Urethra
Small tube leading from internal urethral orifice in floor of bladder to exterior of the body
In males discharges semen as well as urine

University of Jordan 36
Comparison between female and male urethras

Glucose and Amino Acid Reabsorption
Filtered glucose and amino acids are normally reabsorbed by the nephrons. In PCT occurs by secondary active transport with
membrane carriers. Carrier mediated transport displays:
Saturation. Tm.
[Transported molecules] needed to saturate carriers and achieve maximum transport rate.
Renal transport threshold: Minimum plasma [substance] that results in
excretion of that substance in the urine. Renal plasma threshold for glucose = 180-200 mg/dl.

Kidney Diseases
Acute renal failure: Ability of kidneys to excrete wastes and regulate
homeostasis of blood volume, pH, and electrolytes impaired. Rise in blood [creatinine]. Decrease in renal plasma clearance of creatinine.
Glomerulonephritis: Inflammation of the glomeruli. Autoimmune disease by which antibodies have been
raised against the glomerulus basement membrane. Leakage of protein into the urine.

Kidney Diseases (continued)
Renal insufficiency: Nephrons are destroyed. Clinical manifestations:
Salt and H20 retention. Uremia. Elevated plasma [H+] and [K+].
Dialysis: Separates molecules on the basis of the ability to
diffuse through selectively permeable membrane.

University of Jordan 40















![[PRTH 5.1 (2012) 65-80] Practical Theology (print) ISSN 1756 ......Interim Ministry and the Church of England Elizabeth Ann Jordan1 Rawreth Rectory, Church Road Rawreth, nr Wickford](https://img.pdfslide.net/doc/110x75/60bde89c031bce3f4a0a85bd/prth-51-2012-65-80-practical-theology-print-issn-1756-interim-ministry.jpg)